

COVID-19 Is a Confounder of Increased Candida Airway Colonisation



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Case Definition
2.5. Control Definitions
2.6. Data Collection
2.7. Statistical Analysis
3. Results
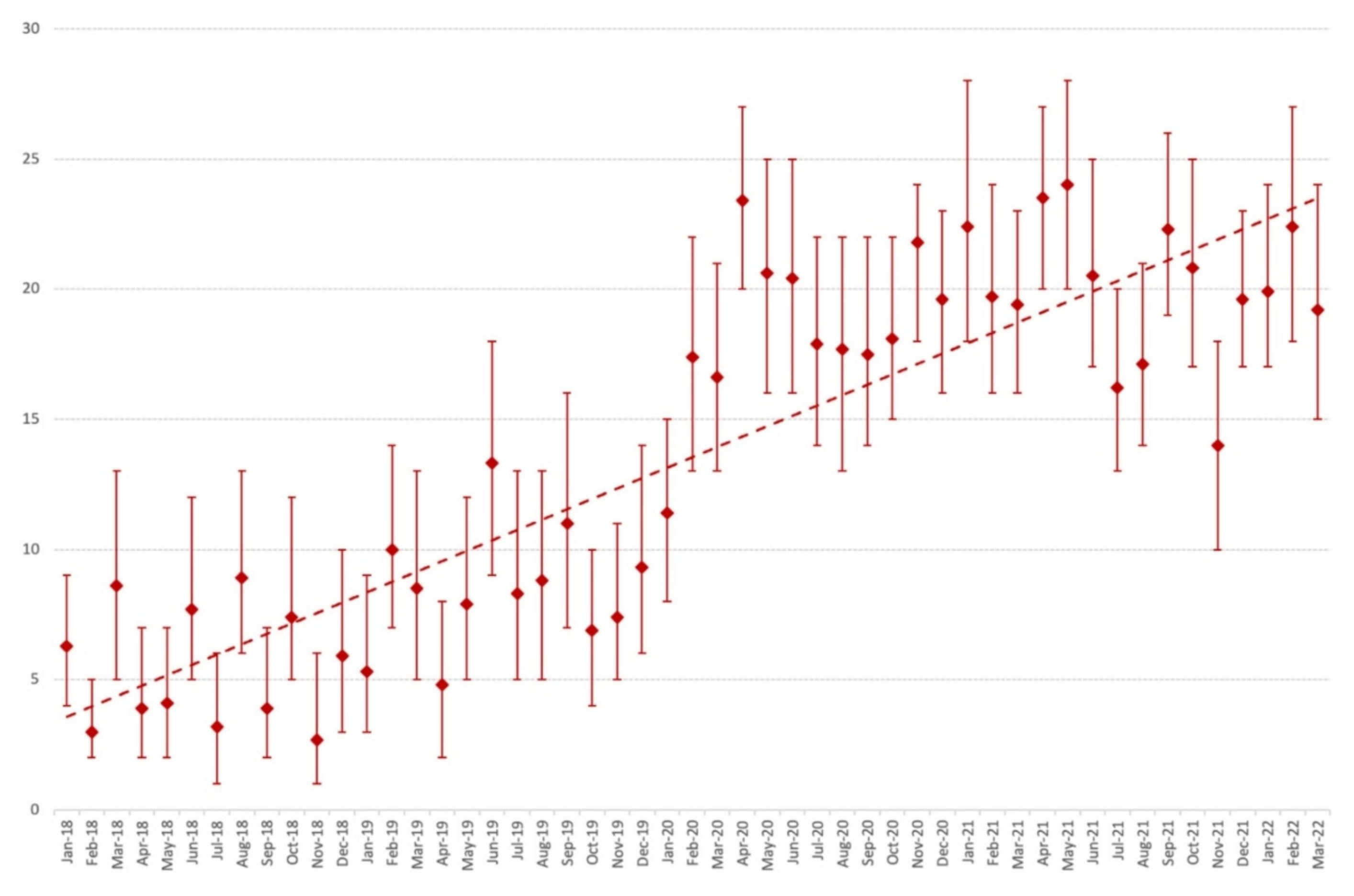
3.1. Time Trends in the Prevalence of Yeast-Positive Culture in Respiratory Samples
