

Human Papillomavirus (HPV) Infection and Risk Behavior in Vaccinated and Non-Vaccinated Paraguayan Young Women

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Specimen Collection
2.3. DNA Extraction from Cervical Samples
2.4. HPV Genotyping
2.5. Statistical Analyses
2.6. Ethical Considerations
3. Results
3.1. Demographic Characteristics of the Study Participants
3.2. Vaccination Status
3.3. Risk and Preventive Behaviors and Vaccination Status
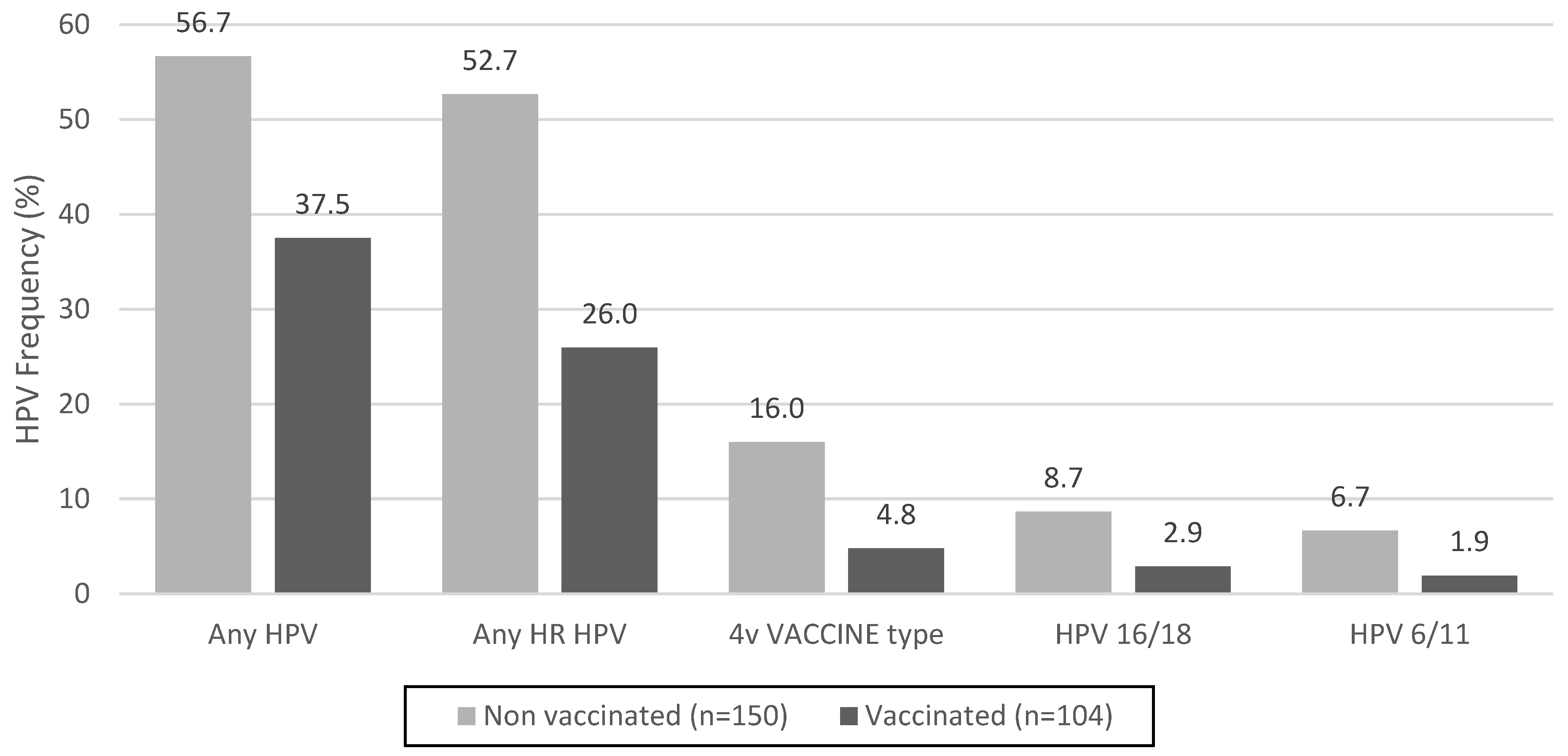
3.4. Prevalence of HPV and Genital Warts and Vaccination Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. 2020. Available online: https://gco.iarc.fr/today (accessed on 20 October 2023).
