
Combination of Heat Shock and Enhanced Thermal Regime to Control the Growth of a Persistent Legionella pneumophila Strain

Abstract
:1. Introduction
2. Results and Discussion
2.1. Effect of Thermal Disinfection on Legionella pneumophila
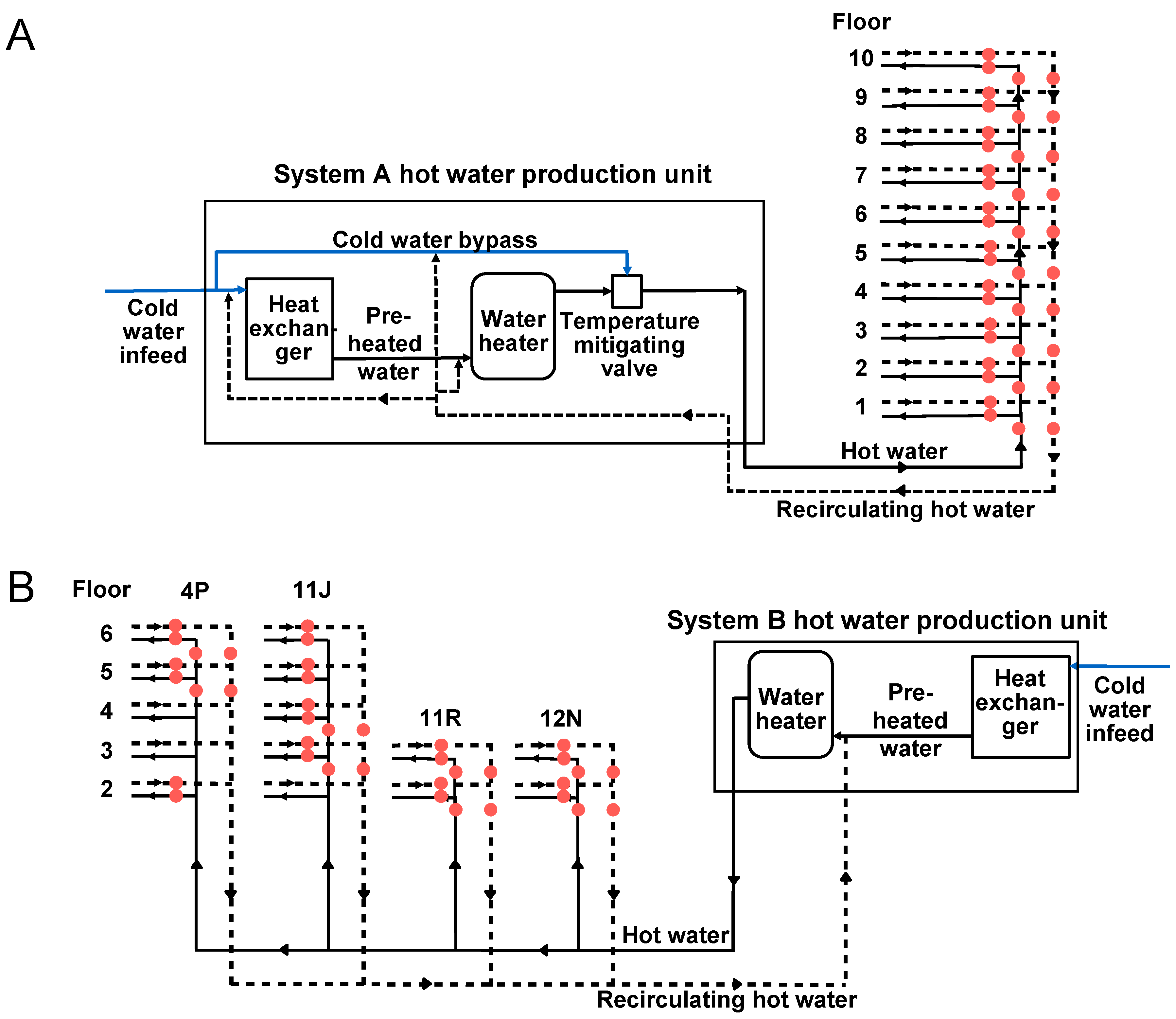
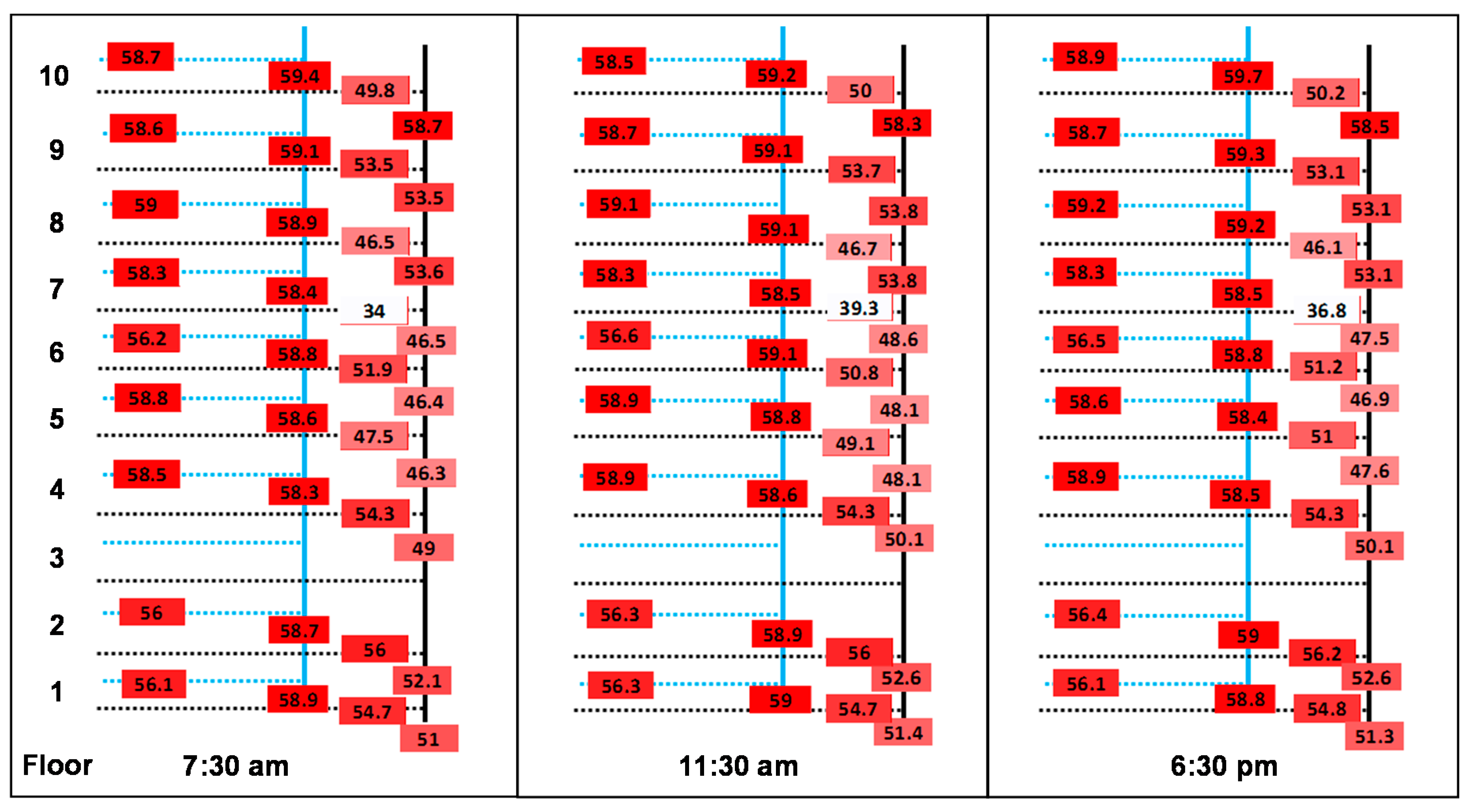
2.2. Hot Water System Temperature Diagnostic
2.2.1. Principal Recirculation Loop
2.2.2. Subordinate Flow and Return Loops
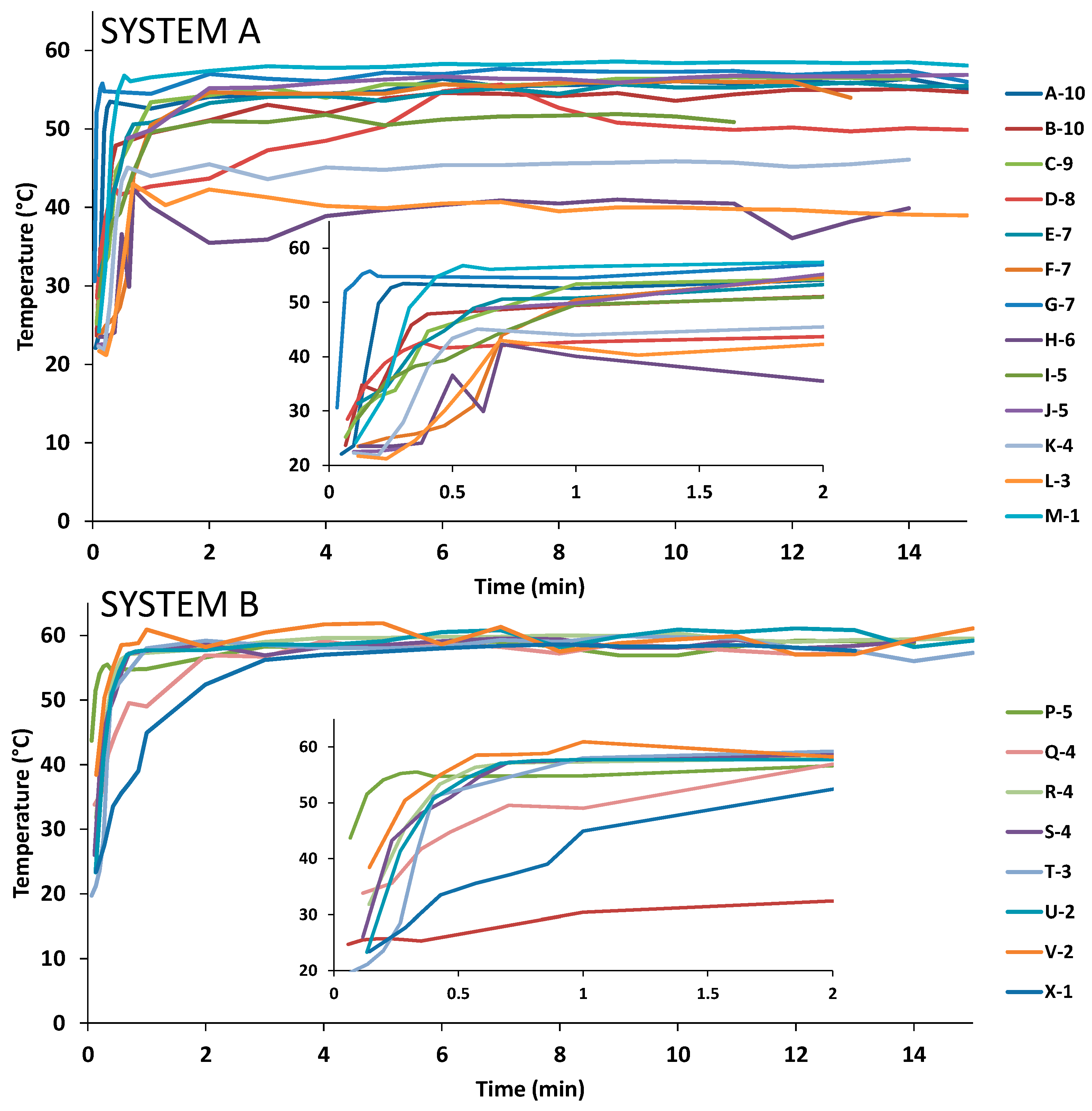
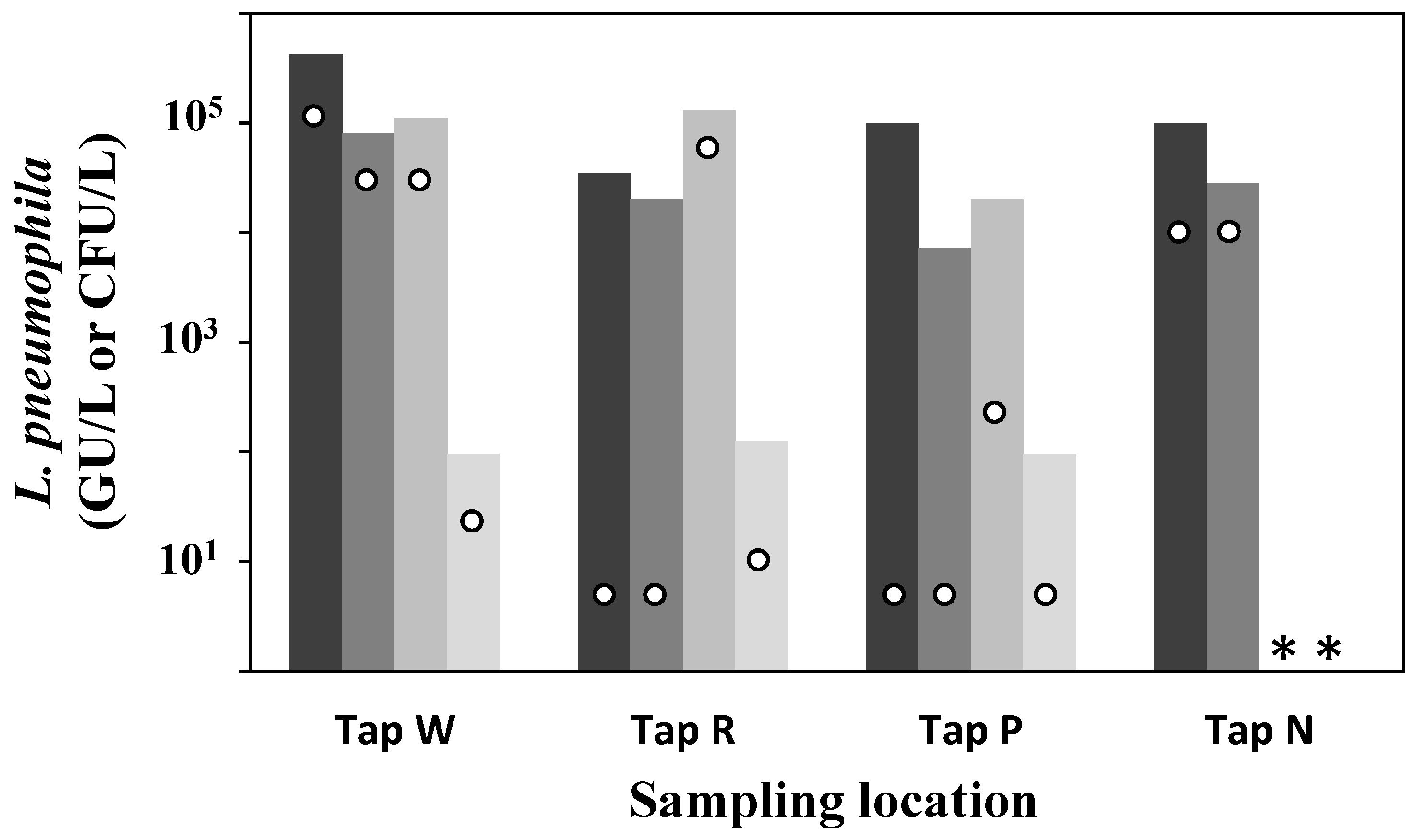
2.2.3. Tertiary Loop and Points-of-Use Characterization
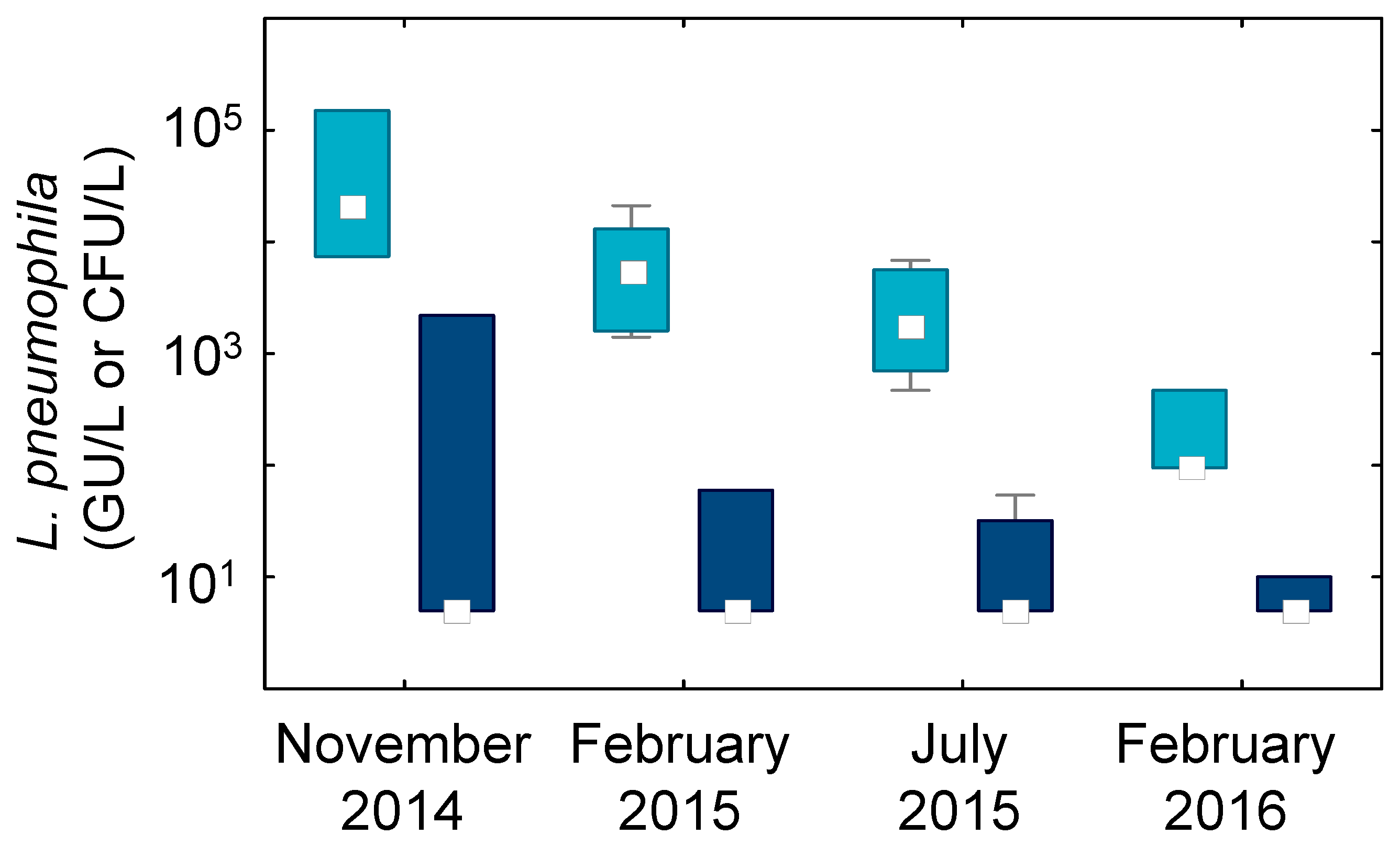
2.3. Legionella pneumophila Occurrence in the Hot Water Systems
3. Experimental Section
3.1. Thermal Disinfection
3.2. Hot Water Recirculation Loop Diagnostic
3.3. Points-of-Use Characterization
3.4. Microbiological Analysis
3.5. Statistics
4. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References and Notes
