
Assessing Tick-Borne Disease Risk and Surveillance: Toward a Multi-Modal Approach to Diagnostic Positioning and Prediction


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey and Respondent Data
2.2. National County-Level Data
2.3. Database and Data Alignment
- −
- Presence of at least 1 CDC-reported LD case between the years of 2000 and 2019;
- −
- CDC-reported presence of I. scapularis and/or I. pacificus as of 2020;
- −
- Presence of at least 1 CAPC-reported canine anaplasmosis case in 2020;
- −
- Presence of at least 1 CAPC-reported canine ehrlichiosis case in 2020;
- −
- Presence of at least 1 CAPC-reported canine LD case in 2020.
3. Results
3.1. Distribution of Self-Reported Infections and Co-Infections
3.2. Distribution of TBEs by County-Level Endpoints
3.3. Counties with Canine TBDs
3.4. Counties with CDC LD Cases
3.5. Counties with I. scapularis or I. pacificus
4. Discussion
4.1. Canine TBD Data as a Potential Proxy for TBD Risk
4.2. Co-Infections and Self-Reported Diagnoses
4.3. Integration of Survey and National Datasets
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hussain, S.; Hussain, A.; Aziz, U.; Song, B.; Zeb, J.; George, D.; Li, J.; Sparagano, O. The Role of Ticks in the Emergence of Borrelia Burgdorferi as a Zoonotic Pathogen and Its Vector Control: A Global Systemic Review. Microorganisms 2021, 9, 2412. [Google Scholar] [CrossRef] [PubMed]
- Böhmer, M.M.; Ens, K.; Böhm, S.; Heinzinger, S.; Fingerle, V. Epidemiological Surveillance of Lyme Borreliosis in Bavaria, Germany, 2013–2020. Microorganisms 2021, 9, 1872. [Google Scholar] [CrossRef] [PubMed]
- Hazen, B. Vector-Borne Diseases in the United States. SciLine. Available online: www.sciline.org/evidence-blog/vector-borne-diseases (accessed on 18 December 2021).
- Centers for Disease Control and Prevention (CDC). Data and Surveillance, National Center for Emerging and Zoonotic Infectious Diseases, Division of Vector-Borne Diseases. 2021. Available online: https://www.cdc.gov/lyme/datasurveillance/index.html (accessed on 18 December 2021).
- Dumic, I.; Severnini, E. “Ticking Bomb”: The Impact of Climate Change on the Incidence of Lyme Disease. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 5719081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parola, P.; Paddock, C.D.; Socolovschi, C.; Labruna, M.B.; Mediannikov, O.; Kernif, T.; Abdad, M.Y.; Stenos, J.; Bitam, I.; Fournier, P.E. Update on Tick-Borne Rickettsioses around the World: A Geographic Approach. Clin. Microbiol. Rev. 2013, 26, 657–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maxwell, S.P.; McNeely, C.L.; Thomas, K.; Brooks, C. Tick-Borne Surveillance Patterns in Perceived Non-Endemic Geographic Areas: Human Tick Encounters and Disease Outcomes. Healthcare 2021, 9, 771. [Google Scholar] [CrossRef] [PubMed]
- Eisen, R.J.; Eisen, L. The Blacklegged Tick, Ixodes Scapularis: An Increasing Public Health Concern. Trends Parasitol. 2018, 34, 295–309. [Google Scholar] [CrossRef] [PubMed]
- Talbot, B.; Kulkarni, M.A.; Colautti, R.I. Convergence Research for Emerging Zoonoses. Trends Parasitol. 2021, 37, 465–467. [Google Scholar] [CrossRef] [PubMed]
- Stricker, R.B.; Fesler, M.C. Chronic Lyme Disease: A Working Case Definition. Am. J. Infect. Dis. 2018, 14, 1–44. [Google Scholar] [CrossRef]
- Rebman, A.W.; Aucott, J.N. Post-Treatment Lyme Disease as a Model for Persistent Symptoms in Lyme Disease. Front. Med. 2020, 7, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobe, J.R.; Jutras, B.L.; Horn, E.J.; Embers, M.E.; Bailey, A.; Moritz, R.L.; Zhang, Y.; Soloski, M.J.; Ostfeld, R.S.; Marconi, R.T.; et al. Recent Progress in Lyme Disease and Remaining Challenges. Front. Med. 2021, 8, 666554. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Tick Surveillance Data Sets. Available online: https://www.cdc.gov/ticks/surveillance/ticksurveillancedata.html (accessed on 17 January 2022).