- World Health Organization. Human Papillomavirus Vaccines. In WHO Position Paper; World Health Organization: Geneva, Switzerland, 2022; Volume 97, pp. 645–672. [Google Scholar]
- Villa, L.L.; Costa, R.L.; Petta, C.A.; Andrade, R.P.; Ault, K.A.; Giuliano, A.R.; Wheeler, C.M.; Koutsky, L.A.; Malm, C.; Lehtinen, M.; et al. Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: A randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol. 2005, 6, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.M.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Harper, D.M.; Leodolter, S.; Tang, G.W.; Ferris, D.G.; Steben, M.; Bryan, J.; et al. Quadrivalent vaccine against human papillomavirus to prevent anogenital diseases. N. Engl. J. Med. 2007, 356, 1928–1943. [Google Scholar] [CrossRef] [PubMed]
- Harper, D.M.; Franco, E.L.; Wheeler, C.M.; Moscicki, A.B.; Romanowski, B.; Roteli-Martins, C.M.; Jenkins, D.; Schuind, A.; Costa Clemens, S.A.; Dubin, G.; et al. Sustained efficacy up to 4.5 years of a bivalent L1 virus-like particle vaccine against human papillomavirus types 16 and 18: Follow-up from a randomised control trial. Lancet 2006, 367, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Harper, D.M.; Franco, E.L.; Wheeler, C.; Ferris, D.G.; Jenkins, D.; Schuind, A.; Zahaf, T.; Innis, B.; Naud, P.; De Carvalho, N.S.; et al. Efficacy of a bivalent L1 virus-like particle vaccine in prevention of infection with human papillomavirus types 16 and 18 in young women: A randomised controlled trial. Lancet 2004, 364, 1757–1765. [Google Scholar] [CrossRef] [PubMed]
- Paavonen, J.; Jenkins, D.; Bosch, F.X.; Naud, P.; Salmeron, J.; Wheeler, C.M.; Chow, S.N.; Apter, D.L.; Kitchener, H.C.; Castellsague, X.; et al. Efficacy of a prophylactic adjuvanted bivalent L1 virus-like-particle vaccine against infection with human papillomavirus types 16 and 18 in young women: An interim analysis of a phase III double-blind, randomised controlled trial. Lancet 2007, 369, 2161–2170. [Google Scholar] [CrossRef]
- Lukács, A.; Máté, Z.; Farkas, N.; Mikó, A.; Tenk, J.; Hegyi, P.; Németh, B.; Czumbel, L.M.; Wuttapon, S.; Kiss, I.; et al. The quadrivalent HPV vaccine is protective against genital warts: A meta-analysis. BMC Public Health 2020, 20, 691. [Google Scholar] [CrossRef]
- Joura, E.A.; Leodolter, S.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Koutsky, L.A.; Garland, S.M.; Harper, D.M.; Tang, G.W.; Ferris, D.G.; et al. Efficacy of a quadrivalent prophylactic human papillomavirus (types 6, 11, 16, and 18) L1 virus-like-particle vaccine against high-grade vulval and vaginal lesions: A combined analysis of three randomized clinical trials. Lancet 2007, 369, 1693–1702. [Google Scholar] [CrossRef]
- Schiller, J.T.; Castellsague, X.; Villa, L.L.; Hildesheim, A. An update of prophylactic human papillomavirus L1 virus-like particle vaccine clinical trial results. Vaccine 2008, 26 (Suppl. S10), K53–K61. [Google Scholar] [CrossRef]
- Luckett, R.; Feldman, S. Impact of 2-, 4- and 9-valent HPV vaccines on morbidity and mortality from cervical cancer. Hum. Vaccines Immunother. 2016, 12, 1332–1342. [Google Scholar] [CrossRef]
- Shu, Y.; Yu, Y.; Ji, Y.; Zhang, L.; Li, Y.; Qin, H.; Huang, Z.; Ou, Z.; Huang, M.; Shen, Q.; et al. Immunogenicity and safety of two novel human papillomavirus 4- and 9-valent vaccines in Chinese women aged 20-45 years: A randomized, blinded, controlled with Gardasil (type 6/11/16/18), phase III non-inferiority clinical trial. Vaccine 2022, 40, 6947–6955. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Immunization, Vaccines and Biologicals. HPV Dashboard. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases/human-papillomavirus-vaccines-(HPV)/hpv-clearing-house/hpv-dashboard (accessed on 26 October 2023).
