

First Report of Autochthonous Canine Leishmaniasis in Hong Kong


Abstract
:1. Introduction
2. Materials and Methods
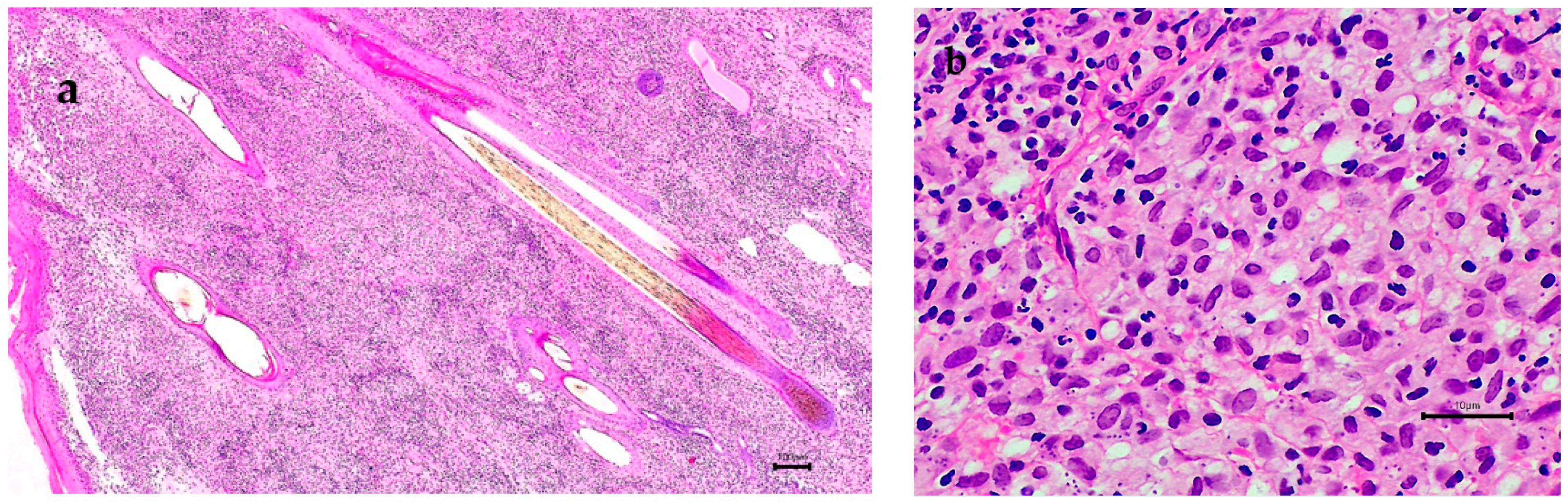
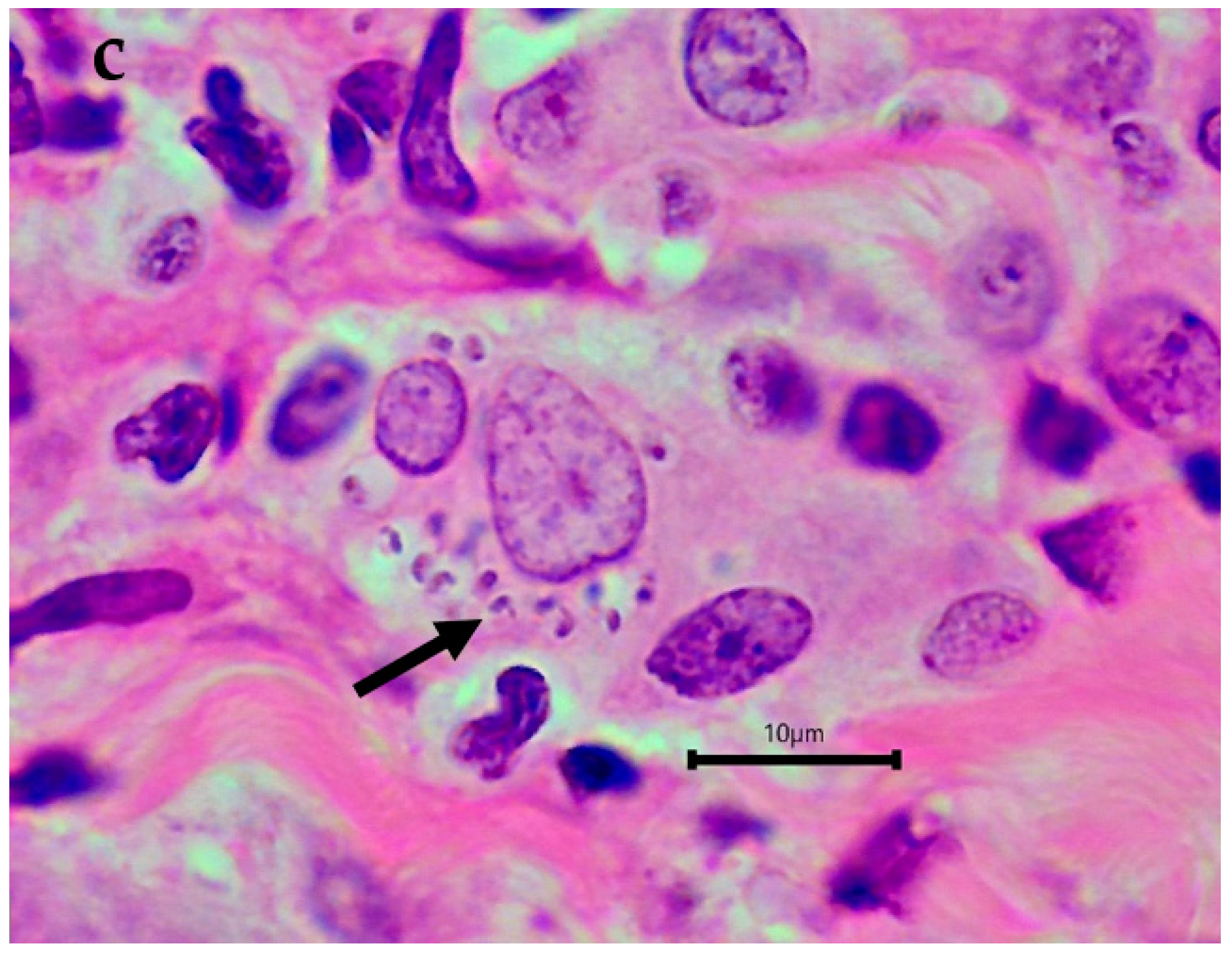
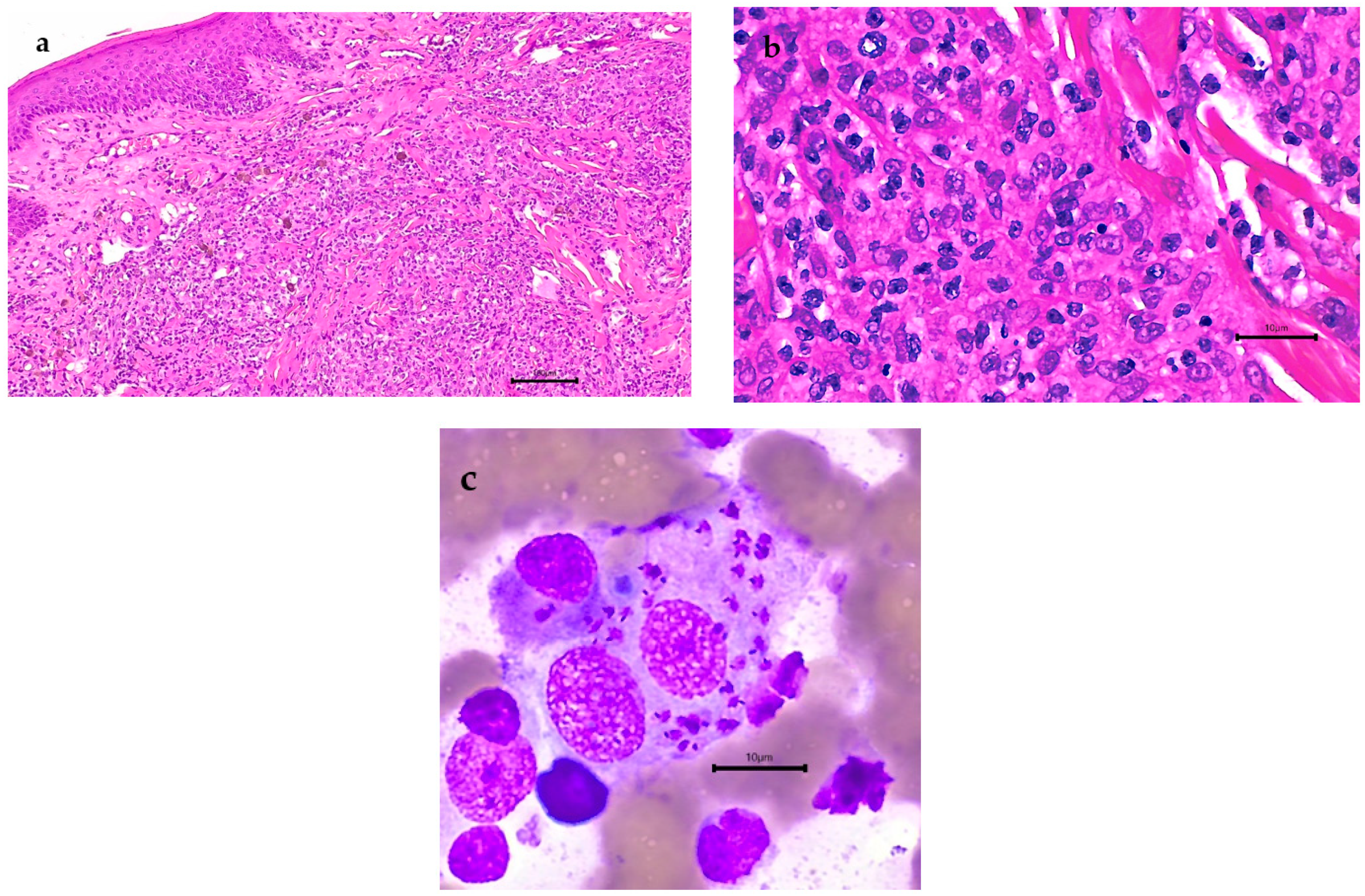
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- José, A.R.-P.; Saurabh, J.; Alexei, M.; Ana, N.M.-E.; Samantha, V.; Supriya, W.; Mona, O.; Zaw, L.; Abate, B.; Aya, Y.; et al. Global Leishmaniasis Surveillance: 2019–2020, a Baseline for the 2030 Roadmap. Available online: https://www.who.int/publications/i/item/who-wer9635-401-419 (accessed on 2 September 2022).
- Lun, Z.R.; Wu, M.S.; Chen, Y.F.; Wang, J.Y.; Zhou, X.N.; Liao, L.F.; Chen, J.P.; Chow, L.M.; Chang, K.P. Visceral Leishmaniasis in China: An Endemic Disease under Control. Clin. Microbiol. Rev. 2015, 28, 987–1004. [Google Scholar] [CrossRef]
- Nicolas, L.; Milon, G.; Prina, E. Rapid differentiation of Old World Leishmania species by LightCycler polymerase chain reaction and melting curve analysis. J. Microbiol. Methods 2002, 51, 295–299. [Google Scholar] [CrossRef]
- Talmi-Frank, D.; Nasereddin, A.; Schnur, L.F.; Schönian, G.; Töz, S.O.; Jaffe, C.L.; Baneth, G. Detection and identification of old world Leishmania by high resolution melt analysis. PLoS Negl. Trop. Dis. 2010, 4, e581. [Google Scholar] [CrossRef] [PubMed]
- Baneth, G.; Nachum-Biala, Y.; Zuberi, A.; Zipori-Barki, N.; Orshan, L.; Kleinerman, G.; Shmueli-Goldin, A.; Bellaiche, M.; Leszkowicz-Mazuz, M.; Salant, H.; et al. Leishmania infection in cats and dogs housed together in an animal shelter reveals a higher parasite load in infected dogs despite a greater seroprevalence among cats. Parasit. Vectors 2020, 13, 115. [Google Scholar] [CrossRef]
