
The Clinical Features and Immunological Signature of Cyclospora cayetanensis Co-Infection among People Living with HIV in Ghana

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection and Laboratory Methods
2.3. Statistical Analysis
3. Results
3.1. Composition of the Study Population
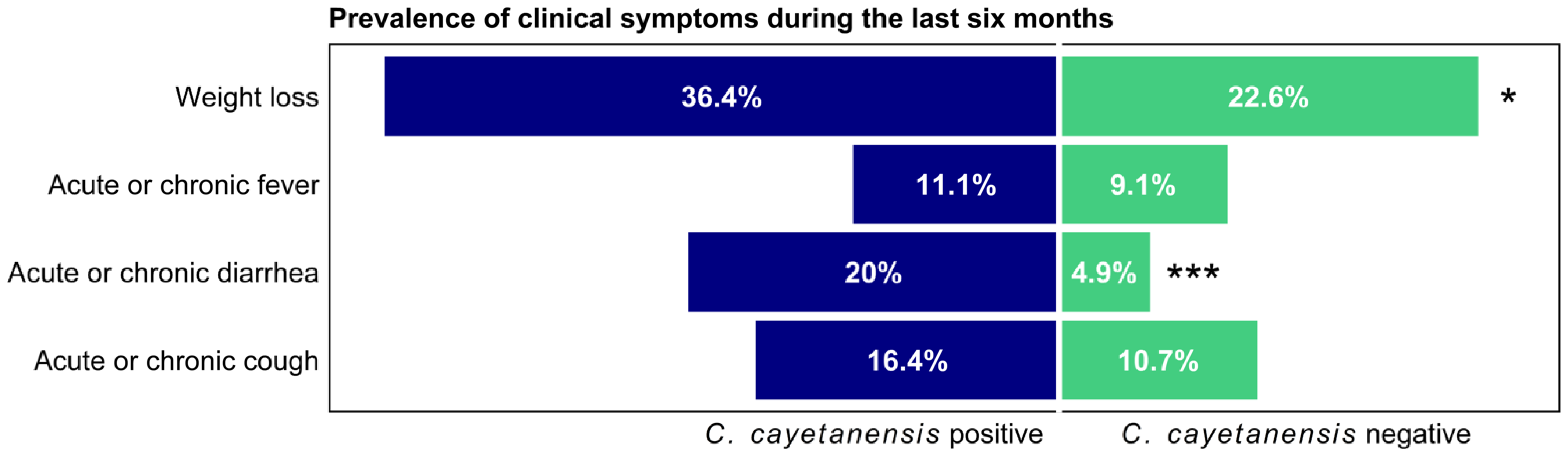
3.2. Comparison of Demographic and Clinical Characteristics of the HIV Cohort by C. cayetanesis Status
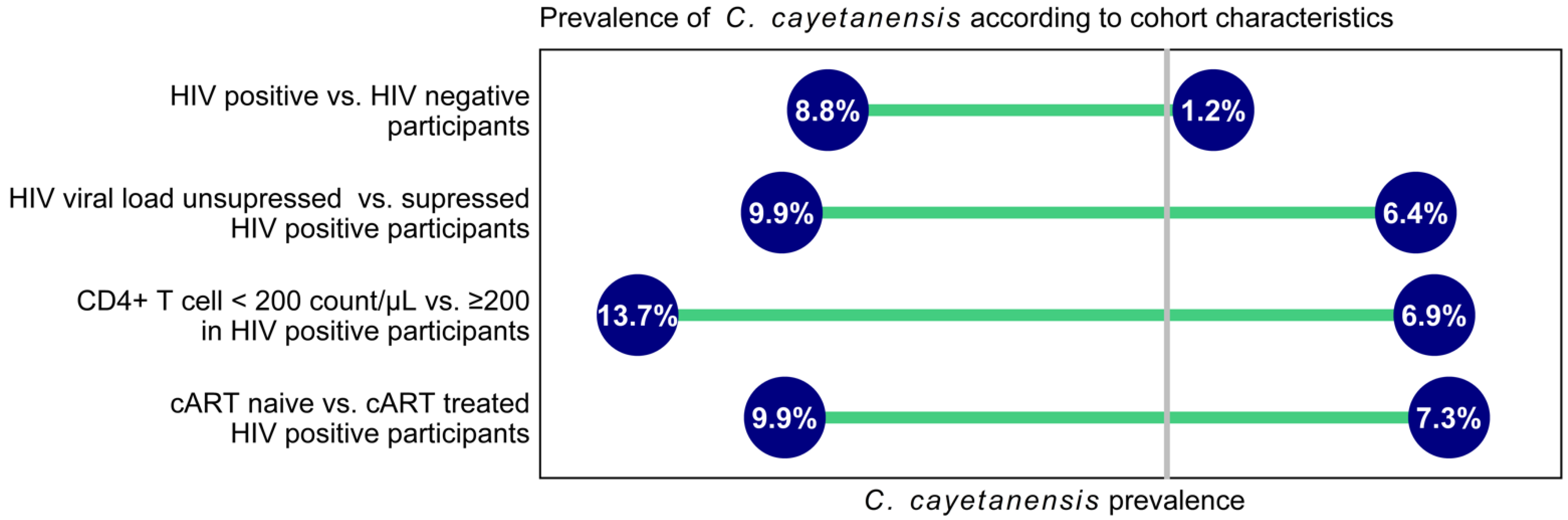
3.3. Comparison of Virological and Immunological Characteristics of the HIV Cohort by C. cayetanesis Status
3.4. Immunological Significance of C. cayetanensis Infection in PLWH
3.5. Correlations of Cycle Threshold (Ct) Values with HIV Viral Load and CD4+ Cell Count
4. Discussion
4.1. Implications of the Study Findings
4.2. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Connor, B.A. Cyclospora infection: A review. Ann. Acad. Med. Singap. 1997, 26, 632–636. [Google Scholar]
- Almeria, S.; Cinar, H.N.; Dubey, J.P. and Cyclosporiasis: An Update. Microorganisms 2019, 7, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramezanzadeh, S.; Beloukas, A.; Pagheh, A.S.; Rahimi, M.T.; Hosseini, S.A.; Oliveira, S.M.R.; de Lourdes Pereira, M.; Ahmadpour, E. Global Burden of Cyclospora cayetanensis Infection and Associated Risk Factors in People Living with HIV and/or AIDS. Viruses 2022, 14, 1279. [Google Scholar] [CrossRef] [PubMed]
- Chacín-Bonilla, L. Transmission of Cyclospora cayetanensis infection: A review focusing on soil-borne cyclosporiasis. Trans. R Soc. Trop. Med. Hyg. 2008, 102, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Helmy, M.M. Cyclospora cayetanensis: A review, focusing on some of the remaining questions about cyclosporiasis. Infect. Disord. Drug. Targets 2010, 10, 368–375. [Google Scholar] [CrossRef]
- Dubey, J.P.; Khan, A.; Rosenthal, B.M. Life Cycle and Transmission of Cyclospora cayetanensis: Knowns and Unknowns. Microorganisms 2022, 10, 118. [Google Scholar] [CrossRef]
- Giangaspero, A.; Gasser, R.B. Human cyclosporiasis. Lancet Infect. Dis. 2019, 19, e226–e236. [Google Scholar] [CrossRef]
- Hoge, C.W.; Shlim, D.R.; Ghimire, M.; Rabold, J.G.; Pandey, P.; Walch, A.; Rajah, R.; Gaudio, P.; Echeverria, P. Placebo-controlled trial of co-trimoxazole for Cyclospora infections among travellers and foreign residents in Nepal. Lancet 1995, 345, 691–693. [Google Scholar] [CrossRef]
