
Effectiveness of Intermittent Preventive Treatment with Sulfadoxine-Pyrimethamine in Pregnancy: Low Coverage and High Prevalence of Plasmodium falciparum dhfr-dhps Quintuple Mutants as Major Challenges in Douala, an Urban Setting in Cameroon

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
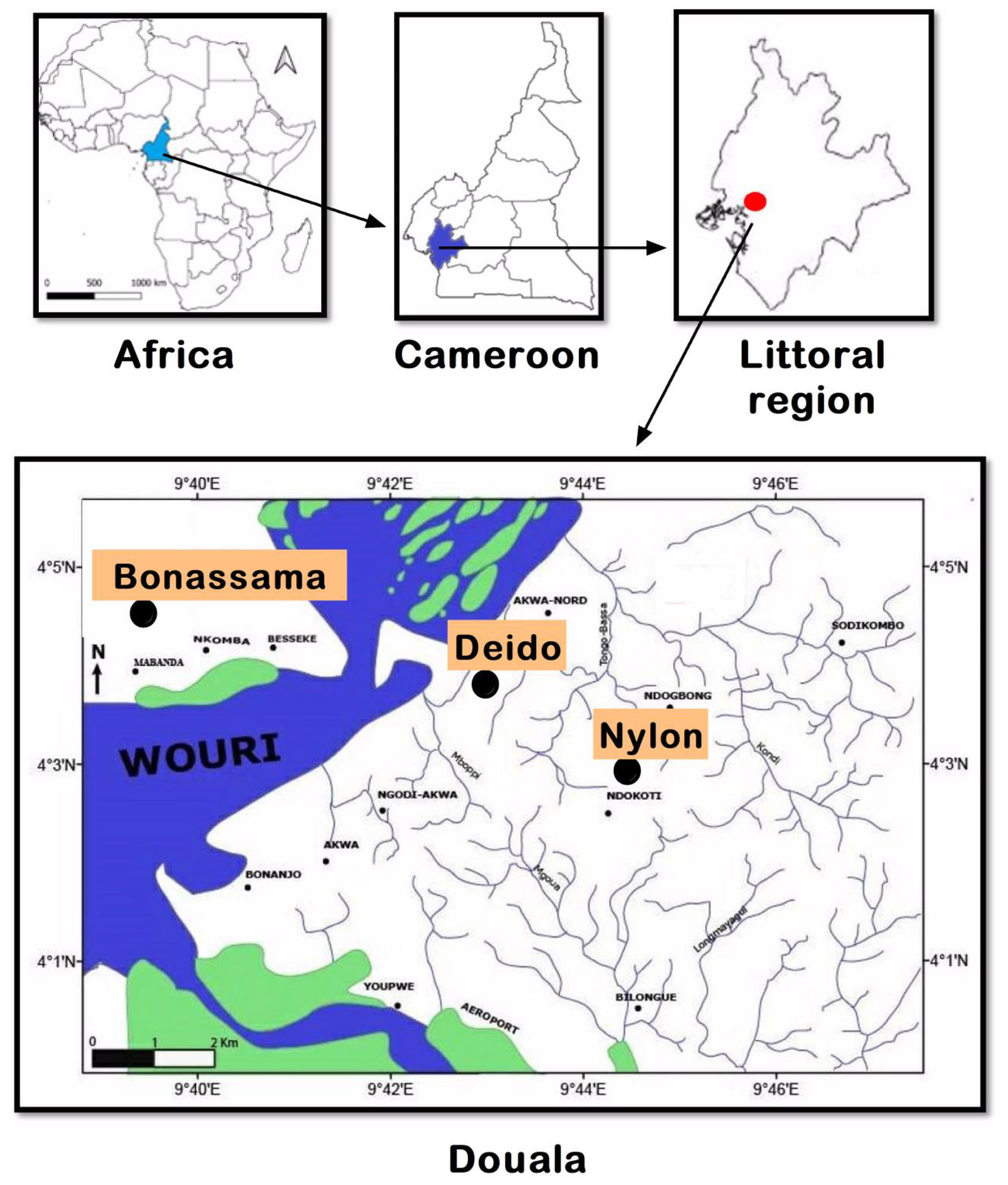
2.1. Study Sites
2.2. Study Design, Study Population, and Sampling Strategy
2.3. Data Collection
2.4. Blood Collection, Hematological, and Parasitological Analyses
2.5. Molecular Analysis: Parasite Detection by PCR and Genotyping of the Pfdhfr, Pfdhps, and Pfk13 Genes by Sequencing
2.6. Statistical Analysis
3. Results
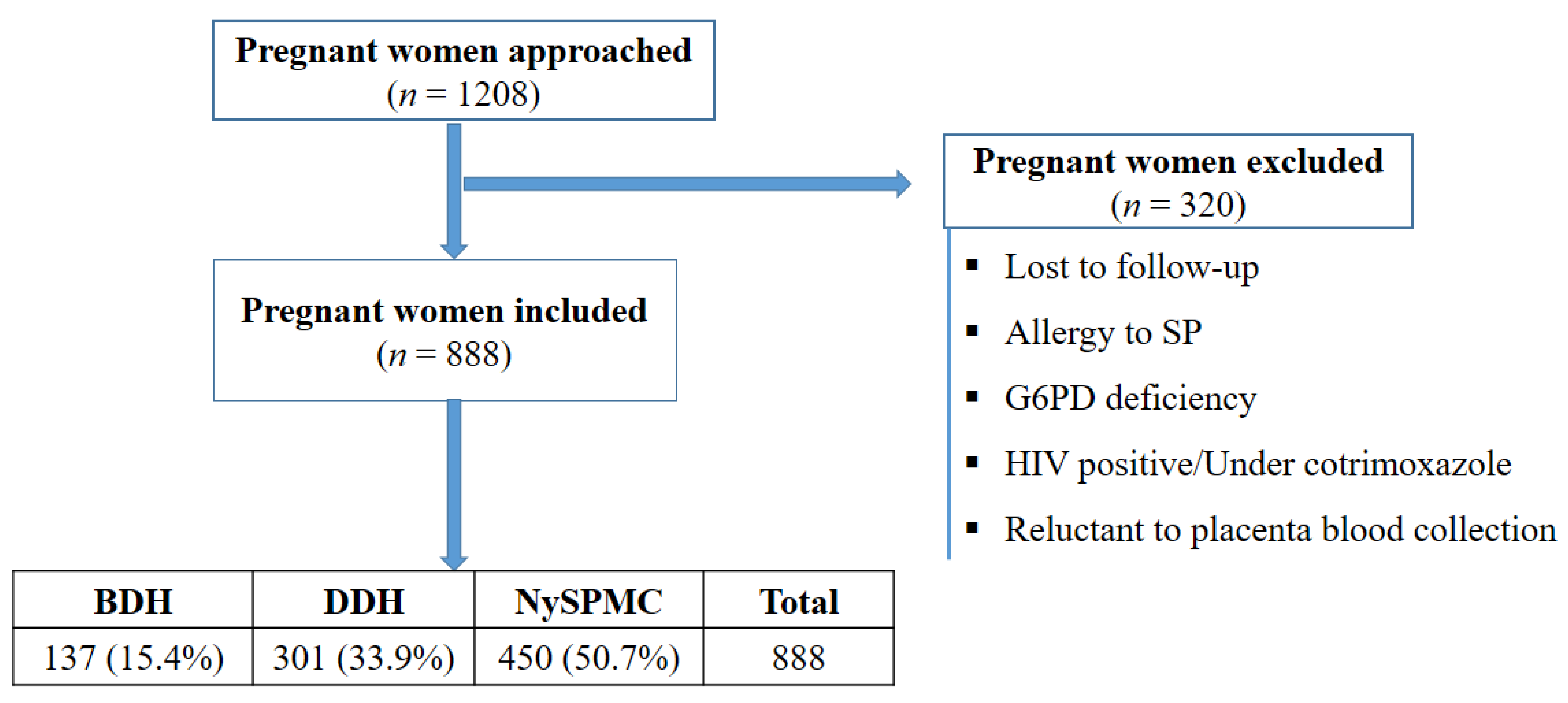
3.1. Pregnant Women Included in the Study
3.2. Sociodemographic and Gynecological Characteristics
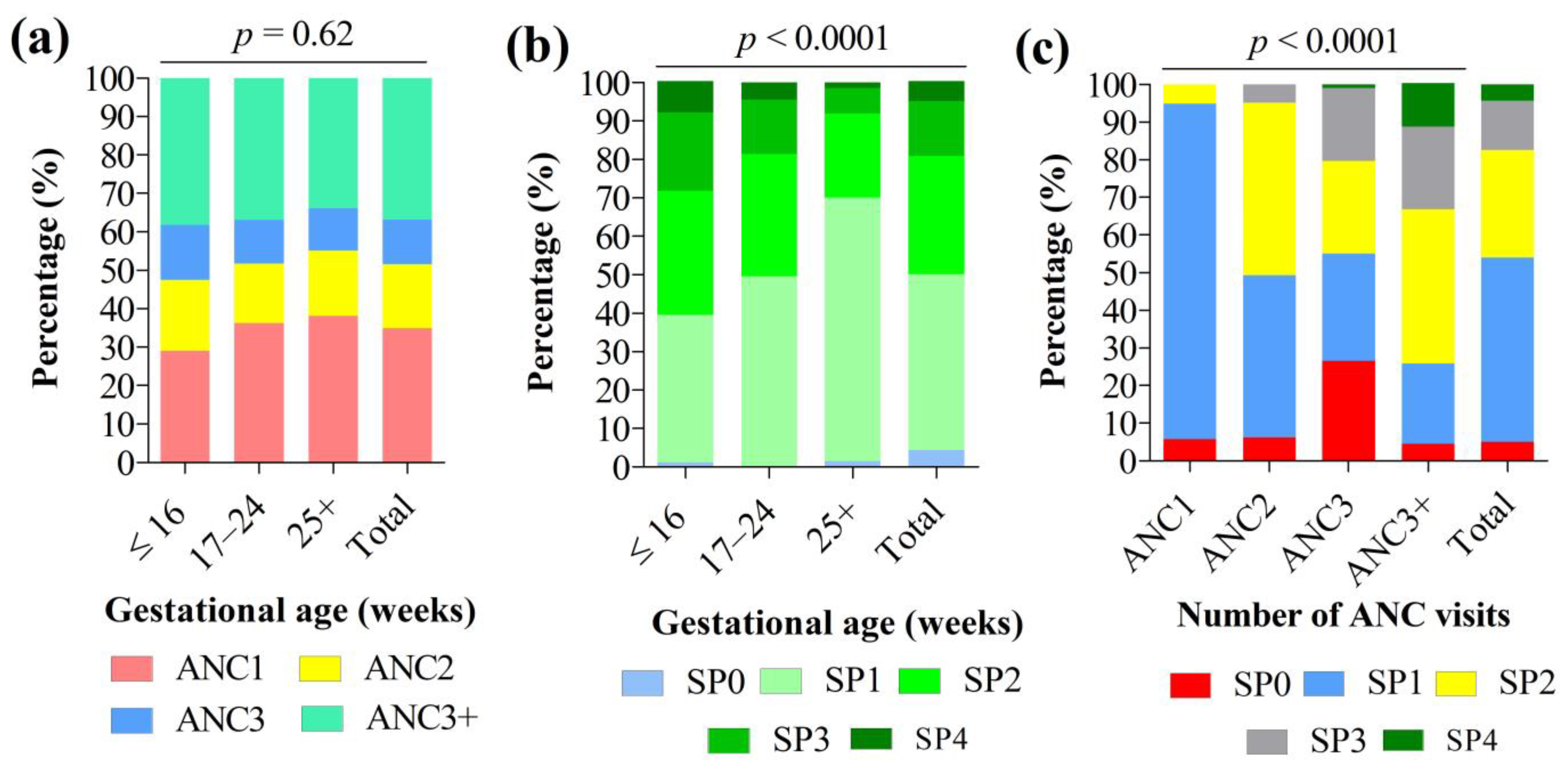
3.3. Antenatal Care Visits and IPTp-SP Coverage
3.4. Factors Associated with Administration of at Least Three Doses of IPTp-SP (IPTp-SP3+) among Women at Delivery
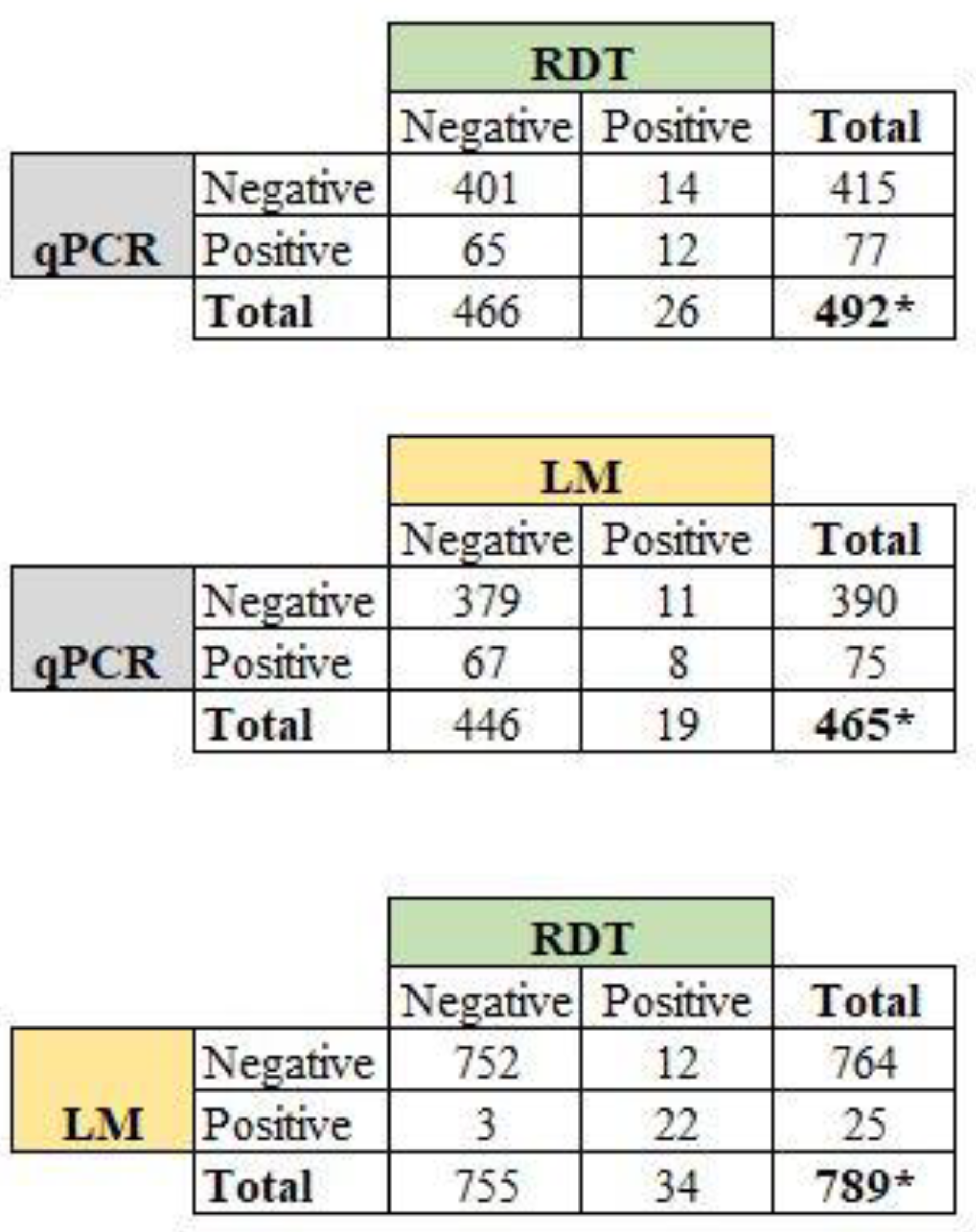
3.5. Prevalence of P. falciparum Malaria and Submicroscopic Infections in Peripheral Blood
3.6. Factors Associated with qPCR-Based P. falciparum Malaria Infection
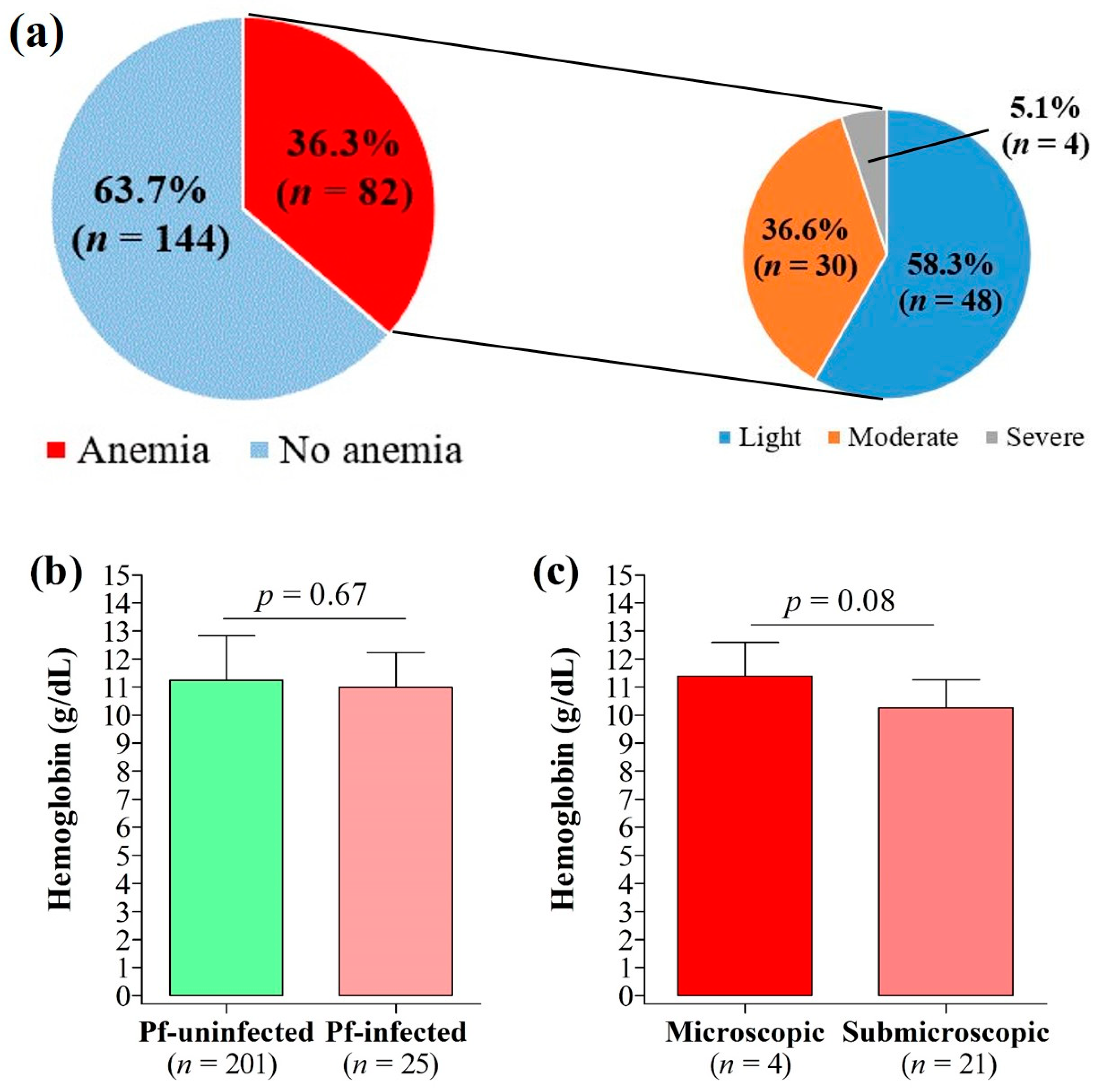
3.7. Anemia and Its Association with Malaria Infection, Submicroscopic Infections, and IPTp-SP
3.8. Impact of SP Dose on Maternal and Birth Outcomes
3.9. Sulfadoxine-Pyrimethamine and Artemisinin Resistance Molecular Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ahmed, M.; Sood, A.; Gupta, J. Toxoplasmosis in pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 255, 44–50. [Google Scholar] [CrossRef]
