
Pharyngeal Colonization by Kingella kingae, Transmission, and Pathogenesis of Invasive Infections: A Narrative Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. Kingella kingae: An Oropharyngeal Resident
3.2. Mechanism of Colonization
3.3. Immunity to Colonization and Infection
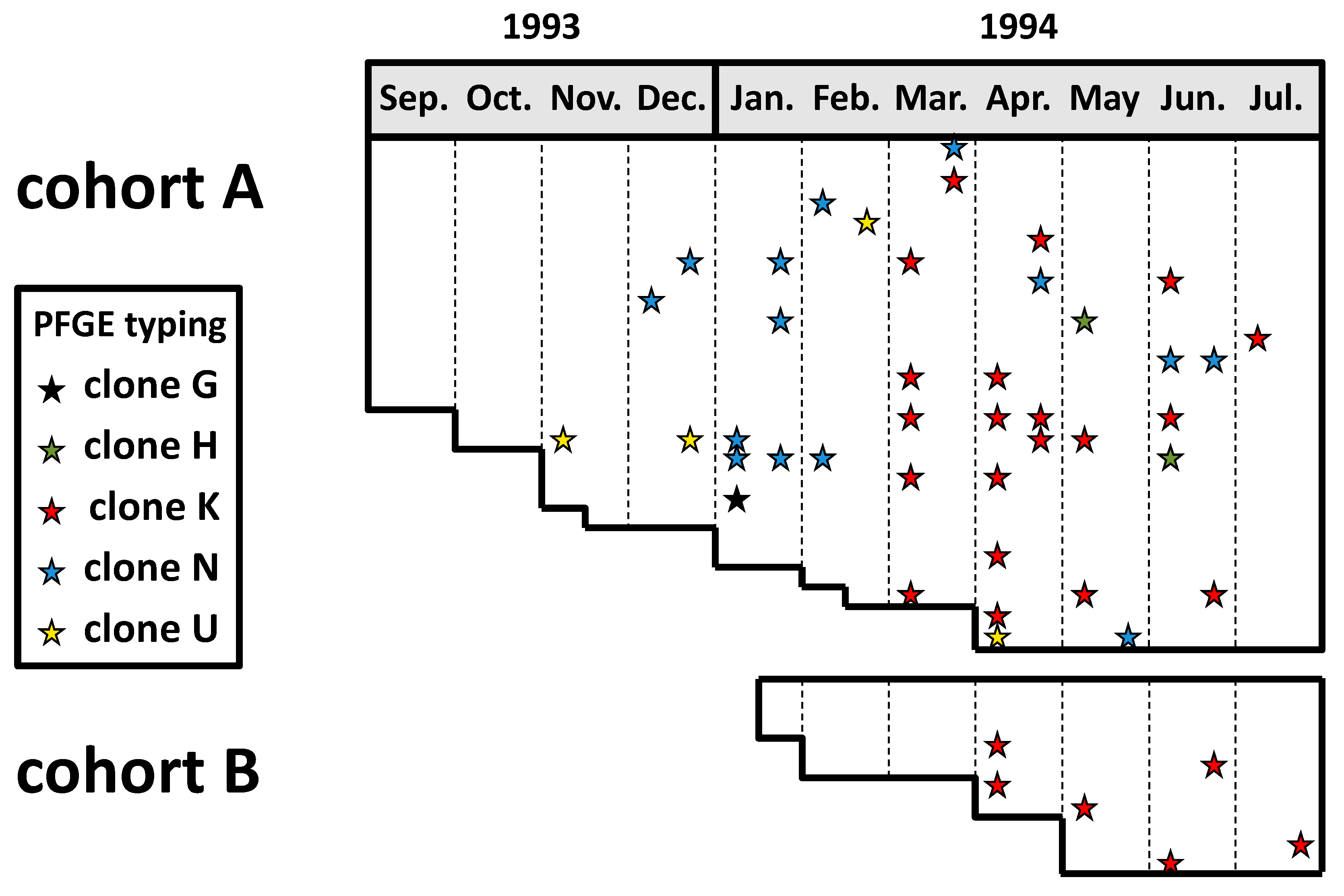
3.4. Colonization and Transmission
3.5. Detection of K. kingae Colonization
3.6. Risk Factors for Carriage and Transmission
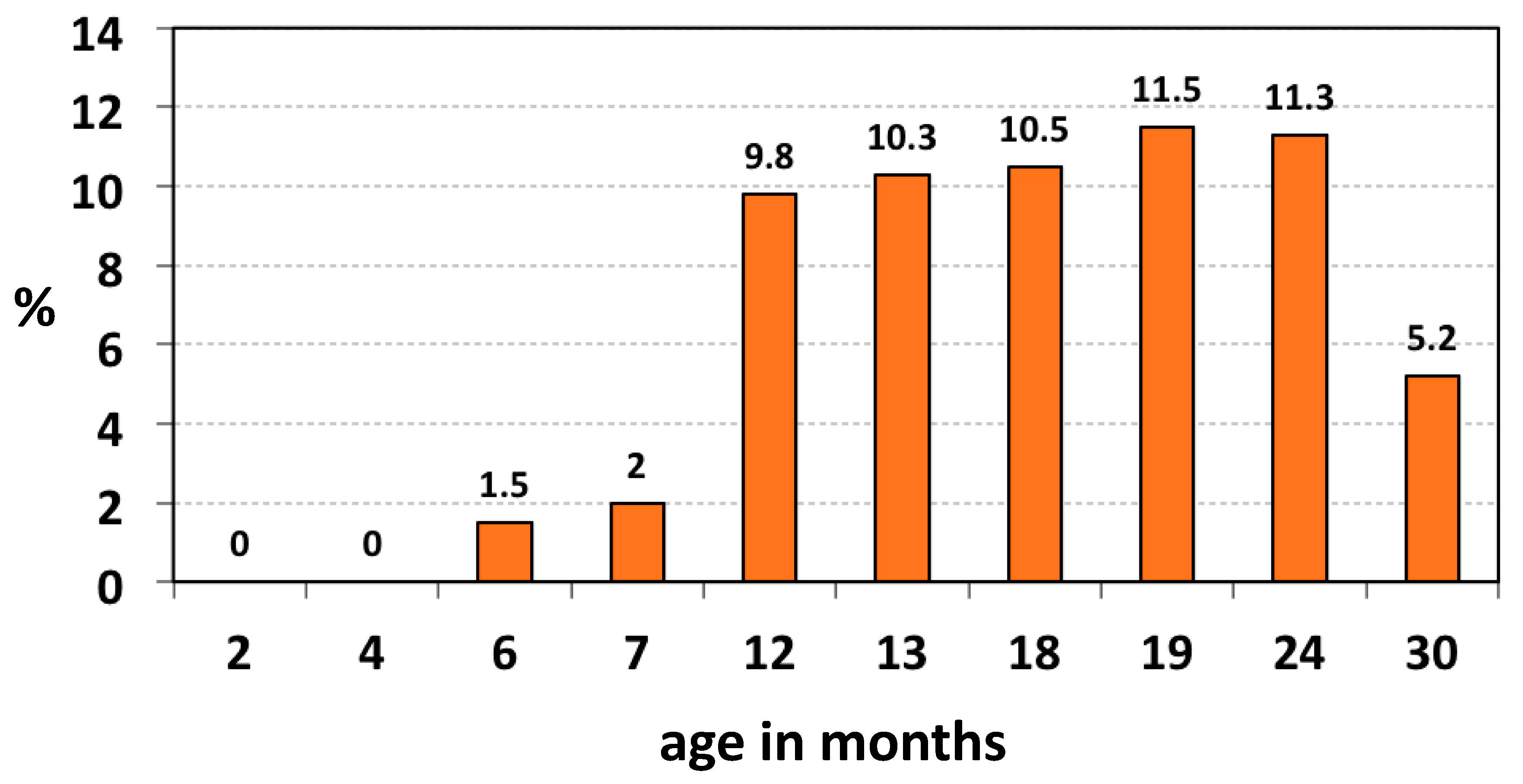
3.6.1. Age
3.6.2. Season
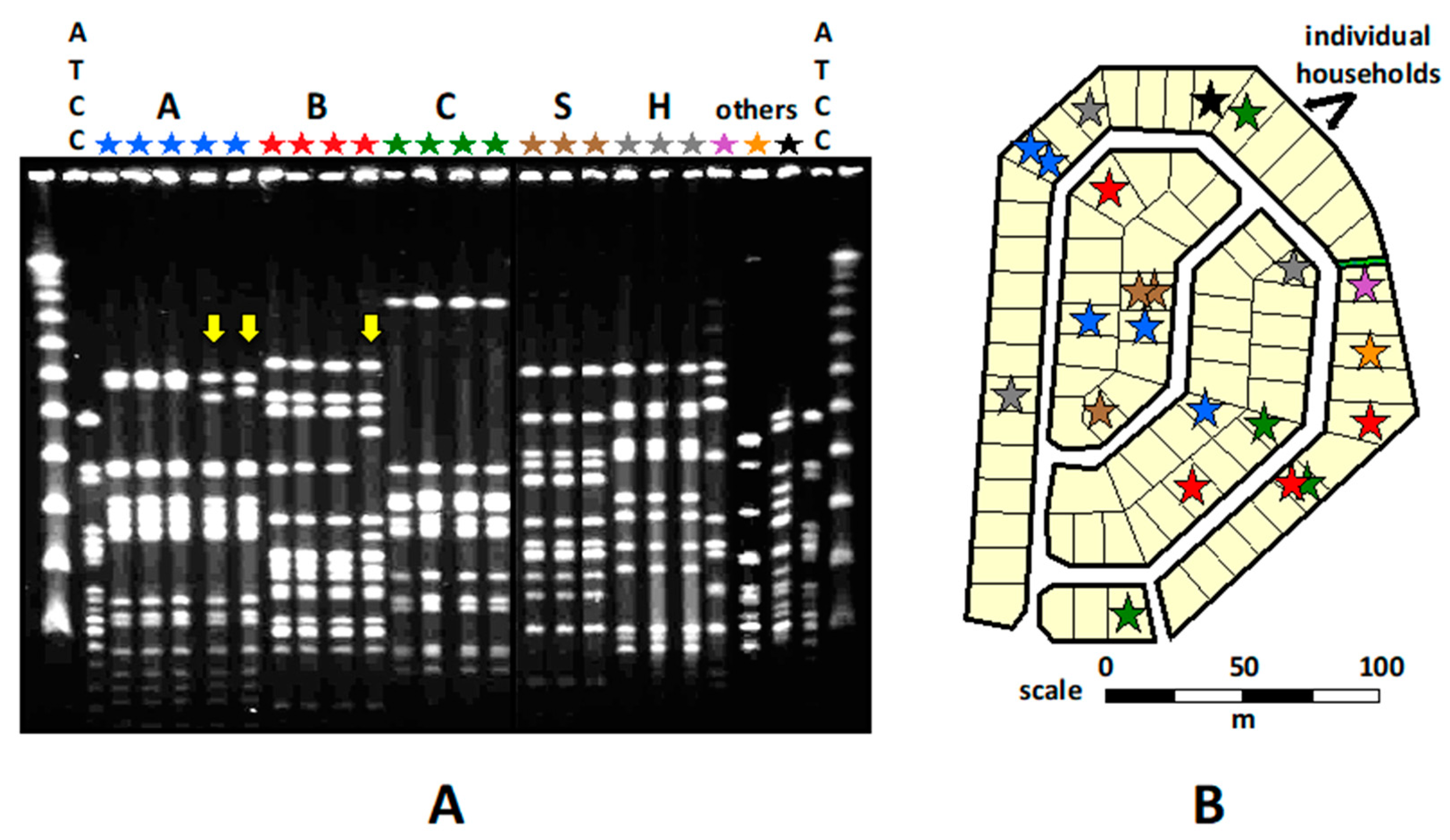
3.6.3. Living Conditions, Prevalence, and Transmission
3.6.4. Daycare Center Attendance
3.6.5. Family Transmission
3.6.6. Carriage in Different Populations
3.7. Colonization and Invasive Disease
3.7.1. Carriage Density and Disease
3.7.2. Kingella kingae Colonization: A Stepping Stone of Invasive Infections
3.7.3. Viral Infections and K. kingae Disease
3.7.4. Strain Diversity
3.7.5. Virulence of Carried Strains
3.7.6. Oropharyngeal Colonization and the Diagnosis of Invasive K. kingae Disease
4. Conclusions
Funding
Conflicts of Interest
References
- García-Rodríguez, J.Á.; Martínez, M.J.F. Dynamics of nasopharyngeal colonization by potential respiratory pathogens. J. Antimicrob. Chemother. 2002, 50 (Suppl. S2), 59–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weintraub, A. Immunology of bacterial polysaccharide antigens. Carbohydr. Res. 2003, 338, 2539–2547. [Google Scholar] [CrossRef] [PubMed]
- Samuelson, A.; Freijd, A.; Jonasson, J.; Lindberg, A.A. Turnover of nonencapsulated Haemophilus influenzae in the nasopharynges of otitis-prone children. J. Clin. Microbiol. 1995, 33, 2027–2031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sethi, S.; Hill, S.L.; Murphy, T.F. Serum antibodies to outer membrane proteins (OMPs) of Moraxella (Branhamella) catarrhalis in patients with bronchiectasis: Identification of OMP B1 as an important antigen. Infect. Immun. 1995, 63, 1516–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagupsky, P.; Dagan, R.; Prajgrod, F.; Merires, M. Respiratory carriage of Kingella kingae among healthy children. Pediatr. Infect. Dis. J. 1995, 14, 673–677. [Google Scholar] [CrossRef]