- Bartley, P.B.; Ben Zakour, N.L.; Stanton-Cook, M.; Muguli, R.; Prado, L.; Garnys, V.; Taylor, K.; Barnett, T.C.; Pinna, G.; Robson, J.; et al. Hospital-wide eradication of a nosocomial Legionella pneumophila serogroup 1 outbreak. Clin. Infect. Dis. 2016, 62, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Darelid, J.; Lofgren, S.; Malmvall, B.E. Control of nosocomial legionnaires’ disease by keeping the circulating hot water temperature above 55 °C: Experience from a 10-year surveillance programme in a district general hospital. J. Hosp. Infect. 2002, 50, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Demirjian, A.; Lucas, C.E.; Garrison, L.E.; Kozak-Muiznieks, N.A.; States, S.; Brown, E.W.; Wortham, J.M.; Beaudoin, A.; Casey, M.L.; Marriott, C.; et al. The importance of clinical surveillance in detecting legionnaires’ disease outbreaks: A large outbreak in a hospital with a Legionella disinfection system—Pennsylvania, 2011–2012. Clin. Infect. Dis. 2015, 60, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Montagna, M.T.; Ricci, C.; Napoli, C.; Tat, D.; Scaturro, M.; Barbuti, G.; Pierucci, G.; Castellani Pastoris, M. Legionella