
Efficacy of Fecal Microbiota Transplant on Behavioral and Gastrointestinal Symptoms in Pediatric Autism: A Systematic Review

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
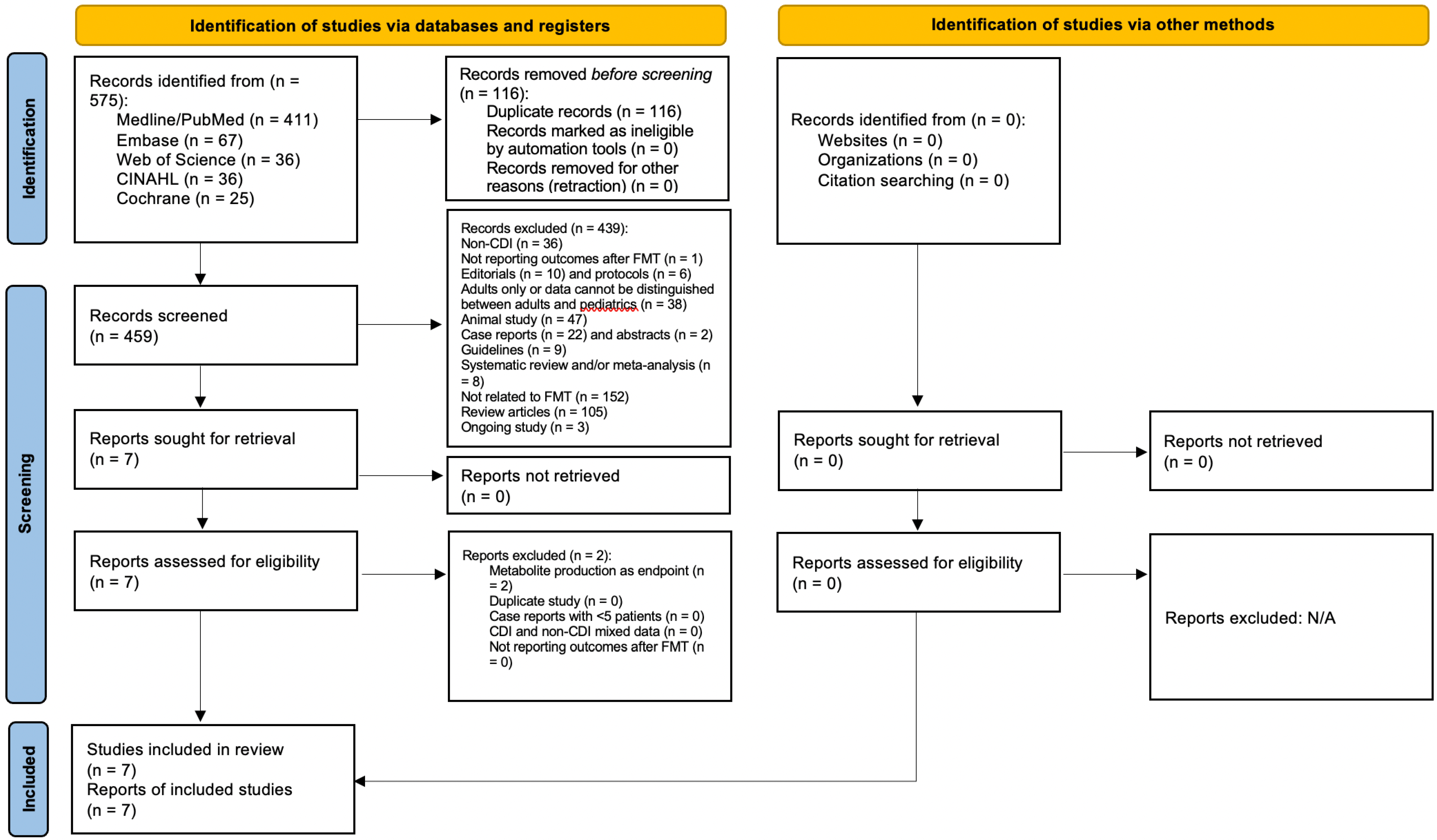
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
2.5. Study Outcomes
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl. Pediatr. 2020, 9 (Suppl. S1), S55–S65. [Google Scholar] [CrossRef] [PubMed]
- Guinchat, V.; Cravero, C.; Lefèvre-Utile, J.; Cohen, D. Multidisciplinary treatment plan for challenging behaviors in neurodevelopmental disorders. Handb. Clin. Neurol. 2020, 174, 301–321. [Google Scholar] [CrossRef] [PubMed]
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef]
- Doshi-Velez, F.; Ge, Y.; Kohane, I. Comorbidity clusters in autism spectrum disorders: An electronic health record time-series analysis. Pediatrics 2014, 133, e54–e63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nardone, S.; Elliott, E. The Interaction between the Immune System and Epigenetics in the Etiology of Autism Spectrum Disorders. Front. Neurosci. 2016, 10, 329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shenoy, M.D.; Indla, V.; Reddy, H. Comprehensive Management of Autism: Current Evidence. Indian J. Psychol. Med. 2017, 39, 727–731. [Google Scholar] [CrossRef]
- Yang, Y.; Tian, J.; Yang, B. Targeting gut microbiome: A novel and potential therapy for autism. Life Sci. 2018, 194, 111–119. [Google Scholar] [CrossRef]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The gut-brain axis: Interactions between enteric microbiota, central and enteric nervous systems. Ann. Gastroenterol. 2015, 28, 203–209. [Google Scholar]
- Kang, D.W.; Adams, J.B.; Coleman, D.M.; Pollard, E.L.; Maldonado, J.; McDonough-Means, S.; Caporaso, J.G.; Krajmalnik-Brown, R. Long-term benefit of Microbiota Transfer Therapy on autism symptoms and gut microbiota. Sci. Rep. 2019, 9, 5821. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.W.; Adams, J.B.; Vargason, T.; Santiago, M.; Hahn, J.; Krajmalnik-Brown, R. Distinct Fecal and Plasma Metabolites in Children with Autism Spectrum Disorders and Their Modulation after Microbiota Transfer Therapy. mSphere 2020, 5, e00314–e00320. [Google Scholar] [CrossRef]
- Prosperi, M.; Santocchi, E.; Guiducci, L.; Frinzi, J.; Morales, M.A.; Tancredi, R.; Muratori, F.; Calderoni, S. Interventions on Microbiota: Where Do We Stand on a Gut-Brain Link in Autism? A Systematic Review. Nutrients 2022, 14, 462. [Google Scholar] [CrossRef]