- Amit, U.; Flaishmakher, S.; Dagan, R.; Porat, N.; Yagupsky, P. Age-dependent carriage of Kingella kingae in young children and turnover of colonizing strains. J. Pediatr. Infect. Dis. Soc. 2013, 3, 160–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehl-Fie, T.E.; Miller, S.E.; St. Geme, J.W., 3rd. Kingella kingae Expresses type IV Pili that mediate adherence to respiratory epithelial and synovial cells. J. Bacteriol. 2008, 190, 7157–7163. [Google Scholar] [CrossRef] [Green Version]
- Porsch, E.A.; Johnson, M.D.L.; Broadnax, A.D.; Garrett, C.K.; Redinbo, M.R.; St. Geme, J.W., 3rd. Calcium Binding Properties of the Kingella kingae PilC1 and PilC2 proteins have differential effects on type IV pilus-mediated adherence and twitching motility. J. Bacteriol. 2012, 195, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Kehl-Fie, T.E.; Porsch, E.A.; Miller, S.E.; St. Geme, J.W., 3rd. Expression of Kingella kingae type IV pili is regulated by θ54, PilS, and PilR. J. Bacteriol. 2009, 191, 4976–4986. [Google Scholar] [CrossRef] [Green Version]
- Kehl-Fie, T.E.; Porsch, E.A.; Yagupsky, P.; Grass, E.A.; Obert, C.; Benjamin, D.K., Jr.; St. Geme, J.W., 3rd. Examination of type IV pilus expression and pilus-associated phenotypes in Kingella kingae clinical isolates. Infect. Immun. 2010, 78, 1692–1699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porsch, E.A.; Kehl-Fie, T.E.; St. Geme, J.W., 3rd. Modulation of Kingella kingae Adherence to human epithelial cells by type IV Pili, capsule, and a novel trimeric autotransporter. mBio 2012, 3, e00372-12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagupsky, P. Kingella kingae: Carriage, transmission, and disease. Clin. Microbiol. Rev. 2015, 28, 54–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slonim, A.; Steiner, M.; Yagupsky, P. Immune response to invasive Kingella kingae infections, age-related incidence of disease, and levels of antibody to outer-membrane proteins. Clin. Infect. Dis. 2003, 37, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Starr, K.F.; Porsch, E.A.; Heiss, C.; Black, I.; Azadi, P.; St. Geme, J.W., 3rd. Characterization of the Kingella kingae polysaccharide capsule and exopolysaccharide. PLoS ONE 2013, 8, e75409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, V.L.; Porsch, E.A.; St. Geme, J.W., 3rd. Kingella kingae surface polysaccharides promote resistance to neutrophil phagocytosis and killing. mBio 2019, 10, e00631-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, V.L.; Porsch, E.A.; St. Geme, J.W., 3rd. Kingella kingae surface polysaccharides promote resistance to human serum and virulence in a juvenile rat model. Infect. Immun. 