- Curcio, A.M.; Shekhawat, P.; Reynolds, A.S.; Thakur, K.T. Neurologic infections during pregnancy. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2020; Volume 172, pp. 79–103. [Google Scholar]
- WHO (World Health Organization). World Malaria Report; WHO: Geneva, Switzerland, 2020; Volume WHO/HTM/GM, 299p, ISBN 978-92-4-001579-1. Available online: https://www.who.int/docs/default-source/malaria/world-malaria-reports/9789240015791-eng.pdf (accessed on 5 August 2022).
- Cowman, A.F.; Healer, J.; Marapana, D.; Marsh, K. Malaria: Biology and Disease. Cell 2016, 167, 610–624. [Google Scholar] [CrossRef] [Green Version]
- Ngai, M.; Weckman, A.M.; Erice, C.; McDonald, C.R.; Cahill, L.S.; Sled, J.G.; Kain, K.C. Malaria in pregnancy and adverse birth outcomes: New mechanisms and therapeutic opportunities. Trends Parasitol. 2020, 36, 127–137. [Google Scholar] [CrossRef]
- Saito, M.; Briand, V.; Min, A.M.; McGready, R. Deleterious effects of malaria in pregnancy on the developing fetus: A review on prevention and treatment with antimalarial drugs. Lancet Child Adolesc. Health 2020, 4, 761–774. [Google Scholar] [CrossRef]
- Kayentao, K.; Garner, P.; van Eijk, A.M.; Naidoo, I.; Roper, C.; Mulokozi, A.; MacArthur, J.R.; Luntamo, M.; Ashorn, P.; Doumbou, O.K.; et al. Intermittent preventive therapy for malaria during pregnancy using 2 vs 3 or more doses of sulfadoxine-pyrimethamine and risk of low birth weight in Africa: Systematic review and meta-analysis. JAMA 2013, 309, 594–604. [Google Scholar] [CrossRef] [Green Version]
