
Reduced Cholesterol Levels during Acute Human Babesiosis

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
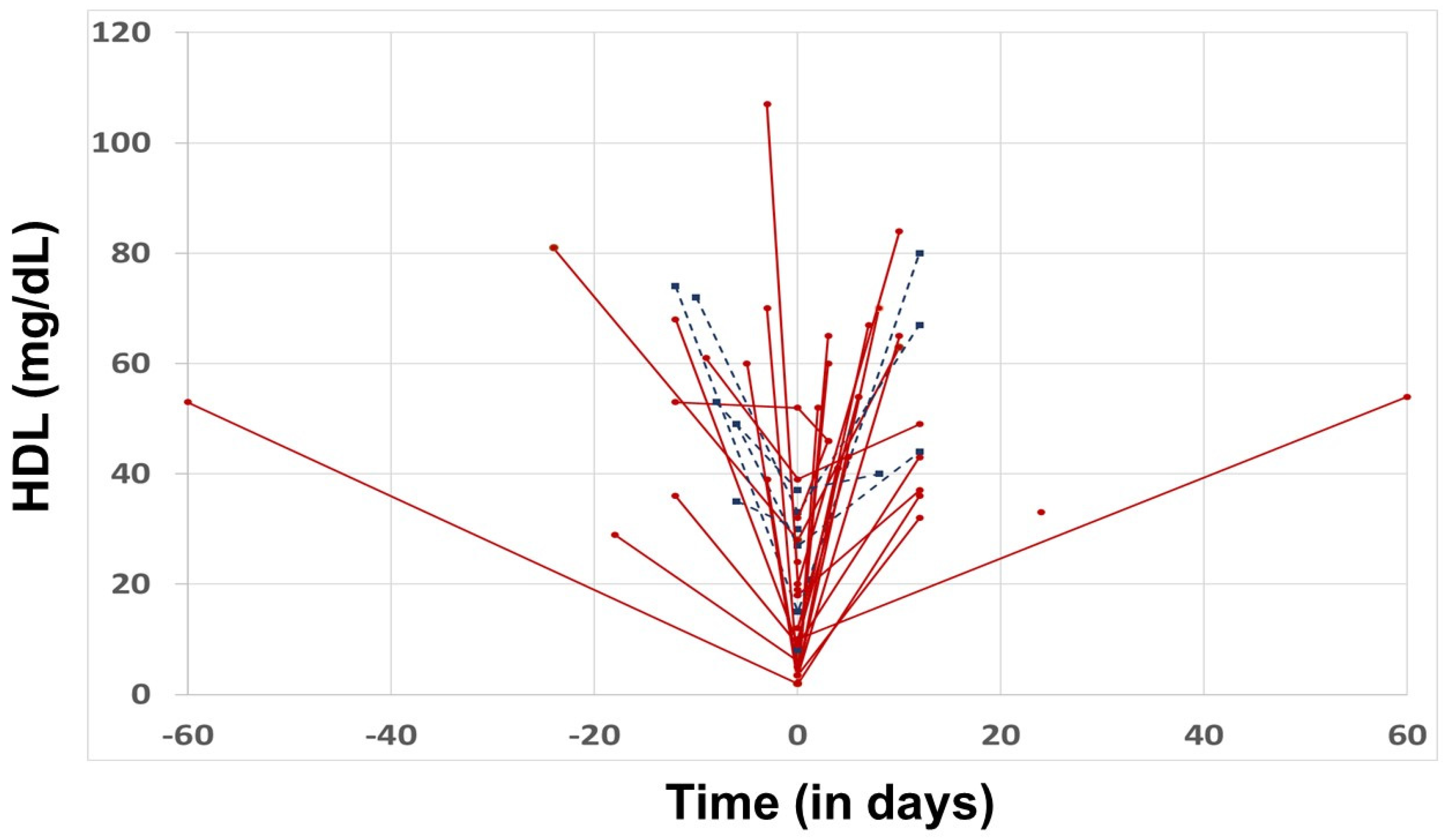
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, A.; O’Bryan, J.; Krause, P.J. The Global Emergence of Human Babesiosis. Pathogens 2021, 10, 1447. [Google Scholar] [CrossRef] [PubMed]
- Kletsova, E.A.; Spitzer, E.D.; Fries, B.C.; Marcos, L.A. Babesiosis in Long Island: Review of 62 cases focusing on treatment with azithromycin and atovaquone. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Puri, A.; Bajpai, S.; Meredith, S.; Aravind, L.; Krause, P.J.; Kumar, S. Babesia microti: Pathogen Genomics, Genetic Variability, Immunodominant Antigens, and Pathogenesis. Front. Microbiol. 2021, 12, 697669. [Google Scholar] [CrossRef] [PubMed]
- Marcos, L.A.; Leung, A.; Kirkman, L.; Wormser, G.P. Use of tafenoquine to treat a patient with relapsing babesiosis with clinical and molecular evidence of resistance to azithromycin and atovaquone. IDCases 2022, 27, e01460. [Google Scholar] [CrossRef] [PubMed]
- Zahra, A.; Marcos, L.A. Hemagophagocytic lymphohistiocytosis associated with recurrent Babesiosis with Lyme disease co-infection in an immunocompromised host on anti-CD20 monoclonal antibody therapy: A case report. IDCases 2022, 29, e01570. [Google Scholar] [CrossRef]
- Bloch, E.M.; Day, J.R.; Krause, P.J.; Kjemtrup, A.; O’Brien, S.F.; Tobian, A.A.R.; Goel, R. Epidemiology of Hospitalized Patients with Babesiosis, United States, 2010–2016. Emerg. Infect. Dis. 2022, 28, 354–362. [Google Scholar] [CrossRef]
- Nixon, C.P.; Park, S.; Nixon, C.E.; Reece, R.M.; Sweeney, J.D. Adjunctive treatment of clinically severe babesiosis with red blood cell exchange: A case series of nineteen patients. Transfusion 2019, 59, 2629–2635. [Google Scholar] [CrossRef]
- Waked, R.; Krause, P.J. Human Babesiosis. Infect. Dis. Clin. N. Am. 2022, 36, 655–670. [Google Scholar] [CrossRef]
- Conte, H.A.; Biondi, M.C.; Janket, S.J.; Ackerson, L.K.; Diamandis, E.P. Babesia microti-induced fulminant sepsis in an immunocompromised host: A case report and the case-specific literature review. Open Life Sci. 2022, 17, 1200–1207. [Google Scholar] [CrossRef]
