Comprehensive Evaluation of Hepatitis E Serology and Molecular Testing in a Large Cohort


Abstract
:1. Introduction
2. Patients and Methods
3. Results
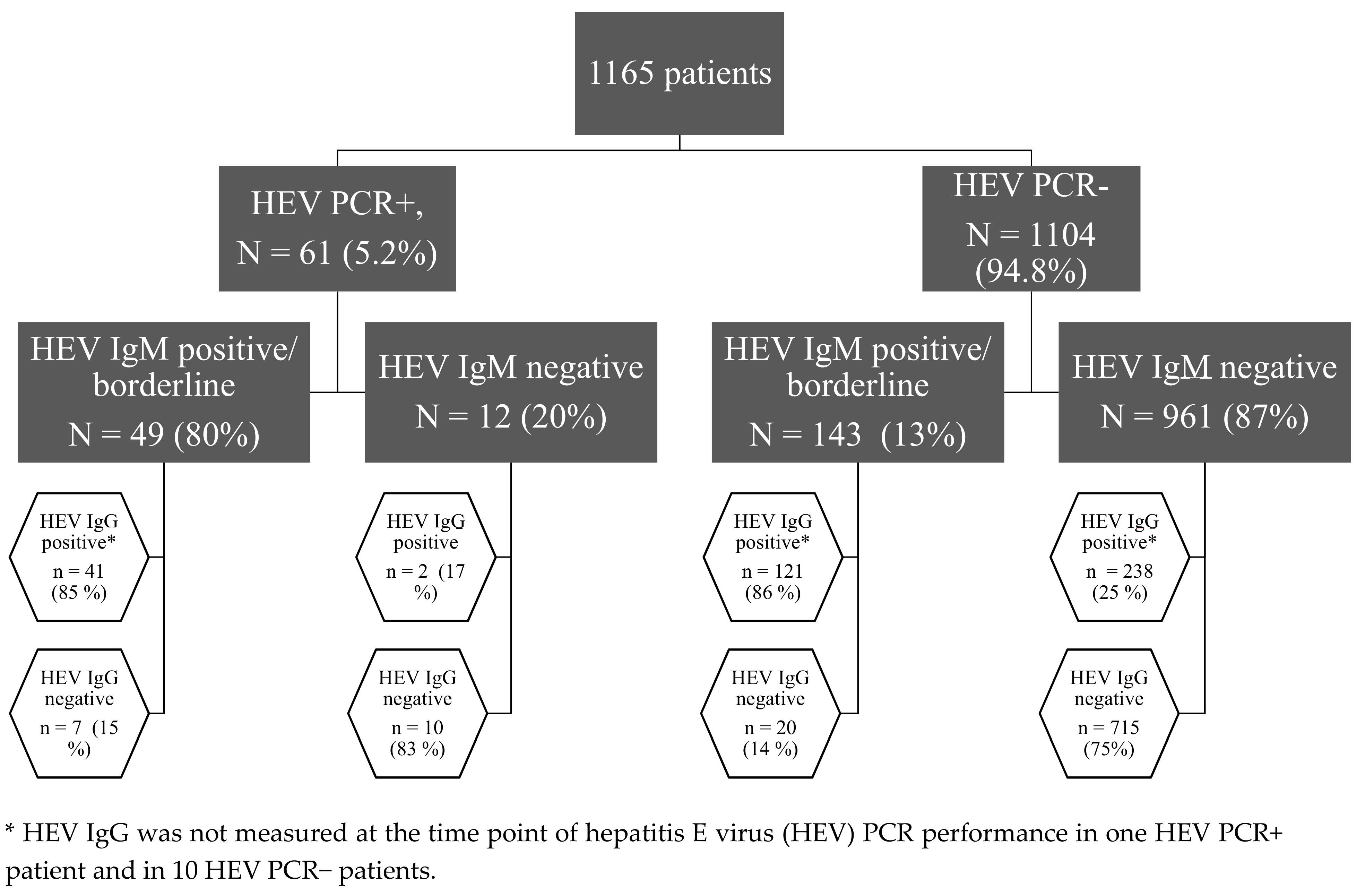
3.1. Not All Patients with Replicative HEV Infection Had Detectable HEV Specific Antibodies
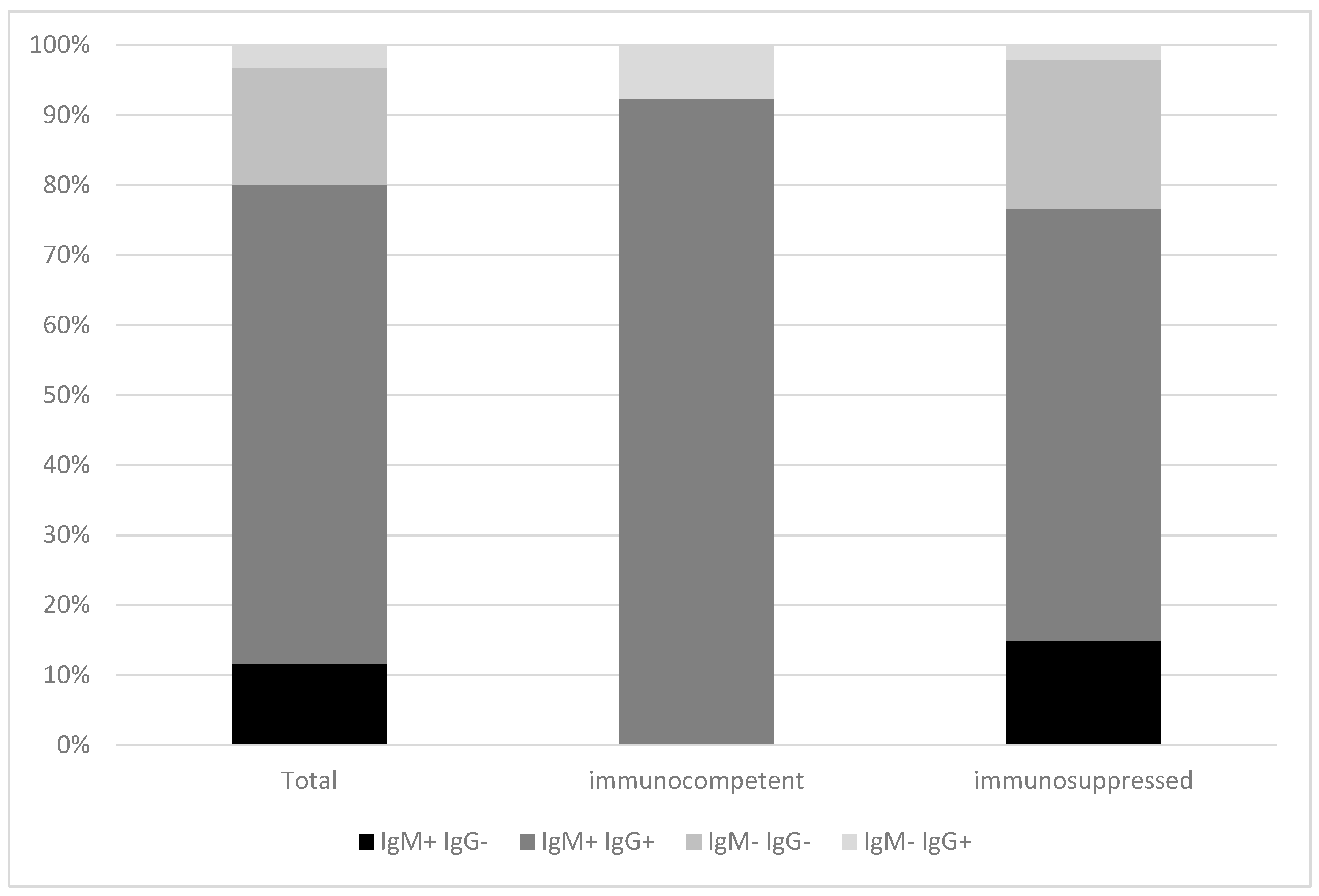
3.2. HEV Infected Immunocompetent Patients Have Higher IgG and HEV IgA Titers and Are at Higher Risk for an Acute Liver Failure Compared to Immunosuppressed Patients
3.3. HEV PCR Positive Patients with Negative HEV IgM Had Lower Serum IgG and Lower HEV IgG Levels
3.4. HEV RNA Negative/HEV IgM Positive Patients Frequently Had No History of HEV Infection
3.5. Sensitivity and Specificity of Commercially Available HEV IgM ELISA Tests Differ between Immunocompetent and Immunosuppressed Individuals
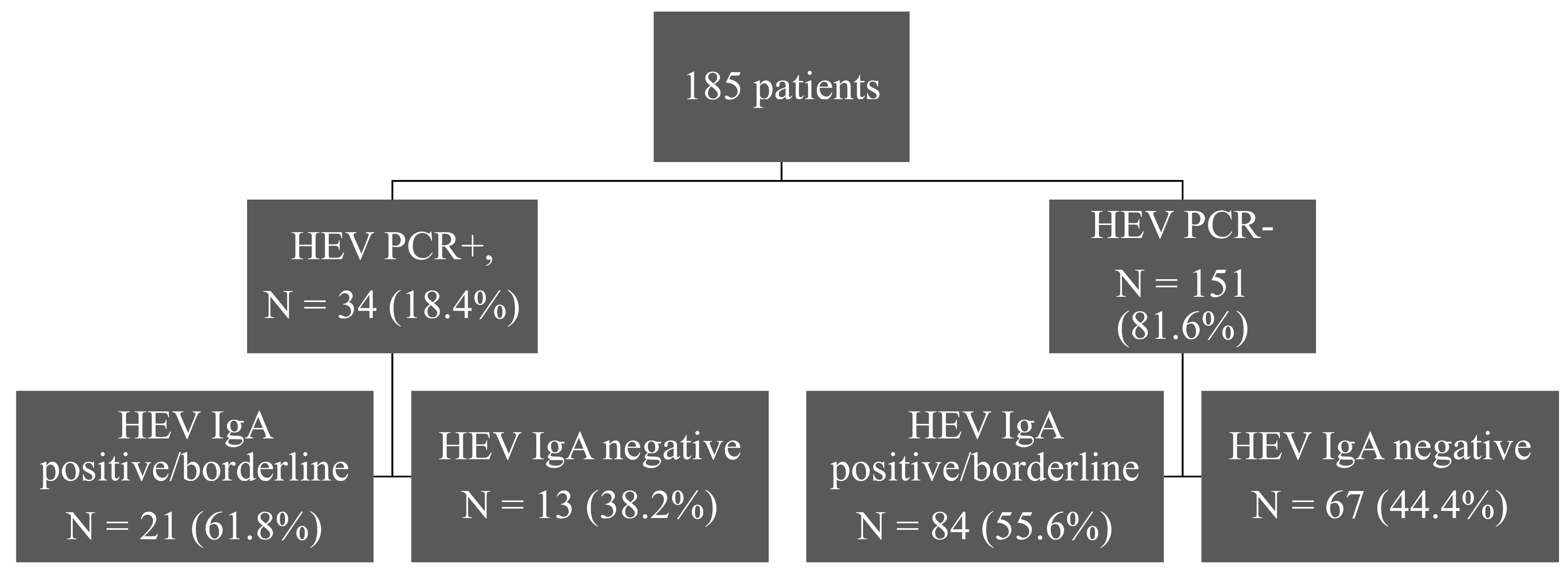
3.6. A Specific HEV IgA ELISA Fails to Detect IgA in HEV RNA Positive/HEV IgM Negative Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Shrestha, A.C.; Flower, R.L.P.; Seed, C.; Rajkarnikar, M.; Shrestha, S.K.; Thapa, U.; Hoad, V.C.; Faddy, H. Hepatitis E virus seroepidemiology: A post-earthquake study among blood donors in Nepal. BMC Infect. Dis. 2016, 16, 707. [Google Scholar] [CrossRef] [Green Version]
- Dalton, H.; Kamar, N.; Baylis, S.A.; Moradpour, D.; Wedemeyer, H.; Negro, F. EASL Clinical Practice Guidelines on hepatitis E virus infection. J. Hepatol. 2018, 68, 1256–1271. [Google Scholar] [CrossRef] [PubMed]
- Adlhoch, C.; Calvo, A.A.; Baylis, S.A.; Ciccaglione, A.R.; Couturier, E.; De Sousa, R.; Epštein, J.; Ethelberg, S.; Faber, M.; Fehér, Á.; et al. Hepatitis E virus: Assessment of the epidemiological situation in humans in Europe, 2014/15. J. Clin. Virol. 2016, 82, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Manka, P.; Bechmann, L.; Coombes, J.; Thodou, V.; Schlattjan, M.; Kahraman, A.; Syn, W.