- World Health Organization. Human Papillomavirus Vaccines: WHO Position Paper. In Weekly Epidemiological Record. WER No 19; World Health Organization: Geneva, Switzerland, 2017; Volume 92, pp. 241–268. [Google Scholar]
- Normas Nacionales de Vacunación, Técnico Administrativas y de Vigilancia del Programa Nacional de Enfermedades Inmunoprevenibles y PAI; Ministerio de Salud Pública y Bienestar Social: Asunción, Paraguay, 2017; ISBN 978-99967-36-63-6.
- Brisson, M.; Bénard, É.; Drolet, M.; Bogaards, J.A.; Baussano, I.; Vänskä, S.; Jit, M.; Boily, M.-C.; Smith, M.; Berkhof, J.; et al. Population-level impact, herd immunity, and elimination after human papillomavirus vaccination: A systematic review and meta-analysis of predictions from transmission-dynamic models. Lancet Public Health 2016, 1, e8–e17. [Google Scholar] [CrossRef]
- Bruni, L.; Diaz, M.; Barrionuevo-Rosas, L.; Herrero, R.; Bray, F.; Bosch, F.X.; de Sanjosé, S.; Castellsagué, X. Global estimates of human papillomavirus vaccination coverage by region and income level: A pooled analysis. Lancet Glob. Health 2016, 4, e453–e463. [Google Scholar] [CrossRef] [PubMed]
- Bird, Y.; Obidiya, O.; Mahmood, R.; Nwankwo, C.; Moraros, J. Human papillomavirus vaccination uptake in Canada: A systematic review and meta-analysis. Int. J. Prev. Med. 2017, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Baines, N.; Memon, S.; Fitzgerald, N.; Chadder, J.; Politis, C.; Nicholson, E.; Earle, C.; Bryant, H. Moving toward the elimination of cervical cancer: Modelling the health and economic benefits of increasing uptake of human papillomavirus vaccines. Curr. Oncol. 2019, 26, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.; Wardle, J.; Stephenson, J.; Waller, J. Passport to promiscuity or lifesaver: Press coverage of HPV vaccination and risky sexual behavior. J. Health Commun. 2020, 15, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Schuler, C.L.; Reiter, P.L.; Smith, J.S.; Brewer, N.T. Human papillomavirus vaccine and behavioral disinhibition. Sex. Transm. Infect. 2011, 87, 349–353. [Google Scholar] [CrossRef]
- Holman, D.M.; Benard, V.; Roland, K.B.; Watson, M.; Liddon, N.; Stokley, S. Barriers to human papillomavirus vaccination among US adolescents: A systematic review of the literature. JAMA Pediatr. 2014, 168, 76–82. [Google Scholar] [CrossRef]
- Bednarczyk, R.A.; Davis, R.; Ault, K.; Orenstein, W.; Omer, S.B.J. Sexual activity–related outcomes after human papillomavirus vaccination of 11-to 12-year-olds. Pediatrics 2012, 130, 798–805. [Google Scholar] [CrossRef]
- Forster, A.S.; Marlow, L.A.; Stephenson, J.; Wardle, J.; Waller, J. Human papillomavirus vaccination and sexual behavior: Cross-sectional and longitudinal surveys conducted in England. Vaccine 2012, 30, 4939–4944. [Google Scholar] [CrossRef]
- Hansen, B.T.; Kjær, S.K.; Arnheim-Dahlström, L.; Liaw, K.-L.; Jensen, K.E.; Thomsen, L.T.; Munk, C.; Nygård, M. Human papillomavirus (HPV) vaccination and subsequent sexual behavior: Evidence from a large survey of Nordic women. Vaccine 2014, 32, 4945–4953. [Google Scholar] [CrossRef]
- Smith, L.M.; Kaufman, J.S.; Strumpf, E.C.; Levesque, L.E. Effect of human papillomavirus (HPV) vaccination on clinical indicators of sexual behavior among adolescent girls: The Ontario Grade 8 HPV Vaccine Cohort Study. Can. Med. Assoc. J. 2015, 187, E74–E81. [Google Scholar] [CrossRef] [PubMed]