- ter Kuile, F.O.; van Eijk, A.M.; Filler, S.J. Resistance on the efficacy of intermittent preventive therapy for malaria control during pregnancy. JAMA 2007, 297, 2603–2616. [Google Scholar] [CrossRef]
- Mpogoro, F.J.; Matovelo, D.; Dosani, A.; Ngallaba, S.; Mugono, M.; Mazigo, H.D. Uptake of intermittent preventive treatment with sulphadoxine-pyrimethamine for malaria during pregnancy and pregnancy outcomes: A cross-sectional study in Geita district, North-Western Tanzania. Malar. J. 2014, 13, 455. [Google Scholar] [CrossRef] [Green Version]
- Kayentao, K.; Kodio, M.; Newman, R.D.; Maiga, H.; Doumtabe, D.; Ongoiba, A.; Coulibaly, D.; Salam Keita, A.; Maiga, B.; Mungai, M.; et al. Comparison of intermittent preventive treatment with chemoprophylaxis for the prevention of malaria during pregnancy in Mali. J. Infect. Dis. 2005, 191, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiga, O.M.; Kayentao, K.; Traore, B.T.; Djimde, A.; Traore, B.; Diallo, M.; Ongoiba, A.; Doumtabé, D.; Doumbo, A.; Traoré, M.S. Superiority of 3 over 2 doses of intermittent preventive treatment with sulfadoxine-pyrimethamine for the prevention of malaria during pregnancy in Mali: A randomized controlled trial. Clin. Infect. Dis. 2011, 53, 215–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO (World Health Organization). WHO Policy Brief for the Implementation of Intermittent Preventive Treatment of Malaria in Pregnancy Using Sulfadoxine-Pyrimethamine (IPTp-SP); World Health Organization: Geneva, Switzerland, 2013; Available online: https://www.afro.who.int/sites/default/files/2017-06/iptp-sp-updated-policy-brief-24jan2014.pdf (accessed on 5 August 2022).