3.2. Patient Demographics
3.3. Characteristics of Hospital Stay
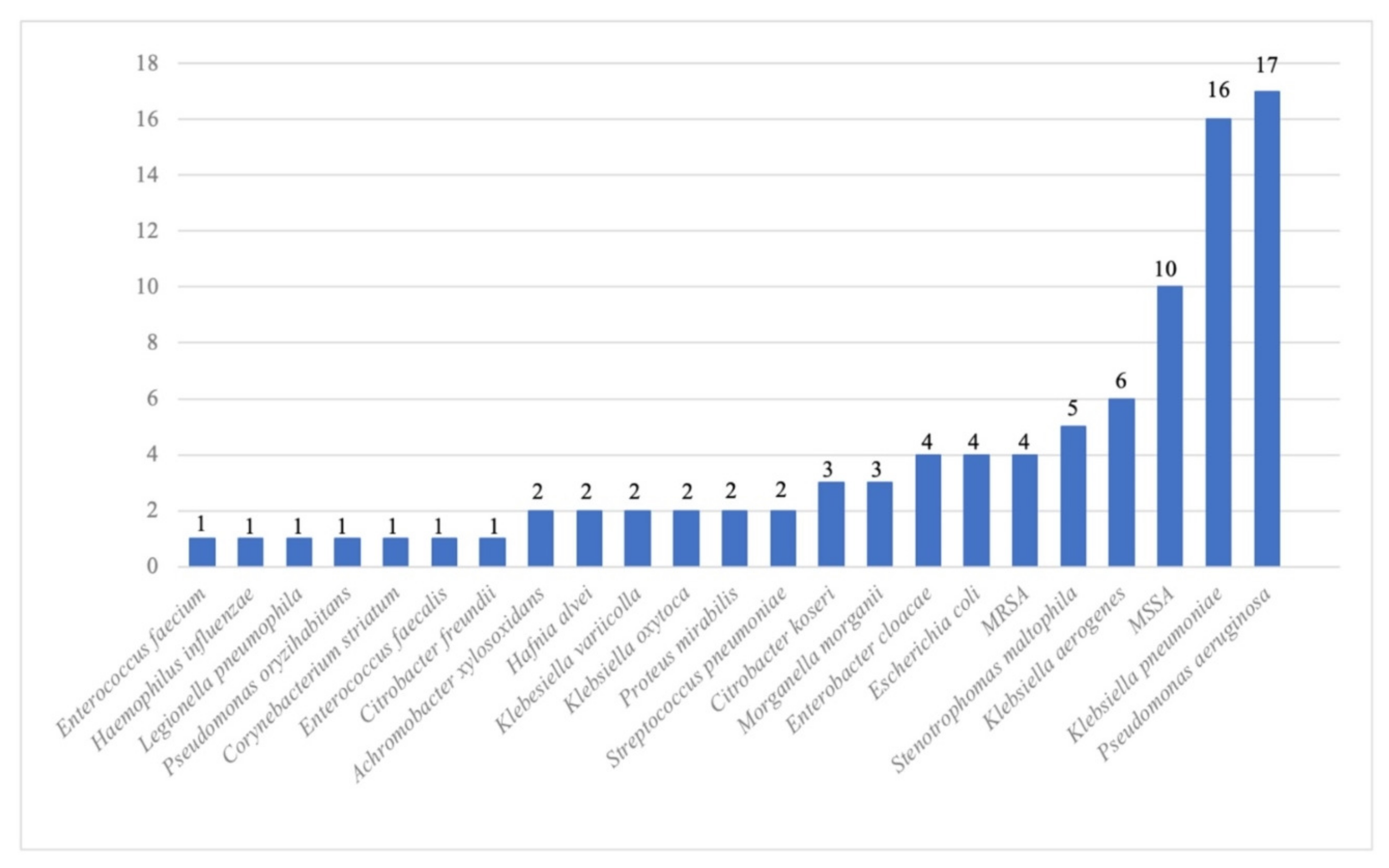
3.4. Microbiological Characteristics
3.5. Description of Candidaemia Cases
3.6. Documented SARS-CoV-2 Infection
3.7. Exposure to Antibacterials
3.8. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/data (accessed on 9 July 2022).
