
Characterization of a 3D Printed Endovascular Magnetic Catheter

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
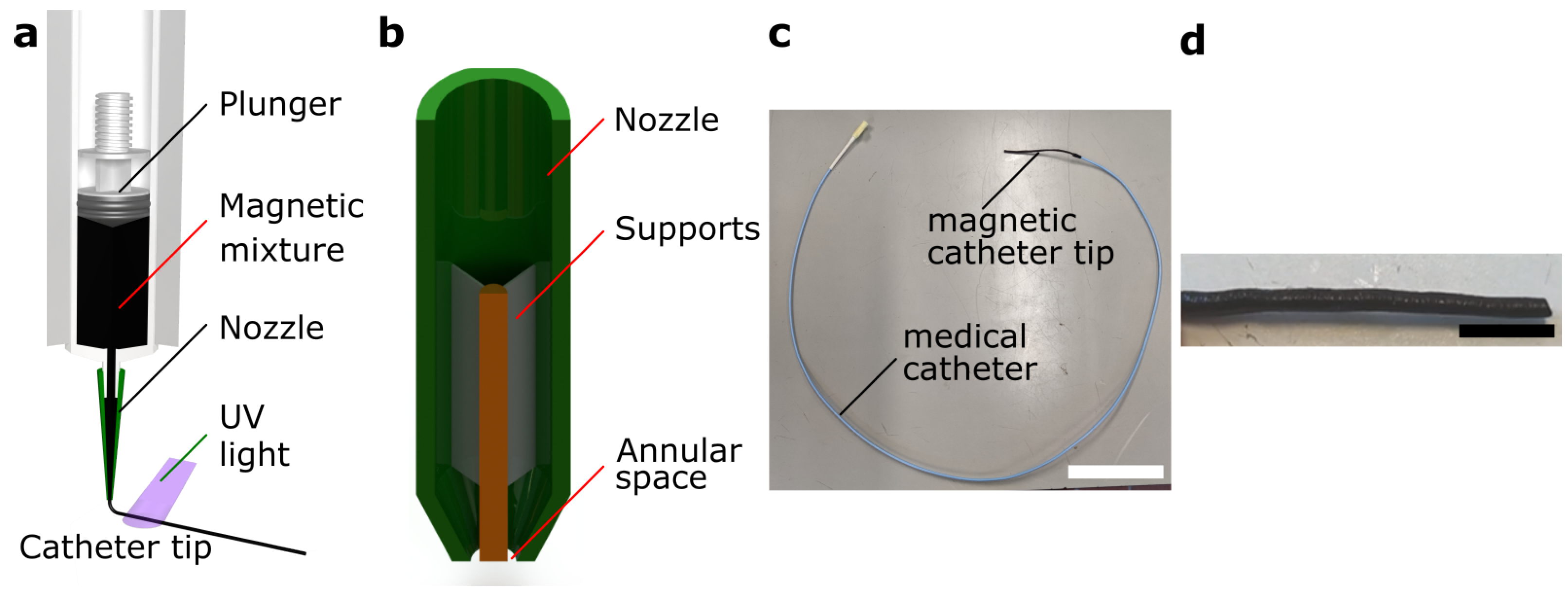
- Custom fabrication of a soft hollow magnetic catheter tip using mold-free extrusion.