- Mathison, B.A.; Pritt, B.S. Cyclosporiasis-Updates on Clinical Presentation, Pathology, Clinical Diagnosis, and Treatment. Microorganisms 2021, 9, 1863. [Google Scholar] [CrossRef]
- Verdier, R.I.; Fitzgerald, D.W.; Johnson, W.D.; Pape, J.W. Trimethoprim-sulfamethoxazole compared with ciprofloxacin for treatment and prophylaxis of Isospora belli and Cyclospora cayetanensis infection in HIV-infected patients. A randomized, controlled trial. Ann. Intern. Med. 2000, 132, 885–888. [Google Scholar] [CrossRef]
- Li, J.; Wang, R.; Chen, Y.; Xiao, L.; Zhang, L. Cyclospora cayetanensis infection in humans: Biological characteristics, clinical features, epidemiology, detection method and treatment. Parasitology 2020, 147, 160–170. [Google Scholar] [CrossRef]
- Sarfo, F.S.; Eberhardt, K.A.; Dompreh, A.; Kuffour, E.O.; Soltau, M.; Schachscheider, M.; Drexler, J.F.; Eis-Hübinger, A.M.; Häussinger, D.; Oteng-Seifah, E.E.; et al. Helicobacter pylori Infection Is Associated with Higher CD4 T Cell Counts and Lower HIV-1 Viral Loads in ART-Naïve HIV-Positive Patients in Ghana. PLoS ONE 2015, 10, e0143388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Cristanziano, V.; D’Alfonso, R.; Berrilli, F.; Sarfo, F.S.; Santoro, M.; Fabeni, L.; Knops, E.; Heger, E.; Kaiser, R.; Dompreh, A.; et al. Lower prevalence of Blastocystis sp. infections in HIV positive compared to HIV negative adults in Ghana. PLoS ONE 2019, 14, e0221968. [Google Scholar] [CrossRef] [Green Version]
- Di Cristanziano, V.; Weimer, K.; Böttcher, S.; Sarfo, F.S.; Dompreh, A.; Cesar, L.G.; Knops, E.; Heger, E.; Wirtz, M.; Kaiser, R.; et al. Molecular Characterization and Clinical Description of Non-Polio Enteroviruses Detected in Stool Samples from HIV-Positive and HIV-Negative Adults in Ghana. Viruses 2020, 12, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eberhardt, K.A.; Sarfo, F.S.; Klupp, E.-M.; Dompreh, A.; Di Cristanziano, V.; Osei Kuffour, E.; Boateng, R.; Norman, B.; Phillips, R.O.; Aepfelbacher, M.; et al. Intestinal Colonization with Tropheryma whipplei—Clinical and Immunological Implications for HIV Positive Adults in Ghana. Microorganisms 2021, 9, 1781. [Google Scholar] [CrossRef]