- Long, N.P.; Anh, N.K.; Yen, N.T.H.; Phat, N.K.; Park, S.; Thu, V.T.A.; Cho, Y.S.; Shin, J.G.; Oh, J.Y.; Kim, D.H. Comprehensive lipid and lipid-related gene investigations of host immune responses to characterize metabolism-centric biomarkers for pulmonary tuberculosis. Sci. Rep. 2022, 12, 13395. [Google Scholar] [CrossRef]
- Shan, J.; Qian, W.; Shen, C.; Lin, L.; Xie, T.; Peng, L.; Xu, J.; Yang, R.; Ji, J.; Zhao, X. High-resolution lipidomics reveals dysregulation of lipid metabolism in respiratory syncytial virus pneumonia mice. RSC Adv. 2018, 8, 29368–29377. [Google Scholar] [CrossRef] [PubMed]
- Manzano, J.I.; Perea-Martínez, A.; García-Hernández, R.; Andrés-León, E.; Terrón-Camero, L.C.; Poveda, J.A.; Gamarro, F. Modulation of Cholesterol Pathways in Human Macrophages Infected by Clinical Isolates of Leishmania infantum. Front. Cell. Infect. Microbiol. 2022, 12, 878711. [Google Scholar] [CrossRef] [PubMed]
- Cunha, B.A.; Crean, J.; Rosenbaum, G. Lipid abnormalities in babesiosis. Am. J. Med. 2000, 108, 758–759. [Google Scholar] [CrossRef] [PubMed]
- Bock, J.L.; Senzel, L.; Spitzer, E.D.; Bifulco, W. Undetectable HDL cholesterol in a patient with flu-like illness. Clin. Chem. 2017, 63, 642–646. [Google Scholar] [CrossRef]
- Mrljak, V.; Kučer, N.; Kuleš, J.; Tvarijonaviciute, A.; Brkljačić, M.; Crnogaj, M.; Živičnjak, T.; Šmit, I.; Ceron, J.J.; Rafaj, R.B. Serum concentrations of eicosanoids and lipids in dogs naturally infected with Babesia canis. Vet Parasitol. 2014, 201, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Milanović, Z.; Vekić, J.; Radonjić, V.; Ilić Božović, A.; Zeljković, A.; Janac, J.; Spasojević-Kalimanovska, V.; Buch, J.; Chandrashekar, R.; Bojić-Trbojević, Ž.; et al. Association of acute Babesia canis infection and serum lipid, lipoprotein, and apoprotein concentrations in dogs. J. Vet. Intern. Med. 2019, 33, 1686–1694. [Google Scholar] [CrossRef] [PubMed]
- Valentin, A.; Rigomier, D.; Précigout, E.; Carcy, B.; Gorenflot, A.; Schrével, J. Lipid trafficking between high density lipoproteins and Babesia divergens-infected human erythrocytes. Biol. Cell 1991, 73, 63–70. [Google Scholar] [CrossRef]
- Tisdall, A.R.; Crowley, V.E.F.; Crook, M.A. Undetectable high-density lipoprotein cholesterol in acute malaria. J. Clin. Lipidol. 2018, 12, 822–825. [Google Scholar] [CrossRef]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. HDL in infectious diseases and sepsis. Handb. Exp. Pharmacol. 2015, 224, 483–508. [Google Scholar]