- Yoah, A.T.; Fru-Cho, J.; Kah, E.; Njukang, E.; Wirsiy, F.S.; Duamor, C.T.; Mboudou, E.T. Impact of Adherence to a Full Course of Intermittent Preventive Treatment of Malaria in Pregnancy on Pregnancy Outcome in Muyuka Health District: A Cross-Sectional Study. Int. Arch. Public Health Community Med. 2018, 2, 008. [Google Scholar]
- Essiben, F.; Foumane, P.; De Nguefack, M.A.T.; Eko, F.E.; Njotang, P.N.; Enow, R.M.; Mboudou, E.T. Factors associated with the failure of Intermittent Preventive Treatment for malaria among pregnant women in Yaounde. Pan Afr. Med. J. 2016, 23, 152. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4894739/pdf/PAMJ-23-152.pdf (accessed on 15 August 2022). (In French). [PubMed]
- Anchang-Kimbi, J.K.; Kalaji, L.N.; Mbacham, H.F.; Wepnje, G.B.; Apinjoh, T.O.; Ngole Sumbele, I.U.; Dione-Odom, J.; Tita, A.T.N.; Achidi, E.A. Coverage and effectiveness of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) on adverse pregnancy outcomes in the Mount Cameroon area, South West Cameroon. Malar. J. 2020, 19, 100. [Google Scholar] [CrossRef]
- van Eijk, A.M.; Larsen, D.A.; Kayentao, K.; Koshy, G.; Slaughter, D.E.C.; Roper, C.; Okell, L.C.; Desai, M.; Gutman, J.; Khairallah, C.; et al. Effect of Plasmodium falciparum sulfadoxine-pyrimethamine resistance on the effectiveness of intermittent preventive therapy for malaria in pregnancy in Africa: A systematic review and meta-analysis. Lancet Infect. Dis. 2019, 19, 546–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massougbodji, A.; Tubert-Bitter, P.; Briand, V.; Journot, V.; Cot, M.; Escolano, S. Mefloquine versus sulfadoxine–pyrimethamine for intermittent preventive treatment in pregnancy: A joint analysis on efficacy and tolerability. Am. J. Trop. Med. Hyg. 2015, 93, 300–304. [Google Scholar] [CrossRef] [Green Version]
- Roh, M.E.; ter Kuile, F.O.; Rerolle, F.; Glymour, M.M.; Shiboski, S.; Gosling, R.; Gutman, J.; Kakuru, A.; Desai, M.; Kajubi, R.; et al. Overall, anti-malarial, and non-malarial effect of intermittent preventive treatment during pregnancy with sulfadoxine-pyrimethamine on birthweight: A mediation analysis. Lancet Glob. Health 2020, 8, e942–e953. [Google Scholar] [CrossRef]
- Ministry of Public Health, National Observatory of Public Health, World Health Organization. Report of the Monitoring of the 100 Key Health Indicators in Cameroon in 2017. Available online: http://cdnss.minsante.cm/sites/default/files/Fr_Rapport-de-Suivi-des-100-Indicateurs-Cl%C3%A9s-de-Sant%C3%A9-Au-Cameroun-en-2017%20%28Derniere%20version%29.pdf (accessed on 15 August 2022). (In French).
- WHO (World Health Organization). High Burden to High Impact: A Targeted Malaria Response; WHO: Geneva, Switzerland, 2018. [Google Scholar] [CrossRef]
- Anchang-Kimbi, J.K.; Achidi, E.A.; Apinjoh, T.O.; Mugri, R.N.; Chi, H.F.; Tata, R.B.; Nkegoum, B.; Mendimi, J.M.; Sverremark-Ekström, E.; Troye-Blomberg, M. Antenatal care visit attendance, intermittent preventive treatment during pregnancy (IPTp) and malaria parasitaemia at delivery. Malar. J. 2014, 13, 162. [Google Scholar] [CrossRef] [Green Version]
- Babakhanyan, A.; Tutterrow, Y.L.; Bobbili, N.; Salanti, A.; Wey, A.; Fogako, J.; Leke, R.J.; Leke, R.G.F.; Taylor, D.W. Influence of intermittent preventive treatment on antibodies to VAR2CSA in pregnant Cameroonian women. Am. J. Trop. Med. Hyg. 2016, 94, 640–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fokam, E.B.; Ngimuh, L.; Anchang-Kimbi, J.K.; Wanji, S. Assessment of the usage and effectiveness of intermittent preventive treatment and insecticide-treated nets on the indicators of malaria among pregnant women attending antenatal care in the Buea Health District, Cameroon. Malar. J. 2016, 15, 172. [Google Scholar] [CrossRef] [Green Version]
- Leonard, N.; Eric, F.B.; Judith, A.K.K.; Samuel, W. Factors associated to the use of insecticide treated nets and intermittent preventive treatment for malaria control during pregnancy in Cameroon. Arch. Public. Health 2016, 74, 5. [Google Scholar] [CrossRef] [Green Version]
- Diengou, N.H.; Cumber, S.N.; Nkfusai, C.N.; Mbinyui, M.S.; Viyoff, V.Z.; Bede, F.; Akwah, L.; Tsoko-Gwegweni, J.M.; Anchang-Kimbi, J. Factors associated with the uptake of intermittent preventive treatment of malaria in pregnancy in the Bamenda health districts, Cameroon. Pan Afr. Med. J. 2020, 35, 42. [Google Scholar] [CrossRef]
- Tonga, C.; Kimbi, H.K.; Anchang-Kimbi, J.K.; Nyabeyeu, H.N.; Bissemou, Z.B.; Lehman, L.G. Malaria risk factors in women on intermittent preventive treatment at delivery and their effects on pregnancy outcome in Sanaga-Maritime, Cameroon. PLoS ONE 2013, 8, e65876. [Google Scholar] [CrossRef] [Green Version]
- Snow, R.W.; Noor, A.M. Malaria Risk Mapping in Africa: The Historical Context to the Information for Malaria (INFORM) Project; Working Paper in Support of the INFORM Project Funded by the Department for International Development and the Wellcome Trust; Kenya Medical Research Institute (KEMRI): Nairobi, Kenya, 2015. [Google Scholar]
- Antonio-Nkondjio, C.; Ndo, C.; Njiokou, F.; Bigoga, J.D.; Awono-Ambene, P.; Etang, J.; Same Ekobo, A.; Wondji, C.S. Review of malaria situation in Cameroon: Technical viewpoint on challenges and prospects for disease elimination. Parasite Vectors 2019, 12, 501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojom Foko, L.; Kouemo Motse, F.D.; Kamgain Mawabo, L.; Pande, V.; Singh, V. First evidence of local circulation of Plasmodium ovale curtisi and reliability of a malaria rapid diagnostic test among febrile outpatients in Douala, Cameroon. Infect. Genet. Evol. 2021, 91, 104797. [Google Scholar] [CrossRef]
- Ngassa Mbenda, H.G.; Gouado, I.; Das, A. An additional observation of Plasmodium vivax malaria infection in Duffy-negative individuals from Cameroon. J. Infect. Dev. Ctries. 2016, 10, 682–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Public Health. 2012 Activity Report of the National Malaria Control Program. Yaoundé: 2012. Available online: https://pnlp.cm/wp-content/uploads/2020/05/Rapport-annuel-PNLP-2012-du-24-07-2013.pdf (accessed on 5 August 2022). (In French).
- WHO (World Health Organization). Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Geneva. 2011. 6p. Available online: https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?sequence=22&isAllowed=y (accessed on 15 August 2022).
- WHO. Malaria Rapid Diagnostic Test Performance: Results of WHO Product Testing of Malaria RDTs: Round 8 (2016–2018); WHO: Geneva, Switzerland, 2018; Volume 8, Available online: https://www.who.int/publications/i/item/9789241514965 (accessed on 5 August 2022).