- Madhivanan, P.; Pierre-Victor, D.; Mukherjee, S.; Bhoite, P.; Powell, B.; Jean-Baptiste, N.; Clarke, R.; Avent, T.; Krupp, K. Human papillomavirus vaccination and sexual disinhibition in females: A systematic review. Am. J. Prev. Med. 2016, 51, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Mullins, T.L.K.; Zimet, G.D.; Rosenthal, S.L.; Morrow, C.; Ding, L.; Huang, B.; Kahn, J.A. Human papillomavirus vaccine-related risk perceptions and subsequent sexual behaviors and sexually transmitted infections among vaccinated adolescent women. Vaccine 2016, 34, 4040–4045. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, G.S.; Phan, F.; Pedersen, H.N.; Dobson, S.R.; Naus, M.; Saewyc, E.M. Population-level sexual behaviors in adolescent girls before and after introduction of the human papillomavirus vaccine (2003–2013). Can. Med. Assoc. J. 2018, 190, E1221–E1226. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.B.; Goldman, D.P.; Seabury, S.A. Incidence of sexually transmitted infections after human papillomavirus vaccination among adolescent females. JAMA Intern. Med. 2015, 175, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Cummings, T.; Zimet, G.D.; Brown, D.; Tu, W.; Yang, Z.; Fortenberry, J.D.; Shew, M.L. Reduction of HPV infections through vaccination among at-risk urban adolescents. Vaccine 2012, 30, 5496–5499. [Google Scholar] [CrossRef] [PubMed]
- Lutringer-Magnin, D.; Kalecinski, J.; Cropet, C.; Barone, G.; Ronin, V.; Régnier, V.; Leocmach, Y.; Jacquard, A.-C.; Vanhems, P.; Chauvin, F.; et al. Prevention of sexually transmitted infections among girls and young women in relation to their HPV vaccination status. Eur. J. Public Health 2013, 23, 1046–1053. [Google Scholar] [CrossRef]
- Rysavy, M.B.; Kresowik, J.D.; Liu, D.; Mains, L.; Lessard, M.; Ryan, G.L. Human papillomavirus vaccination and sexual behavior in young women. J. Pediatr. Adolesc. Gynecol. 2014, 27, 67–71. [Google Scholar] [CrossRef]
- Sadler, L.; Roberts, S.A.; Hampal, G.; McManus, D.; Mandal, D.; Brabin, L. Comparing risk behaviours of human papillomavirus-vaccinated and non-vaccinated women. J. Fam. Plann. Reprod. Health Care 2015, 41, 255–258. [Google Scholar] [CrossRef]
- Liddon, N.C.; Leichliter, J.S.; Markowitz, L.E. Human papillomavirus vaccine and sexual behavior among adolescent and young women. Am. J. Prev. Med. 2012, 42, 44–52. [Google Scholar] [CrossRef]
- Ruiz-Sternberg, A.M.; Pinzon-Rondon, A.M. Risk perception and sexual behavior in HPV-vaccinated and unvaccinated young Colombian women. Int. J. Gynaecol. Obstet. 2014, 126, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Mattebo, M.; Grün, N.; Rosenblad, A.; Larsson, M.; Häggström-Nordin, E.; Dalianis, T.; Tydén, T. Sexual experiences in relation to HPV vaccination status in female high school students in Sweden. Eur. J. Contracept. Reprod. Health Care 2014, 19, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Kamolratanakul, S.; Pitisuttithum, P. Human Papillomavirus Vaccine Efficacy and Effectiveness against Cancer. Vaccines 2021, 9, 1413. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Human Papillomavirus (HPV) Vaccination Coverage. OMS: Switzerland. 2023. Available online: https://immunizationdata.who.int/pages/coverage/hpv.html?CODE=amr (accessed on 27 November 2023).