-K.; Saner, F.; Gerken, G.; Baba, H.; et al. Hepatitis E Virus Infection as a Possible Cause of Acute Liver Failure in Europe. Clin. Gastroenterol. Hepatol. 2015, 13, 1836–1842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blasco-Perrin, H.; Madden, R.G.; Stanley, A.; Crossan, C.; Hunter, J.G.; Vine, L.; Lane, K.; Devooght-Johnson, N.; McLaughlin, C.; Petrik, J.; et al. Hepatitis E virus in patients with decompensated chronic liver disease: A prospective UK/French study. Aliment. Pharmacol. Ther. 2015, 42, 574–581. [Google Scholar] [CrossRef]
- Bazerbachi, F.; Haffar, S.; Garg, S.K.; Lake, J.R. Extra-hepatic manifestations associated with hepatitis E virus infection: A comprehensive review of the literature. Gastroenterol. Rep. 2015, 4, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Hyams, C.; Mabayoje, D.A.; Copping, R.; Maranao, D.; Patel, M.; Labbett, W.; Haque, T.; Webster, D.P. Serological cross reactivity to CMV and EBV causes problems in the diagnosis of acute hepatitis E virus infection. J. Med. Virol. 2014, 86, 478–483. [Google Scholar] [CrossRef]
- Fogeda, M.; De Ory, F.; Avellón, A.; Echevarría, J. Differential diagnosis of hepatitis E virus, cytomegalovirus and Epstein-Barr virus infection in patients with suspected hepatitis E. J. Clin. Virol. 2009, 45, 259–261. [Google Scholar] [CrossRef]
- Gray, J.; Caldwell, J.; Sillis, M. The rapid serological diagnosis of infectious mononucleosis. J. Infect. 1992, 25, 39–46. [Google Scholar] [CrossRef]
- WHO. Hepatitis, E. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-e (accessed on 17 January 2019).
- Sommerkorn, F.M.; Schauer, B.; Schreiner, T.; Fickenscher, H.; Krumbholz, A. Performance of Hepatitis E Virus (HEV)-antibody tests: A comparative analysis based on samples from individuals with direct contact to domestic pigs or wild boar in Germany. Med. Microbiol. Immunol. 2017, 206, 277–286. [Google Scholar] [CrossRef]