2018, 86, e00100-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slonim, A.; Walker, E.S.; Mishori, E.; Porat, N.; Dagan, R.; Yagupsky, P. Person-to-person transmission of Kingella kingae among day care center attendees. J. Infect Dis. 1998, 78, 1843–1846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amit, U.; Dagan, R.; Porat, N.; Trefler, R.; Yagupsky, P. Epidemiology of invasive Kingella kingae infections in two distinct pediatric populations cohabiting in one geographic area. Pediatr. Infect. Dis. J. 2012, 31, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Yagupsky, P.; Weiss-Salz, I.; Fluss, R.; Freedman, L.; Peled, N.; Trefler, R.; Porat, N.; Dagan, R. Dissemination of Kingella kingae in the community and long-term persistence of invasive clones. Pediatr. Infect. Dis. J. 2009, 28, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Yagupsky, P.; Merires, M.; Bahar, J.; Dagan, R. Evaluation of a novel vancomycin-containing medium for primary isolation of Kingella kingae from upper respiratory tract specimens. J. Clin. Microbiol. 1995, 33, 426–427. [Google Scholar] [CrossRef] [Green Version]
- Basmaci, R.; Ilharreborde, B.; Bidet, P.; Doit, C.; Lorrot, M.; Mazda, K.; Bingen, E.; Bonacorsi, S. Isolation of Kingella kingae in the oropharynx during K. kingae arthritis on children. Clin. Microbiol. Infect. 2012, 18, e134–e136. [Google Scholar] [CrossRef] [PubMed]
- Yagupsky, P.; El Houmami, N.; Fournier, P.-E. Outbreaks of invasive Kingella kingae infections in daycare facilities: Approach to investigation and management. J. Pediatr. 2017, 182, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Seña, A.C.; Seed, P.; Nicholson, B.; Joyce, M.; Cunningham, C.K. Kingella kingae endocarditis and a cluster investigation among daycare attendeES. Pediatr. Infect. Dis. J. 2010, 29, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Chometon, S.; Benito, Y.; Chaker, M.; Boisset, S.S.; Ploton, C.; Bérard, J.; Vandenesch, F.; Freydiere, A.M. Specific real-time polymerase chain reaction places Kingella kingae as the most common cause of osteoarticular infections in young children. Pediatr. Infect. Dis. J. 2007, 26, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Ceroni, D.; Anderson della