- Michalsky, E.M.; Rocha, M.F.; da Rocha Lima, A.C.; França-Silva, J.C.; Pires, M.Q.; Oliveira, F.S.; Pacheco, R.S.; dos Santos, S.L.; Barata, R.A.; Romanha, A.J.; et al. Infectivity of seropositive dogs, showing different clinical forms of leishmaniasis, to Lutzomyia longipalpis phlebotomine sand flies. Vet. Parasitol. 2007, 147, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Toepp, A.J.; Petersen, C.A. The balancing act: Immunology of leishmaniosis. Res. Vet. Sci. 2020, 130, 19–25. [Google Scholar] [CrossRef]
- Marcondes, M.; Day, M.J. Current status and management of canine leishmaniasis in Latin America. Res. Vet. Sci. 2019, 123, 261–272. [Google Scholar] [CrossRef]
- Baneth, G.; Koutinas, A.F.; Solano-Gallego, L.; Bourdeau, P.; Ferrer, L. Canine leishmaniosis—new concepts and insights on an expanding zoonosis: Part one. Trends Parasitol. 2008, 24, 324–330. [Google Scholar] [CrossRef]
- Laurenti, M.D.; Rossi, C.N.; da Matta, V.L.; Tomokane, T.Y.; Corbett, C.E.; Secundino, N.F.; Pimenta, P.F.; Marcondes, M. Asymptomatic dogs are highly competent to transmit Leishmania (Leishmania) infantum chagasi to the natural vector. Vet. Parasitol. 2013, 196, 296–300. [Google Scholar] [CrossRef]
- Magalhães-Junior, J.T.; Mota, T.F.; Porfirio-Passos, G.; Larangeira, D.F.; Franke, C.R.; Barrouin-Melo, S.M. Xenodiagnosis on dogs with visceral leishmaniasis: Canine and sand fly aspects related to the parasite transmission. Vet. Parasitol. 2016, 223, 120–126. [Google Scholar] [CrossRef]
- Serafim, T.D.; Iniguez, E.; Oliveira, F. Leishmania infantum. Trends Parasitol. 2020, 36, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Young, C.W.; Hertig, M. The development of flagellates in Chinese sandflies (phlebotomus) fed on hamsters infected with Leishmania donovani. Proc. Soc. Exp. Biol. Med. 1926, 23, 611–615. [Google Scholar] [CrossRef]