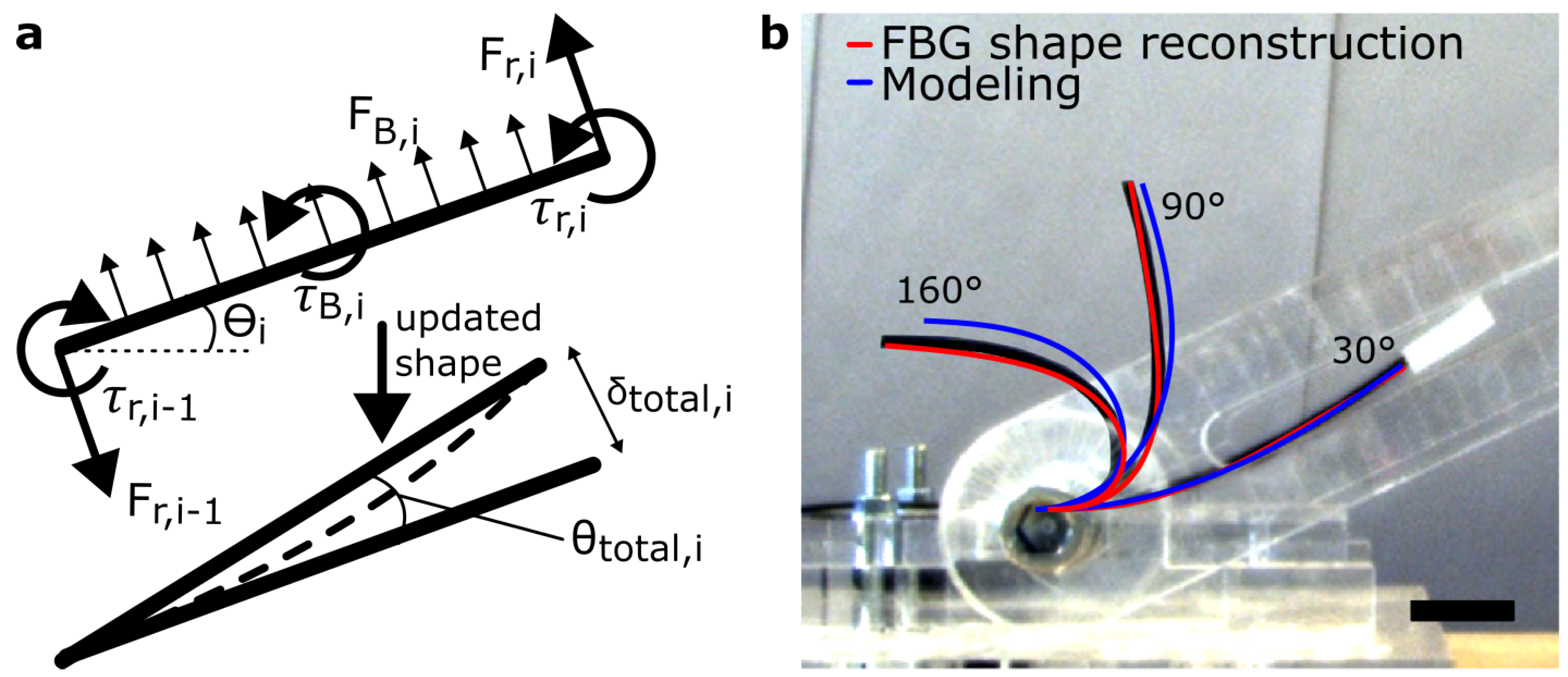
- Numerical modeling of the steerable tip bending and its verification, required for the prediction of its bending.