- Companion Animal Parasite Council (CAPC). Available online: https://capcvet.org/Maps#/2021/all-year/lyme-disease/dog/united-states (accessed on 4 January 2022).
- National Insitutite of Allergy and Infectious Diseases. Lyme Disease Diagnostics Research. 2021. Available online: https://www.niaid.nih.gov/diseases-conditions/lyme-disease-diagnostics-research (accessed on 4 January 2022).
- Omodior, O.; Kianersi, S.; Luetke, M. Spatial clusters and Non-Spatial Predictors of Tick-Borne Disease Diagnosis in Indiana. J. Community Health 2019, 44, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Hook, S.A.; Nawrocki, C.C.; Meek, J.I.; Feldman, K.A.; White, J.L.; Connally, N.P.; Hinckley, A.F. Human-Tick Encounters as a Measure of Tickborne Disease Risk in Lyme Disease Endemic Areas. Zoonoses Public Health 2021, 68, 384–392. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age | Reported Tick Bite Encounter | Did Not Report Tick Bite Encounter | All Respondents |
|---|---|---|---|
| 9–20 | 3 | 9 | 12 |
| 21–30 | 6 | 6 | 12 |
| 31–45 | 56 | 18 | 74 |
| 46–64 | 80 | 20 | 100 |
| Older than 65 | 36 | 4 | 40 |
| Age not reported | 1 | 0 | 1 |
| Total | 182 | 57 | 239 |
| Co-Infections | Recall Tick Bite | Do Not Recall Tick Bite | All Respondents |
| Total number of respondents who reported Lyme disease only | 20 | 6 | 26 |
| Total number of respondents who reported Lyme disease plus another infection | 37 | 23 | 60 |
| Total number of respondents who reported no Lyme disease or other infection noted | 81 | 18 | 99 |
| Total number of respondents who reported no Lyme disease but reported another infection | 44 | 10 | 54 |
| Total number of respondents | 182 | 57 | 239 |
| Diagnostic Category | Number of Respondents (% of Total) | Number of TBEs (% of Total) | ||
|---|---|---|---|---|
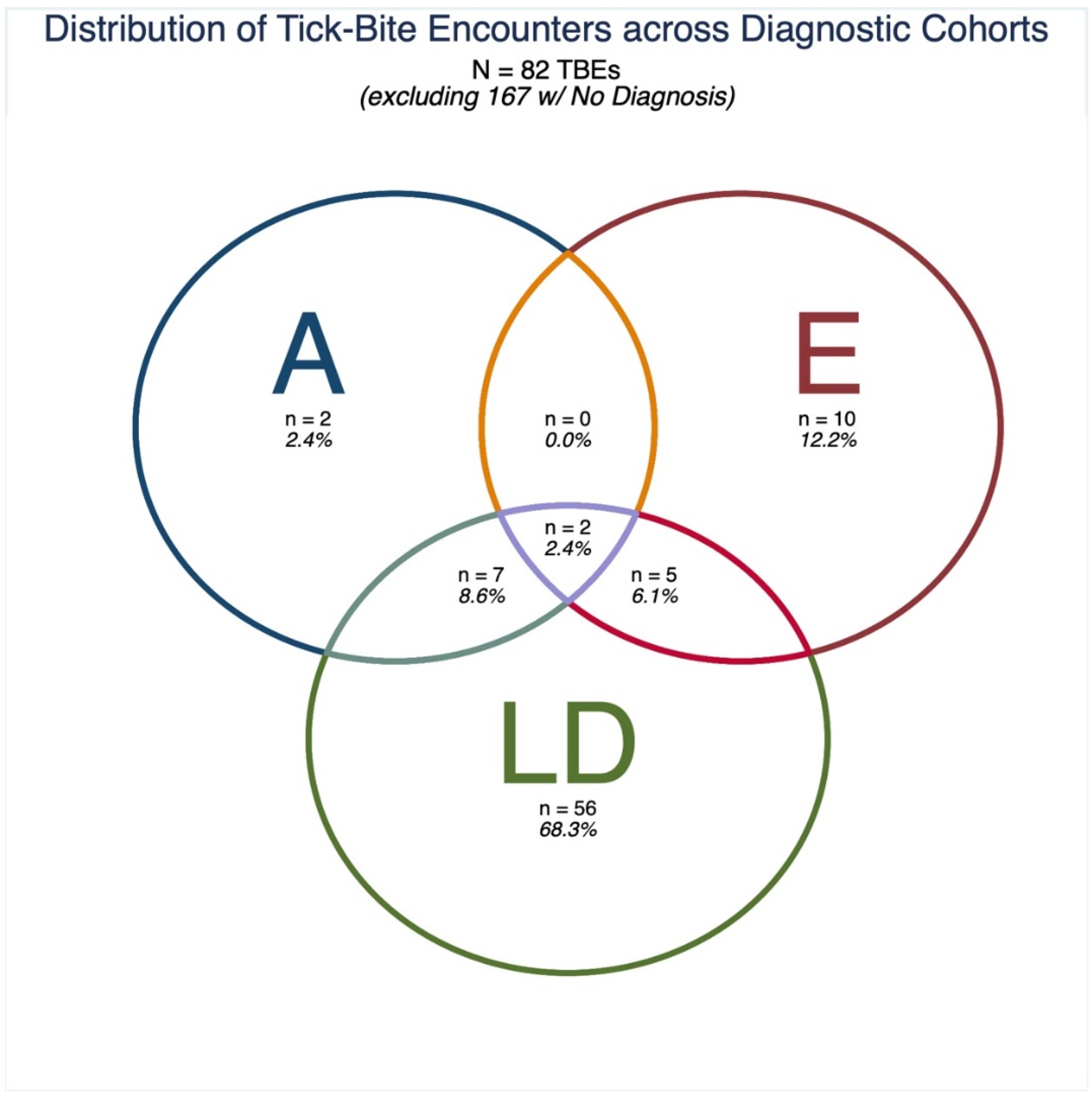
| No Diagnosis/“maybe, not sure” | 97 (65.54%) | - | 167 (67.07%) | - |
| LD Only | 34 (22.97%) | 34 (66.67%) | 56 (22.49%) | 56 (68.29%) |
| Ehrlichiosis Only | 6 (4.05%) | 6 (11.76%) | 10 (4.02%) | 10 (12.20%) |
| Anaplasmosis Only | 2 (1.35%) | 2 (3.92%) | 2 (0.80%) | 2 (2.44%) |
| Anaplasmosis and Lyme Disease Only | 3 (2.03%) | 3 (5.88%) | 7 (2.81%) | 7 (8.54%) |
| Ehrlichiosis and Lyme Disease Only | 4 (2.70%) | 4 (7.84%) | 5 (2.01%) | 5 (6.10%) |