- Duprey, Z.H.; Steurer, F.J.; Rooney, J.A.; Kirchhoff, L.V.; Jackson, J.E.; Rowton, E.D.; Schantz, P.M. Canine visceral leishmaniasis, United States and Canada, 2000–2003. Emerg. Infect. Dis. 2006, 12, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.A. Leishmaniasis, an emerging disease found in companion animals in the United States. Top. Companion Anim. Med. 2009, 24, 182–188. [Google Scholar] [CrossRef]
- Boggiatto, P.M.; Gibson-Corley, K.N.; Metz, K.; Gallup, J.M.; Hostetter, J.M.; Mullin, K.; Petersen, C.A. Transplacental transmission of Leishmania infantum as a means for continued disease incidence in North America. PLoS Negl. Trop. Dis. 2011, 5, e1019. [Google Scholar] [CrossRef]
- de Almeida, M.E.; Spann, D.R.; Bradbury, R.S. Leishmania infantum in US-Born Dog. Emerg. Infect. Dis. 2020, 26, 1882–1884. [Google Scholar] [CrossRef]
- Alonso, F.H.; Vasilatis, D.M.; Veluvolu, S.M.; Willcox, J.L.; Scorza, B.M.; Petersen, C.A.; Kol, A. Canine leishmaniasis in Northern California-A case report. Vet. Clin. Pathol. 2021, 50, 71–75. [Google Scholar] [CrossRef]
- Fondevila, D.; Vilafranca, M.; Ferrer, L. Epidermal immunocompetence in canine leishmaniasis. Vet. Immunol. Immunopathol. 1997, 56, 319–327. [Google Scholar] [CrossRef]
- Ferrer, L.; Rabanal, R.; Fondevila, D.; Ramos, J.; Domingo, M. Skin lesions in canine leishmaniasis. J. Small Anim. Pract. 1988, 29, 381–388. [Google Scholar] [CrossRef]
- Ordeix, L.; Dalmau, A.; Osso, M.; Llull, J.; Montserrat-Sangrà, S.; Solano-Gallego, L. Histological and parasitological distinctive findings in clinically-lesioned and normal-looking skin of dogs with different clinical stages of leishmaniasis. Parasit. Vectors 2017, 10, 121. [Google Scholar] [CrossRef] [Green Version]
- Toepp, A.J.; Bennett, C.; Scott, B.; Senesac, R.; Oleson, J.J.; Petersen, C.A. Maternal Leishmania infantum infection status has significant impact on leishmaniasis in offspring. PLoS Negl. Trop. Dis. 2019, 13, e0007058. [Google Scholar] [CrossRef] [PubMed]