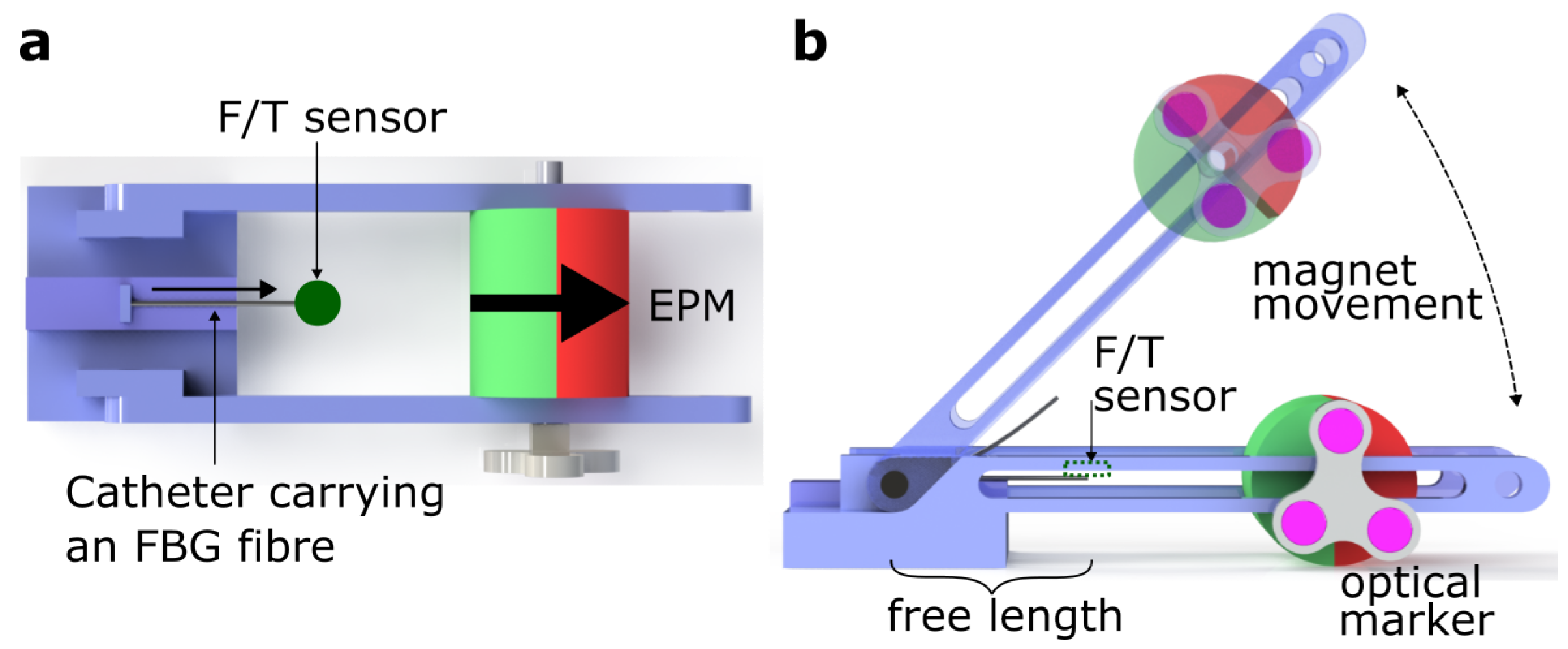
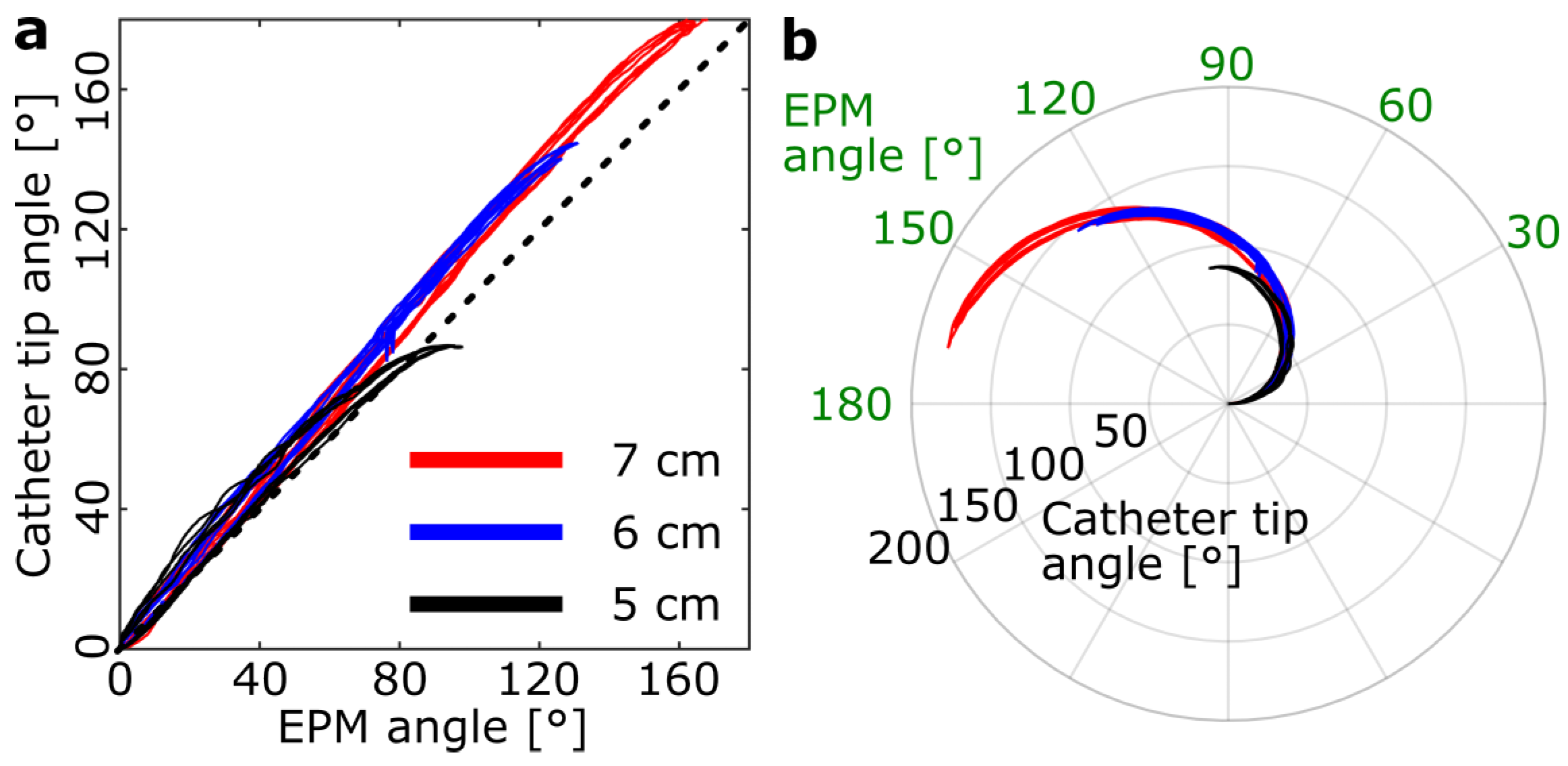
- Characterization of bending hysteresis and bending forces. Through such characterizations, a control strategy can be developed.
2. Fabrication of the Magnetic Catheter
3. Mathematical Modeling of Catheter Bending
3.1. Fields around an External Permanent Magnet
3.2. Modeling the Soft Magnetic Catheter
4. Bending Characterization of the Magnetic Catheter
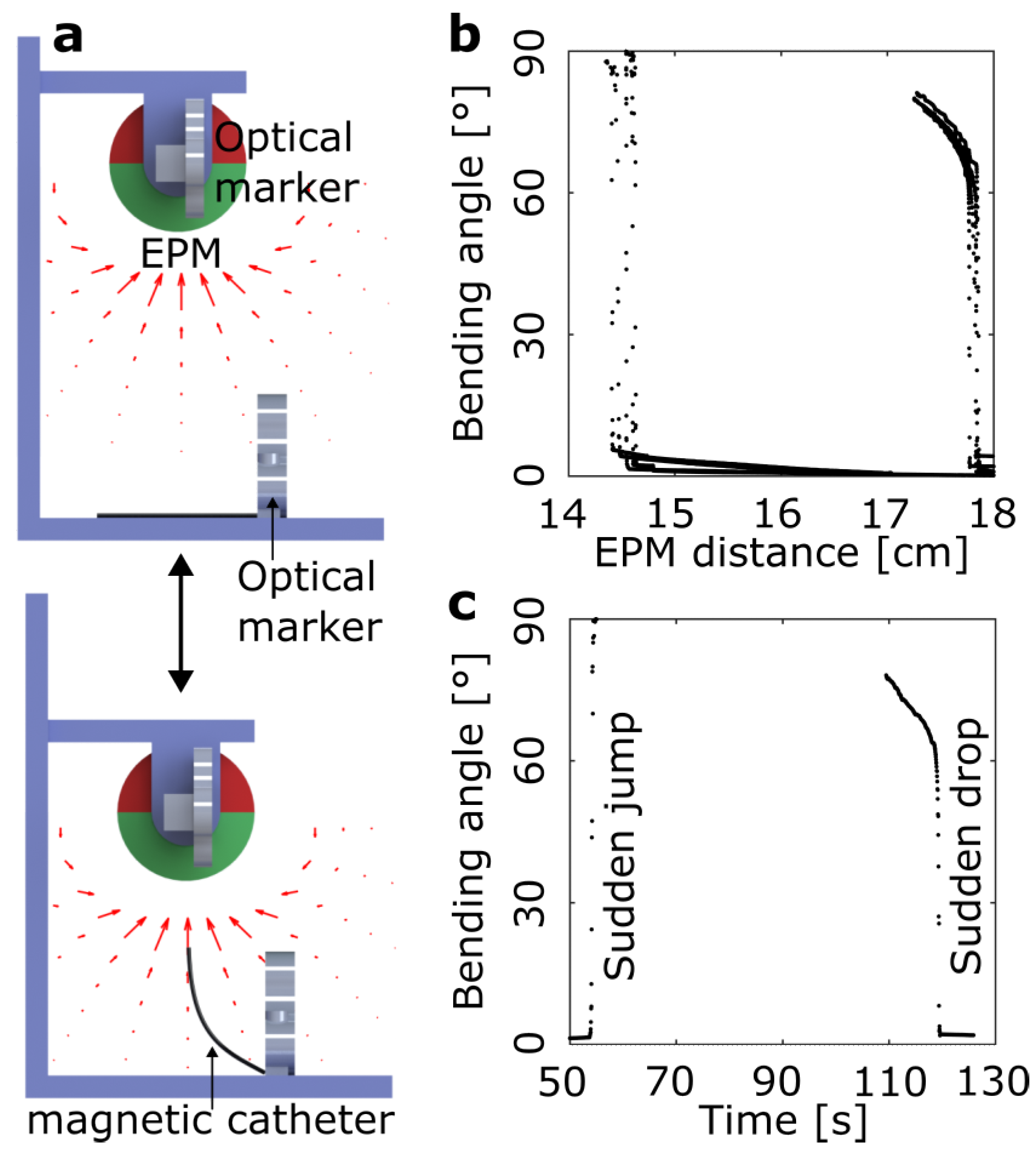
4.1. Sensors
4.2. Bending Hysteresis
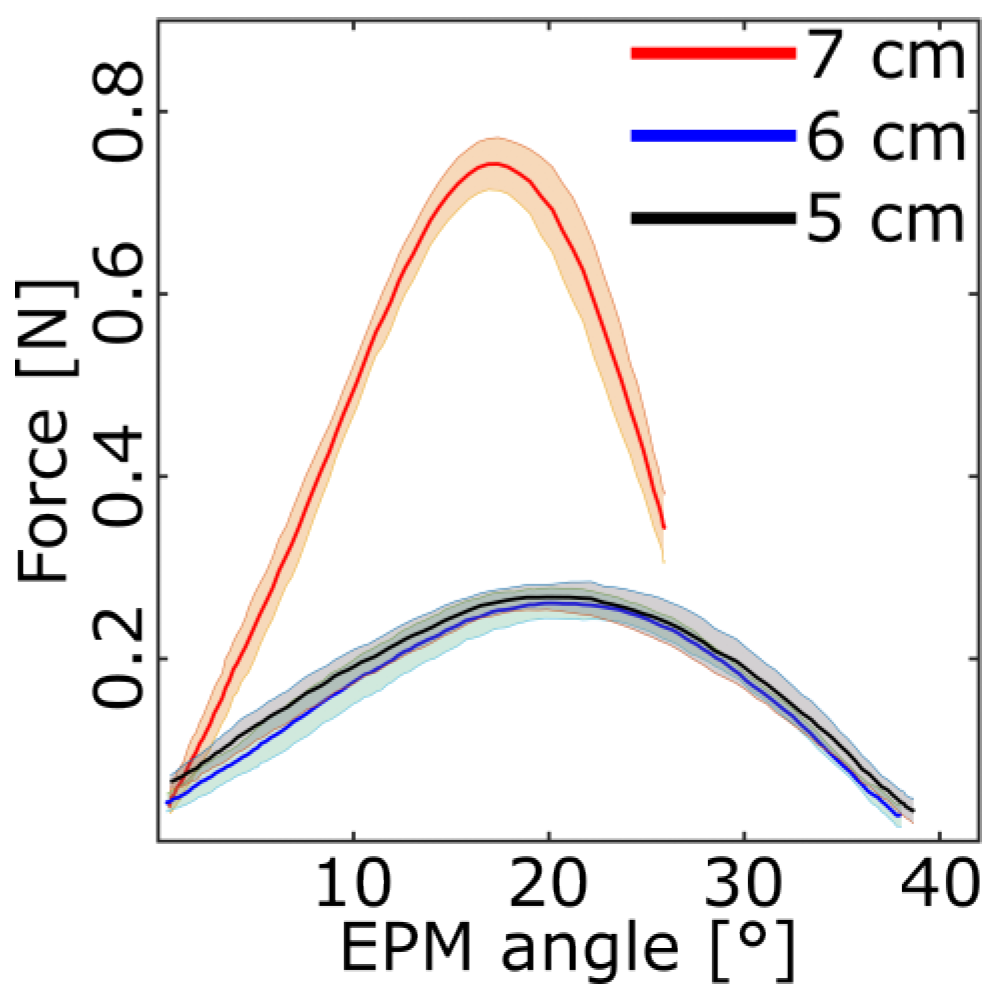
4.3. Bending Forces
4.4. Dynamic Response
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 3D | Three Dimensional |
| DoFs | Degrees of Freedom |
| EM | Electro-Magnetic |