Llana, R.; Kherad, O.; Lascombes, P.; Renzi, G.; Manzano, S.; Cherkaoui, A.; Schrenzel, J. Comparing the oropharyngeal colonizationisation density of Kingella kingae between asymptomatic carriers and children with invasive osteoarticular infections. Pediatr. Infect. Dis. J. 2013, 32, 412–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosey, A.L.; Abachin, E.; Quesnes, G.; Cadilhac, C.; Pejin, Z.; Glorion, C.; Berche, P.; Ferroni, A. Development of a braod-range 16S rDNA real-time PCR for the diagnosis of septic arthritis in children. J. Microbiol. Methods. 2007, 68, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Moumile, K.; Merckx, J.; Glorion, C.; Berche, P.; Ferroni, A. Osteoarticular infections caused by Kingella kingae in children: Contribution of polymerase chain reaction to the microbiologic diagnosis. Pediatr. Infect. Dis. J. 2003, 22, 837–839. [Google Scholar] [CrossRef]
- El Houmami, N.; Durand, G.A.; Bzdrenga, J.; Darmon, A.; Minodier, P.; Seligmann, H.; Raoult, D.; Fournier, P.-E. A new highly sensitive and specific real-time pcr assay targeting the malate dehydrogenase gene of Kingella kingae and application to 201 pediatric clinical specimens. J. Clin. Microbiol. 2018, 56, e00505-18. [Google Scholar] [CrossRef] [Green Version]
- Ceroni, D.; Cherkaoui, A.; Kaelin, A.; Schrenzel, J. Kingella kingae spondylodiscitis in young children: Toward a new approach for bacteriological investigations? A preliminary report. J. Child. Orthop. 2010, 4, 173–175. [Google Scholar] [CrossRef] [Green Version]
- Juchler, C.; Spyropoulou, V.; Wagner, N.; Merlini, L.; Dhouib, A.; Manzano, S.; Tabard-Fougère, A.; Samara, E.; Ceroni, D. The contemporary bacteriologic epidemiology of osteoarticular infections in children in Switzerland. J. Pediatr. 2018, 194, 190–196.e1. [Google Scholar] [CrossRef]
- Masud, S.; Greenman, J.; Mulpuri, K.; Hasan, M.R.; David, M.; Goldfarb, D.M.; Tilley, P.; Gadkar, V.J.; Al-Rawahi, G.N. Asymptomatic pharyngeal carriage of Kingella kingae among young children in Vancouver, British Columbia, Canada. Pediatr. Infect. Dis. J. 2019, 38, 990–993. [Google Scholar] [CrossRef] [PubMed]