- Mancianti, F.; Sozzi, S. Isolation of Leishmania from a newborn puppy. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 402. [Google Scholar] [CrossRef]
- Díaz-Espiñeira, M.M.; Slappendel, R.J. A case of autochthonous canine leishmaniasis in The Netherlands. Vet. Q. 1997, 19, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Gaskin, A.A.; Schantz, P.; Jackson, J.; Birkenheuer, A.; Tomlinson, L.; Gramiccia, M.; Levy, M.; Steurer, F.; Kollmar, E.; Hegarty, B.C.; et al. Visceral leishmaniasis in a New York foxhound kennel. J. Vet. Intern. Med. 2002, 16, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Salant, H.; Nachum-Biala, Y.; Feinmesser, B.; Perelmutter, M.; Baneth, G. Early onset of clinical leishmaniosis in a litter of pups with evidence of in utero transmission. Parasit. Vectors. 2021, 14, 326. [Google Scholar] [CrossRef]
- Owens, S.D.; Oakley, D.A.; Marryott, K.; Hatchett, W.; Walton, R.; Nolan, T.J.; Newton, A.; Steurer, F.; Schantz, P.; Giger, U. Transmission of visceral leishmaniasis through blood transfusions from infected English foxhounds to anemic dogs. J. Am. Vet. Med. Assoc. 2001, 219, 1076–1083. [Google Scholar] [CrossRef]
- Svobodova, V.; Svoboda, M.; Friedlaenderova, L.; Drahotsky, P.; Bohacova, E.; Baneth, G. Canine leishmaniosis in three consecutive generations of dogs in Czech Republic. Vet. Parasitol. 2017, 237, 122–124. [Google Scholar] [CrossRef]
- Karkamo, V.; Kaistinen, A.; Näreaho, A.; Dillard, K.; Vainio-Siukola, K.; Vidgrén, G.; Tuoresmäki, N.; Anttila, M. The first report of autochthonous non-vector-borne transmission of canine leishmaniosis in the Nordic countries. Acta Vet. Scand. 2014, 56, 84. [Google Scholar] [CrossRef]
- Naucke, T.J.; Amelung, S.; Lorentz, S. First report of transmission of canine leishmaniosis through bite wounds from a naturally infected dog in Germany. Parasit. Vectors 2016, 9, 256. [Google Scholar] [CrossRef]