- Vanhamme, L.; Paturiaux-Hanocq, F.; Poelvoorde, P.; Nolan, D.P.; Lins, L.; Van Den Abbeele, J.; Pays, A.; Tebabi, P.; Van Xong, H.; Jacquet, A.; et al. Apolipoprotein L-I is the trypanosome lytic factor of human serum. Nature 2003, 422, 83–87. [Google Scholar] [CrossRef]
- Samanovic, M.; Molina-Portela, M.P.; Chessler, A.D.; Burleigh, B.A.; Raper, J. Trypanosome lytic factor, an antimicrobial high-density lipoprotein, ameliorates Leishmania infection. PLoS Pathog. 2009, 5, e1000276. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, A.J.; Butler, L.R.; Rolandelli, A.; Gilk, S.D.; Pedra, J.H. Lipid hijacking: A unifying theme in vector-borne diseases. eLife 2020, 9, e61675. [Google Scholar] [CrossRef] [PubMed]
- Iso-o, N.; Komatsuya, K.; Tokumasu, F.; Isoo, N.; Ishigaki, T.; Yasui, H.; Yotsuyanagi, H.; Hara, M.; Kita, K. Malaria Parasites Hijack Host Receptors From Exosomes to Capture Lipoproteins. Front. Cell Dev. Biol. 2021, 9, 749153. [Google Scholar] [CrossRef] [PubMed]
- Maier, A.G.; van Ooij, C. The role of cholesterol in invasion and growth of malaria parasites. Front. Cell. Infect. Microbiol. 2022, 12, 984049. [Google Scholar] [CrossRef]
- Koopman, J.P.R.; Lule, S.A.; Zziwa, C.; Akurut, H.; Lubyayi, L.; Nampijja, M.; Akello, F.; Balungi, P.; Tumusiime, J.; Oduru, G.; et al. The determinants of lipid profiles in early adolescence in a Ugandan birth cohort. Sci. Rep. 2021, 11, 16503. [Google Scholar] [CrossRef]
- Usman, M.A.; Ibrahim, M.A.; Salman, A.A.; Sallau, A.B. Depletion of cholesterol could be associated with modulation of progesterone but not other sex hormone levels during Plasmodium falciparum infection in humans: A cross-sectional study from Zaria, Nigeria. Parasitol. Res. 2020, 119, 4143–4150. [Google Scholar] [CrossRef]


{kind=link}
| Admitted | Not Admitted | ||||
|---|---|---|---|---|---|
| Variable | N | Median (IQR) | N | Median (IQR) | p Value |
| Age | 33 | 67.00 (56.00–83.50) | 6 | 72.50 (67.00–80.00) | 0.57 |
| Parasitemia (%) | 33 | 0.90 (0.30–2.65) | 6 | 0.40 (0.10–0.50) | 0.08 |
| Hemoglobin (g/dL) | 33 | 11.60 (9.85–13.00) | 6 | 12.65 (12.00–13.20) | 0.30 |