| Anaplasmosis and ehrlichiosis Only | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) |
| Anaplasmosis, ehrlichiosis, and Lyme Disease | 2 (1.35%) | 2 (3.92%) | 2 (0.80%) | 2 (2.44%) |
| Total | 148 (100.00%) | 51 (100.00%) | 249 (100.00%) | 82 (100%) |
| (A) | ||||
|---|---|---|---|---|
| Self-Reported Diagnosis Category (Total Number of TBEs in Diagnostic Category)—Canine Data | Counties with 1 + Canine Anaplasmosis Cases | Counties with 1 + Canine Ehrlichiosis Cases | Counties with 1 + Canine Lyme Disease Cases | Counties with 1 + Canine TBD Cases |
| No Diagnoses * (n = 157) | 120 (76.43%) | 143 (91.08%) | 129 (82.17%) | 149 (94.9%) |
| Anaplasmosis (n = 10) | 10 (100%) | 10 (100%) | 9 (90%) | 10 (100%) |
| Anaplasmosis Only * (n = 2) | 2 (100%) | 2 (100%) | 2 (100%) | 2 (100%) |
| Ehrlichiosis (n = 15) | 10 (66.67%) | 13 (86.67%) | 9 (60%) | 14 (93.33%) |
| Ehrlichiosis Only * (n = 8) | 4 (50%) | 7 (87.5%) | 4 (50%) | 8 (100%) |
| Lyme Disease (n = 67) | 52 (77.61%) | 66 (98.51%) | 64 (95.52%) | 66 (98.51%) |
| Lyme Disease Only * (n = 54) | 40 (74.07%) | 54 (100%) | 53 (98.15%) | 54 (100%) |
| Anaplasmosis and Ehrlichiosis (n = 2) | 2 (100%) | 2 (100%) | 1 (50%) | 2 (100%) |
| Anaplasmosis and Ehrlichiosis Only *,** (n = 0) | No respondents reported being diagnosed with only anaplasmosis and ehrlichiosis | |||
| Anaplasmosis and Lyme Disease (n = 8) | 8 (100%) | 8 (100%) | 7 (87.5%) | 8 (100%) |
| Anaplasmosis and Lyme Disease Only *,** (n = 6) | 6 (100%) | 6 (100%) | 6 (100%) | 6 (100%) |
| Ehrlichiosis and Lyme Disease (n = 7) | 6 (85.71%) | 6 (85.71%) | 5 (71.43%) | 6 (85.71%) |
| Ehrlichiosis and Lyme Disease Only *,** (n = 5) | 4 (80%) | 4 (80%) | 4 (80%) | 4 (80%) |
| Anaplasmosis, Ehrlichiosis, and Lyme Disease *,** (n = 2) | 2 (100%) | 2 (100%) | 1 (50%) | 2 (100%) |
| Total of Mutually Exclusive Coinfection Diagnostic Categories * | 12 out of 13 (92.31%) | 12 out of 13 (92.31%) | 11 out of 13 (84.62%) | 12 out of 13 (92.31%) |
| Total of Mutually Exclusive Diagnostic Categories ** | 178 out of 234 (76.07%) | 218 out of 234 (93.16%) | 199 out of 234 (85.04%) | 225 out of 234 (96.15%) |
| (B) | ||||
| Self-Reported Diagnosis Category (Total Number of TBEs in Diagnostic Category)—CDC Data | Counties with 1 + CDC-Reported Lyme Disease Cases | Counties with either I. scapularis or I. pacificus | ||