- Petanides, T.A.; Koutinas, A.F.; Mylonakis, M.E.; Day, M.J.; Saridomichelakis, M.N.; Leontides, L.S.; Mischke, R.; Diniz, P.; Breitschwerdt, E.B.; Kritsepi, M.; et al. Factors associated with the occurrence of epistaxis in natural canine leishmaniasis (Leishmania infantum). J. Vet. Intern. Med. 2008, 22, 866–872. [Google Scholar] [CrossRef]
- Foglia Manzillo, V.; Di Muccio, T.; Cappiello, S.; Scalone, A.; Paparcone, R.; Fiorentino, E.; Gizzarelli, M.; Gramiccia, M.; Gradoni, L.; Oliva, G. Prospective study on the incidence and progression of clinical signs in naïve dogs naturally infected by Leishmania infantum. PLoS Negl. Trop. Dis. 2013, 7, e2225. [Google Scholar] [CrossRef] [PubMed]
- Saridomichelakis, M.N.; Koutinas, A.F. Cutaneous involvement in canine leishmaniasis due to Leishmania infantum (syn. L. chagasi). Vet. Dermatol. 2014, 25, 61-e22–71-e22. [Google Scholar] [CrossRef] [PubMed]
- Squarre, D.; Chambaro, H.M.; Hayashida, K.; Moonga, L.C.; Qiu, Y.; Goto, Y.; Oparaocha, E.; Mumba, C.; Muleya, W.; Bwalya, P.; et al. Autochthonous Leishmania infantum in Dogs, Zambia, 2021. Emerg. Infect. Dis. 2022, 28, 888–890. [Google Scholar] [CrossRef]
- Levy, E.; Mylonakis, M.E.; Saridomichelakis, M.N.; Polizopoulou, Z.S.; Psychogios, V.; Koutinas, A.F. Nasal and oral masses in a dog. Vet. Clin. Pathol. 2006, 35, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Paltrinieri, S.; Gradoni, L.; Roura, X.; Zatelli, A.; Zini, E. Laboratory tests for diagnosing and monitoring canine leishmaniasis. Vet. Clin. Pathol. 2016, 45, 552–578. [Google Scholar] [CrossRef] [PubMed]
- Courtenay, O.; Quinnell, R.J.; Garcez, L.M.; Shaw, J.J.; Dye, C. Infectiousness in a cohort of brazilian dogs: Why culling fails to control visceral leishmaniasis in areas of high transmission. J. Infect. Dis. 2002, 186, 1314–1320. [Google Scholar] [CrossRef]