pneumophila serogroup 5 infection in the presence of multiple environmental contamination. The importance of a bacteriological diagnosis. Ital. J. Public Health 2007. [Google Scholar] [CrossRef]
- Arvand, M.; Jungkind, K.; Hack, A. Contamination of the cold water distribution system of health care facilities by Legionella pneumophila: Do we know the true dimension? Eurosurveillance 2011, 16, 1–6. [Google Scholar]
- Bargellini, A.; Marchesi, I.; Righi, E.; Ferrari, A.; Cencetti, S.; Borella, P.; Rovesti, S. Parameters predictive of Legionella contamination in hot water systems: Association with trace elements and heterotrophic plate counts. Water Res. 2011, 45, 2315–2321. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, F.; Caruso, A.; Moschini, L.; Turano, A.; Scarcella, C.; Speziani, F. A comparison of Legionella pneumophila occurrence in hot water tanks and instantaneous devices in domestic, nosocomial, and community environments. Curr. Microbiol. 2000, 41, 374–376. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Suarez, A.; Dellunde, J.; Salvado, H.; Cervero-Arago, S.; Mendez, J.; Canals, O.; Blanco, S.; Arcas, A.; Araujo, R. Microbial and physicochemical parameters associated with Legionella contamination in hot water recirculation systems. Environ. Sci. Pollut. Res. Int. 2013, 20, 5534–5544. [Google Scholar] [CrossRef] [PubMed]
- Stout, J.E.; Muder, R.R.; Mietzner, S.; Wagener, M.M.; Perri, M.B.; DeRoos, K.; Goodrich, D.; Arnold, W.; Williamson, T.; Ruark, O.; et al. Role of environmental surveillance in determining the risk of hospital-acquired legionellosis: A national surveillance study with clinical correlations. Infect. Control Hosp. Epidemiol. 2007, 28, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Collier, S.A.; Stockman, L.J.; Hicks, L.A.; Garrison, L.E.; Zhou, F.J.; Beach, M.J. Direct healthcare costs of selected diseases primarily or partially transmitted by water. Epidemiol. Infect. 2012, 140, 2003–2013. [Google Scholar] [CrossRef] [PubMed]