- Eberhardt, K.A.; Sarfo, F.S.; Dompreh, A.; Kuffour, E.O.; Geldmacher, C.; Soltau, M.; Schachscheider, M.; Drexler, J.F.; Eis-Hübinger, A.M.; Häussinger, D.; et al. Helicobacter pylori Coinfection Is Associated With Decreased Markers of Immune Activation in ART-Naive HIV-Positive and in HIV-Negative Individuals in Ghana. Clin. Infect. Dis. 2015, 61, 1615–1623. [Google Scholar] [CrossRef] [Green Version]
- Verweij, J.J.; Laeijendecker, D.; Brienen, E.A.; van Lieshout, L.; Polderman, A.M. Detection of Cyclospora cayetanensis in travellers returning from the tropics and subtropics using microscopy and real-time PCR. Int. J. Med. Microbiol. 2003, 293, 199–202. [Google Scholar] [CrossRef]
- Frickmann, H.; Hoffmann, T.; Köller, T.; Hahn, A.; Podbielski, A.; Landt, O.; Loderstädt, U.; Tannich, E. Comparison of five commercial real-time PCRs for in-vitro diagnosis of Entamoeba histolytica, Giardia duodenalis, Cryptosporidium spp., Cyclospora cayetanensis, and Dientamoeba fragilis in human stool samples. Travel Med. Infect. Dis. 2021, 41, 102042. [Google Scholar] [CrossRef]
- Weinreich, F.; Hahn, A.; Eberhardt, K.A.; Feldt, T.; Sarfo, F.S.; Di Cristanziano, V.; Frickmann, H.; Loderstädt, U. Comparison of Three Real-Time PCR Assays for the Detection of Cyclospora cayetanensis in Stool Samples Targeting the 18S rRNA Gene and the hsp70 Gene. Pathogens 2022, 11, 165. [Google Scholar] [CrossRef]
- Niesters, H.G. Quantitation of viral load using real-time amplification techniques. Methods 2001, 25, 419–429. [Google Scholar] [CrossRef]
- Agholi, M.; Hatam, G.R.; Motazedian, M.H. HIV/AIDS-associated opportunistic protozoal diarrhea. AIDS Res. Hum. Retrovir. 2013, 29, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saksirisampant, W.; Prownebon, J.; Saksirisampant, P.; Mungthin, M.; Siripatanapipong, S.; Leelayoova, S. Intestinal parasitic infections: Prevalences in HIV/AIDS patients in a Thai AIDS-care centre. Ann. Trop. Med. Parasitol. 2009, 103, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Udeh, E.O.; Obiezue, R.N.N.; Okafor, F.C.; Ikele, C.B.; Okoye, I.C.; Otuu, C.A. Gastrointestinal Parasitic Infections and Immunological Status of HIV/AIDS Coinfected Individuals in Nigeria. Ann. Glob. Health 2019, 85, 99. [Google Scholar] [CrossRef]