- Ricco, G.; Bonino, F.; Lanza, M.; Scatena, F.; Alfieri, C.M.; Messa, P.; Marchisio, E.; Mascolo, G.; Romano’, L.; Galli, C.; et al. New immunoassays for total, IgA and IgM antibodies against hepatitis E virus: Prevalence in Italian blood donors and patients with chronic liver or kidney diseases. Dig. Liver Dis. 2016, 48, 536–541. [Google Scholar] [CrossRef]
- Drobeniuc, J.; Meng, J.; Reuter, G.; Greene-Montfort, T.; Khudyakova, N.; Dimitrova, Z.; Kamili, S.; Teo, C.-G. Serologic Assays Specific to Immunoglobulin M Antibodies against Hepatitis E Virus: Pangenotypic Evaluation of Performances. Clin. Infect. Dis. 2010, 51, e24–e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo, A.A.; Morago, L.; Del Carmen, M.G.-G.; Munoz, M.; Echevarria, J.-M.; Garcia-Galera, M. Comparative sensitivity of commercial tests for hepatitis E genotype 3 virus antibody detection. J. Med. Virol. 2015, 87, 1934–1939. [Google Scholar]
- Pas, S.; Streefkerk, R.H.; Pronk, M.; De Man, R.A.; Beersma, M.F.; Osterhaus, A.D.; Van Der Eijk, A.A. Diagnostic performance of selected commercial HEV IgM and IgG ELISAs for immunocompromised and immunocompetent patients. J. Clin. Virol. 2013, 58, 629–634. [Google Scholar] [CrossRef]
- Norder, H.; Karlsson, M.; Mellgren, Å.; Konar, J.; Sandberg, E.; Lasson, A.; Castedal, M.; Magnius, L.; Lagging, M. Diagnostic Performance of Five Assays for Anti-Hepatitis E Virus IgG and IgM in a Large Cohort Study. J. Clin. Microbiol. 2016, 54, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, M.; Kusakai, S.; Mizuo, H.; Suzuki, K.; Fujimura, K.; Masuko, K.; Sugai, Y.; Aikawa, T.; Nishizawa, T.; Okamoto, H. Simultaneous Detection of Immunoglobulin A (IgA) and IgM Antibodies against Hepatitis E Virus (HEV) Is Highly Specific for Diagnosis of Acute HEV Infection. J. Clin. Microbiol. 