- Costa, F.A.; Goto, H.; Saldanha, L.C.; Silva, S.M.; Sinhorini, I.L.; Silva, T.C.; Guerra, J.L. Histopathologic patterns of nephropathy in naturally acquired canine visceral leishmaniasis. Vet. Pathol. 2003, 40, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Solcà Mda, S.; Bastos, L.A.; Guedes, C.E.; Bordoni, M.; Borja, L.S.; Larangeira, D.F.; da Silva Estrela Tuy, P.G.; Amorim, L.D.; Nascimento, E.G.; de Sá Oliveira, G.G.; et al. Evaluating the accuracy of molecular diagnostic testing for canine visceral leishmaniasis using latent class analysis. PLoS ONE 2014, 9, e103635. [Google Scholar] [CrossRef]
- Gonçalves, A.A.M.; Leite, J.C.; Resende, L.A.; Mariano, R.; Silveira, P.; Melo-Júnior, O.A.O.; Ribeiro, H.S.; de Oliveira, D.S.; Soares, D.F.; Santos, T.A.P.; et al. An Overview of Immunotherapeutic Approaches Against Canine Visceral Leishmaniasis: What Has Been Tested on Dogs and a New Perspective on Improving Treatment Efficacy. Front. Cell. Infect. Microbiol. 2019, 9, 427. [Google Scholar] [CrossRef]
- Ribeiro, R.R.; Michalick, M.S.M.; da Silva, M.E.; Dos Santos, C.C.P.; Frézard, F.J.G.; da Silva, S.M. Canine Leishmaniasis: An Overview of the Current Status and Strategies for Control. Biomed. Res. Int. 2018, 2018, 3296893. [Google Scholar] [CrossRef] [Green Version]
- Miró, G.; Cardoso, L.; Pennisi, M.G.; Oliva, G.; Baneth, G. Canine leishmaniosis--new concepts and insights on an expanding zoonosis: Part two. Trends Parasitol. 2008, 24, 371–377. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
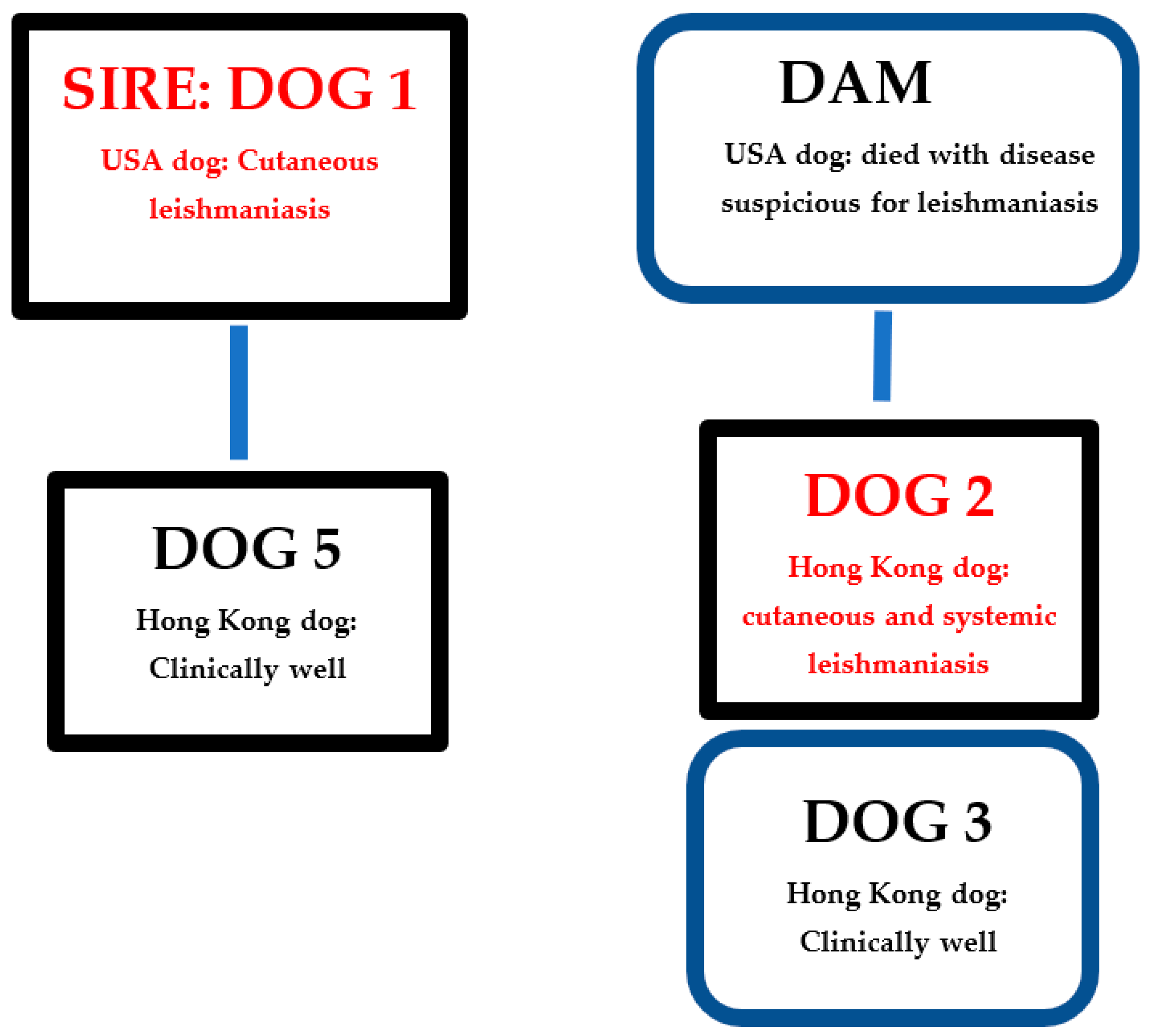