- Lehours, P.; Freydière, A.M.; Richer, O.; Burucoa, C.; Boisset, S.; Lanotte, P.; Prère, M.F.; Ferroni, A.; Lafuente, C.; Vandenesch, F.; et al. The rtxA toxin gene of Kingella kingae: A pertinent target for molecular diagnosis of osteo- articular infections. J. Clin. Microbiol. 2011, 49, 1245–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amit, U.; Dagan, R.; Yagupsky, P. Prevalence of pharyngeal carriage of Kingella kingae in young children and risk factors for colonization. Pediatr. Infect. Dis. J. 2013, 32, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Dubnov-Raz, G.; Ephros, M.; Garty, B.Z.; Schlesinger, Y.; Maayan-Metzger, A.; Hasson, J.; Kassis, I.; Schwartz-Harari, O.; Yagupsky, P. Invasive pediatric Kingella kingae infections: A nationwide collaborative study. Pediatr. Infect. Dis. J. 2010, 29, 639–643. [Google Scholar] [CrossRef]
- Kampouroglou, G.; Dubois-Ferrière, V.; De La Llana, R.A.; Renzi, G.; Manzano, S.; Cherkaoui, A.; Schrenzel, J.; Ceroni, D. A Prospective study of intrafamilial oropharyngeal transmission of Kingella kingae. Pediatr. Infect. Dis. J. 2014, 33, 410–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagupsky, P.; Peled, N.; Katz, O. Epidemiological features of invasive Kingella kingae infections and respiratory carriage of the organism. J. Clin. Microbiol. 2002, 40, 4180–4184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claesson, B.; Falsen, E.; Kjellman, B. Kingella kingae infections: A review and a presentation of data from 10 Swedish cases. Scand. J. Infect. Dis. 1985, 17, 233–243. [Google Scholar] [CrossRef] [PubMed]
- De La Llana, R.A.; Dubois-Ferriere, V.; Maggio, A.; Cherkaoui, A.; Manzano, S.; Renzi, G.; Hibbs, J.; Schrenzel, J.; Ceroni, D. Oropharyngeal Kingella kingae carriage in children: Characteristics and correlation with osteoarticular infections. Pediatr. Res. 2015, 78, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J. Infectious diseases in schools and child care facilities. Pediatr. Rev. 2001, 22, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.V.; McCracken, G.H., Jr.; Moore, B.S.; Gulig, P.A.; Hansen, H.J. Haemophilus influenzae type b disease after rifampin prophylaxis in a day care center: Possible reasons for its failure. Pediatr. Infect. Dis. J. 1983, 2, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Samuels, M.E.; Shi, L.; Baker, S.L.; Glover, S.H.; Sanders, J.M. Child day care risks of common infectious diseases revisited. Child Care Health Dev. 2004, 30, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Huskins, W.C. Transmission and control of infections in out-of-home child care. Pediatr. Infect. Dis. J. 2000, 19, S106–S110. [Google Scholar] [CrossRef] [PubMed]