| EPM | External Permanent Magnet |
| FBG | Fiber Bragg Grating |
| F/T | Force/Torque |
| IVUS | Intravascular Ultrasound |
| MC | magnetic catheter |
| MRI | Magnetic Resonance Imaging |
| NdFeB | Neodymium Iron Boron |
| PAM | Pneumatic Artificial Muscle |
| RMSE | root mean square error |
| ROS | Robotic Operative System |
| UV | Ultra-violet |
References
- Hoffman, S.N.; TenBrook, J.A.; Wolf, M.P.; Wong, J.B.; Pauker, S.G.; Salem, D.N. A meta-analysis of randomized controlled trials comparing coronary artery bypass graft with percutaneous transluminal coronary angioplasty: One- to eight-year outcomes. J. Am. Coll. Cardiol. 2003, 41, 1293–1304. [Google Scholar] [CrossRef] [PubMed]
- Guez, D.; Hansberry, D.R.; Gonsalves, C.F.; Eschelman, D.J.; Parker, L.; Rao, V.M.; Levin, D.C. Recent Trends in Endovascular and Surgical Treatment of Peripheral Arterial Disease in the Medicare Population. Am. J. Roentgenol. 2020, 214, 962–966. [Google Scholar] [CrossRef] [PubMed]
- O’Laughlin, M.P.; Perry, S.B.; Lock, J.E.; Mullins, C.E. Use of endovascular stents in congenital heart disease. Circulation 1991, 83, 1923–1939. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Ren, S.; Yang, Y.; Liu, J.; Ye, Z.; Lin, F. Intravenous Catheter-Guided Laser Ablation: A Novel Alternative for Branch Varicose Veins. Int. Surg. 2011, 96, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Farola Barata, B.; Tran, P.T.; Borghesan, G.; McCutcheon, K.; Dall’Alba, D.; Fiorini, P.; Vander Sloten, J.; Poorten, E.V. IVUS-Based Local Vessel Estimation for Robotic Intravascular Navigation. IEEE Robot. Autom. Lett. 2021, 6, 8102–8109. [Google Scholar] [CrossRef]
- Gunduz, S.; Albadawi, H.; Oklu, R. Robotic Devices for Minimally Invasive Endovascular Interventions: A New Dawn for Interventional Radiology. Adv. Intell. Syst. 2021, 3, 2000181. [Google Scholar] [CrossRef]
- Ali, A.; Plettenburg, D.H.; Breedveld, P. Steerable Catheters in Cardiology: Classifying Steerability and Assessing Future Challenges. IEEE Trans. Biomed. Eng. 2016, 63, 679–693. [Google Scholar] [CrossRef]
- Agilis Nxt Steerable Introducer. Available online: https://www.cardiovascular.abbott/us/en/hcp/products/electrophysiology/access-introducers/agilis-nxt/about.html (accessed on 15 October 2022).