- Cheesbrough, M. District Laboratory Practice in Tropical Countries; Part 2: Se; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Trape, J.-F. Rapid evaluation of malaria parasite density and standardization of thick smear examination for epidemiological investigations. Trans. R. Soc. Trop. Med. Hyg. 1985, 79, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Plowe, C.V.; Djimde, A.; Bouare, M.; Doumbo, O.; Wellems, T.E. Pyrimethamine and proguanil resistance-conferring mutations in Plasmodium falciparum dihydrofolate reductase: Polymerase chain reaction methods for surveillance in Africa. Am. J. Trop. Med. Hyg. 1995, 52, 565–568. Available online: https://www.ajtmh.org/view/journals/tpmd/52/6/article-p565.xml (accessed on 5 August 2022). [CrossRef] [PubMed]
- Diallo, A.; Ndam, N.T.; Moussiliou, A.; Dos Santos, S.; Ndonky, A.; Borderon, M.; Oliveau, S.; Lalou, R.; Le Hesran, J.Y. Asymptomatic carriage of plasmodium in urban Dakar: The risk of malaria should not be underestimated. PLoS ONE 2012, 7, e31100. [Google Scholar] [CrossRef] [Green Version]
- Arya, A.; Kojom Foko, L.P.; Chaudhry, S.; Sharma, A.; Singh, V. Artemisinin-based combination therapy (ACT) and drug resistance molecular markers: A systematic review of clinical studies from two malaria endemic regions–India and sub-Saharan Africa. Int. J. Parasitol. Drugs Drug Resist. 2021, 15, 43–56. [Google Scholar] [CrossRef]
- Pearce, R.J.; Drakeley, C.; Chandramohan, D.; Mosha, F.; Roper, C. Molecular determination of point mutation haplotypes in the dihydrofolate reductase and dihydropteroate synthase of Plasmodium falciparum in three districts of Northern Tanzania. Antimicrob. Agents Chemother. 2003, 47, 1347–1354. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC152520/pdf/0879.pdf (accessed on 5 August 2022). [CrossRef] [Green Version]
- Goodstadt, L.; Ponting, C.P. CHROMA: Consensus-based colouring of multiple alignments for publication. Bioinformatics 2001, 17, 845–846. [Google Scholar] [CrossRef] [Green Version]
- Edgar, R.C. MUSCLE: Multiple sequence alignment with high accuracy and high throughput. Nucleic Acids Res. 2004, 32, 1792–1797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akpa, C.O.; Akinyemi, J.O.; Umeokonkwo, C.D.; Bamgboye, E.A.; Dahiru, T.; Adebowale, A.S.; Oyeneye Ajayi, I. Uptake of intermittent preventive treatment for malaria in pregnancy among women in selected communities of Ebonyi State, Nigeria. BMC Pregnancy Childbirth 2019, 19, 457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okethwangu, D.; Opigo, J.; Atugonza, S.; Kizza, C.T.; Nabatanzi, M.; Biribawa, C.; Kyabayinze, D.; Ario, A.R. Factors associated with uptake of optimal doses of intermittent preventive treatment for malaria among pregnant women in Uganda: Analysis of data from the Uganda Demographic and Health Survey, 2016. Malar. J. 2019, 18, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pons-Duran, C.; Llach, M.; Sacoor, C.; Sanz, S.; Macete, E.; Arikpo, I.; Ramirez, M.; Meremikwu, M.; Ndombo Ndombe, D.; Mendes, S.; et al. Coverage of intermittent preventive treatment of malaria in pregnancy in four sub-Saharan countries: Findings from household surveys. Int. J. Epidemiol. 2021, 50, 550–559. [Google Scholar] [CrossRef]
- Mushi, V.; Mbotwa, C.H.; Zacharia, A.; Ambrose, T.; Moshi, F.V. Predictors for the uptake of optimal doses of sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria during pregnancy in Tanzania: Further analysis of the data of the 2015–2016 Tanzania demographic and health survey and malaria indicators. Malar. J. 2021, 20, 75. [Google Scholar] [CrossRef]
- Kojom Foko, L.P.; Lehman, L.G. Knowledge and beliefs towards malaria and associated factors among residents of the town of Douala, Cameroon. Arch. Curr. Res. Int. 2018, 14, 1–17. [Google Scholar] [CrossRef]
- Mbohou Nchetnkou, C.; Kojom Foko, L.P.; Lehman, L.G. Knowledge, attitude, and practices towards malaria among employees from enterprises in the town of Douala, Cameroon. BioMed Res. Int. 2020, 2020, 8652084. [Google Scholar] [CrossRef]
- Azizi, S.C. Uptake of intermittent preventive treatment for malaria during pregnancy with Sulphadoxine-Pyrimethamine in Malawi after adoption of updated World Health Organization policy: An analysis of demographic and health survey 2015–2016. BMC Public Health 2020, 20, 335. [Google Scholar] [CrossRef]
- Wafula, S.T.; Mendoza, H.; Nalugya, A.; Musoke, D.; Waiswa, P. Determinants of uptake of malaria preventive interventions among pregnant women in eastern Uganda. Malar. J. 2021, 20, 5. [Google Scholar] [CrossRef]
- Lehman, L.G.; Kojom Foko, L.; Tonga, C.; Nyabeyeu, H.; Eboumbou, E.C.; Kouodjip Nono, L.; Kangam, L.; Ngapmen, A.L.; Assomo Ndemba, P.B.; Matip, I.; et al. Epidemiology of malaria using LED fluorescence microscopy among schoolchildren in Douala, Cameroon. Int. J. Trop. Dis. Health 2018, 29, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Unger, H.W.; Rosanas-Urgell, A.; Robinson, L.J.; Ome-Kaius, M.; Jally, S.; Umbers, A.J.; Pomat, W.; Mueller, I.; Kattenberg, E.; Rogerson, S.J. Microscopic and submicroscopic Plasmodium falciparum infection, maternal anaemia and adverse pregnancy outcomes in Papua New Guinea: A cohort study. Malar. J. 2019, 18, 302. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Bharti, P.K.; Singh, M.P.; Singh, R.; Yeboah-Antwi, K.; Desai, M.; Udhayakumar, V.; Muniyandi, M.; Hamer, D.H.; Wylie, B.J. What is the burden of submicroscopic malaria in pregnancy in central India? Pathog. Glob. Health 2015, 109, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Cohee, L.M.; Kalilani-Phiri, L.; Boudova, S.; Joshi, S.; Mukadam, R.; Seydel, K.B.; Mawindo, P.; Thesing, P.; Kamiza, S.; Makwakwa, K.; et al. Submicroscopic malaria infection during pregnancy and the impact of intermittent preventive treatment. Malar. J. 2014, 13, 274. [Google Scholar] [CrossRef] [Green Version]
- Elbadry, M.A.; Tagliamonte, M.S.; Raccurt, C.P.; Lemoine, J.F.; Existe, A.; Boncy, J.; Weppelmann, T.A.; Dame, J.B.; Okech, B.A. Submicroscopic malaria infections in pregnant women from six departments in Haiti. Trop. Med. Int. Health 2017, 22, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Ndam, N.T.; Tornyigah, B.; Dossou, A.Y.; Escriou, G.; Nielsen, M.A.; Salanti, A.; Issifou, S.; Massougbodji, A.; Chippaux, J.P.; Deloron, P. Persistent Plasmodium falciparum infection in women with an intent to become pregnant as a risk factor for pregnancy-associated malaria. Clin. Infect. Dis. 2018, 67, 1890–1896. [Google Scholar] [CrossRef]
