
Nosocomial Infections in Adult Patients Supported by Extracorporeal Membrane Oxygenation in a Cardiac Intensive Care Unit

 , , ,
, , ,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Patients
2.2. Cannulation Characteristics
2.3. Antimicrobial Surveillance and Standard of Care
2.4. Nosocomial Infections
2.5. Variables Analyzed
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Risk Factors Associated with Infection Development
3.2. Type of Nosocomial Infection and Microbiology
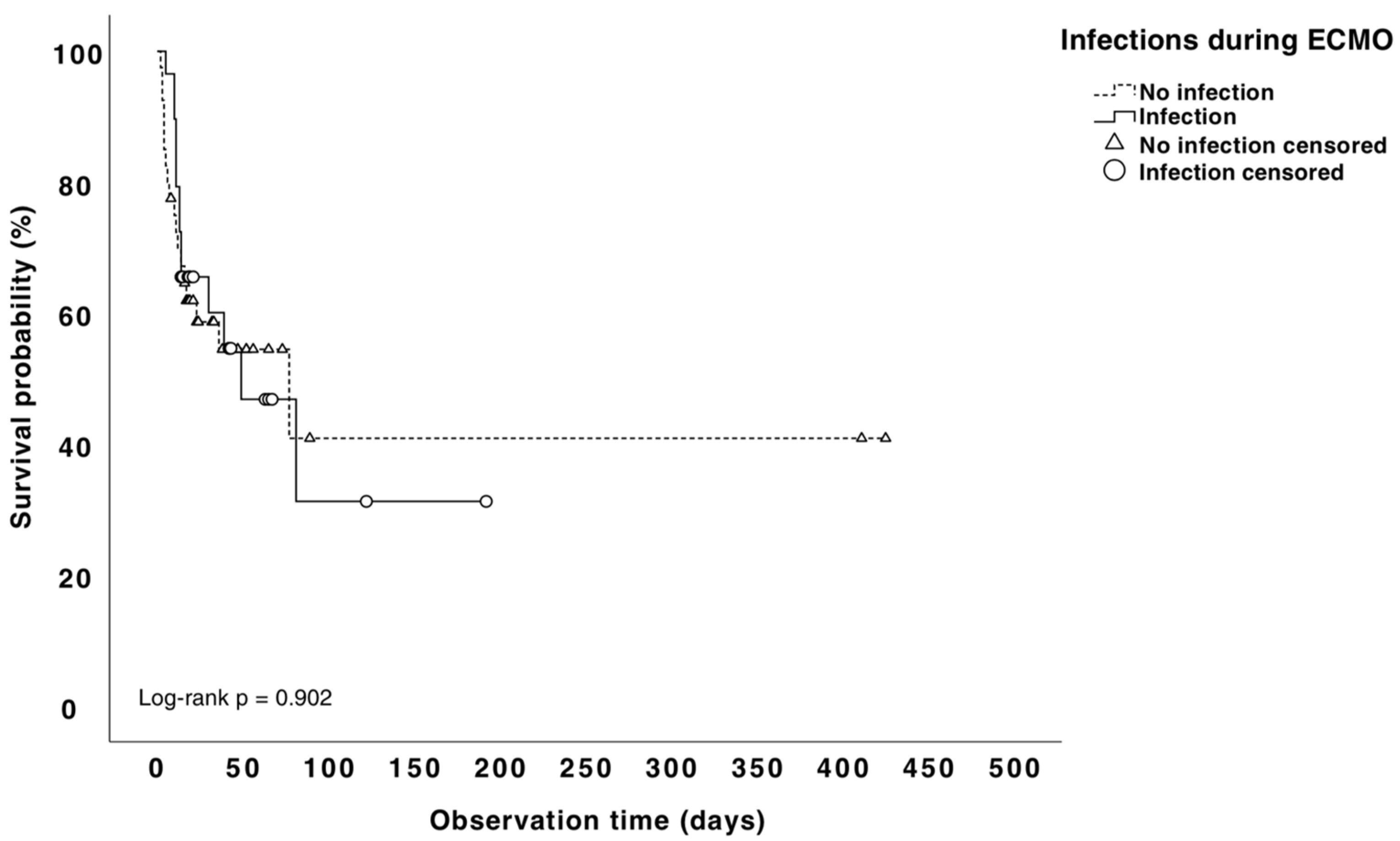
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Keebler, M.E.; Haddad, E.V.; Choi, C.W.; McGrane, S.; Zalawadiya, S.; Schlendorf, K.H.; Brinkley, D.M.; Danter, M.R.; Wigger, M.; Menachem, J.N.; et al. Venoarterial Extracorporeal Membrane Oxygenation in Cardiogenic Shock. JACC Heart Fail. 2018, 6, 503–516. [Google Scholar] [CrossRef]
- ELSO Society. ECLS Registry Report. International Summary January 2020; ECMO Registry of the Extracorporeal Life Support Organization (ELSO): Ann Arbor, MI, USA, 2020; pp. 1–37. [Google Scholar]
- Bougouin, W.; Aissaoui, N.; Combes, A.; Deye, N.; Lamhaut, L.; Jost, D.; Maupain, C.; Beganton, F.; Bouglé, A.; Karam, N.; et al. Post-cardiac arrest shock treated with veno-arterial extracorporeal membrane oxygenation: An observational study and propensity-score analysis. Resuscitation 2017, 110, 126–132. [Google Scholar] [CrossRef]
- Pineton De Chambrun, M.; Bréchot, N.; Combes, A. Venoarterial extracorporeal membrane oxygenation in cardiogenic shock: Indications, mode of operation, and current evidence. Curr. Opin. Crit. Care 2019, 25, 397–402. [Google Scholar] [CrossRef]