- Uncovering Treatment Pathways with Robotic Assisted Procedures. Available online: https://www.jnjmedtech.com/en-US/product-family/monarch (accessed on 15 October 2022).
- Dario, P.; Valleggi, R.; Pardini, M.; Sabatini, A. A miniature device for medical intracavitary intervention. In Proceedings of the [1991] Proceedings, IEEE Micro Electro Mechanical Systems, Nara, Japan, 30 January–2 February 1991; pp. 171–175. [Google Scholar]
- Kalita, B.; Leonessa, A.; Dwivedy, S.K. A Review on the Development of Pneumatic Artificial Muscle Actuators: Force Model and Application. Actuators 2022, 11, 288. [Google Scholar] [CrossRef]
- Gopesh, T.; Wen, J.H.; Santiago-Dieppa, D.; Yan, B.; Pannell, J.S.; Khalessi, A.; Norbash, A.; Friend, J. Soft robotic steerable microcatheter for the endovascular treatment of cerebral disorders. Sci. Robot. 2021, 6, eabf0601. [Google Scholar] [CrossRef]
- Webster, R.J.; Romano, J.M.; Cowan, N.J. Mechanics of Precurved-Tube Continuum Robots. IEEE Trans. Robot. 2009, 25, 67–78. [Google Scholar] [CrossRef]
- Hu, X.; Chen, A.; Luo, Y.; Zhang, C.; Zhang, E. Steerable catheters for minimally invasive surgery: A review and future directions. Comput. Assist. Surg. 2018, 23, 21–41. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Yu, J.; Yan, X.; Choi, H.; Zhang, L. Magnetic Actuation Based Motion Control for Microrobots: An Overview. Micromachines 2015, 6, 1346–1364. [Google Scholar] [CrossRef]
- El-Atab, N.; Mishra, R.B.; Al-Modaf, F.; Joharji, L.; Alsharif, A.A.; Alamoudi, H.; Diaz, M.; Qaiser, N.; Hussain, M.M. Soft Actuators for Soft Robotic Applications: A Review. Adv. Intell. Syst. 2020, 2, 2000128. [Google Scholar] [CrossRef]
- Choi, M.S.; Oh, Y.S.; Jang, S.W.; Kim, J.H.; Shin, W.S.; Youn, H.J.; Jung, W.S.; Lee, M.Y.; Seong, K.B. Comparison of Magnetic Navigation System and Conventional Method in Catheter Ablation of Atrial Fibrillation: Is Magnetic Navigation System Is More Effective and Safer Than Conventional Method? Korean Circ. J. 2011, 41, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Schenck, J.F. Safety of Strong, Static Magnetic Fields. J. Magn. Reson. Imaging 2000, 12, 2–19. [Google Scholar] [CrossRef] [PubMed]
- Tillander, H. Magnetic Guidance of a Catheter with Articulated Steel Tip. Acta Radiol. 1951, 35, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Faddis, M.N.; Blume, W.; Finney, J.; Hall, A.; Rauch, J.; Sell, J.; Bae, K.T.; Talcott, M.; Lindsay, B. Novel, Magnetically Guided Catheter for Endocardial Mapping and Radiofrequency Catheter Ablation. Circulation 2002, 106, 2980–2985. [Google Scholar] [CrossRef]
- Pittiglio, G.; Lloyd, P.; da Veiga, T.; Onaizah, O.; Pompili, C.; Chandler, J.H.; Valdastri, P. Patient-Specific Magnetic Catheters for Atraumatic Autonomous Endoscopy. Soft Robot. 2022, 9, 1120–1133. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration (FDA). Class 2 Medical Device Recalls: Cronus Endovascular Guidewires (510(K) Number: K021363, FDA, 2004). Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfRES/res.cfm?start_search=1&knumber=K021363 (accessed on 16 October 2022).