- Rivero-Rodríguez, Z.; Hernández, A.; Bracho, Á.; Salazar, S.; Villalobos, R. Prevalence of intestinal microsporidia and other intestinal parasites in hiv positive patients from Maracaibo, Venezuela. Biomedica 2013, 33, 538–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cegielski, J.P.; Ortega, Y.R.; McKee, S.; Madden, J.F.; Gaido, L.; Schwartz, D.A.; Manji, K.; Jorgensen, A.F.; Miller, S.E.; Pulipaka, U.P.; et al. Cryptosporidium, enterocytozoon, and cyclospora infections in pediatric and adult patients with diarrhea in Tanzania. Clin. Infect. Dis. 1999, 28, 314–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pape, J.W.; Verdier, R.I.; Boncy, M.; Boncy, J.; Johnson, W.D. Cyclospora infection in adults infected with HIV. Clinical manifestations, treatment, and prophylaxis. Ann. Intern. Med. 1994, 121, 654–657. [Google Scholar] [CrossRef]
- Escobedo, A.A.; Núñez, F.A. Prevalence of intestinal parasites in Cuban acquired immunodeficiency syndrome (AIDS) patients. Acta Trop. 1999, 72, 125–130. [Google Scholar] [CrossRef]
- Wondmieneh, A.; Gedefaw, G.; Alemnew, B.; Getie, A.; Bimerew, M.; Demis, A. Intestinal parasitic infections and associated factors among people living with HIV/AIDS in Ethiopia: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0244887. [Google Scholar] [CrossRef]
- Basile, F.W.; Fedele, M.C.; Lo Vecchio, A. Gastrointestinal Diseases in Children Living with HIV. Microorganisms 2021, 9, 1572. [Google Scholar] [CrossRef]
- Elfstrand, L.; Florén, C.H. Management of chronic diarrhea in HIV-infected patients: Current treatment options, challenges and future directions. HIV AIDS 2010, 2, 219–224. [Google Scholar] [CrossRef] [Green Version]
- WHO. Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach; WHO: Geneve, Switzerland, 2021. [Google Scholar]
- Frickmann, H.; Alker, J.; Hansen, J.; Dib, J.C.; Aristizabal, A.; Concha, G.; Schotte, U.; Kann, S. Seasonal Differences in Cyclospora cayetanensis Prevalence in Colombian Indigenous People. Microorganisms 2021, 9, 627. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | HIV-Positive C. cayetanensis Positive, n = 56 (8.75%) | HIV-Positive C. cayetanensis Negative, n = 584 (91.25%) | p-Value | |
|---|---|---|---|---|
| Demographics | Age in years ± SD | 39.0 ± 9.2 | 40.7 ± 9.5 | 0.208 |
| Female, n (%) | 37 (67.27) | 425 (74.43) | 0.321 | |