- Sumbele, I.U.N.; Teh, R.N.; Nkeudem, G.A.; Mekachie, S.S.; Moyeh, M.N.; Shey, R.A.; Mounchili Shintouo, C.; Mbigha Ghogomu, S.; El-Saber Batiha, G.; Alkazmi, L.; et al. Asymptomatic and sub-microscopic Plasmodium falciparum infection in children in the Mount Cameroon area : A cross-sectional study on altitudinal influence, haematological parameters and risk factors. Malar. J. 2021, 20, 382. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, C.; Slater, H.; Nash, R.; Bousema, T.; Drakeley, C.; Ghani, A.C.; Ghani, A.V.; Okell, L.C. Global patterns of submicroscopic Plasmodium falciparum malaria infection: Insights from a systematic review and meta-analysis of population surveys. Lancet Microb. 2021, 2, e366–e374. [Google Scholar] [CrossRef] [PubMed]
- Anto, F.; Agongo, I.H.; Asoala, V.; Awini, E.; Oduro, A.R. Intermittent preventive treatment of malaria in pregnancy: Assessment of the sulfadoxine-pyrimethamine three-dose policy on birth outcomes in rural Northern Ghana. J. Trop. Med. 2019, 2019, 6712685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikomangwa, W.P.; Minzi, O.; Mutagonda, R.; Baraka, V.; Mlugu, E.M.; Aklillu, E.; Kamuhabwa, A.A.R. Effect of sulfadoxine-pyrimethamine doses for prevention of malaria during pregnancy in hypoendemic area in Tanzania. Malar. J. 2020, 19, 160. [Google Scholar] [CrossRef] [Green Version]
- Amimo, F.; Lambert, B.; Magit, A.; Sacarlal, J.; Hashizume, M.; Shibuya, K. Plasmodium falciparum resistance to sulfadoxine-pyrimethamine in Africa: A systematic analysis of national trends. BMJ Glob. Health 2020, 5, e003217. [Google Scholar] [CrossRef] [PubMed]
- Chauvin, P.; Menard, S.; Iriart, X.; Nsango, S.E.; Tchioffo, M.T.; Abate, L.; Awono-Ambene, P.H.; Morlais, I.; Berry, A. Prevalence of Plasmodium falciparum parasites resistant to sulfadoxine/pyrimethamine in pregnant women in Yaoundé Cameroon: Emergence of highly resistant pfdhfr/pfdhps alleles. J. Antimicrob. Chemother. 2015, 70, 2566–2571. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, R.; Chhibber-Goel, J.; Verma, I.; Gopinathan, S.; Parvez, S.; Sharma, A. Geographical spread and structural basis of sulfadoxine-pyrimethamine drug-resistant malaria parasites. Int. J. Parasitol. 2021, 51, 505–525. [Google Scholar] [CrossRef]
- Niba, P.T.N.; Nji, A.M.; Evehe, M.S.; Ali, I.M.; Netongo, P.M.; Ngwafor, R.; Moyeh, M.N.; Ngum Ngum, L.; Ndum, O.E.; Acho, F.A.; et al. Drug resistance markers within an evolving efficacy of anti-malarial drugs in Cameroon: A systematic review and meta-analysis (1998–2020). Malar. J. 2021, 20, 32. [Google Scholar] [CrossRef]
- Amenga-Etego, L.N.; Asoala, V.; Agongo, G.; Jacob, C.; Goncalves, S.; Awandare, G.A.; Rockett, K.A.; Kwiatkowski, D. Temporal evolution of sulfadoxine-pyrimethamine resistance genotypes and genetic diversity in response to a decade of increased interventions against Plasmodium falciparum in northern Ghana. Malar. J. 2021, 20, 152. [Google Scholar] [CrossRef]
- Mama, A.; Ahiabor, C.; Tornyigah, B.; Frempong, N.A.; Kusi, K.A.; Adu, B.; Courtin, D.; Houzé, S.; Deloron, P.; Ofori, M.F.; et al. Intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine and parasite resistance: Cross-sectional surveys from antenatal care visit and delivery in rural Ghana. Malar. J. 2022, 21, 107. [Google Scholar] [CrossRef]
- Naidoo, I.; Roper, C. Mapping ‘partially resistant’, ‘fully resistant’, and ‘super resistant’ malaria. Trends Parasitol. 2013, 29, 505–515. [Google Scholar] [CrossRef]
- Zhao, L.; Pi, L.; Qin, Y.; Lu, Y.; Zeng, W.; Xiang, Z.; Qin, P.; Chen, X.; Li, C.; Zhang, Y.; et al. Widespread resistance mutations to sulfadoxine-pyrimethamine in malaria parasites imported to China from Central and Western Africa. Int. J. Parasitol. Drugs Drug Resist. 2020, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bwire, G.M.; Mikomangwa, W.P.; Kilonzi, M. Occurrence of septuple and elevated Pfdhfr-Pfdhps quintuple mutations in a general population threatens the use of sulfadoxine-pyrimethamine for malaria prevention during pregnancy in eastern-coast of Tanzania. BMC Infect. Dis. 2020, 20, 530. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Cheng, W.; Yao, Y.; Tan, H.; Wu, K.; Li, J. Molecular surveillance of anti-malarial resistance Pfdhfr and Pfdhps polymorphisms in African and Southeast Asia Plasmodium falciparum imported parasites to Wuhan, China. Malar. J. 2020, 19, 434. [Google Scholar] [CrossRef] [PubMed]
- Voumbo-Matoumona, D.F.; Kouna, L.C.; Madamet, M.; Maghendji-Nzondo, S.; Pradines, B.; Lekana-Douki, J.B. Prevalence of Plasmodium falciparum antimalarial drug resistance genes in Southeastern Gabon from 2011 to 2014. Infect. Drug Resist. 2018, 11, 1329–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarah-Matio, E.M.; Guillochon, E.; Nsango, S.E.; Abate, L.; Ngou, C.M.; Bouopda, G.A.; Feufack-Donfack, L.B.; Bayibéki, A.N.; Tchioffo Tsapi, M.; Talman, A.; et al. Genetic Diversity of Plasmodium falciparum and Distribution of Antimalarial Drug Resistance Mutations in Symptomatic and Asymptomatic Infections. Antimicrob. Agents Chemother. 2022, 66, e0018822. [Google Scholar] [CrossRef] [PubMed]
- Bushman, M.; Morton, L.; Duah, N.; Quashie, N.; Abuaku, B.; Koram, K.A.; Dimbu, P.R.; Plucinski, M.; Gutman, J.; Lyaruu, P.; et al. Within-host competition and drug resistance in the human malaria parasite Plasmodium falciparum. Proc. Biol. Sci. 2016, 283, 20153038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldh, M.; Hammar, U.; Arnot, D.; Beck, H.P.; Garcia, A.; Liljander, A.; Mercereau-Puijalon, O.; Migot-Nabias, F.; Mueller, I.; Ntoumi, F.; et al. Multiplicity of Asymptomatic Plasmodium falciparum Infections and Risk of Clinical Malaria: A Systematic Review and Pooled Analysis of Individual Participant Data. J. Infect. Dis. 2020, 221, 775–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Bonassama | Deido | St Paul | Total | p-Value |
|---|---|---|---|---|---|
| Age groups | |||||
