
Achromobacter Species: An Emerging Cause of Community-Onset Bloodstream Infections

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Microbiologic Methods
2.3. Data Linkage
2.4. Definitions
2.5. Statistics
2.6. Ethical Approval
3. Results
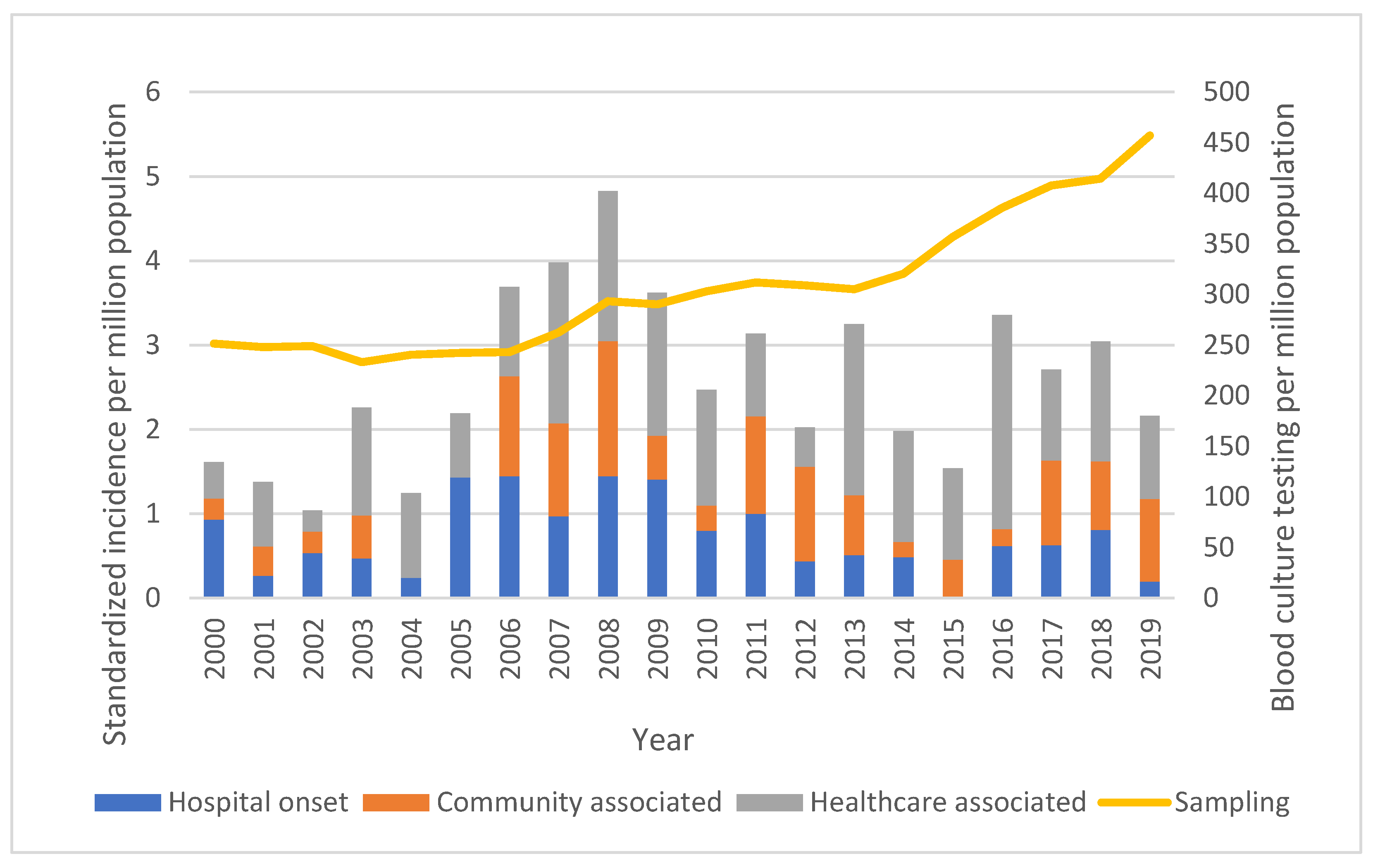
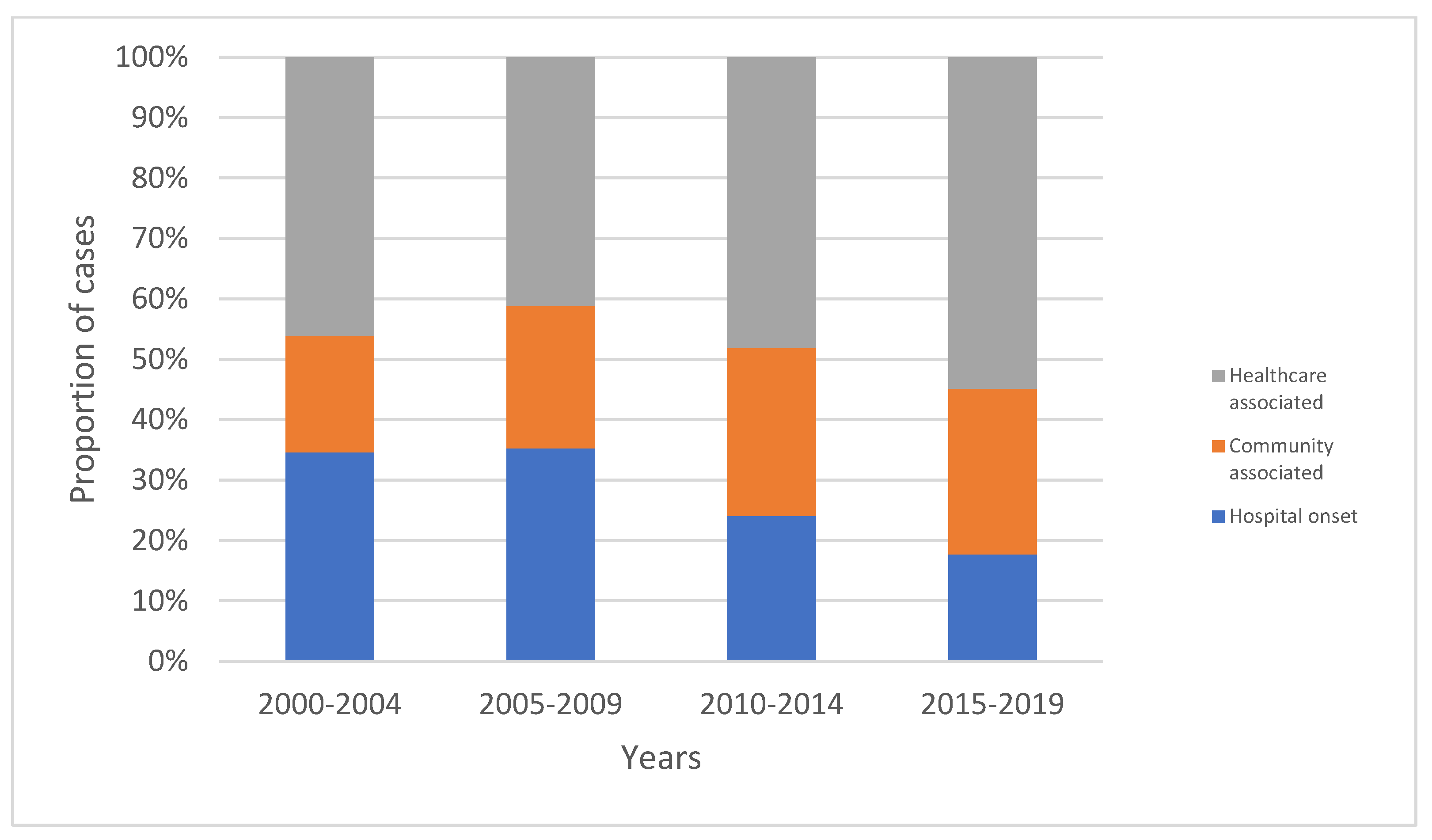
3.1. Incidence
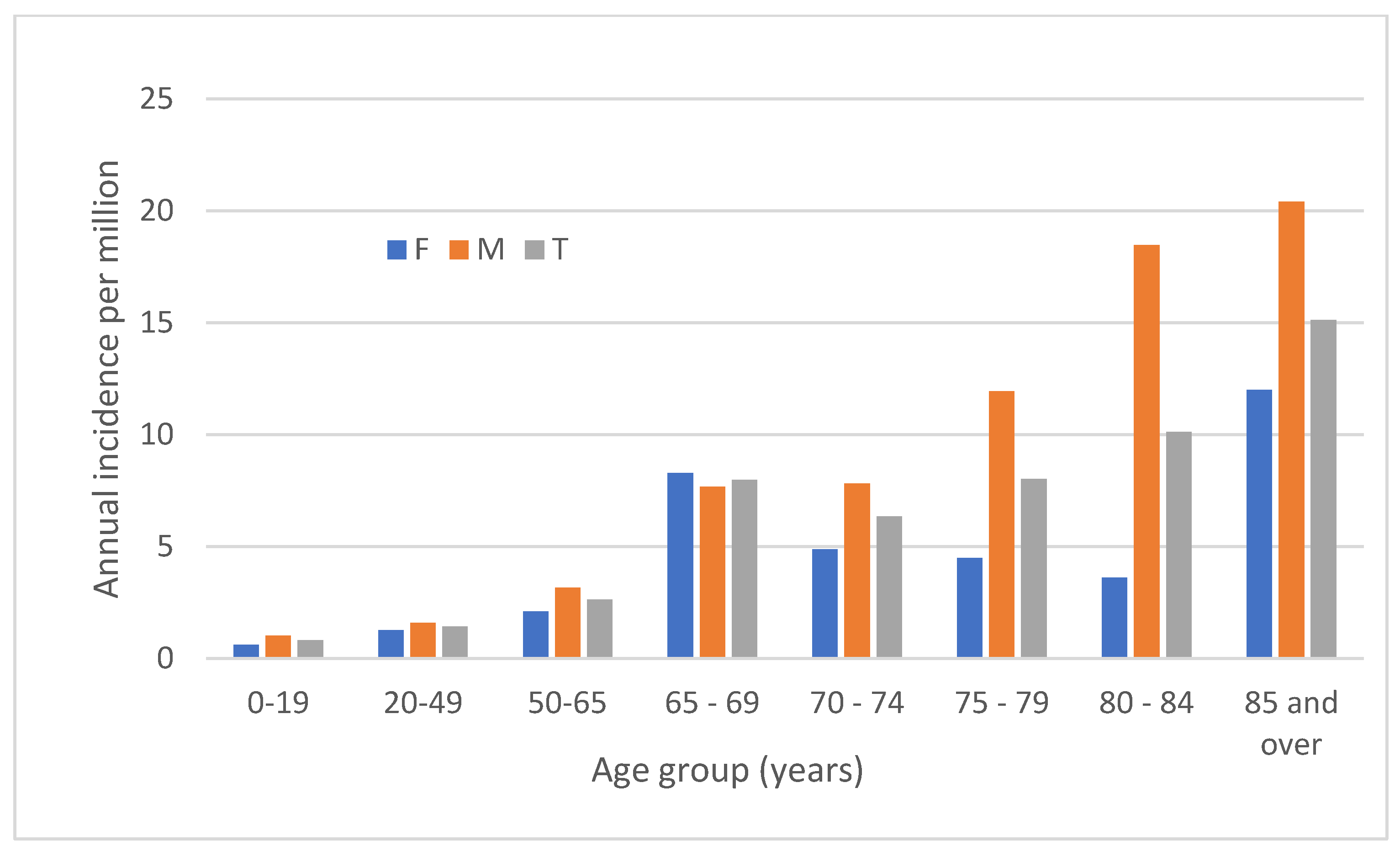
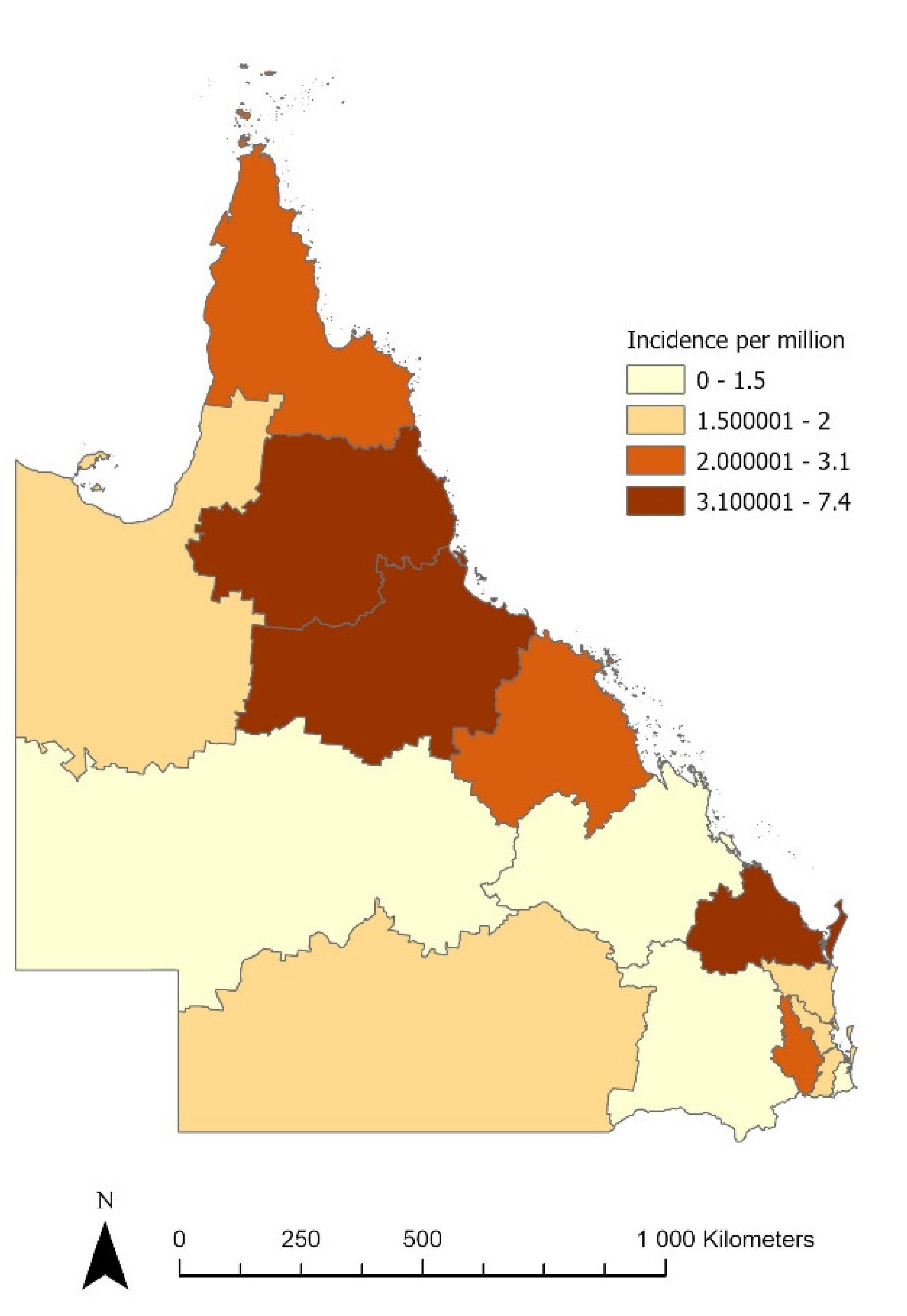
3.2. Demographic Risk Factors for Acquisition
3.3. Clinical Determinants
3.4. Antimicrobial Susceptibility
3.5. Hospital Admission and Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Parkins, M.D.; Floto, R.A. Emerging bacterial pathogens and changing concepts of bacterial pathogenesis in cystic fibrosis. J. Cyst. Fibros. 2015, 14, 293–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menetrey, Q.; Sorlin, P.; Jumas-Bilak, E.; Chiron, R.; Dupont, C.; Marchandin, H. Achromobacter xylosoxidans and Stenotrophomonas maltophilia: Emerging Pathogens Well-Armed for Life in the Cystic Fibrosis Patients’ Lung. Genes 2021, 12, 610. [Google Scholar] [CrossRef] [PubMed]
- Høiby, N.; Bjarnsholt, T.; Moser, C.; Jensen, P.; Kolpen, M.; Qvist, T.; Aanaes, K.; Pressler, T.; Skov, M.; Ciofu, O. Diagnosis of biofilm infections in cystic fibrosis patients. APMIS 2017, 