2005, 43, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Tian, D.; Zhang, Z.; Xiong, J.; Yuan, Q.; Ge, S.; Zhang, J.; Xia, N. Clinical Significance of Anti-HEV IgA in Diagnosis of Acute Genotype 4 Hepatitis E Virus Infection Negative for Anti-HEV IgM. Dig. Dis. Sci. 2009, 54, 2512–2518. [Google Scholar] [CrossRef]
- Chamot, E.; Hirschel, B.; Wintsch, J.; Robert, C.-F.; Gabriel, V.; Deglon, J.-J.; Yerly, S.; Perrin, L. Loss of antibodies against hepatitis C virus in HIV-seropositive intravenous drug users. AIDS 1990, 4, 1275–1278. [Google Scholar] [CrossRef]
- Gennery, A.R.; Cant, A.J.; Spickett, G.P.; Walshaw, D.; Hunter, S.; Hasan, A.; Hamilton, J.L.; Dark, J. Effect of immunosuppression after cardiac transplantation in early childhood on antibody response to polysaccharide antigen. Lancet 1998, 351, 1778–1781. [Google Scholar] [CrossRef]
- Eibl, M.M.; Wolf, H.M. Vaccination in patients with primary immune deficiency, secondary immune deficiency and autoimmunity with immune regulatory abnormalities. Immunotherapy 2015, 7, 1273–1292. [Google Scholar] [CrossRef] [Green Version]
- Vollmer, T.; Diekmann, J.; Eberhardt, M.; Knabbe, C.; Dreier, J. Hepatitis E in blood donors: Investigation of the natural course of asymptomatic infection, Germany, 2011. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendall, R.; Ellis, V.; Ijaz, S.; Thurairajah, P.; Dalton, H.R. Serological response to hepatitis E virus genotype 3 infection: IgG quantitation, avidity, and IgM response. J. Med. Virol. 2008, 80, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Lutz, E.; Ward, K.N.; Gray, J.J. Maturation of antibody avidity after primary human cytomegalovirus infection is delayed in immunosuppressed solid organ transplant patients. J. Med. Virol. 1994, 44, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Gärtner, B.C.; Kortmann, K.; Schäfer, M.; Mueller-Lantzsch, N.; Sester, U.; Kaul, H.; Pees, H. No Correlation in Epstein-Barr Virus Reactivation Between Serological Parameters and Viral Load. J. Clin. Microbiol. 2000, 38, 2458. [Google Scholar]