- Coronavirus: Chiffres clés et évolution de la COVID-19 en France et dans le Monde. Available online: https://www.santepubliquefrance.fr/dossiers/coronavirus-covid-19/coronavirus-chiffres-cles-et-evolution-de-la-covid-19-en-france-et-dans-le-monde (accessed on 9 July 2022).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, S.; Lee, N.; Park, Y.; Kim, J.; Jeon, K.; Park, M.-J.; Song, W. Prevalence and Clinical Impact of Coinfection in Patients with Coronavirus Disease 2019 in Korea. Viruses 2022, 14, 446. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; Timsit, J.-F.; Tafflet, M.; de Lassence, A.; Darmon, M.; Zahar, J.-R.; Adrie, C.; Garrouste-Orgeas, M.; Cohen, Y.; Mourvillier, B.; et al. Candida Colonization of the Respiratory Tract and Subsequent Pseudomonas Ventilator-Associated Pneumonia. Chest 2006, 129, 110–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.-L. The Prevalence of Nosocomial Infection in Intensive Care Units in Europe: Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. JAMA 1995, 274, 639. [Google Scholar] [CrossRef] [PubMed]
- Hamet, M.; Pavon, A.; Dalle, F.; Pechinot, A.; Prin, S.; Quenot, J.-P.; Charles, P.-E. Candida Spp. Airway Colonization Could Promote Antibiotic-Resistant Bacteria Selection in Patients with Suspected Ventilator-Associated Pneumonia. Intensive Care Med. 2012, 38, 1272–1279. [Google Scholar] [CrossRef]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and Fungal Coinfection among Hospitalized Patients with COVID-19: A Retrospective Cohort Study in a UK Secondary-Care Setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef]
- Pendleton, K.M.; Huffnagle, G.B.; Dickson, R.P. The Significance of Candida in the Human Respiratory Tract: Our Evolving Understanding. Pathog. Dis. 2017, 75, ftx029. [Google Scholar] [CrossRef] [Green Version]
- Erami, M.; Raiesi, O.; Momen-Heravi, M.; Getso, M.I.; Fakhrehi, M.; Mehri, N.; Yarahmadi, M.; Amiri, S.; Raissi, V.; Hashemi, S.J. Clinical Impact of Candida Respiratory Tract Colonization and Acute Lung Infections in Critically Ill Patients with COVID-19 Pneumonia. Microb. Pathog. 2022, 166, 105520. [Google Scholar] [CrossRef]
- Huang, D.; Qi, M.; Hu, Y.; Yu, M.; Liang, Z. The Impact of Candida Spp Airway Colonization on Clinical Outcomes in Patients with Ventilator-Associated Pneumonia: A Systematic Review and Meta-Analysis. Am. J. Infect. Control 2020, 48, 695–701. [Google Scholar] [CrossRef]
- Delisle, M.-S.; Williamson, D.R.; Perreault, M.M.; Albert, M.; Jiang, X.; Heyland, D.K. The Clinical Significance of Candida Colonization of Respiratory Tract Secretions in Critically Ill Patients. J. Crit. Care 2008, 23, 11–17. [Google Scholar] [CrossRef]
- Kaba, L.; Giraud-Gatineau, A.; Jimeno, M.-T.; Rolain, J.-M.; Colson, P.; Raoult, D.; Chaudet, H. Consequences of the COVID-19 Outbreak Lockdown on Non-Viral Infectious Agents as Reported by a Laboratory-Based Surveillance System at the IHU Méditerranée Infection, Marseille, France. JCM 2021, 10, 3210. [Google Scholar] [CrossRef]
- SPF. COVID-19: Point épidémiologique du 4 mars. 2020. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-4-mars-2020 (accessed on 29 August 2022).
- COVID-19: Prise En Charge Des Patients En Soins Critiques Au Cours Des Trois Premières Vagues de l’épidémie | Direction de La Recherche, Des Études, de l’évaluation et Des Statistiques. Available online: https://drees.solidarites-sante.gouv.fr/publications-communique-de-presse/etudes-et-resultats/covid-19-prise-en-charge-des-patients-en (accessed on 3 September 2022).