- Osterholm, M.T. Infectious disease in child day care: An overview. Pediatrics 1994, 94, 987–990. [Google Scholar] [CrossRef] [PubMed]
- Kiang, K.M.; Ogunmodede, F.; Juni, B.A.; Boxrud, D.J.; Glennen, A.; Bartkus, J.M.; Cebelinski, E.A.; Harriman, K.; Koop, S.; Faville, R.; et al. Outbreak of osteomyelitis/septic arthritis caused by Kingella kingae among child care center attendees. Pediatrics 2005, 116, e206–e213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagupsky, P.; Erlich, Y.; Ariela, S.; Trefler, R.; Porat, N. Outbreak of Kingella kingae skeletal system infections in children in daycare. Pediatr. Infect. Dis. J. 2006, 25, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Bidet, P.; Collin, E.; Basmaci, R.; Courroux, C.; Prisse, V.; Dufour, V.; Bingen, E.; Grimprel, E.; Bonacorsi, S. Investigation of an outbreak of osteoarticular infections caused by Kingella kingae in a childcare center using molecular techniques. Pediatr. Infect. Dis. J. 2013, 32, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Lillebo, K.; Breistein, R.I.; Aamas, J.V.; Kommedal, O. The first report on epidemiology of oropharyngeal Kingella kingae carriage in Scandinavian children: K. kingae carriage is very common in children attending day care facilities in Western Norway. APMIS 2020, 128, 35–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagupsky, P.; Ben-Ami, Y.; Trefler, R.; Porat, N. Outbreaks of invasive Kingella kingae infections in closed communities. J. Pediatr. 2016, 169, 135–139.e1. [Google Scholar] [CrossRef]
- Yagupsky, P.; El Houmami, N.; Fluss, R. Outbreaks of Kingella kingae infections in daycare centers suggest tissue tropism of the causative strains. J. Pediatr. Infect. Dis. Soc. 2020, 9, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Guarch-Ibáñez, B.; Cabacas, A.; González-López, J.J.; García-González, M.D.M.; Mora, C.; Villalobos, P. First documented outbreak of arthritis caused by Kingella kingae in a Spanish childcare center. Enferm. Infecc. Microbiol. Clin. (Eng. Ed). 2021. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0213005X20304079?via%3Dihub (accessed on 18 January 2022). [CrossRef]
- Klein, C.; Peltier, F.; Pluquet, E.; Haraux, E.; Gouron, R.; Joseph, C. Management of an outbreak of invasive Kingella kingae skeletal infections in a day care center. Arch. Pediatr. 2020, 28, 12–15. [Google Scholar] [CrossRef]