- Combes, A.; Leprince, P.; Luyt, C.-E.; Bonnet, N.; Trouillet, J.-L.; Léger, P.; Pavie, A.; Chastre, J. Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock*. Crit. Care Med. 2008, 36, 1404–1411. [Google Scholar] [CrossRef]
- Cheng, R.; Hachamovitch, R.; Kittleson, M.; Patel, J.; Arabia, F.; Moriguchi, J.; Esmailian, F.; Azarbal, B. Complications of Extracorporeal Membrane Oxygenation for Treatment of Cardiogenic Shock and Cardiac Arrest: A Meta-Analysis of 1866 Adult Patients. Ann. Thorac. Surg. 2014, 97, 610–616. [Google Scholar] [CrossRef]
- Cheng, R.; Kittleson, M.; Moriguchi, J.; Esmailian, F.; Azarbal, B. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: A weighted meta-analysis. J. Am. Coll. Cardiol. 2013, 61, E638. [Google Scholar] [CrossRef]
- Maclaren, G.; Schlapbach, L.J.; Aiken, A.M.; Bchir, M.B. Nosocomial Infections During Extracorporeal Membrane Oxygenation in Neonatal, Pediatric, and Adult Patients: A Comprehensive Narrative Review. Pediatr. Crit. Care Med. 2019, 21, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.S.; Lee, K.S.; Park, C.K.; Kang, S.K.; Kim, D.W.; Oh, S.G.; Oh, B.S.; Jung, Y.; Kim, S.; Yun, J.S.; et al. Nosocomial infection in adult patients undergoing veno-arterial extracorporeal membrane oxygenation. J. Korean Med. Sci. 2017, 32, 593–598. [Google Scholar] [CrossRef]
- Garner, J.S.; Jarvis, W.R.; Emori, T.G.; Horan, T.C.; Hughes, J.M. CDC definitions for nosocomial infections, 1988. Am. J. Infect. Control 1988, 16, 128–140. [Google Scholar] [CrossRef] [PubMed]
- CDC, Ncezid & DHQP. Pneumonia (Ventilator-Associated [VAP] and Non-Ventilator-Associated Pneumonia [PNEU]) Event; CDC: Atlanta, GA, USA, 2021.