- Roberts, J.R.; Thompson, D.; Rogacki, B.; Hale, J.J.; Jacobson, R.M.; Opel, D.J.; Darden, P.M. Vaccine hesitancy among parents of adolescents and its association with vaccine uptake. Vaccine 2015, 33, 1748–1755. [Google Scholar] [CrossRef] [PubMed]
- Kornides, M.L.; Garrell, J.M.; Gilkey, M.B. Content of web-based continuing medical education about HPV vaccination. Vaccine 2017, 35 Pt B, 4510–4514. [Google Scholar] [CrossRef]
- Brouwer, A.F.; Delinger, R.L.; Eisenberg, M.C.; Campredon, L.P.; Walline, H.M.; Carey, T.E.; Meza, R. HPV vaccination has not increased sexual activity or accelerated sexual debut in a college-aged cohort of men and women. BMC Public Health 2019, 19, 821. [Google Scholar] [CrossRef] [PubMed]
- Marchand, E.; Glenn, B.A.; Bastani, R. HPV vaccination and sexual behavior in a community college sample. J. Community Health 2013, 38, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Mather, T.; McCaffery, K.; Juraskova, I. Does HPV vaccination affect women’s attitudes to cervical cancer screening and safe sexual behavior? Vaccine 2012, 30, 3196–3201. [Google Scholar] [CrossRef]
- Aujo, J.C.; Bakeera-Kitaka, S.; Kiguli, S.; Mirembe, F. No difference in sexual behavior of adolescent girls following human papillomavirus vaccination: A case study two districts in Uganda; Nakasongola and Luwero. BMC Public Health 2014, 14, 155. [Google Scholar] [CrossRef]
- Sopracordevole, F.; Cigolot, F.; Mancioli, F.; Agarossi, A.; Boselli, F.; Ciavattini, A. Knowledge of HPV infection and vaccination among vaccinated and unvaccinated teenaged girls. Int. J. Gynaecol. Obstet. 2013, 122, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Ratanasiripong, N.T. Human papillomavirus vaccine increases high-risk sexual behaviors: A myth or valid concern. J. Sch. Nurs. 2014, 30, 456–463. [Google Scholar] [CrossRef] [PubMed]
- González, J.V.; DeLuca, G.D.; Liotta, D.J.; Correa, R.M.; Basiletti, J.A.; Colucci, M.C.; Katz, N.; Vizzotti, C.; Picconi, M.A.; MALBRAN HPV Surveillance Study Group. Baseline prevalence and type distribution of Human papillomavirus in sexually active non-vaccinated adolescent girls from Argentina. Rev. Argent. Microbiol. 2021, 53, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Wendland, E.M.; Kops, N.L.; Bessel, M.; Comerlato, J.; Maranhão, A.G.K.; Souza, F.M.A.; Villa, L.L.; Pereira, G.F.M. Effectiveness of a universal vaccination program with an HPV quadrivalent vaccine in young Brazilian women. Vaccine 2021, 39, 1840–1845. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, S.N.; Brotherton, J.M.L.; Kaldor, J.M.; Skinner, S.R.; Liu, B.; Bateson, D.; McNamee, K.; Garefalakis, M.; Phillips, S.; Cummins, E.; et al. Assessment of herd immunity and cross-protection after a human papillomavirus vaccination programme in Australia: A repeat cross-sectional study. Lancet Infect. Dis. 2014, 14, 958–966. [Google Scholar] [CrossRef] [PubMed]