- Ceroni, D.; Dubois-Ferrière, V.; Anderson, R.; Combescure, C.; Lamah, L.; Cherkaoui, A.; Schrenzel, J. Small risk of osteoarticular infections in children with asymptomatic oropharyngeal carriage of Kingella kingae. Pediatr. Infect. Dis. J. 2012, 31, 983–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagupsky, P. Outbreaks of Kingella kingae infections in daycare facilities. Emerg. Infect. Dis. 2014, 20, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Matuschek, E.; Åhman, J.; Kahlmeter, G.; Yagupsky, P. Antimicrobial susceptibility testing of Kingella kingae with broth microdilution and disk diffusion using EUCAST recommended media. Clin. Microbiol. Infect. 2018, 24, 396–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olijve, L.; Podmore, R.; Anderson, T.; Walls, T. High rate of oropharyngeal Kingella kingae carriage in New Zealand children. J. Paediatr. Child Health 2016, 52, 1081–1085. [Google Scholar] [CrossRef] [PubMed]
- Basmaci, R.; Deschamps, K.; Levy, C.; Mathy, V.; Corrard, F.; Thollot, F.; Béchet, S.; Sobral, E.; Bidet, P.; Cohen, R.; et al. Prevalence of Kingella kingae oropharyngeal carriage and predominance of type a and type b polysaccharide capsules among French young children. Clin. Microbiol. Infect. 2018, 25, 114–116. [Google Scholar] [CrossRef] [Green Version]
- Khatami, A.; Rivers, B.R.; Outhred, A.C.; Kesson, A.M. Low prevalence of Kingella kingae carriage in children aged 6–48 months in Sydney, Australia. J. Paediatr. Child Health 2017, 53, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Ceroni, D.; Dubois-Ferriere, V.; Della Llana, R.A.; Kherad, O.; Lascombes, P.; Renzi, G.; Manzano, S.; Cherkaoui, A.; Schrenzel, J. Oropharyngeal Colonization Density of Kingella kingae. Pediatr. Infect. Dis. J. 2013, 32, 803–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagupsky, P.; Porat, N.; Pinco, E. Pharyngeal colonization by Kingella kingae in children with invasive disease. Pediatr. Infect. Dis. J. 2009, 28, 155–157. [Google Scholar] [CrossRef]
- Ceroni, D.; Dubois-Ferriere, V.; Cherkaoui, A.; Gesuele, R.; Combescure, C.; Lamah, L.; Manzano, S.; Hibbs, J.; Schrenzel, J. Detection of Kingella kingae osteoarticular infections in children by oropharyngeal swab PCR. Pediatrics 2013, 131, e230–e235. [Google Scholar] [CrossRef] [Green Version]