- Salluh, J.I.F.; de Souza-Dantas, V.C.; Martin-Loeches, I.; Lisboa, T.C.; Rabello, L.S.C.F.; Saad, N.; Póvoa, P. Ventilator-associated tracheobronchitis: An update. Rev. Bras. Ter. Intensiv. 2019, 31, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Silvetti, S.; Ranucci, M.; Pistuddi, V.; Isgrò, G.; Ballotta, A.; Ferraris, L.; Cotza, M. Bloodstream infections during post-cardiotomy extracorporeal membrane oxygenation: Incidence, risk factors, and outcomes. Int. J. Artif. Organs 2018, 42, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Scaravilli, V.; Di Bella, S.; Biffi, S.; Bombino, M.; Patroniti, N.; Bisi, L.; Peri, A.M.; Pesenti, A.; Gori, A.; et al. Nosocomial infections during extracorporeal membrane oxygenation: Incidence, etiology, and impact on patients’ outcome. Crit. Care Med. 2017, 45, 1726–1733. [Google Scholar] [CrossRef]
- Brown, K.L.; Ridout, D.A.; Shaw, M.; Dodkins, I.; Smith, L.C.; O’Callaghan, M.A.; Goldman, A.P.; Macqueen, S.; Hartley, J.C. Healthcare-associated infection in pediatric patients on extracorporeal life support: The role of multidisciplinary surveillance. Pediatr. Crit. Care Med. 2006, 7, 546–550. [Google Scholar] [CrossRef]
- Calderón Checa, R.M.; Rojo Conejo, P.; González-Posada Flores, A.F.; Llorente de la Fuente, A.M.; Palacios Cuesta, A.; Aguilar, J.M.; Belda Hofheinz, S. Experience with infections in the use of extracorporeal membrane oxygenation. An. Pediatr. 2018, 89, 86–91. [Google Scholar] [CrossRef]
- Bizzarro, M.J.; Conrad, S.A.; Kaufman, D.A.; Rycus, P. Infections acquired during extracorporeal membrane oxygenation in neonates, children, and adults. Pediatr. Crit. Care Med. 2011, 12, 277–281. [Google Scholar] [CrossRef]
- O’Neill, J.; Schutze, G.; Heulitt, M.; Simpson, P.; Taylor, B. Nosocomial infections during extracorporeal membrane oxygenation. Intensive Care Med. 2001, 27, 1247–1253. [Google Scholar] [CrossRef]
- Hsu, M.S.; Chiu, K.M.; Huang, Y.T.; Kao, K.L.; Chu, S.H.; Liao, C.H. Risk factors for nosocomial infection during extracorporeal membrane oxygenation. J. Hosp. Infect. 2009, 73, 210–216. [Google Scholar] [CrossRef]
- Burket, J.S.; Bartlett, R.H.; Hyde, K.V.; Chenoweth, C.E. Nosocomial Infections in Adult Patients Undergoing Extracorporeal Membrane Oxygenation. Clin. Infect. Dis. 1999, 28, 828–833. [Google Scholar] [CrossRef]
- Schmidt, M.; Bréchot, N.; Hariri, S.; Guiguet, M.; Luyt, C.E.; Makri, R.; Leprince, P.; Trouillet, J.L.; Pavie, A.; Chastre, J.; et al. Nosocomial infections in adult cardiogenic shock patients supported by venoarterial extracorporeal membrane oxygenation. Clin. Infect. Dis. 2012, 55, 1633–1641. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Jeon, K.-H.; Lee, H.J.; Kim, J.-B.; Jang, H.-J.; Kim, J.S.; Kim, T.H.; Park, J.-S.; Choi, R.K.; Choi, Y.J. Complications of veno-arterial extracorporeal membrane oxygenation for refractory cardiogenic shock or cardiac arrest. Int. J. Artif. Organs 2019, 43, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Solla-Buceta, M.; González-Vílchez, F.; Almenar-Bonet, L.; Lambert-Rodríguez, J.L.; Segovia-Cubero, J.; González-Costello, J.; Delgado, J.F.; Pérez-Villa, F.; Crespo-Leiro, M.G.; Rangel-Sousa, D.; et al. Infectious complications associated with short-term mechanical circulatory support in urgent heart transplant candidates. Rev. Española Cardiol. (Engl. Ed.) 2022, 75, 141–149. [Google Scholar] [CrossRef]