| [14–17[ | 0 (0.0) | 4 (1.4) | 3 (0.7) | 7 (0.9) | 0.14 |
| [17–22[ | 15 (31.2) | 38 (13.0) | 56 (12.5) | 109 (13.8) | |
| [22–26[ | 11 (22.9) | 84 (28.7) | 126 (28.1) | 221 (28.0) | |
| [26–31[ | 13 (27.1) | 95 (32.3) | 151 (33.7) | 259 (32.9) | |
| [31–36[ | 6 (12.5) | 51 (17.4) | 82 (18.3) | 139 (17.6) | |
| ≥36 | 3 (6.3) | 21 (7.2) | 30 (6.7) | 54 (6.8) | |
| Level of education | |||||
| None | 1 (0.8) | 0 (0.0) | 3 (0.7) | 4 (0.5) | 0.005 * |
| Primary | 19 (14.3) | 32 (10.7) | 69 (15.4) | 120 (13.6) | |
| Secondary | 92 (69.2) | 169 (56.3) | 264 (58.8) | 525 (59.5) | |
| University | 21 (15.7) | 99 (33.0) | 113 (25.1) | 233 (26.4) | |
| Marital status | |||||
| Single | 74 (60.2) | 208 (69.3) | 319 (71.1) | 601 (68.9) | 0.06 |
| Married | 49 (39.8) | 92 (30.7) | 130 (28.9) | 271 (31.1) | |
| Occupation | |||||
| Agent | 12 (8.9) | 39 (13.2) | 65 (14.7) | 116 (13.3) | 0.18 |
| Top manager | 12 (8.9) | 29 (9.8) | 27 (6.1) | 68 (7.8) | |
| Student | 31 (23.0) | 88 (29.8) | 103 (23.4) | 222 (25.5) | |
| Housewife | 36 (26.7) | 70 (23.7) | 120 (27.2) | 226 (26.0) | |
| Unemployed | 44 (32.5) | 69 (23.5) | 126 (28.6) | 239 (27.4) | |
| Health-related expenses | |||||
| Insurance | 0 (0.0) | 1 (0.3) | 1 (0.2) | 2 (0.2) | 1 |
| Insurance + Personal | 1 (0.8) | 0 (0.0) | 0 (0.0) | 1 (0.1) | |
| Personal | 131 (99.2) | 299 (99.7) | 448 (99.8) | 878 (99.7) | |
| IPTp-SP during previous pregnancies | |||||
| No | 40 (29.6) | 68 (22.6) | 155 (34.6) | 263 (29.8) | 0.002 * |
| Yes | 95 (70.4) | 233 (77.4) | 293 (65.4) | 621 (70.2) | |
| Parity | |||||
| Primiparous | 45 (33.8) | 131 (43.5) | 140 (31.3) | 316 (35.8) | 0.006 * |
| Secundiparous | 47 (35.3) | 91 (30.2) | 145 (32.4) | 283 (32.1) | |
| Multiparous | 41 (30.9) | 79 (26.3)0 | 163 (36.3) | 283 (32.1) | |
| Number of children | |||||
| 0 | 45 (33.9) | 131 (43.6) | 140 (31.3) | 316 (35.8) | 0.01 * |
| 1 | 47 (35.4) | 91 (30.2) | 145 (32.4) | 283 (32.1) | |
| 2 | 15 (11.2) | 45 (14.9) | 76 (16.9) | 136 (15.4) | |
| 3 | 20 (15.0) | 18 (6.0) | 57 (12.7) | 95 (10.8) | |
| 4 | 0 (0.0) | 0 (0.0) | 1 (0.2) | 1 (0.1) | |
| ≥4 | 6 (4.5) | 16 (5.3) | 29 (6.5) | 51 (5.8) | |
| Number of abortion events | |||||
| 0 | 78 (58.6) | 175 (58.4) | 269 (60.4) | 522 (59.4) | 0.04 * |
| 1 | 32 (24.1) | 97 (32.3) | 113 (25.3) | 242 (27.5) | |
| 2 | 14 (10.5) | 18 (6.0) | 41 (9.2) | 73 (8.3) | |
| 3 | 8 (6.0) | 4 (1.3) | 18 (4.0) | 30 (3.4) | |
| 4 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| ≥4 | 1 (0.8) | 6 (2.0) | 5 (1.1) | 12 (1.4) |
| Variables | N | n (%) | rOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Health facility | ||||||
| Bonassama | 11 | 2 (18.2%) | 1 | 1 | ||
| Deido | 29 | 10 (34.5%) | 2.37 (0.43–13.13) | 0.32 | 1.06 (0.24–4.73) | 0.93 |
| St Paul | 108 | 16 (14.8%) | 0.70 (0.15–3.96) | 0.76 | 0.60 (0.13–2.71) | 0.51 |
| Age (years old) | - | - | 1.06 (0.98–1.15) | 0.17 | 1.19 (1.02–1.40) | 0.03 * |
| Level of education | ||||||
| Primary | 19 | 2 (10.5%) | 1 | 1 | ||
| Secondary | 78 | 16 (20.5%) | 2.19 (0.45–10.49) | 0.32 | 21.61 (1.15–406.46) | 0.007 * |
| University | 51 | 10 (19.6%) | 2.07 (0.41–10.48) | 0.37 | 6.30 (2.37–124.38) | 0.002 * |
| Marital status | ||||||
| Single | 91 | 17 (18.7%) | 1 | 1 | ||
| Married | 57 | 11 (19.3%) | 1.04 (0.45–2.42) | 0.92 | 0.29 (0.07–1.19) | 0.08 |
| Parity | ||||||
| Primiparous | 313 | 59 (18.8%) | 1 | 1 | ||
| Secundiparous | 278 | 47 (16.9%) | 0.88 (0.57–1.34) | 0.54 | 0.38 (0.09–1.62) | 0.19 |
| Multiparous | 279 | 47 (16.8%) | 0.87 (0.57–1.33) | 0.53 | 0.28 (0.04–1.74) | 0.17 |
| Number of ANC | ||||||
| 1 | 293 | 6 (2.0%) | 1 | 1 | ||
| 2 | 142 | 7 (4.9%) | 2.48 (0.82–7.52) | 0.11 | 1.61 (0.35–7.44) | 0.54 |
| 3 | 100 | 29 (29.0%) | 19.54 (7.81–48.86) | <0.0001 * | 19.44 (6.36–59.43) | <0.0001 * |
| 4+ | 313 | 104 (33.2%) | 23.80 (10.25–55.25) | <0.0001 * | 23.82 (2.01–282.25) | 0.01* |
| No | 123 | 20 (16.3%) | 1 | 1 | ||
| Yes | 25 | 8 (32.0%) | 2.42 (0.92–6.38) | 0.07 | 2.91 (1.01–11.91) | 0.04 * |
| History of malaria | ||||||
| No | 106 | 20 (18.9%) | 1 | 1 | ||
| Yes | 40 | 8 (20.0%) | 1.08 (0.43–2.68) | 0.87 | 1.33 (0.40–4.39) | 0.63 |
| Malaria prevention plan | ||||||
| No | 20 | 2 (10.0%) | 1 | 1 | ||
| Yes | 128 | 26 (20.3%) | 2.29 (0.50–10.52) | 0.28 | 6.10 (0.55–67.58) | 0.14 |
| Implementation of malaria prevention plan | ||||||
| No | 34 | 8 (23.5%) | 1 | 1 | ||
| Yes | 110 | 20 (18.2%) | 0.72 (0.29–1.82) | 0.49 | 0.09 (0.02–0.52) | 0.007 * |
| Previous administration of IPTp-SP | ||||||
| No | 37 | 7 (18.9%) | 1 | 1 | ||
| Yes | 111 | 21 (18.9%) | 1.00 (0.39–2.59) | 0.99 | 1.04 (0.23–4.80) | 0.95 |
| Timing of the first ANC † | ||||||
| ≤16 weeks | 30 | 7 (23.3%) | 1 | 1 | ||
| 17–24 weeks | 91 | 19 (20.9%) | 0.87 (0.32–2.32) | 0.77 | 0.38 (0.09–1.50) | 0.16 |
| 25+ weeks | 24 | 2 (8.3%) | 0.30 (0.06–1.60) | 0.15 | 0.10 (0.01–0.96) | 0.04 * |
| Variables | N μ | n # (%) | rOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Health facility | ||||||
| Bonassama | 137 | 4 (2.9%) | 1 | 1 | ||
| Deido | 301 | 25 (8.3%) | 3.01 (1.03–8.83) | 0.04 * | 3.03 (1.02–8.85) | 0.03 * |
| St Paul | 450 | 52 (11.6%) | 4.34 (1.54–12.24) | 0.005 * | 4.37 (1.52–12.27) | 0.003 * |
| Age groups | ||||||
| [14–17[ | 7 | 2 (28.6%) | 1 | 1 | ||
| [17–22[ | 109 | 16 (14.7%) | 0.43 (0.08–2.41) | 0.34 | 0.60 (0.04–8.81) | 0.71 |
| [22–26[ | 221 | 19 (8.6%) | 0.24 (0.04–1.30) | 0.09 | 0.38 (0.03–5.61) | 0.48 |
| [26–31[ | 259 | 20 (7.7%) | 0.21 (0.04–1.15) | 0.07 | 0.33 (0.02–4.77) | 0.41 |
| [31–36[ | 139 | 14 (10.1%) | 0.28 (0.05–1.58) | 0.15 | 0.40 (0.03–6.41) | 0.52 |
| ≥36 | 54 | 8 (14.8%) | 0.43 (0.07–2.64) | 0.37 | 1.61 (0.09–27.90) | 0.74 |
| Marital status | ||||||
| Single | 601 | 59 (9.8%) | 1 | 1 | ||
| Married | 271 | 22 (8.1%) | 0.81 (0.49–1.36) | 0.42 | 0.68 (0.34–1.37) | 0.28 |
| Occupation | ||||||
| Agent | 116 | 13 (11.2%) | 1 | 1 | ||
| Top manager | 68 | 3 (4.4%) | 0.37 (0.10–1.33) | 0.12 | 0.15 (0.02–1.33) | 0.09 |
| Student | 222 | 23 (10.4%) | 1.05 (0.52–2.11) | 0.89 | 0.81 (0.31–2.16) | 0.68 |
| Housewife | 226 | 14 (6.2%) | 0.92 (0.45–1.88) | 0.81 | 0.50 (0.20–1.30) | 0.16 |
| Unemployed | 239 | 28 (11.7%) | 0.52 (0.24–1.15) | 0.11 | 0.92 (0.38–2.21) | 0.84 |
| Parity | ||||||