- Health and Safety Executive (HSE). Legionnaires’ Disease: Technical Guidance. Part 2: The Control of Legionella Bacteria in Hot and Cold Water Systems; HSE Books: Liverpool, UK, 2013. [Google Scholar]
- Torii, K.; Iinuma, Y.; Ichikawa, M.; Kato, K.; Koide, M.; Baba, H.; Suzuki, R.; Ohta, M. A case of nosocomial Legionella pneumophila pneumonia. Jpn. J. Infect. Dis. 2003, 56, 101–102. [Google Scholar] [PubMed]
- République Française. Arrêté du 1er Février 2010 Relatif à la Surveillance des Légionelles dans les Installations de Production, de Stockage et de Distribution d’eau Chaude Sanitaire; Legifrance: Paris, France, 2010. [Google Scholar]
- DVGW German Technical and Scientific Association for Gas and Water. Drinking Water Heating and Drinking Water Piping Systems; Technical Measures to Reduce Legionella Growth; Design, Construction, Operation and Rehabilitation Of Drinking Water Installations; Technical Rule: Code of Practice w 551; Drinking Water Heating and Drinking Water Piping Systems: Bonn, Germany, 2004. [Google Scholar]
- Regiona Assessorato alla Sanità; Ministero della Santa Dipartimento della Prevenzione; Instituto Superiore di Sanita Registro Nazionale delle Legionellosi. Conferenza Permanente per i Rapporti tra lo Stato, le Regioni e le Province Autonome di Trento e Bolzano. Documento di Linee-Guida per la Prevenzione e il Controllo della Legionellosi; Health Ministry: Rome, Italy, 2002.
- Austrian Standards Institute. Hygienerelevante Planung, Ausführung, Betrieb, Wartung, Überwachung und Sanierung von Zentralen Trinkwasser-Wärmungsanlagen; Austrian Standards Institute: Vienna, Austria, 2007. [Google Scholar]
- Office Fédéral de la Santé Publique. Legionella et Légionellose; Office Fédéral de la Santé Publique: Berne, Switzerland, 2008. [Google Scholar]
- Government of South Australia; Health Protection Programs; Public Health Services; Public Health and Clinical Systems; Department for Health and Ageing; On the recommendation of the Chief Public Health Officer. Guidelines for the Control of Legionella in Manufactured Water Systems in South Australia 2008; 9781742435169; Government of South Australia: Rundle, Australia, 2013.