125, 339–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isler, B.; Kidd, T.J.; Stewart, A.G.; Harris, P.; Paterson, D.L. Achromobacter Infections and Treatment Options. Antimicrob. Agents Chemother. 2020, 64, e01025-20. [Google Scholar] [CrossRef] [PubMed]
- Duggan, J.M.; Goldstein, S.J.; Chenoweth, C.E.; Kauffman, C.A.; Bradley, S.F. Achromobacter xylosoxidans Bacteremia: Report of Four Cases and Review of the Literature. Clin. Infect. Dis. 1996, 23, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marion-Sanchez, K.; Pailla, K.; Olive, C.; Le Coutour, X.; Derancourt, C. Achromobacter spp. healthcare associated infections in the French West Indies: A longitudinal study from 2006 to 2016. BMC Infect. Dis. 2019, 19, 795. [Google Scholar] [CrossRef] [PubMed]
- Pérez Barragán, E.; Sandino Pérez, J.; Corbella, L.; Orellana, M.A.; Fernández-Ruiz, M. Achromobacter xylosoxidans bacteremia: Clinical and microbiological features in a 10-year case series. Rev. Esp. Quimioter. 2018, 31, 268–273. [Google Scholar] [PubMed]
- Laupland, K.B. Defining the epidemiology of bloodstream infections: The ‘gold standard’ of population-based assessment. Epidemiol. Infect. 2013, 141, 2149–2157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anonymous. Hospital and Health Service Maps; Queensland Health: Queensland, Australia, 2021. Available online: https://www.health.qld.gov.au/maps (accessed on 22 September 2021).