- Hedderwick, S.A.; Lyons, M.J.; Liu, M.; Vazquez, J.A.; Kauffman, C.A. Epidemiology of Yeast Colonization in the Intensive Care Unit. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 663–670. [Google Scholar] [CrossRef] [Green Version]
- Kayaaslan, B.; Kaya Kalem, A.; Asilturk, D.; Kaplan, B.; Dönertas, G.; Hasanoglu, I.; Eser, F.; Korkmazer, R.; Oktay, Z.; Ozkocak Turan, I.; et al. Incidence and Risk Factors for COVID-19 Associated Candidemia (CAC) in ICU Patients. Mycoses 2022, 65, 508–516. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; Nguyen, M.H.; Hedayati, M.T.; Netea, M.G.; Perlin, D.S.; Hoenigl, M. COVID-19-Associated Candidiasis (CAC): An Underestimated Complication in the Absence of Immunological Predispositions? J. Fungi 2020, 6, 211. [Google Scholar] [CrossRef]
- Avkan-Oğuz, V.; Çelİk, M.; Eren-Kutsoylu, O.Ö.; Nazli, A.; Uğur, Y.L.; Taylan, A.; Ergan, B.; Irmak, Ç.; Duğral, E.; Özkütük, A.A. Fungal Colonization and Infections in Patients with COVID-19 in Intensive Care Units: A Real-Life Experience at a Tertiary-Care Hospital. Respir. Med. Res. 2022, 82, 100937. [Google Scholar] [CrossRef]
- Blaize, M.; Raoelina, A.; Kornblum, D.; Kamus, L.; Lampros, A.; Berger, M.; Demeret, S.; Constantin, J.-M.; Monsel, A.; Mayaux, J.; et al. Occurrence of Candidemia in Patients with COVID-19 Admitted to Five ICUs in France. J. Fungi 2022, 8, 678. [Google Scholar] [CrossRef]
- Gangneux, J.-P.; Dannaoui, E.; Fekkar, A.; Luyt, C.-E.; Botterel, F.; De Prost, N.; Tadié, J.-M.; Reizine, F.; Houzé, S.; Timsit, J.-F.; et al. Fungal Infections in Mechanically Ventilated Patients with COVID-19 during the First Wave: The French Multicentre MYCOVID Study. Lancet Respir. Med. 2022, 10, 180–190. [Google Scholar] [CrossRef]
- Pittet, D.; Monod, M.; Suter, P.M.; Frenk, E.; Auckenthaler, R. Candida Colonization and Subsequent Infections in Critically III Surgical Patients. Ann. Surg. 1994, 220, 751–758. [Google Scholar] [CrossRef]
- Eggimann, P.; Garbino, J.; Pittet, D. Epidemiology of Candida Species Infections in Critically Ill Non-Immunosuppressed Patients. Lancet Infect. Dis. 2003, 3, 685–702. [Google Scholar] [CrossRef]
- Tran, L.T.; Auger, P.; Marchand, R.; Carrier, M.; Pelletier, C. Epidemiological Study of Candida Spp. Colonization in Cardiovascular Surgical Patients. Mycoses 1997, 40, 169–173. [Google Scholar] [CrossRef]
- Blot, S.I.; Vandewoude, K.H.; Hoste, E.A.; Colardyn, F.A. Effects of Nosocomial Candidemia on Outcomes of Critically Ill Patients. Am. J. Med. 2002, 113, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Delisle, M.-S.; Williamson, D.R.; Albert, M.; Perreault, M.M.; Jiang, X.; Day, A.G.; Heyland, D.K. Impact of Candida Species on Clinical Outcomes in Patients with Suspected Ventilator-Associated Pneumonia. Can. Respir. J. 2011, 18, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakraborti, A.; Jaiswal, A.; Verma, P.K.; Singhal, R. A Prospective Study of Fungal Colonization and Invasive Fungal Disease in Long-Term Mechanically Ventilated Patients in a Respiratory Intensive Care Unit. Indian J. Crit. Care Med. 2018, 22, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Charles, P.E.; Dalle, F.; Aube, H.; Doise, J.M.; Quenot, J.P.; Aho, L.S.; Chavanet, P.; Blettery, B. Candida Spp. Colonization Significance in Critically Ill Medical Patients: A Prospective Study. Intensive Care Med. 2005, 31, 393–400. [Google Scholar] [CrossRef]