- Anastasiou, O.E.; Widera, M.; Verheyen, J.; Korth, J.; Gerken, G.; Helfritz, F.A.; Canbay, A.; Wedemeyer, H.; Ciesek, S. Clinical course and core variability in HBV infected patients without detectable anti-HBc antibodies. J. Clin. Virol. 2017, 93, 46–52. [Google Scholar] [CrossRef]
- Boccia, D.; Guthmann, J.-P.; Klovstad, H.; Hamid, N.; Tatay, M.; Ciglenecki, I.; Nizou, J.-Y.; Nicand, E.; Guerin, P. High Mortality Associated with an Outbreak of Hepatitis E among Displaced Persons in Darfur, Sudan. Clin. Infect. Dis. 2006, 42, 1679–1684. [Google Scholar] [CrossRef] [Green Version]
- Rayis, A.D.; Jumaa, A.M.; Gasim, G.; Karsany, M.S.; Adam, I. An outbreak of hepatitis E and high maternal mortality at Port Sudan, Eastern Sudan. Pathog. Glob. Heal. 2013, 107, 66–68. [Google Scholar] [CrossRef] [Green Version]
- Gurley, E.S.; Hossain, M.J.; Paul, R.C.; Sazzad, H.; Islam, M.S.; Parveen, S.; Faruque, L.I.; Husain, M.; Ara, K.; Jahan, Y.; et al. Outbreak of hepatitis E in urban Bangladesh resulting in maternal and perinatal mortality. Clin. Infect. Dis. 2014, 59, 658–665. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Immunocompetent Patients n = 13 | Immunosuppressed Patients n = 48 | p | |
|---|---|---|---|
| Age in years | 56.5 (46–61.5) | 51 (26–58) | 0.044 |
| Sex (m/f) | 12/1 | 35/13 | 0.264 |
| HEV RNA at diagnosis, IU/mL | 1.06 × 106 (0.41 × 106–5 × 106) | 2.27 × 106 (0.1 × 106–5 × 106) | 0.899 |
| ALT, IU/mL n = 58 | 2351 (1546–3443) | 138 (38–413) | <0.001 |
| ALT > ULN, n,% n = 59 | 13 (100%) | 38 (82.6%) | 0.180 |
| IgG, g/L n = 29 | 13.1 (9.9–14.6) | 8.9 (6.95–12.2) | 0.011 |