| No Diagnoses * (n = 167) | 152 (91.02%) | 127 (76.05%) | ||
| Anaplasmosis (n = 11) | 9 (81.82%) | 8 (72.73%) | ||
| Anaplasmosis Only * (n = 2) | 2 (100%) | 2 (100%) | ||
| Ehrlichiosis (n = 17) | 12 (70.59%) | 13 (76.47%) | ||
| Ehrlichiosis Only * (n = 10) | 5 (50%) | 8 (80%) | ||
| Lyme Disease (n = 70) | 67 (95.71%) | 61 (87.14%) | ||
| Lyme Disease Only * (n = 56) | 55 (98.21%) | 51 (91.07%) | ||
| Anaplasmosis and Ehrlichiosis (n = 2) | 2 (100%) | 1 (50%) | ||
| Anaplasmosis and Ehrlichiosis Only *,** (n = 0) | No respondents reported being diagnosed with only anaplasmosis and ehrlichiosis | |||
| Anaplasmosis and Lyme Disease (n = 9) | 7 (77.78%) | 6 (66.67%) | ||
| Anaplasmosis and Lyme Disease Only *,** (n = 7) | 5 (71.43%) | 5 (71.43%) | ||
| Ehrlichiosis and Lyme Disease (n = 7) | 7 (100%) | 5 (71.43%) | ||
| Ehrlichiosis and Lyme Disease Only *,** (n = 5) | 5 (100%) | 4 (80%) | ||
| Anaplasmosis, Ehrlichiosis, and Lyme Disease *,** (n = 2) | 2 (100%) | 1 (50%) | ||
| Total of Mutually Exclusive Coinfection Diagnostic Categories * | 12 out of 14 (85.71%) | 10 out of 14 (71.43%) | ||
| Total of Mutually Exclusive Diagnostic Categories ** | 226 out of 249 (90.76%) | 198 out of 249 (79.52%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brooks, C.; McNeely, C.L.; Maxwell, S.P.; Thomas, K.C. Assessing Tick-Borne Disease Risk and Surveillance: Toward a Multi-Modal Approach to Diagnostic Positioning and Prediction. Microorganisms 2022, 10, 832. https://doi.org/10.3390/microorganisms10040832
Brooks C, McNeely CL, Maxwell SP, Thomas KC. Assessing Tick-Borne Disease Risk and Surveillance: Toward a Multi-Modal Approach to Diagnostic Positioning and Prediction. Microorganisms. 2022; 10(4):832. https://doi.org/10.3390/microorganisms10040832
Chicago/Turabian StyleBrooks, Chris, Connie L. McNeely, Sarah P. Maxwell, and Kevin C. Thomas. 2022. "Assessing Tick-Borne Disease Risk and Surveillance: Toward a Multi-Modal Approach to Diagnostic Positioning and Prediction" Microorganisms 10, no. 4: 832. https://doi.org/10.3390/microorganisms10040832
APA StyleBrooks, C., McNeely, C. L., Maxwell, S. P., & Thomas, K. C. (2022). Assessing Tick-Borne Disease Risk and Surveillance: Toward a Multi-Modal Approach to Diagnostic Positioning and Prediction. Microorganisms, 10(4), 832. https://doi.org/10.3390/microorganisms10040832