- León, C.; Álvarez-Lerma, F.; Ruiz-Santana, S.; León, M.Á.; Nolla, J.; Jordá, R.; Saavedra, P.; Palomar, M. The EPCAN Study Group Fungal Colonization and/or Infection in Non-Neutropenic Critically Ill Patients: Results of the EPCAN Observational Study. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 233–242. [Google Scholar] [CrossRef]
- el-Ebiary, M.; Torres, A.; Fàbregas, N.; de la Bellacasa, J.P.; González, J.; Ramirez, J.; del Baño, D.; Hernández, C.; Jiménez de Anta, M.T. Significance of the Isolation of Candida Species from Respiratory Samples in Critically Ill, Non-Neutropenic Patients. An Immediate Postmortem Histologic Study. Am. J. Respir. Crit. Care Med. 1997, 156, 583–590. [Google Scholar] [CrossRef]
- Magill, S.S.; Swoboda, S.M.; Johnson, E.A.; Merz, W.G.; Pelz, R.K.; Lipsett, P.A.; Hendrix, C.W. The Association between Anatomic Site of Candida Colonization, Invasive Candidiasis, and Mortality in Critically Ill Surgical Patients. Diagn. Microbiol. Infect. Dis. 2006, 55, 293–301. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) | Case (n = 100) | Bbact (n = 100) | NegC (n = 100) | p * |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Males | 66 (66) | 64 (64) | 61 (61) | 0.7605 |
| Age, years † | 57 ± 16 | 58 ± 16 | 58 ± 15 | 0.8752 |
| Intensive care unit | 80 (80) | 62 (62) | 18 (18) | <10−4 |
| Hospital length of stay, days † | 46 ± 37 | 26 ± 22 | 9 ± 8 | <0.0001 |
| Comorbidities | ||||
| BMI | ||||
| BMI < 25 | 33 (44) | 46 (56) | 51 (59) | 0.1283 |
| 25 < BMI < 30 | 19 (25) | 21(25) | 17 (20) | 0.6033 |
| 30 ≤ BMI < 35 | 16 (21) | 9 (11) | 10 (12) | 0.1200 |
| 35 ≤ BMI < 40 | 7 (9) | 3 (4) | 4 (5) | 0.2691 |
| 40 ≥ BMI | 0 (0) | 3 (4) | 2 (2) | 0.2659 |
| High blood pressure | 42 (42) | 39 (39) | 31 (31) | 0.2511 |
| Cardiovascular disease | 15 (15) | 20 (20) | 14 (14) | 0.4695 |
| Diabetes | 31 (31) | 26 (26) | 7 (7) | <10−4 |
| Smoking | 25 (25) | 21 (21) | 28 (28) | 0.5149 |
| Chronic respiratory failure | 28 (28) | 28 (28) | 23 (23) | 0.6508 |
| Chronic renal failure ‡ | 10 (10) | 15 (15) | 7 (7) | 0.1801 |
| Solid cancer | 7 (7) | 16 (16) | 22 (22) | 0.0114 |
| Haematological disease | 0 (0) | 3 (3) | 4 (4) | 0.1493 |
| Transplantation | 11 (11) | 19 (19) | 14 (14) | 0.2712 |
| Immunosuppression | 17 (17) | 31 (31) | 33 (33) | 0.0212 |
| Immunosuppressive treatments § | 15 (15) | 28 (28) | 26 (26) | 0.0629 |
| Ventilation/oxygen therapy | ||||
| Low-dose oxygen therapy | 6 (6) | 13 (13) | 12 (12) | 0.2129 |
| HFNC | 1 (1) | 2 (2) | 3 (3) | 0.6004 |
| Non-invasive ventilation | 1 (1) | 5 (5) | 3 (3) | 0.2529 |
| Mechanical ventilation | 80 (80) | 56 (56) | 15 (15) | <10−4 |
| ECMO | 22 (22) | 13 (13) | 1 (1) | <10−4 |
| Nutrition | 77 (77) | 53 (53) | 14 (14) | |
| Enteral nutrition | 76 (76) | 50 (50) | 14 (14) | <10−4 |
| Parenteral nutrition | 1 (1) | 3 (3) | 0 (0) | 0.1697 |
| Central venous catheter | 79 (79) | 58 (58) | 15 (15) | <10−4 |
| Abdominal surgery | 10 (10) | 2 (2) | 4 (4) | 0.0323 |
| SARS-CoV-2 infection | 53 (53) | 29 (29) | 17 (17) | <10−4 |
| Antibiotic therapy | 88 (88) | 88 (88) | 35 (35) | <10−4 |
| Antifungals | 26 (26) | 5 (5) | 2 (2) | <10−4 |
| Antivirals | 27 (27) | 12 (12) | 1 (1) | <10−4 |
| Nature of respiratory sample | ||||
| BAL | 78 (78) | 76 (76) | 75 (75) | 0.8788 |
| TBA | 70 (70) | 43 (43) | 12 (12) | <10−4 |
| CBES | 27 (27) | 26 (26) | 28 (28) | 0.9505 |
| Respiratory viral infection | 25 (25) | 13 (13) | 1 (1) | <10−4 |