- Yang, J.; Fu, X.; Liao, X.; Li, Y. Effects of gut microbial-based treatments on gut microbiota, behavioral symptoms, and gastrointestinal symptoms in children with autism spectrum disorder: A systematic review. Psychiatry Res. 2020, 293, 113471. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Chen, H.; Cheng, Y.; Xu, F.; Ruan, G.; Ying, S.; Tang, W.; Chen, L.; Chen, M.; Lv, L.; et al. Fecal Microbiota Transplantation Relieves Gastrointestinal and Autism Symptoms by Improving the Gut Microbiota in an Open-Label Study. Front. Cell. Infect. Microbiol. 2021, 11, 759435. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Gao, Z.; Liu, C.; Liu, T.; Gao, J.; Cai, Y.; Fan, X. Alteration of Gut Microbiota: New Strategy for Treating Autism Spectrum Disorder. Front. Cell. Dev. Biol. 2022, 10, 792490. [Google Scholar] [CrossRef] [PubMed]
- Hardin, A.P.; Hackell, J.M.; Committee on Practice and Ambulatory Medicine. Age Limit of Pediatrics. Pediatrics 2017, 140, e20172151. [Google Scholar] [CrossRef] [Green Version]
- Abu-Zidan, F.M.; Abbas, A.K.; Hefny, A.F. Clinical “case series”: A concept analysis. Afr. Health Sci. 2012, 12, 557–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenize, J.E.; Bossuy, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The prisma 2020 statement an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Zhang, T.; Lu, G.; Zhao, Z.; Liu, Y.; Shen, Q.; Li, P.; Chen, Y.; Yin, H.; Wang, H.; Marcella, C.; et al. Washed microbiota transplantation vs. manual fecal microbiota transplantation: Clinical findings, animal studies and in vitro screening. Protein Cell. 2020, 11, 251–266. [Google Scholar] [CrossRef] [Green Version]
- Pan, Z.Y.; Zhong, H.J.; Huang, D.N.; Wu, L.H.; He, X.X. Beneficial Effects of Repeated Washed Microbiota Transplantation in Children with Autism. Front. Pediatr. 2022, 10, 928785. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Pan, Z.; He, X. Effects of Washed Fecal Bacteria Transplantation in Sleep Quality, Stool Features and Autism Symptomatology: A Chinese Preliminary Observational Study. Neuropsychiatr. Dis. Treat. 2022, 18, 1165–1173. [Google Scholar] [CrossRef]
- Kang, D.W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef]
- Abou-Setta, A.M.; Beaupre, L.A.; Jones, C.A.; Rashiq, S.; Hamm, M.P.; Sadowski, C.A.; Menon, M.R.G.; Majumdar, S.R.; Wilson, D.M.; Karkhaneh, M.; et al. Pain Management Interventions for Hip Fracture [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2011 May. (Comparative Effectiveness Reviews, No. 30.) Appendix I, Newcastle-Ottawa Scale Assessment of Cohort Studies. Available online: https://www.ncbi.nlm.nih.gov/books/NBK56664/ (accessed on 7 January 2023).
- Miani, C.; Martin, A.; Exley, J.; Doble, B.; Wilson, E.; Payne, R.; Avery, A.; Meads, C.; Kirtley, A.; Jones, M.M.; et al. Clinical Effectiveness and Cost-Effectiveness of Issuing Longer Versus Shorter Duration (3-Month vs. 28-Day) Prescriptions in Patients with Chronic Conditions: Systematic Review and Economic Modelling. Southampton (UK): NIHR Journals Library; 2017 Dec. (Health Technology Assessment, No. 21.78.) Appendix 4, Risk-of-Bias Assessments: Risk of Bias in Non-Randomized Studies—Of Interventions. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470102/ (accessed on 7 January 2023).