| ANA positivity, n, % n = 24 | 7 (63.6%) | 3 (23%) | 0.095 |
| Death/Survival | 4/9 | 2/46 | 0.016 |
| Liver failure (yes/no) | 6/7 | 1/47 | <0.001 |
| Chronification (yes/no) n = 45 | 0/5 | 13/27 | 0.301 |
| HEV IgM (S/CO) n = 60 | 6.35 (3.12–7.62) | 3.72 (0.84–6.68) | 0.056 |
| HEV IgG (S/CO) n = 60 | 5.49 (0.88–6.32) | 4.19 (0.51–5.59) | 0.355 |
| HEV IgA (S/CO) n = 34 | 4.63 (3.39–4.65) | 1.33 (0.32–3.59) | 0.012 |
| Total n = 61 | IgM+ n = 49 | IgM− n = 12 | p | |
|---|---|---|---|---|
| Age in years | 54 (38.5–59) | 54 (39–59) | 52.5 (36–58) | 0.842 |
| Sex (m/f) | 47/14 | 40/9 | 7/5 | 0.124 |
| HEV RNA at diagnosis, IU/mL | 1.82 × 106 (0.24 × 106–5 × 106) | 1.82 × 106 (0.24 × 106–5 × 106) | 3.2 × 106 (0.15*106–5 × 106) | 0.970 |
| HEV IgM (S/CO), n = 60 | 4.63 (1.54–6.76) | 5.96 (3.01–7.13) | 0.03 (0.03–0.12) | <0.001 |
| HEV IgG (S/CO), n = 60 | 4.25 (0.57–6.11) | 5.32 (2.87–6.35) | 0.26 (0.19–0.53) | <0.001 |
| HEV IgA (S/CO), n = 34 | 2.58 (0.41–4.56) | 3.59 (1.96–4.62) | 0.16 (0.11–0.32) | <0.001 |
| ALT, IU/mL n = 58 | 152 (82–914) | 181.5 (86–1021) | 134.5 (22–233) | 0.253 |
| ALT > ULN, n,% n = 59 | 51 (86.4%) | 44 (89.8%) | 7 (70%) | 0.125 |
| IgG, g/L n = 29 | 10.4 (7.8–12.9) n = 29 | 12.1 (9.2–13.7) n = 21 | 7.1 (6.6–8.9) n = 8 | 0.004 |
| ANA positivity, n, % n = 24 | 10 (41.7%) | 9 (56.3%) | 1 (12.5%) | 0.079 |
| Immunosuppression (y/n) | 48/13 | 37/12 | 11/1 | 0.432 |
| Neurological symptoms (y/n) | 1/60 | 1/48 | 0/12 | 1 |
| Outcome (survival vs. non survival) | 55/6 | 44/5 | 11/1 | 1 |
| Existing liver disease (y/n) | 15/46 | 11/38 | 4/8 | 0.467 |
| Presence of cirrhosis (y/n) | 5/56 | 5/44 | 0/12 | 0.573 |
| Liver failure (y/n) | 7/54 | 7/42 | 0/12 | 0.327 |
| Liver transplanted patient (y/n) | 9/52 | 7/42 | 2/10 | 1 |
| Chronification (y/n) | 13/32 | 9/27 | 4/5 | 0.411 |