| Dog | Dog Country of Origin | Relationship with Other Dogs in Kennel | Year of Birth | Year of Test | Detection and Anatomic Location of Leishmania Amastigotes by Microscopy | ELISA Serology | PCR Result and Tissue | Leishmania Treatment/Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | USA | Sire of dog 5 | 2011 | 2015 | Yes: Skin | ND | − (blood) * | Skin disease resolved but relapsed |
| 2020 | ND | - | − (blood) + (skin) ** | Skin disease resolved | ||||
| 2 | Hong Kong | Full brother of dog 3 | 2012 | 2018 | Suspected: Skin and nasal mucosa | ND | ND | Skin disease resolved but relapsed and became systemic |
| 2019 | Yes: Spleen and liver | + *** | + (blood, spleen) | Disease resolved | ||||
| 3 | Hong Kong | Full sister of dog 2 | 2012 | 2019 | No | - | − (blood and skin) | NA |
| 4 | Netherlands | None | 2009 | 2019 | No | - | − (blood and skin) | NA |
| 5 | Hong Kong | Son of dog 1 | 2013 | 2020 | ND | - | − (blood) | NA |
| 6 | Hong Kong | None | 2011 | 2020 | ND | - | − (blood) | NA |
| 7 | Sweden | None | 2011 | 2020 | ND | - | − (blood) | NA |
| 8 | Netherlands | None | 2012 | 2020 | ND | - | − (blood) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandy, J.; Matthews, A.; Nachum-Biala, Y.; Baneth, G. First Report of Autochthonous Canine Leishmaniasis in Hong Kong. Microorganisms 2022, 10, 1873. https://doi.org/10.3390/microorganisms10091873
Sandy J, Matthews A, Nachum-Biala Y, Baneth G. First Report of Autochthonous Canine Leishmaniasis in Hong Kong. Microorganisms. 2022; 10(9):1873. https://doi.org/10.3390/microorganisms10091873
Chicago/Turabian StyleSandy, Jeanine, Anthony Matthews, Yaarit Nachum-Biala, and Gad Baneth. 2022. "First Report of Autochthonous Canine Leishmaniasis in Hong Kong" Microorganisms 10, no. 9: 1873. https://doi.org/10.3390/microorganisms10091873
APA StyleSandy, J., Matthews, A., Nachum-Biala, Y., & Baneth, G. (2022). First Report of Autochthonous Canine Leishmaniasis in Hong Kong. Microorganisms, 10(9), 1873. https://doi.org/10.3390/microorganisms10091873