- Kat, S.; Xu, L.; Guo, Y.; Ma, J.; Ma, Z.; Tang, X.; Yang, Y.; Wang, H.; Li, X.; Liu, J. Reliability and Validity of the Simplified Chinese Version of the Aberrant Behavior Checklist in Chinese Autism Population. Front. Psychiatry 2020, 11, 545445. [Google Scholar] [CrossRef] [PubMed]
- Rellini, E.; Tortolani, D.; Trillo, S.; Carbone, S.; Montecchi, F. Childhood Autism Rating Scale (CARS) and Autism Behavior Checklist (ABC) correspondence and conflicts with DSM-IV criteria in diagnosis of autism. J. Autism Dev. Disord. 2004, 34, 703–708. [Google Scholar] [CrossRef]
- Chlebowski, C.; Green, J.A.; Barton, M.L.; Fein, D. Using the childhood autism rating scale to diagnose autism spectrum disorders. J. Autism Dev. Disord. 2010, 40, 787–799. [Google Scholar] [CrossRef] [Green Version]
- Schopler, E.; Reichler, R.J.; DeVellis, R.F.; Daly, K. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J. Autism Dev. Disord. 1980, 10, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef] [PubMed]
- Holingue, C.; Newill, C.; Lee, L.C.; Pasricha, P.J.; Daniele Fallin, M. Gastrointestinal symptoms in autism spectrum disorder: A review of the literature on ascertainment and prevalence. Autism Res. 2018, 11, 24–36. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Vasa, R.A.; Kalb, L.G.; Kanne, S.M.; Rosenberg, D.; Keefer, A.; Murray, D.S.; Freedman, B.; Lowery, L.A. Anxiety, sensory over-responsivity, and gastrointestinal problems in children with autism spectrum disorders. J. Abnorm Child. Psychol. 2013, 41, 165–176. [Google Scholar] [CrossRef]


{kind=link}
| Author/Year | Study Design | Pre-FMT Intervention | Intervention | Follow-Up |
|---|---|---|---|---|
| Pan 2022 [20] | Retrospective cohort study | None | WMT* injected through a transendoscopic enteral tube daily for 6 consecutive days. Participants received 2–5 treatments administered 4 weeks apart. | About 1 month after each treatment course |
| Zhang 2022 [21] | Retrospective cohort study | Probiotics (Bifidobacteria capsule, compound Lactobacillus acidophilus tablets, etc.) before and during FMT | WMT* injected via transendoscopic enteral tubing or nasojejunal tube daily for 6 days. Participants received two treatments administered 4 weeks apart. | 8 weeks after each treatment course |
| Kang 2017 [22] | Open-label, non-randomized clinical trial | 2-week antibiotic treatment with vancomycin, Prilosec, and Moviprep followed by a clear liquid diet the day before FMT | Initial high dose of FMT administered orally followed by lower oral dose daily for 8 weeks or one-time rectal dose of FMT followed by lower oral dose daily for 7 weeks. | 8 weeks after treatment |