| Ribavirin Therapy (y/n) | 14/47 | 13/36 | 1/11 | 0.264 |
| CMV reactivation (y/n) | 4/36 | 3/30 | 1/6 | 0.552 |
| EBV reactivation (y/n) | 20/18 | 18/14 | 2/4 | 0.395 |
| BKV reactivation (y/n) | 3/17 | 3/16 | 0/1 | 1 |
| Total | Immunocompetent Patients | Immunosuppressed Patients | |
|---|---|---|---|
| Sensitivity, % | 80.3 (67.8–89) | 92.9 (64.2–99.6) | 76.6 (61.6–87.2) |
| Specificity, % | 87 (84.9–88.9) | 89.4 (86.3–91.8) | 85 (81.8–87.7) |
| PPV | 0.26 (0.2–0.32) | 0.19 (0.11–0.31) | 0.29 (0.21–0.38) |
| NPV | 0.99 (0.98–0.99) | 1 (0.99–1) | 0.98 (0.96–0.99) |
| HEV RNA+ | ||
| HEV IgA− | HEV IgA+ or borderline | |
| HEV IgM−, n = 9 | 9 (100%) | 0 (0%) |
| HEV IgM+, n = 25 | 4 (16%) | 21 (84%) |
| HEV RNA− | ||
| HEV IgA− | HEV IgA+ or borderline | |
| HEV IgM+, n = 84 | 17 (20.2%) | 67 (79.8%) |
| HEV IgM−, n = 67 | 50 (74.6%) | 17 (25.4%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anastasiou, O.E.; Thodou, V.; Berger, A.; Wedemeyer, H.; Ciesek, S. Comprehensive Evaluation of Hepatitis E Serology and Molecular Testing in a Large Cohort. Pathogens 2020, 9, 137. https://doi.org/10.3390/pathogens9020137
Anastasiou OE, Thodou V, Berger A, Wedemeyer H, Ciesek S. Comprehensive Evaluation of Hepatitis E Serology and Molecular Testing in a Large Cohort. Pathogens. 2020; 9(2):137. https://doi.org/10.3390/pathogens9020137
Chicago/Turabian StyleAnastasiou, Olympia E., Viktoria Thodou, Annemarie Berger, Heiner Wedemeyer, and Sandra Ciesek. 2020. "Comprehensive Evaluation of Hepatitis E Serology and Molecular Testing in a Large Cohort" Pathogens 9, no. 2: 137. https://doi.org/10.3390/pathogens9020137
APA StyleAnastasiou, O. E., Thodou, V., Berger, A., Wedemeyer, H., & Ciesek, S. (2020). Comprehensive Evaluation of Hepatitis E Serology and Molecular Testing in a Large Cohort. Pathogens, 9(2), 137. https://doi.org/10.3390/pathogens9020137