| Socioeconomic parameters | Access to tap water, n (%) | 30 (54.55) | 303 (53.06) | 0.945 |
| Electricity in household, n (%) | 54 (98.18) | 531 (92.99) | 0.230 | |
| Television in household, n (%) | 47 (85.45) | 464 (81.26) | 0.559 | |
| Refrigerator in household, n (%) | 39 (70.91) | 415 (72.68) | 0.902 | |
| Owning a car, n (%) | 4 (7.27) | 56 (9.81) | 0.809 | |
| Medical therapy | Co-trimoxazole prophylaxis, n (%) | 14 (26.92) | 189 (33.69) | 0.402 |
| Antiretroviral therapy, n (%) | 19 (34.55) | 242 (42.38) | 0.326 | |
| Months since initiation of cART, median (IQR) | 17.3 (6.9–36.6) | 55.2 (28.6–79.5) | 0.001 |
| Variable | HIV-Positive Cohort | HIV-Positive cART Exposed | HIV Positive cART Naïve | ||||||
|---|---|---|---|---|---|---|---|---|---|
| C. cayetanensis Positive, Median (IQR), n = 56 | C. cayetanensis Negative, Median (IQR), n = 584 | p-Value | C. cayetanensis Positive, Median (IQR), n = 19 | C. cayetanensis Negative, Median (IQR), n = 242 | p-Value | C. cayetanensis Positive, Median (IQR), n = 36 | C. cayetanensis Negative, Median (IQR), n = 329 | p-Value | |
| Viral load, log10 copies/mL | 5.0 (2.2–5.6) | 4.1 (1.6–5.3) | 0.012 | 1.6 (0.0–1.9) | 1.6 (0.0–1.9) | 0.126 | 5.4 (4.8–5.8) | 5.1 (4.3–5.6) | 0.054 |
| CD4+ T-cell count/µL | 228.0 (91.5–395.5) | 355.0 (163.5–586.5) | 0.001 | 308.0 (259.5–599.5) | 516.5 (329.0–712.8) | 0.053 | 141.0 (46.0–297.8) | 246.0 (94.0–451.0) | 0.012 |
| CD8+ T-cell count/µL | 938.0 (565.5–1279.0) | 977.0 (659.5–1390.5) | 0.576 | 896.0 (796.0–1172.0) | 961.0 (656.2–1331.2) | 0.961 | 988.0 (493.5–1388.0) | 995.0 (661.5–1507.5) | 0.477 |
| CD4+/CD8+ T-cell ratio | 0.3 (0.1–0.4) | 0.4 (0.2–0.7) | 0.005 | 0.4 (0.3–0.6) | 0.5 (0.4–0.9) | 0.205 | 0.2 (0.1–0.3) | 0.3 (0.1–0.5) | 0.013 |
| HLA-DR+ CD38+ CD4+ (%) | 31.0 (19.2–38.6) | 17.3 (9.5–30.6) | 0.002 | 16.4 (15.4–26.1) | 10.5 (6.5–18.2) | 0.018 | 33.4 (23.9–38.7) | 23.6 (13.7–35.9) | 0.043 |
| HLA-DR+ CD38+ CD8+ (%) | 49.3 (42.8–60.9) | 43.4 (27.8–56.7) | 0.042 | 45.6 (34.4–52.3) | 27.5 (19.4–38.1) | 0.045 | 54.0 (43.3–62.7) | 51.5 (41.3–64.7) | 0.565 |
| CD57+ CD4+ (%) | 19.2 (9.2–30.3) | 14.4 (8.8–23.9) | 0.293 | 16.9 (13.1–30.9) | 13.3 (8.5–20.7) | 0.274 | 19.5 (8.5–25.3) | 14.4 (9.1–26.5) | 0.726 |