- Kim, Y.; Parada, G.A.; Liu, S.; Zhao, X. Ferromagnetic soft continuum robots. Sci. Robot. 2019, 4, eaax7329. [Google Scholar] [CrossRef]
- Cianchetti, M.; Laschi, C.; Menciassi, A.; Dario, P. Biomedical applications of soft robotics. Nat. Rev. Mater. 2018, 3, 143–153. [Google Scholar] [CrossRef]
- Ansari, M.H.D.; Iacovacci, V.; Pane, S.; Ourak, M.; Borghesan, G.; Tamadon, I.; Vander Poorten, E.; Menciassi, A. 3D Printing of Small-Scale Soft Robots with Programmable Magnetization. Adv. Funct. Mater. 2023, 33, 2211918. [Google Scholar] [CrossRef]
- Petruska, A.J.; Abbott, J.J. Optimal Permanent-Magnet Geometries for Dipole Field Approximation. IEEE Trans. Magn. 2013, 49, 811–819. [Google Scholar] [CrossRef]
- Ha, X.T.; Ourak, M.; Al-Ahmad, O.; Wu, D.; Borghesan, G.; Menciassi, A.; Vander Poorten, E. Robust Catheter Tracking by Fusing Electromagnetic Tracking, Fiber Bragg Grating and Sparse Fluoroscopic Images. IEEE Sens. J. 2021, 21, 23422–23434. [Google Scholar] [CrossRef]
- Quigley, M.; Conley, K.; Gerkey, B.; Faust, J.; Foote, T.; Leibs, J.; Wheeler, R.; Ng, A.Y. ROS: An open-source Robot Operating System. In Proceedings of the ICRA Workshop on Open Source Software, Kobe, Japan, 12–17 May 2009; Volume 3, p. 5. [Google Scholar]
- Kaladji, A.; Dumenil, A.; Mahé, G.; Castro, M.; Cardon, A.; Lucas, A.; Haigron, P. Safety and Accuracy of Endovascular Aneurysm Repair Without Pre-operative and Intra-operative Contrast Agent. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 255–261. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ansari, M.H.D.; Ha, X.T.; Ourak, M.; Borghesan, G.; Iacovacci, V.; Vander Poorten, E.; Menciassi, A. Characterization of a 3D Printed Endovascular Magnetic Catheter. Actuators 2023, 12, 409. https://doi.org/10.3390/act12110409
Ansari MHD, Ha XT, Ourak M, Borghesan G, Iacovacci V, Vander Poorten E, Menciassi A. Characterization of a 3D Printed Endovascular Magnetic Catheter. Actuators. 2023; 12(11):409. https://doi.org/10.3390/act12110409
Chicago/Turabian StyleAnsari, Mohammad Hasan Dad, Xuan Thao Ha, Mouloud Ourak, Gianni Borghesan, Veronica Iacovacci, Emmanuel Vander Poorten, and Arianna Menciassi. 2023. "Characterization of a 3D Printed Endovascular Magnetic Catheter" Actuators 12, no. 11: 409. https://doi.org/10.3390/act12110409
APA StyleAnsari, M. H. D., Ha, X. T., Ourak, M., Borghesan, G., Iacovacci, V., Vander Poorten, E., & Menciassi, A. (2023). Characterization of a 3D Printed Endovascular Magnetic Catheter. Actuators, 12(11), 409. https://doi.org/10.3390/act12110409