- García-Perdomo, H.A.; Osorio, J.C.; Fernandez, A.; Zapata-Copete, J.A.; Castillo, A. The effectiveness of vaccination to prevent the papillomavirus infection: A systematic review and meta-analysis. Epidemiol. Infect. 2019, 147, e156. [Google Scholar] [CrossRef] [PubMed]
- Donovan, B.; Franklin, N.; Guy, R.; Grulich, A.E.; Regan, D.G.; Ali, H.; Wand, H.; Fairley, C.K. Quadrivalent human papillomavirus vaccination and trends in genital warts in Australia: Analysis of national sentinel surveillance data. Lancet Infect. Dis. 2011, 11, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Read, T.R.H.; Hocking, J.S.; Chen, M.Y.; Donovan, B.; Bradshaw, C.S.; Fairley, C.K. The near disappearance of genital warts in young women 4 years after commencing a national human papillomavirus (HPV) vaccination programme. Sex. Transm. Infect. 2011, 87, 544–547. [Google Scholar] [CrossRef]
- Ali, H.; Donovan, B.; Wand, H.; Read, T.R.H.; Regan, D.G.; Grulich, A.; Fairley, C.K.; Guy, R.J. Genital warts in young Australians five years into national human papillomavirus vaccination programme: National surveillance data. BMJ 2013, 346, f2032. [Google Scholar] [CrossRef]
- Baandrup, L.; Blomberg, M.; Dehlendorff, C.; Sand, C.; Andersen, K.K.; Kjaer, S.K. Significant decrease in the incidence of genital warts in young Danish women after implementation of a national human papillomavirus vaccination program. Sex. Transm. Dis. 2013, 40, 130–135. [Google Scholar] [CrossRef]
- Blomberg, M.; Dehlendorff, C.; Munk, C.; Kjaer, S.K. Strongly decreased risk of genital warts after vaccination against human papillomavirus: Nationwide follow-up of vaccinated and unvaccinated girls in Denmark. Clin. Infect. Dis. 2013, 57, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Dochez, C.; Bogers, J.J.; Verhelst, R.; Rees, H. HPV vaccines to prevent cervical cancer and genital warts: An update. Vaccine 2014, 32, 1595–1601. [Google Scholar] [CrossRef] [PubMed]
- Bollerup, S.; Baldur-Felskov, B.; Blomberg, M.; Baandrup, L.; Dehlendorff, C.; Kjaer, S.K. Significant Reduction in the Incidence of Genital Warts in Young Men 5 Years into the Danish Human Papillomavirus Vaccination Program for Girls and Women. Sex. Transm. Dis. 2016, 43, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Dominiak-Felden, G.; Gobbo, C.; Simondon, F. Evaluating the Early Benefit of Quadrivalent HPV Vaccine on Genital Warts in Belgium: A Cohort Study. PLoS ONE 2015, 10, e0132404. [Google Scholar] [CrossRef] [PubMed]