| CD57+ CD8+ (%) | 46.9 (33.8–63.2) | 48.4 (38.4–57.3) | 0.816 | 39.0 (30.9–63.8) | 51.2 (43.2–58.5) | 0.227 | 52.9 (34.7–59.7) | 44.8 (35.5–55.6) | 0.480 |
| PD-1+ CD4+ (%) | 42.3 (29.8–63.2) | 32.4 (22.6–46.1) | 0.069 | 40.6 (22.3–53.8) | 30.0 (18.7–39.9) | 0.227 | 42.3 (30.2–66.1) | 36.5 (24.6–52.8) | 0.201 |
| PD-1+ CD8+ (%) | 43.1 (30.1–49.2) | 31.9 (21.4–44.0) | 0.042 | 38.0 (26.1–49.3) | 25.0 (15.5–36.0) | 0.074 | 44.6 (35.1–47.0) | 38.7 (26.0–50.3) | 0.334 |
| Ki67+ CD4+ (%) | 23.8 (14.7–26.8) | 13.0 (6.3–30.6) | 0.174 | 15.3 (10.7–21.1) | 7.9 (5.1–16.4) | 0.404 | 25.1 (17.0–42.3) | 21.1 (9.6–44.7) | 0.492 |
| Ki67+ CD8+ (%) | 16.0 (10.9–19.4) | 10.2 (6.2–17.2) | 0.153 | 21.7 (21.7–21.7) | 6.7 (4.0–12.2) | 0.219 | 14.0 (10.3–17.8) | 12.0 (8.1–18.7) | 0.658 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarfo, F.S.; Dompreh, A.; Asibey, S.O.; Boateng, R.; Weinreich, F.; Kuffour, E.O.; Norman, B.; Di Cristanziano, V.; Frickmann, H.; Feldt, T.; et al. The Clinical Features and Immunological Signature of Cyclospora cayetanensis Co-Infection among People Living with HIV in Ghana. Microorganisms 2022, 10, 1407. https://doi.org/10.3390/microorganisms10071407
Sarfo FS, Dompreh A, Asibey SO, Boateng R, Weinreich F, Kuffour EO, Norman B, Di Cristanziano V, Frickmann H, Feldt T, et al. The Clinical Features and Immunological Signature of Cyclospora cayetanensis Co-Infection among People Living with HIV in Ghana. Microorganisms. 2022; 10(7):1407. https://doi.org/10.3390/microorganisms10071407
Chicago/Turabian StyleSarfo, Fred Stephen, Albert Dompreh, Shadrack Osei Asibey, Richard Boateng, Felix Weinreich, Edmund Osei Kuffour, Betty Norman, Veronica Di Cristanziano, Hagen Frickmann, Torsten Feldt, and et al. 2022. "The Clinical Features and Immunological Signature of Cyclospora cayetanensis Co-Infection among People Living with HIV in Ghana" Microorganisms 10, no. 7: 1407. https://doi.org/10.3390/microorganisms10071407
APA StyleSarfo, F. S., Dompreh, A., Asibey, S. O., Boateng, R., Weinreich, F., Kuffour, E. O., Norman, B., Di Cristanziano, V., Frickmann, H., Feldt, T., & Eberhardt, K. A. (2022). The Clinical Features and Immunological Signature of Cyclospora cayetanensis Co-Infection among People Living with HIV in Ghana. Microorganisms, 10(7), 1407. https://doi.org/10.3390/microorganisms10071407