- Lee, J.V.; Lai, S.; Exner, M.; Lenz, J.; Gaia, V.; Casati, S.; Hartemann, P.; Lück, C.; Pangon, B.; Ricci, M.L.; et al. An international trial of quantitative PCR for monitoring Legionella in artificial water systems. J. Appl. Microbiol. 2011, 110, 1032–1044. [Google Scholar] [CrossRef] [PubMed]
- Bédard, E.; Fey, S.; Charron, D.; Lalancette, C.; Cantin, P.; Dolcé, P.; Laferrière, C.; Déziel, E.; Prévost, M. Temperature diagnostic to identify high risk areas and optimize Legionella pneumophila surveillance in hot water distribution systems. Water Res. 2015, 71, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Centre Scientifique et Technique du Bâtiment (CSTB). Guide Technique—Maîtrise du Risque de Développement des Légionelles dans les Réseaux d’eau Chaude Sanitaire—Défaillances et Préconisations; CSTB Éditions: Marne la Vallée, France, 2012. [Google Scholar]
- République Française. Circulaire n° dgs/ea4/2010/448 du 21 Décembre 2010 Relative aux Missions des Agences Régionales de Santé dans la Mise en Oeuvre de L’arrêté du 1er Février 2010 Relatif à la Surveillance des Légionelles dans les Installations de Production, de Stockage et de Distribution d’eau Chaude Sanitaire; Legifrance: Paris, France, 2010. [Google Scholar]
- Lin, Y.E.; Stout, J.E.; Yu, V.L. Controlling Legionella in hospital drinking water: An evidence-based review of disinfection methods. Infect. Control Hosp. Epidemiol. 2011, 32, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Ezzeddine, H.; Van Ossel, C.; Delmee, M.; Wauters, G. Legionella spp. in a hospital hot water system: Effect of control measures. J. Hosp. Infect. 1989, 13, 121–131. [Google Scholar] [CrossRef]
- Blanc, D.S.; Carrara, P.; Zanetti, G.; Francioli, P. Water disinfection with ozone, copper and silver ions, and temperature increase to control Legionella: Seven years of experience in a university teaching hospital. J. Hosp. Infect. 2005, 60, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Hruba, L. The colonization of hot water systems by Legionella. Ann. Agric. Environ. Med. 2009, 16, 115–119. [Google Scholar] [PubMed]
- García, M.T.; Jones, S.; Pelaz, C.; Millar, R.D.; Abu Kwaik, Y. Acanthamoeba polyphaga resuscitates viable non-culturable Legionella pneumophila after disinfection. Environ. Microbiol. 2007, 9, 1267–1277. [Google Scholar] [CrossRef] [PubMed]
- Alleron, L.; Merlet, N.; Lacombe, C.; Frère, J. Long-term survival of Legionella pneumophila in the viable but nonculturable state after monochloramine treatment. Curr. Microbiol. 2008, 57, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Suarez, A.; Araujo, R. Evaluation of Legionella presence in the water system of a public building by semi-nested polymerase chain reaction as a rapid screening method complementary to plate count. Water Sci. Technol. Water Supply 2013, 13, 1560–1568. [Google Scholar] [CrossRef]
- Donohue, M.J.; Vesper, S.J.; Mistry, J.; King, D.; Kostich, M.; Pfaller, S.; O’Connell, K. Widespread molecular detection of Legionella pneumophila serogroup 1 in cold water taps across the United States. Environ. Sci. Technol. 2014, 48, 3145–3152. [Google Scholar] [CrossRef] [PubMed]
- Rhoads, W.; Pruden, A.; Edwards, M. Convective mixing in distal pipes exacerbates Legionella pneumophila growth in hot water plumbing. Pathogens 2016. [Google Scholar] [CrossRef] [PubMed]
- Bedard, E.; Laferriere, C.; Charron, D.; Lalancette, C.; Renaud, C.; Desmarais, N.; Deziel, E.; Prevost, M. Post-outbreak investigation of pseudomonas aeruginosa faucet contamination by quantitative polymerase chain reaction and environmental factors affecting positivity. Infect. Control Hosp. Epidemiol. 2015, 36, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Best, M.; Yu, V.L.; Stout, J.; Goetz, A.; Muder, R.R.; Taylor, F. Legionellaceae in the hospital water-supply. Epidemiological link with disease and evaluation of a method for control of nosocomial legionnaires’ disease and pittsburgh pneumonia. Lancet 1983, 2, 307–310. [Google Scholar] [CrossRef]
- Bédard, E.; Lévesque, S.; Paranjape, K.; Lalancette, C.; Dolcé, C.E.; Villion, M.; Valiquette, L.; Faucher, S.; Prévost, M. Energy conservation promotes Legionella pneumophila outbreak: The role of heat exchangers. Unpublished work. 2016. [Google Scholar]
- Cristina, M.L.; Spagnolo, A.M.; Casini, B.; Baggiani, A.; Del Giudice, P.; Brusaferro, S.; Poscia, A.; Moscato, U.; Perdelli, F.; Orlando, P. The impact of aerators on water contamination by emerging gram-negative opportunists in at-risk hospital departments. Infect. Control Hosp. Epidemiol. 2014, 35, 122–129. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency (USEPA). Method 200.8—Determination of Trace Elements in Waters and Wastes by Inductively Coupled Plasma—Mass Spectrometry (Revision 5.4—Emmc Version); Office of Research and Development: Cincinnati, OH, USA, 1994.