- Puerto, D.; Reyes, V.; Lozano, C.; Buitrago, L.; Garcia, D.; Murillo, R.H.; Muñoz, N.; Hernandez, G.A.; Sanchez, L.; Wiesner, C.; et al. Detection and Genotyping of HPV DNA in a Group of Unvaccinated Young Women from Colombia: Baseline Measures Prior to Future Monitoring Program. Cancer Prev. Res. 2018, 11, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Dunne, E.F.; Klein, N.P.; Naleway, A.L.; Baxter, R.; Weinmann, S.; Riedlinger, K.; Fetterman, B.; Steinau, M.; Scarbrough, M.Z.; Gee, J.; et al. Prevalence of HPV types in cervical specimens from an integrated healthcare delivery system: Baseline assessment to measure HPV vaccine impact. Cancer Causes Control 2013, 24, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.V.; Kothari, S.; Skufca, J.; Giuliano, A.R.; Sundström, K.; Nygård, M.; Koro, C.; Baay, M.; Verstraeten, T.; Luxembourg, A.; et al. Real-world impact and effectiveness of the quadrivalent HPV vaccine: An updated systematic literature review. Expert. Rev. Vaccines 2022, 21, 1799–1817. [Google Scholar] [CrossRef]
- Herweijer, E.; Feldman, A.L.; Ploner, A.; Arnheim-Dahlström, L.; Uhnoo, I.; Netterlid, E.; Dillner, J.; Sparén, P.; Sundström, K. The Participation of HPV-Vaccinated Women in a National Cervical Screening Program: Population-Based Cohort Study. PLoS ONE 2015, 10, e0134185. [Google Scholar] [CrossRef]
- El-Zein, M.; Richardson, L.; Franco, E.L. Cervical cancer screening of HPV vaccinated populations: Cytology, molecular testing, both or none. J. Clin. Virol. 2016, 76 (Suppl. S1), S62–S68. [Google Scholar] [CrossRef]
- Thomas, C.; Wright, T.C.; Valentin Parvu, V.; Mark, H.; Stoler, M.H.; Salma Kodsi, S.; Karen Eckert, K.; Karen Yanson, K.; Charles, K.; Cooper, C.K. HPV infections and cytologic abnormalities in vaccinated women 21–34 years of age: Results from the baseline phase of the Onclarity trial. Gynecol. Oncol. 2019, 153, 259–265. [Google Scholar] [CrossRef]
- Bobadilla, M.L.; Villagra, V.; Ortiz, V.; Deluca, G.; de Paula, V.S. High prevalence and co-infection of high-risk Human Papillomavirus genotypes among unvaccinated young women from Paraguay. PLoS ONE 2023, 18, e0283542. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Study Population (n = 254) | |||
|---|---|---|---|---|
| N | % or Mean | 95% Confidence Interval | ||
| Age (mean years) | 22.1 ± 2.2 | 21.8 | 22.4 | |
| Residency | ||||
| Asunción | 63 | 24.8 | 19.6 | 30.6 |
| Other localities | 191 | 75.2 | 69.4 | 80.4 |
| Education level | ||||
| Primary/Secondary | 70 | 27.6 | 22.2 | 33.5 |
| Tertiary | 184 | 72.4 | 66.5 | 77.8 |
| Occupation | ||||
| Economically active (have any job) | 69 | 27.2 | 21.8 | 33.1 |
| Not economically active (unemployed, student, houseworkers) | 185 | 72.8 | 66.9 | 78.2 |
| Live with | ||||
| Parents/Friends/Alone | 211 | 83.1 | 77.9 | 87.5 |
| Partner | 43 | 16.9 | 12.5 | 22.1 |
| Variable | Vaccination Status | p Value | |
|---|---|---|---|
| Yes n (%)/Mean (SD) (n = 104) | No n (%)/Mean (SD) (n = 150) | ||
| Sexual behavior | |||
| Age at sexual debut (mean years) | 16.8 ± 2.2 | 16.7 ± 2.1 | 0.9744 |
| ≤15 years | 27 (26.0) | 38 (25.3) | 0.9102 |
| >15 years | 77 (74.0) | 112 (74.7) | |