- Leal, J.; Gregson, D.B.; Ross, T.; Flemons, W.W.; Church, D.L.; Laupland, K.B. Development of a novel electronic surveillance system for monitoring of bloodstream infections. Infect. Control Hosp. Epidemiol. 2010, 31, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.D.; Kaye, K.S.; Stout, J.E.; McGarry, S.A.; Trivette, S.L.; Briggs, J.P.; Lamm, W.; Clark, C.; MacFarquhar, J.; Walton, A.L.; et al. Health care--associated bloodstream infections in adults: A reason to change the accepted definition of community-acquired infections. Ann. Intern. Med. 2002, 137, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Aisenberg, G.; Rolston, K.V.; Safdar, A. Bacteremia caused by Achromobacter and Alcaligenes species in 46 patients with cancer (1989–2003). Cancer 2004, 101, 2134–2140. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Cerezo, J.; Suárez, I.; Ríos, J.J.; Peña, P.; García De Miguel, M.J.G.; De José, M.; Monteagudo, O.; Linares, P.; Barbado-Cano, A.; Vázquez, J.J. Achromobacter xylosoxidans Bacteremia: A 10-Year Analysis of 54 Cases. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Ronin, E.; Derancourt, C.; Cabié, A.; Marion-Sanchez, K. Achromobacter spp. Surgical Site Infections: A Systematic Review of Case Reports and Case Series. Microorganisms 2021, 9, 2471. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, K.A.; Butler, C.A.; Paynter, S.; Ware, R.S.; Kidd, T.J.; Wainwright, C.E.; Bell, S.C. Factors influencing acquisition of Burkholderia cepacia complex organisms in patients with cystic fibrosis. J. Clin. Microbiol. 2013, 51, 3975–3980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.; Nistal, C.; Jayan, R.; Kuduvalli, M.; Anijeet, H. Achromobacter xylosoxidans, an emerging pathogen in catheter-related infection in dialysis population causing prosthetic valve endocarditis: A case report and review of literature. Clin. Nephrol. 2009, 71, 350–354. [Google Scholar] [CrossRef]
- MacKinnon, M.C.; McEwen, S.A.; Pearl, D.L.; Lyytikäinen, O.; Jacobsson, G.; Collignon, P.; Gregson, D.B.; Valiquette, L.; Laupland, K.B. Mortality in Escherichia coli bloodstream infections: A multinational population-based cohort study. BMC Infect. Dis. 2021, 21, 606. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | No Charlson Comorbidity (n = 38) | Charlson 1 or More (n = 172) | p-Value |
|---|---|---|---|
| Onset classification | 0.035 | ||
| Hospital-onset | 9 (24%) | 48 (28%) | |