- Association Française de Normalisation (AFNOR). Qualité de l’eau—Recherche et Dénombrement de Legionella spp. et de Legionella pneumophila—Méthode par Ensemencement Direct et Après Concentration par Filtration sur Membrane ou Centrifugation; NF T90–431; AFNOR: La Plaine Saint-Denis, France, 2014. [Google Scholar]
- Association Française de Normalisation (AFNOR). Qualité de l’eau—Détection et quantification des Legionella et/ou Legionella pneumophila par concentration et amplification génique par réaction de polymérisation en chaîne en temps réel (rt-PCR). In Norme Française; NFT90-471AFNOR: La Plaine Saint-Denis, France, 2010. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| L. pneumophila Positivity | System A | System B | ||
|---|---|---|---|---|
| Before | After | Before | After | |
| Mean L. pneumophila levels 1 (CFU/L) | 27,200 | <LD 2 | 1700 | 2000 |
| Number of samples | 27 | 20 | 10 | 10 |
| % positives | 81.5 | 0 | 50 | 40 |
| n | Mean Temperature ± SD (°C) | % at 55 °C after 2 min | % TMAX ≥ 55 °C | ||||
|---|---|---|---|---|---|---|---|
| First Flush | 1 min | 2 min | Max | ||||
| System A | 13 | 25.2 ± 3.4 | 48.8 ± 5.4 | 50.4 ± 6.6 | 52.5 ± 6.1 | 31% | 54% |
| System B | 8 | 30.0 ± 8.3 | 55.0 ± 5.4 | 57.2 ± 2.1 | 59.0 ± 1.3 | 88% | 100% |
| System | Prior stagnation | Copper (µg/L) | Silver (µg/L) | ||
|---|---|---|---|---|---|
| Hot Water n = 23 | Cold Water n = 12 | Hot Water n = 23 | Cold Water n = 12 | ||
| System A | 15-min flush | 332 ± 38 | 103 ± 40 | 0.014 ± 0.004 | <LD |
| 30-min stagnation | 399 ± 66 | 215 ± 65 | 0.016 ± 0.008 | <LD | |
| System B | 15-min flush | 266 ± 44 | 45 ± 14 | 0.01 ± 0.003 | <LD |
| 30-min stagnation | 357 ± 75 | 184 ± 52 | 0.01 ± 0.003 | <LD | |
| System A | System B | |||||||
|---|---|---|---|---|---|---|---|---|
| 14 November | 15 February | 15 July | 16 February | 14 November | 15 February | 15 July | 16 February | |
| n | 9 | 11 | 10 | 10 | 4 | 4 | 3 | 3 |
| qPCR | 100% | 91% | 90% | 20% | 100% | 100% | 100% | 0% |
| Culture | 33% | 45% | 20% | 20% | 50% | 50% | 100% | 67% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bédard, E.; Boppe, I.; Kouamé, S.; Martin, P.; Pinsonneault, L.; Valiquette, L.; Racine, J.; Prévost, M. Combination of Heat Shock and Enhanced Thermal Regime to Control the Growth of a Persistent Legionella pneumophila Strain. Pathogens 2016, 5, 35. https://doi.org/10.3390/pathogens5020035
Bédard E, Boppe I, Kouamé S, Martin P, Pinsonneault L, Valiquette L, Racine J, Prévost M. Combination of Heat Shock and Enhanced Thermal Regime to Control the Growth of a Persistent Legionella pneumophila Strain. Pathogens. 2016; 5(2):35. https://doi.org/10.3390/pathogens5020035
Chicago/Turabian StyleBédard, Emilie, Inès Boppe, Serge Kouamé, Philippe Martin, Linda Pinsonneault, Louis Valiquette, Jules Racine, and Michèle Prévost. 2016. "Combination of Heat Shock and Enhanced Thermal Regime to Control the Growth of a Persistent Legionella pneumophila Strain" Pathogens 5, no. 2: 35. https://doi.org/10.3390/pathogens5020035
APA StyleBédard, E., Boppe, I., Kouamé, S., Martin, P., Pinsonneault, L., Valiquette, L., Racine, J., & Prévost, M. (2016). Combination of Heat Shock and Enhanced Thermal Regime to Control the Growth of a Persistent Legionella pneumophila Strain. Pathogens, 5(2), 35. https://doi.org/10.3390/pathogens5020035