| Sex partners in the past 12 months | |||
| ≥2 | 39 (37.5) | 65 (43.3) | 0.3525 |
| ≤1 | 65 (62.5) | 85 (56.7) | |
| Oral sex | |||
| Yes | 92 (86.5) | 131 (87.3) | 0.7871 |
| No | 12 (11.5) | 19 (12.7) | |
| Hormonal contraceptives | |||
| Yes | 30 (28.9) | 41 (27.3) | 0.7916 |
| No | 74 (71.2) | 109 (72.7) | |
| Condom use | |||
| Less than every time | 76 (73.1) | 112 (74.7) | 0.7763 |
| Every time | 28 (26.9) | 38 (25.3) | |
| History of any sexually transmitted disease | |||
| Yes | 24 (23.1) | 50 (33.3) | 0.0768 |
| No | 80 (76.9) | 100 66.7) | |
| History of anogenital warts | |||
| Yes | 12 (11.5) | 31 (20.7) | 0.0564 |
| No | 92 (88.5) | 119 (79.3) | |
| HPV infection | |||
| Yes | 39 (37.5) | 85 (56.7) | 0.0026 |
| No | 65 (62.5) | 65 (43.3) | |
| Smoking status | |||
| Yes | 18 (17.3) | 33 (22.0) | 0.3586 |
| No | 86 (82.7) | 117 (78.0) | |
| Alcohol use | |||
| Yes | 77 (74.0) | 123 (82.0) | 0.1273 |
| No | 27 (26.0) | 27 (18.0) | |
| Genotype | Cases (n) | Frequency (%) n = 85 | |
|---|---|---|---|
| LR-HPV | 6 | 8 | 9.4 |
| 11 | 2 | 2.4 | |
| 40 | 2 | 2.4 | |
| 42 | 5 | 5.9 | |
| 54 | 2 | 2.4 | |
| 61 | 2 | 2.4 | |
| 71 | 2 | 2.4 | |
| 72 | 1 | 1.2 | |
| 81 | 8 | 9.4 | |
| 83 | 2 | 2.4 | |
| 84 | 2 | 2.4 | |
| pHR-HPV | 26 | 2 | 2.4 |
| 53 | 11 | 12.9 | |
| 66 | 9 | 10.6 | |
| 70 | 5 | 5.9 | |
| 82 | 4 | 4.7 | |
| 85 | 1 | 1.2 | |
| HR-HPV | 16 | 11 | 12.9 |
| 18 | 3 | 3.5 | |
| 31 | 8 | 9.4 | |
| 33 | 8 | 9.4 | |
| 35 | 5 | 5.9 | |
| 39 | 1 | 1.2 | |
| 45 | 1 | 1.2 | |
| 51 | 11 | 12.9 | |
| 52 | 9 | 10.6 | |
| 56 | 1 | 1.2 | |
| 58 | 16 | 18.8 | |
| 59 | 5 | 5.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bobadilla, M.L.; Villagra, V.; Castro, H.; von Horoch, M.; Araya, S.; Deluca, G.; de Paula, V.S. Human Papillomavirus (HPV) Infection and Risk Behavior in Vaccinated and Non-Vaccinated Paraguayan Young Women. Pathogens 2024, 13, 209. https://doi.org/10.3390/pathogens13030209
Bobadilla ML, Villagra V, Castro H, von Horoch M, Araya S, Deluca G, de Paula VS. Human Papillomavirus (HPV) Infection and Risk Behavior in Vaccinated and Non-Vaccinated Paraguayan Young Women. Pathogens. 2024; 13(3):209. https://doi.org/10.3390/pathogens13030209
Chicago/Turabian StyleBobadilla, María Liz, Verónica Villagra, Héctor Castro, Marta von Horoch, Soraya Araya, Gerardo Deluca, and Vanessa Salete de Paula. 2024. "Human Papillomavirus (HPV) Infection and Risk Behavior in Vaccinated and Non-Vaccinated Paraguayan Young Women" Pathogens 13, no. 3: 209. https://doi.org/10.3390/pathogens13030209
APA StyleBobadilla, M. L., Villagra, V., Castro, H., von Horoch, M., Araya, S., Deluca, G., & de Paula, V. S. (2024). Human Papillomavirus (HPV) Infection and Risk Behavior in Vaccinated and Non-Vaccinated Paraguayan Young Women. Pathogens, 13(3), 209. https://doi.org/10.3390/pathogens13030209