| Total Cholesterol | 31 | 104.00 (84.00–129.00) | 6 | 119.00 (106.00–127.00) | 0.29 |
| LDL (mg/dL) | 23 | 46.00 (32.00–67.00) | 5 | 76.00 (59.00–85.00) | 0.04 |
| HDL (mg/dL) | 31 | 9.00 (3.50–19.00) | 6 | 28.50 (15.00–33.00) | 0.03 |
| TG (mg/dL) | 31 | 190.00 (123.00–311.00) | 6 | 110.00 (100.00–121.00) | 0.07 |
| VLDL (mg/dL) | 29 | 38.00 (25.00–55.00) | 6 | 22.00 (20.00–24.00) | 0.09 |
| Variable | Change | N | Median | Lower Quartile | Upper Quartile | p Value |
|---|---|---|---|---|---|---|
| Total Cholesterol | [acute]-[pre] | 16 | −73 | −95.5 | −33 | 0.0002 |
| [post]-[acute] | 23 | 61 | 25 | 108 | <0.0001 | |
| LDL | [acute]-[pre] | 12 | −26.5 | −54.5 | 3.5 | 0.082 |
| [post]-[acute] | 15 | 37 | 26 | 55 | 0.0006 | |
| HDL | [acute]-[pre] | 16 | −37.25 | −58.5 | −22 | <0.0001 |
| [post]-[acute] | 23 | 35 | 19 | 58 | <0.0001 | |
| TG | [acute]-[pre] | 16 | 58.5 | 15.5 | 175.5 | 0.0013 |
| [post]-[acute] | 23 | −72 | −168 | −24 | <0.0001 | |
| VLDL | [acute]-[pre] | 15 | 10 | 0 | 32 | 0.0022 |
| [post]-[acute] | 21 | −14 | −26 | −5 | 0.0002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcos, L.A.; Vorkas, C.K.; Mann, I.; Garry, E.; Lamba, P.; Pham, S.K.; Spector, R.; Papamanoli, A.; Krivacsy, S.; Lum, M.; et al. Reduced Cholesterol Levels during Acute Human Babesiosis. Pathogens 2023, 12, 613. https://doi.org/10.3390/pathogens12040613
Marcos LA, Vorkas CK, Mann I, Garry E, Lamba P, Pham SK, Spector R, Papamanoli A, Krivacsy S, Lum M, et al. Reduced Cholesterol Levels during Acute Human Babesiosis. Pathogens. 2023; 12(4):613. https://doi.org/10.3390/pathogens12040613
Chicago/Turabian StyleMarcos, Luis A., Charles Kyriakos Vorkas, Inderjit Mann, Evan Garry, Pooja Lamba, Sophia K. Pham, Rachel Spector, Aikaterini Papamanoli, Sara Krivacsy, Michael Lum, and et al. 2023. "Reduced Cholesterol Levels during Acute Human Babesiosis" Pathogens 12, no. 4: 613. https://doi.org/10.3390/pathogens12040613
APA StyleMarcos, L. A., Vorkas, C. K., Mann, I., Garry, E., Lamba, P., Pham, S. K., Spector, R., Papamanoli, A., Krivacsy, S., Lum, M., Zahra, A., Hou, W., & Spitzer, E. D. (2023). Reduced Cholesterol Levels during Acute Human Babesiosis. Pathogens, 12(4), 613. https://doi.org/10.3390/pathogens12040613