| Li 2021 [13] | Open-label, non-randomized clinical trial | 2 L of polyethylene glycol | FMT administered orally via freeze-dried capsules or via colonoscopy once a week for 4 weeks. | 0 weeks and 8 weeks after treatment |
| Author/Year | Location (City, Country) | Population Characteristics | Sample Size (n) | Age (Mean) | Male (n) | Female (n) | BMI (Mean) | Baseline ABC Score (Mean) | Baseline CARS Score (Mean) | Baseline BSFS Score (Mean) |
|---|---|---|---|---|---|---|---|---|---|---|
| Pan 2022 [20] | Guangzhou, China | ASD children | 42 | 6.00 | 34 | 8 | 17.01 | 59.00 | 36.00 | 3.00 |
| Zhang 2022 [21] | Guangzhou, China | ASD children (24 with constipation, 25 without constipation) | 49 | 5.67 | 41 | 8 | NR | Constipation group: 56.21 Without constipation: 63.52 | Constipation group: 35.25 Without constipation 36.64 | Constipation group: 1.29 Without constipation 4.08 |
| Kang 2017 [22] | Phoenix, United States of America | ASD children who had moderate to severe gastrointestinal problems | 18 | 10.8 | 16 | 2 | 18.2 | NR | NR | No stool: 33% (n = 5.94) Type I/II: 19% (n = 3.42) Type VI or VII: 10% (n = 1.8) |
| Li 2021 [13] | Nanjing, China | ASD children who had symptoms of the GI tract (constipation, diarrhea) | 40 | 8.03 | 37 | 3 | 17.96 | NR | NR | NR |
| Author/Year | ABC Score end of First Treatment | ABC Score End of Additional Treatment(s) | ABC Score at Follow-Up | CARS Score End of First Treatment | CARS Score End of Additional Treatment(s) | CARS Score at Follow-Up |
|---|---|---|---|---|---|---|
| Pan 2022 [20] | Decrease (p < 0.001) | 2nd WMT **: Lower scores (p < 0.001) 3rd WMT: Lower scores (p < 0.001) 4th WMT: Lower scores (p < 0.01) 5th WMT: Lower scores (p < 0.05) | NR | Decrease (p < 0.0001) | 2nd WMT: Lower scores (p < 0.0001) 3rd WMT: Lower scores (p < 0.001) 4th WMT: Lower scores (p < 0.01) 5th WMT: Lower scores (p < 0.05) | NR |
| Zhang 2022 [21] | Constipation group: Decrease; 50.92 (p = 0.286). Non-constipation group: Decrease; 57.56 (p = 0.309). | 2nd WMT: Constipation group: Decrease; 46.54 (p = 0.046). Non-constipation group: Decrease; 52.88 (p = 0.053). | NR | Constipation group: Decrease; 33.15 (p = 0.059). Non-constipation group: Decrease; 34.54 (p = 0.033). | 2nd WMT: Constipation group: Decrease; 32.50 (p = 0.015). Non-constipation group: Decrease; 33.88 (p = 0.002). | NR |
| Kang 2017 [22] | Decrease (p < 0.01). | N/A | Scores remained lower 8 eight weeks after treatment compared to baseline (p < 0.01). | Decrease (p < 0.001). | N/A | Scores remained lower 8 weeks after treatment (p < 0.001). |
| Li 2021 [13] | Decrease (p < 0.0001) | N/A | Scores remained lower 8 weeks after treatment (p < 0.01) | Decrease by 10% (p < 0.0001) | N/A | Scores remained lower by 6%, 8 weeks after treatment (p < 0.0001). |
| Author/Year | BSFS Scores | GSRS | Constipation Symptoms |
|---|---|---|---|