| Fungal infection | 16 (16) | 3 (3) | 0 (0) | <10−4 |
| Fatality, n (%) | 29 (29) | 23 (23) | 10 (10) | 0.0032 |
| Patients | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Demographic characteristics | |||||
| Gender | Male | Female | Male | Male | Female |
| Age (years) | 62 | 68 | 46 | 72 | 69 |
| Known immunosuppression | No | Anti-TNF α treatment | No | No | No |
| Comorbidities * | HBP | Diab, CV | Ob, Smo | HBP, Diab, Smo | HBP, Ob |
| Clinical characteristics | |||||
| Length of stay (days) | 120 | 108 | 72 | 49 | 72 |
| Mechanical ventilation | Yes | Yes | Yes | Yes | Yes |
| ECMO ** | Yes | No | No | No | No |
| SARS-CoV-2 | Yes | Yes | No | Yes | No |
| Abdominal surgery | No | Yes | Yes | No | No |
| Mycological culture | |||||
| Respiratory colonisation | C. albicans | C. albicans | C. glabrata | C. glabrata | C. utilis |
| Other colonised site | Urine | Urine | No | No | Urine |
| Blood cultures (BC) | C. albicans | K. marxianus | C. glabrata | C. glabrata | C. metapsilosis |
| No. of positive BCs | 3 | 2 | 2 | 3 | 2 |
| Treatments and outcome | |||||
| Antifungal treatments *** | Casp | Casp | Casp, Vorico | Casp | Casp, Fluco |
| Outcome | Alive | Alive | Alive | Alive | Alive |
| Characteristics | Cases = n (%) | BactC = n (%) | NegC = n (%) | p |
|---|---|---|---|---|
| SARS-CoV-2 | 53 (53) | 29 (29) | 17 (17) | <10−4 |
| Intensive care unit | 51 (51) | 18 (18) | 17 (17) | <10−4 |
| Immunomodulatory treatments | ||||
| Dexamethasone | 53 (53) | 28 (28) | 10 (10) | <10−4 |
| Methylprednisolone | 37 (37) | 16 (16) | 3 (3) | <10−4 |
| Tocilizumab | 6 (6) | 7 (7) | 0 (0) | 0.6045 |
| Cases vs. BactC + NegC | Cases vs. BactC | Cases vs. NegC | |
|---|---|---|---|
| OR [95% CI] *, p | OR [95%CI], p | OR, [95% CI], p | |
| Oxacillin IV | 4.42 [1.05–18.62], 0.0427 | - | - |
| Ceftazidime | 2.30 [1.13–4.66)], 0.0213 | - | - |
| Cefepime | 2.83 [1.42–1.64], 0.0030 | 17.66 [3.95–79.06], 0.0002 | - |
| Piperacillin/tazobactam | 1.99 [1.14–3.45], 0.0148 | - | - |
| Linezolid | - | - | 2.57 [1.23–5.36], 0.0120 |
| Carbapenems | 3.00 [1.58–5.68], 0.0007 | 22.84 [5.18–100.61], <10−4 | |
| Length of stay | 1.02 [1.01–1.03], <10−4 | 1.06 [1.02–1.09], 0.0007 | 1.02 [1.01–1.03], 0.0021 |
| Diabetes | 2.12 [1.10–4.07], 0.0248 | 7.44 [2.85–19.65], 0.0006 | - |
| MV † | 3.48 [1.79–6.74], 0.0002 | 7.48 [2.85–19.65], <10−4 | - |
| Fungal coinfection | 6.71 [1.67–26.97], 0.0073 | - | - |
| Solid malignancies | - | 0.22 [0.06–0.73], 0.0138 | - |
| Antifungal | - | - | 4,17 [0.46–11.96], 0.0078 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Froidefond, M.; Sevestre, J.; Chaudet, H.; Ranque, S. COVID-19 Is a Confounder of Increased Candida Airway Colonisation. Pathogens 2023, 12, 463. https://doi.org/10.3390/pathogens12030463
Froidefond M, Sevestre J, Chaudet H, Ranque S. COVID-19 Is a Confounder of Increased Candida Airway Colonisation. Pathogens. 2023; 12(3):463. https://doi.org/10.3390/pathogens12030463
Chicago/Turabian StyleFroidefond, Margaux, Jacques Sevestre, Hervé Chaudet, and Stéphane Ranque. 2023. "COVID-19 Is a Confounder of Increased Candida Airway Colonisation" Pathogens 12, no. 3: 463. https://doi.org/10.3390/pathogens12030463
APA StyleFroidefond, M., Sevestre, J., Chaudet, H., & Ranque, S. (2023). COVID-19 Is a Confounder of Increased Candida Airway Colonisation. Pathogens, 12(3), 463. https://doi.org/10.3390/pathogens12030463