- Bouglé, A.; Bombled, C.; Margetis, D.; Lebreton, G.; Vidal, C.; Coroir, M.; Hajage, D.; Amour, J. Ventilator-associated pneumonia in patients assisted by veno-arterial extracorporeal membrane oxygenation support: Epidemiology and risk factors of treatment failure. PLoS ONE 2018, 13, e0194976. [Google Scholar] [CrossRef] [PubMed]
- Wałaszek, M.; Różańska, A.; Wałaszek, M.Z.; Wójkowska-Mach, J. Epidemiology of Ventilator-Associated Pneumonia, microbiological diagnostics and the length of antimicrobial treatment in the Polish Intensive Care Units in the years 2013–2015. BMC Infect. Dis. 2018, 18, 308. [Google Scholar] [CrossRef]
- De Rosa, F.G.; Corcione, S.; Pagani, N.; Stella, M.L.; Urbino, R.; Di Perri, G.; Ranieri, V.M. High rate of respiratory MDR gram-negative bacteria in H1N1-ARDS treated with ECMO. Intensive Care Med. 2013, 39, 1880–1881. [Google Scholar] [CrossRef]
- Limaye, A.P.; Kirby, K.A.; Rubenfeld, G.D.; Leisenring, W.M.; Bulger, E.M.; Neff, M.J.; Gibran, N.S.; Huang, M.-L.; Santo Hayes, T.K.; Corey, L.; et al. Cytomegalovirus Reactivation in Critically Ill Immunocompetent Patients. JAMA 2008, 300, 413–422. [Google Scholar] [CrossRef]
- Papazian, L.; Hraiech, S.; Lehingue, S.; Roch, A.; Chiche, L.; Wiramus, S.; Forel, J.-M. Cytomegalovirus reactivation in ICU patients. Intensive Care Med. 2016, 42, 28–37. [Google Scholar] [CrossRef]
- Martínez-Solano, J.; Sousa-Casasnovas, I.; Bellón-Cano, J.M.; García-Carreño, J.; Juárez-Fernández, M.; Díez-Delhoyo, F.; Sanz-Ruiz, R.; Devesa-Cordero, C.; Elízaga-Corrales, J.; Fernández-Avilés, F.; et al. Lactate levels as a prognostic predict in cardiogenic shock under venoarterial extracorporeal membrane oxygenation support. Rev. Esp. Cardiol. (Engl. Ed). 2021, 75, 595–603. [Google Scholar] [CrossRef]
- Schumacher, M.; Wangler, M.; Wolkewitz, M.; Beyersmann, J. Attributable mortality due to nosocomial infections. A simple and useful application of multistate models. Methods Inf. Med. 2007, 46, 595–600. [Google Scholar]
- Nguile-Makao, M.; Zahar, J.-R.; Français, A.; Tabah, A.; Garrouste-Orgeas, M.; Allaouchiche, B.; Goldgran-Toledano, D.; Azoulay, E.; Adrie, C.; Jamali, S.; et al. Attributable mortality of ventilator-associated pneumonia: Respective impact of main characteristics at ICU admission and VAP onset using conditional logistic regression and multi-state models. Intensive Care Med. 2010, 36, 781–789. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total (n = 69) | Noninfected = 40 (58%) | Infected = 29 (42.0%) | p |
|---|---|---|---|---|
| Baseline Characteristics | ||||
| Sex, male (%) | 57 (82.7%) | 31 (77.5) | 26 (89.7) | 0.218 |
| Age, median years (IQR) | 58 (50.5–62.8) | 59 (50–64.5) | 55 (50.6–61.1) | 0.491 |
| Underlying conditions (%): | ||||
| BMI > 25 kg/m2 | 35 (50.7) | 20 (50) | 15 (51.7) | 0.999 |
| Arterial hypertension | 33 (49.3) | 16 (42.1) | 17 (58.6) | 0.222 |
| Cigarette smoking * | 26 (38.8) | 12 (31.6) | 14 (48.3) | 0.365 |
| Stopped smoking > 5 years | 13 (19.4) | 9 (23.7) | 4 (13.8) | 0.365 |