| Pan 2022 [20] | Lower scores after the 1st, 2nd, 3rd, and 4th WMT ** (p < 0.05) 18.92% improvement (p = 0.016) in the number of children with normal fecal form after the first treatment compared to baseline. | N/A | Reduced after each WMT when compared to baseline. 1st WMT: (p < 0.05); resolution of constipation in 23.8% of patients after 1st WMT: (p = 0.001). 2nd and 3rd WMT: (p < 0.01) 4th WMT: (p < 0.001) 5th WMT: (p < 0.05) |
| Zhang 2022 [21] | Constipation group: After 1st WMT: Increase; 2.33 (p = 0 < 0.001). After 2nd WMT: Increase; 2.92 (p < 0.001). Non-Constipation group: After 1st WMT: Decrease; 3.96 (p = 0.599). After 2nd WMT: Decrease; 4.00 (p = 0.337). | N/A | NR |
| Kang 2017 [22] | Reduction in the reported percent of days with:
| Average score dropped 82% from the beginning to the end of treatment (p < 0.001) and remained 77% improved 8 weeks after treatment (p < 0.001). | Reduction in the reported percent of days with no stool by 7% (p = 0.29) at end of treatment and 8 weeks after treatment |
| Li 2021 [13] | 60% of participants reporting hard stools (BSFS Type I/Type II) reduced to 10% at week 12 (p < 0.001). | Average scores decreased by 35% at the end of the 4-week treatment (p < 0.0001) and remained improved 8 weeks after treatment (p < 0.0001). | NR |
| WMT ** Course | Δ ABC Scores (mean) | Δ CARS Scores (mean) |
|---|---|---|
| Second vs. first | −6.50 vs. −5.00, p = 0.045 | NR |
| Third vs. second | 14.04 vs. 8.83, p = 0.022 | NR |
| Fourth vs. third | 13.57 vs. 11.57, p = 0.527 | 2.75 vs. 2.00, p = 0.930 |
| Fifth vs. fourth | 19.40 vs. 16.60, p = 0.351 | 3.92 vs. 1.58, p = 0.084 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dossaji, Z.; Khattak, A.; Tun, K.M.; Hsu, M.; Batra, K.; Hong, A.S. Efficacy of Fecal Microbiota Transplant on Behavioral and Gastrointestinal Symptoms in Pediatric Autism: A Systematic Review. Microorganisms 2023, 11, 806. https://doi.org/10.3390/microorganisms11030806
Dossaji Z, Khattak A, Tun KM, Hsu M, Batra K, Hong AS. Efficacy of Fecal Microbiota Transplant on Behavioral and Gastrointestinal Symptoms in Pediatric Autism: A Systematic Review. Microorganisms. 2023; 11(3):806. https://doi.org/10.3390/microorganisms11030806
Chicago/Turabian StyleDossaji, Zahra, Adam Khattak, Kyaw Min Tun, Mark Hsu, Kavita Batra, and Annie S. Hong. 2023. "Efficacy of Fecal Microbiota Transplant on Behavioral and Gastrointestinal Symptoms in Pediatric Autism: A Systematic Review" Microorganisms 11, no. 3: 806. https://doi.org/10.3390/microorganisms11030806
APA StyleDossaji, Z., Khattak, A., Tun, K. M., Hsu, M., Batra, K., & Hong, A. S. (2023). Efficacy of Fecal Microbiota Transplant on Behavioral and Gastrointestinal Symptoms in Pediatric Autism: A Systematic Review. Microorganisms, 11(3), 806. https://doi.org/10.3390/microorganisms11030806