| Primiparous | 316 | 30 (9.5%) | 1 | 1 | ||
| Secundiparous | 283 | 26 (9.2%) | 0.96 (0.56–1.67) | 0.89 | 1.05 (0.50–2.23) | 0.89 |
| Multiparous | 283 | 25 (8.8%) | 0.92 (0.53–1.61) | 0.78 | 0.86 (0.35–2.12) | 0.74 |
| Number of ANC | ||||||
| 1 | 300 | 29 (9.7%) | 1 | 1 | ||
| 2 | 143 | 11 (7.7%) | 0.78 (0.38–1.61) | 0.49 | 1.08 (0.37–3.13) | 0.89 |
| 3 | 100 | 12 (12.0%) | 1.27 (0.62–2.60) | 0.51 | 2.36 (0.89–6.22) | 0.08 |
| 4+ | 317 | 29 (9.1%) | 0.94 (0.55–1.62) | 0.83 | 1.62 (0.71–3.69) | 0.25 |
| Received education on malaria | ||||||
| No | 574 | 55 (9.6%) | 1 | 1 | ||
| Yes | 304 | 26 (8.6%) | 0.88 (0.54–1.44) | 0.61 | 1.23 (0.63–2.40) | 0.54 |
| Knowledge of route of transmission | ||||||
| No | 167 | 19 (11.4%) | 1 | 1 | ||
| Yes | 479 | 49 (10.2%) | 0.89 (0.51–1.56) | 0.68 | 1.35 (0.69–2.63) | 0.38 |
| Knowledge of IPTp-SP | ||||||
| No | 707 | 76 (10.7%) | 1 | 1 | ||
| Yes | 178 | 5 (2.8%) | 0.24 (0.09–0.60) | 0.002 * | 0.30 (0.07–1.34) | 0.11 |
| History of malaria | ||||||
| No | 659 | 52 (7.9%) | 1 | 1 | ||
| Yes | 202 | 29 (14.4%) | 1.96 (1.21–3.18) | 0.006 * | 2.01 (1.08–3.73) | 0.02 * |
| Presence of water collections around the house | ||||||
| No | 403 | 31 (7.7%) | 1 | 1 | ||
| Yes | 479 | 50 (10.4%) | 1.40 (0.88–2.24) | 0.16 | 1.53 (0.72–3.25) | 0.26 |
| Presence of swamp around the house | ||||||
| No | 496 | 39 (7.9%) | 1 | 1 | ||
| Yes | 386 | 42 (10.9%) | 1.43 (0.91–2.26) | 0.13 | 0.94 (0.45–1.94) | 0.86 |
| Outside Douala in the last 6 days | ||||||
| No | 809 | 74 (9.1%) | 1 | 1 | ||
| Yes | 68 | 7 (10.3%) | 1.14 (0.50–2.58) | 0.75 | 1.26 (0.45–3.51) | 0.65 |
| Implementation of malaria prevention plan | ||||||
| No | 196 | 22 (11.2%) | 1 | 1 | ||
| Yes | 595 | 50 (8.4%) | 0.73 (0.43–1.23) | 0.23 | 0.69 (0.30–1.57) | 0.37 |
| Previous administration of IPTp-SP | ||||||
| No | 263 | 28 (10.6%) | 1 | 1 | ||
| Yes | 621 | 53 (8.5%) | 0.78 (0.48–1.27) | 0.32 | 0.99 (0.39–2.50) | 0.98 |
| Utilization of ITNs | ||||||
| No | 247 | 28 (11.3%) | 1 | 1 | ||
| Yes | 634 | 53 (8.4%) | 0.71 (0.44–1.16) | 0.17 | 0.85 (0.35–2.06) | 0.71 |
| Indoor residual spraying | ||||||
| No | 424 | 45 (10.6%) | 1 | 1 | ||
| Yes | 459 | 36 (7.8%) | 0.72 (0.45–1.14) | 0.16 | 0.53 (0.30–0.95) | 0.03 * |
| Aeration of sleeping place | ||||||
| No | 713 | 65 (9.1%) | 1 | 1 | ||
| Yes | 161 | 16 (9.9%) | 1.10 (0.62–1.97) | 0.75 | 1.47 (0.74–2.92) | 0.27 |
| IPTp-SP Doses | ||||||
|---|---|---|---|---|---|---|
| Variables | 0 | 1 | 2 | 3 | 3+ | p-Value |
| Maternal infection ‡ | ||||||
| Primiparous | 1 (6.3%) | 18 (12.2%) | 7 (7.8%) | 3 (6.4%) | 1 (8.3%) | 0.69 |
| Secundiparous | 4 (33.3%) | 9 (6.5%) | 10 (12.5%) | 2 (5.9%) | 1 (7.7%) | 0.02 * |
| Multiparous | 4 (25%) | 17 (12.4%) | 3 (3.0%) | 1 (2.9%) | 0 (0.0%) | 0.01 * |
| Overall | 9 (20%) | 44 (10.3%) | 20 (8.0%) | 6 (5.2%) | 2 (5.3%) | 0.03 * |
| Maternal anemia | ||||||
| Primiparous | 3 (75%) | 12 (41.4%) | 11 (37.9%) | 4 (40%) | 1 (33.3%) | 0.68 |
| Secundiparous | 0 (0%) | 8 (27.6%) | 6 (28.6%) | 2 (33.3%) | 1 (50.0%) | 0.88 |
| Multiparous | 2 (33.3%) | 14 (37.8%) | 11 (40.7%) | 4 (40%) | 1 (16.7%) | 0.22 |
| Overall | 6 (40%) | 34 (35.8%) | 28 (36.4%) | 10 (38.5%) | 3 (27.3%) | 0.22 |
| Newborn infection ‡,# | 2 (4.4%) | 2 (5.3%) | 0 (%) | 0 (0%) | 0 (0%) | 0.03 * |
| Low birthweight # | 5 (11.1%) | 4 (10.5%) | 3 (5.6%) | 2 (6.1%) | 2 (16.7%) | 0.78 |
| Genes | wt/mt Codons * | Muted Alleles and Position † | n | % |
|---|---|---|---|---|
| dhfr mutations (N = 37) | AAT/ATT | 51I | 31 | 83.8 |
| TGT/CGT | 59R | 36 | 97.3 | |
| AGC/AAC | 108N | 36 | 97.3 | |
| ATA/TTA | 164L | 0 | 0.0 | |
| dhps mutations (N = 35) | TCT/GCT | 436A | 14 | 40.0 |
| TCT/TTT | 436F | 21 | 60.0 | |
| GCT/GGT | 437G | 33 | 94.3 | |
| AAA/GAA | 540E | 1 | 2.9 | |
| GCG/GGG | 581G | 1 | 2.9 | |
| GCC/TCC | 613S | 3 | 8.6 | |
| dhfr-dhps mutations (N = 35) | Quadruple mutants | NRNI-FGKAA | 4 | 11.4 |
| IRNI-AAKAA | 1 | 2.9 | ||
| IRNI-FAKAA | 1 | 2.9 | ||
| IRNI-AGKAA | 10 | 28.6 | ||
| Quintuple mutants | IRNI-FGKAA | 15 | 42.9 | |
| IRNI-AGKAS | 2 | 5.7 | ||
| Sextuple mutants | IRNI-FGEAA | 1 | 2.9 | |
| Septuple mutant | IRNI-AGKGS | 1 | 2.9 | |
| k13 mutations (N = 32) | - | Mutants | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eboumbou Moukoko, C.E.; Kojom Foko, L.P.; Ayina, A.; Tornyigah, B.; Epote, A.R.; Penda, I.C.; Epee Eboumbou, P.; Ebong, S.B.; Texier, G.; Nsango, S.E.; et al. Effectiveness of Intermittent Preventive Treatment with Sulfadoxine-Pyrimethamine in Pregnancy: Low Coverage and High Prevalence of Plasmodium falciparum dhfr-dhps Quintuple Mutants as Major Challenges in Douala, an Urban Setting in Cameroon. Pathogens 2023, 12, 844. https://doi.org/10.3390/pathogens12060844
Eboumbou Moukoko CE, Kojom Foko LP, Ayina A, Tornyigah B, Epote AR, Penda IC, Epee Eboumbou P, Ebong SB, Texier G, Nsango SE, et al. Effectiveness of Intermittent Preventive Treatment with Sulfadoxine-Pyrimethamine in Pregnancy: Low Coverage and High Prevalence of Plasmodium falciparum dhfr-dhps Quintuple Mutants as Major Challenges in Douala, an Urban Setting in Cameroon. Pathogens. 2023; 12(6):844. https://doi.org/10.3390/pathogens12060844
Chicago/Turabian StyleEboumbou Moukoko, Carole Else, Loick Pradel Kojom Foko, Angèle Ayina, Bernard Tornyigah, Annie Rachel Epote, Ida Calixte Penda, Patricia Epee Eboumbou, Serge Bruno Ebong, Gaetan Texier, Sandrine Eveline Nsango, and et al. 2023. "Effectiveness of Intermittent Preventive Treatment with Sulfadoxine-Pyrimethamine in Pregnancy: Low Coverage and High Prevalence of Plasmodium falciparum dhfr-dhps Quintuple Mutants as Major Challenges in Douala, an Urban Setting in Cameroon" Pathogens 12, no. 6: 844. https://doi.org/10.3390/pathogens12060844
APA StyleEboumbou Moukoko, C. E., Kojom Foko, L. P., Ayina, A., Tornyigah, B., Epote, A. R., Penda, I. C., Epee Eboumbou, P., Ebong, S. B., Texier, G., Nsango, S. E., Ayong, L., Tuikue Ndam, N., & Same Ekobo, A. (2023). Effectiveness of Intermittent Preventive Treatment with Sulfadoxine-Pyrimethamine in Pregnancy: Low Coverage and High Prevalence of Plasmodium falciparum dhfr-dhps Quintuple Mutants as Major Challenges in Douala, an Urban Setting in Cameroon. Pathogens, 12(6), 844. https://doi.org/10.3390/pathogens12060844