| Healthcare-associated | 13 (34%) | 87 (51%) | |
| Community-associated | 16 (42%) | 37 (22%) | |
| Male sex | 26 (68%) | 98 (57%) | 0.2 |
| Charlson variables | - | - | |
| Myocardial infarction | 26 (15%) | ||
| Congestive heart failure | 45 (26%) | ||
| Peripheral vascular disease | 32 (19%) | ||
| Cerebrovascular disease | 13 (8%) | ||
| Dementia | 4 (2%) | ||
| Chronic pulmonary | 39 (23%) | ||
| Rheumatic | 5 (3%) | ||
| Peptic ulcer disease | 5 (2%) | ||
| Liver disease | 26 (15%) | ||
| Diabetes mellitus | 62 (36%) | ||
| Plegia | 15 (9%) | ||
| Renal disease | 82 (48%) | ||
| Malignancy | 48 (28%) | ||
| Focus of infection | <0.001 | ||
| No focus identified | 10 (27%) | 90 (52%) | |
| Soft tissue | 3 (8%) | 20 (12%) | |
| Bone and joint | 5 (14%) | 8 (5%) | |
| Head and neck | 3 (8%) | 0 | |
| Lower respiratory | 2 (5%) | 15 (9%) | |
| Endovascular | 7 (19%) | 19 (11%) | |
| Abdominal | 3 (8%) | 16 (9%) | |
| Urinary/pelvic | 4 (11%) | 4 (2%) | |
| Polymicrobial infection | 8 (21%) | 39 (23%) | 1.0 |
| Antibiotic Name (Number of Isolates Tested) | Susceptible, n (%) | Intermediate, n (%) | Resistant, n (%) |
|---|---|---|---|
| Ciprofloxacin (198) | 72 (36) | 7 (4) | 119 (60) |
| Gentamicin (203) | 21 (10) | 0 | 182 (90) |
| Meropenem (182) | 178 (98) | 0 | 4 (2) |