- Basmaci, R.; Bonacorsi, S.; Ilharreborde, B.; Doit, C.; Lorrot, M.; Kahil, M.; Visseaux, B.; Houhou, N.; Bidet, P. High respiratory virus oropharyngeal carriage rate during Kingella kingae osteoarticular infections in children. Future Microbiol. 2015, 10, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Basmaci, R.; Bidet, P.; Bonacorsi, S. Kingella kingae and viral infections. Microorganisms 2022, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Basmaci, R.; Yagupsky, P.; Ilharreborde, B.; Guyot, K.; Porat, N.; Chomton, M.; Thiberge, J.-M.; Mazda, K.; Bingen, E.; Bonacorsi, S.; et al. Multilocus sequence typing and rtxA toxin gene sequencing analysis of Kingella kingae isolates demonstrates genetic diversity and international clones. PLoS ONE 2012, 7, e38078. [Google Scholar] [CrossRef] [PubMed]
- Basmaci, R.; Bidet, P.; Yagupsky, P.; Muñoz-Almagro, C.; Balashova, N.V.; Doit, C.; Bonacorsi, S. Major Intercontinentally distributed sequence types of Kingella kingae and development of a rapid molecular typing tool. J. Clin. Microbiol. 2014, 52, 3890–3897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amit, U.; Porat, N.; Basmaci, R.; Bidet, P.; Bonacorsi, S.; Dagan, R.; Yagupsky, P. Genotyping of invasive Kingella kingae isolates reveals predominant clones and association with specific clinical syndromes. Clin. Infect. Dis. 2012, 55, 1074–1079. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yagupsky, P. Pharyngeal Colonization by Kingella kingae, Transmission, and Pathogenesis of Invasive Infections: A Narrative Review. Microorganisms 2022, 10, 637. https://doi.org/10.3390/microorganisms10030637
Yagupsky P. Pharyngeal Colonization by Kingella kingae, Transmission, and Pathogenesis of Invasive Infections: A Narrative Review. Microorganisms. 2022; 10(3):637. https://doi.org/10.3390/microorganisms10030637
Chicago/Turabian StyleYagupsky, Pablo. 2022. "Pharyngeal Colonization by Kingella kingae, Transmission, and Pathogenesis of Invasive Infections: A Narrative Review" Microorganisms 10, no. 3: 637. https://doi.org/10.3390/microorganisms10030637
APA StyleYagupsky, P. (2022). Pharyngeal Colonization by Kingella kingae, Transmission, and Pathogenesis of Invasive Infections: A Narrative Review. Microorganisms, 10(3), 637. https://doi.org/10.3390/microorganisms10030637