| Co-trimoxazole (190) | 176 (93) | 0 | 14 (7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isler, B.; Paterson, D.L.; Harris, P.N.A.; Ling, W.; Edwards, F.; Rickard, C.M.; Kidd, T.J.; Gassiep, I.; Laupland, K.B. Achromobacter Species: An Emerging Cause of Community-Onset Bloodstream Infections. Microorganisms 2022, 10, 1449. https://doi.org/10.3390/microorganisms10071449
Isler B, Paterson DL, Harris PNA, Ling W, Edwards F, Rickard CM, Kidd TJ, Gassiep I, Laupland KB. Achromobacter Species: An Emerging Cause of Community-Onset Bloodstream Infections. Microorganisms. 2022; 10(7):1449. https://doi.org/10.3390/microorganisms10071449
Chicago/Turabian StyleIsler, Burcu, David L. Paterson, Patrick N. A. Harris, Weiping Ling, Felicity Edwards, Claire M. Rickard, Timothy J. Kidd, Ian Gassiep, and Kevin B. Laupland. 2022. "Achromobacter Species: An Emerging Cause of Community-Onset Bloodstream Infections" Microorganisms 10, no. 7: 1449. https://doi.org/10.3390/microorganisms10071449
APA StyleIsler, B., Paterson, D. L., Harris, P. N. A., Ling, W., Edwards, F., Rickard, C. M., Kidd, T. J., Gassiep, I., & Laupland, K. B. (2022). Achromobacter Species: An Emerging Cause of Community-Onset Bloodstream Infections. Microorganisms, 10(7), 1449. https://doi.org/10.3390/microorganisms10071449