| Dyslipidemia | 27 (40.3) | 13 (34.2) | 14 (48.3) | 0.317 |
| Peripheric vascular disease | 7 (10.4) | 4 (10.5) | 3 (10.3) | 0.999 |
| Cardiac disease | 52 (75.4) | 25 (62.5) | 27 (93.1) | 0.004 |
| Chronic pulmonary disease | 8 (11.8) | 5 (12.5) | 3 (10.7) | 0.999 |
| Diabetes mellitus | 19 (27.5) | 9 (22.5) | 10 (34.5) | 0.290 |
| Liver cirrhosis | 1 (1.4) | 0 | 1 (3.4) | 0.420 |
| Chronic kidney failure | 9 (13) | 3 (7.5) | 6 (20.7) | 0.152 |
| Chronic renal replacement | 0 | 05 (12.5) | 0 | - |
| Immunosuppression: | 10 (14.5) | 5 (17.2) | 0.732 | |
| HIV infection (<200 CD4+) | 0 | |||
| Solid tumor with active CT | 0 | 0 | 0 | - |
| HT neoplasia/HSCT (<5 yrs) | 0 | 3 (7.5) | 0 | - |
| Solid organ transplant | 3 (4.3) | 0 | 0 | 0.258 |
| IS therapy/corticosteroids | 2 (2.9) | 2 (5) | 2 (6.9) | 0.173 |
| Autoimmune disease | 6 (8.7) | 2 (5) | 4 (13.8) | 0.230 |
| 5 (7.2) | 0 | 3 (10.3) | 0.643 | |
| 0 | 0 | - | ||
| Clinical and analytical data before ECMO | ||||
| Lactic acid prior to ECMO | 8.1 (4.9–12.2) | 8.7 (4.75–13.6) | 7.6 (5–10.7) | 0.202 |
| Serum creatinine prior to ECMO | 1 (0.9–1.3) | 0.9 (0.8–1.2) | 1.2 (0.9–1.6) | 0.027 |
| Days of MV before ECMO | 1.3 (0.6–2.0) | 1.3 (0.9–1.9) | 2 (0.5–5.5) | 0.930 |
| Ejective fraction (%) prior to ECMO | 18.1 (11.3–30.8) | 19.1 (10.8–34.2) | 17.3 (11.7–25.6) | 0.374 |
| RBC requirement before ECMO (5 U) (%) | 3 (4.3) | 3 (7.5) | 0 | 0.258 |
| Type of failure (%) | ||||
| Cardiac | 62 (89.9) | 36 (90) | 26 (89.7) | 0.999 |
| Cardiac + respiratory | 5 (7.2) | 3 (7.5) | 2 (6.9) | 0.999 |
| Respiratory | 2 (2.9) | 1 (2.5) | 1 (2.5) | 0.999 |
| ECMO indication: | ||||
| Cardiogenic shock | 38 (55.1) | 21 (52.5) | 17 (58.6) | 0.634 |
| Myocarditis | 1 (1.4) | 1 (2.5) | 0 | 0.999 |
| End-stage heart failure | 0 | 0 | 0 | - |
| Cardiac arrest | 21 (30.4) | 11 (27.5) | 10 (34.5) | 0.601 |
| Pulmonary embolism | 8 (11.6) | 6 (15) | 2 (6.9) | 0.453 |
| Arrhythmic storm | 13 (18.8) | 8 (20) | 5 (17.2%) | 0.999 |
| ECMO as bridge to heart Tx (%) | 9 (13%) | 5 (12.5) | 4 (13.8) | 0.999 |
| Cardiac arrest in the last 24 h (%) | 44 (66.7) | 26 (70.3) | 18 (62.1) | 0.600 |
| SOFA score | 7.9 (5.8–10.4) | 8.2 (6.30–10.0) | 7.0 (5.4–10.4) | 0.537 |
| Charlson comorbidity score | 2.8 (1.9–3.7) | 3 (2.0–4.0) | 2.7 (1.86–3.6) | 0.557 |
| Major surgery before ECMO (%) | 2 (2.9) | 2 (5) | 0 | 0.506 |
| Colonization before ECMO (%) | 21 (30.4) | 10 (25) | 11 (37.9) | 0.295 |
| MDR colonization | 0 | 0 | 0 | - |
| Any infection before ECMO (%) | 10 (14.5) | 9 (22.5) | 1 (3.4) | 0.037 |
| Antibiotics >24 h before ECMO (%) | 7 (5.2) | 2 (5) | 3 (10.3) | 0.643 |
| Clinical and Analytical Data during ECMO Support | Total (n = 69) | Noninfected = 40 (57.9%) | Infected = 29 (42.0%) | p |
|---|---|---|---|---|
| BCIAO (%) | 51 (76.1) | 26 (68.4) | 25 (86.2) | 0.147 |
| Peripheric cannulation (%) | 59 (86.8) | 35 (89.7) | 24 (82.8) | 0.481 |
| Cannulation time (minutes) SD | 25.7 (20.2–31.8) | 25.7 (20.3–33.1) | 25.71 (20.0–30.9) | 0.245 |
| Days on ECMO | 6.30 (4.6–9.4) | 5.73 (5.7–7.7) | 7.20 (5.4–10.4) | 0.053 |
| Complications during ECMO | 41 (61.2%) | 19 (46.3%) | 22 (53.7%) | 0.044 |
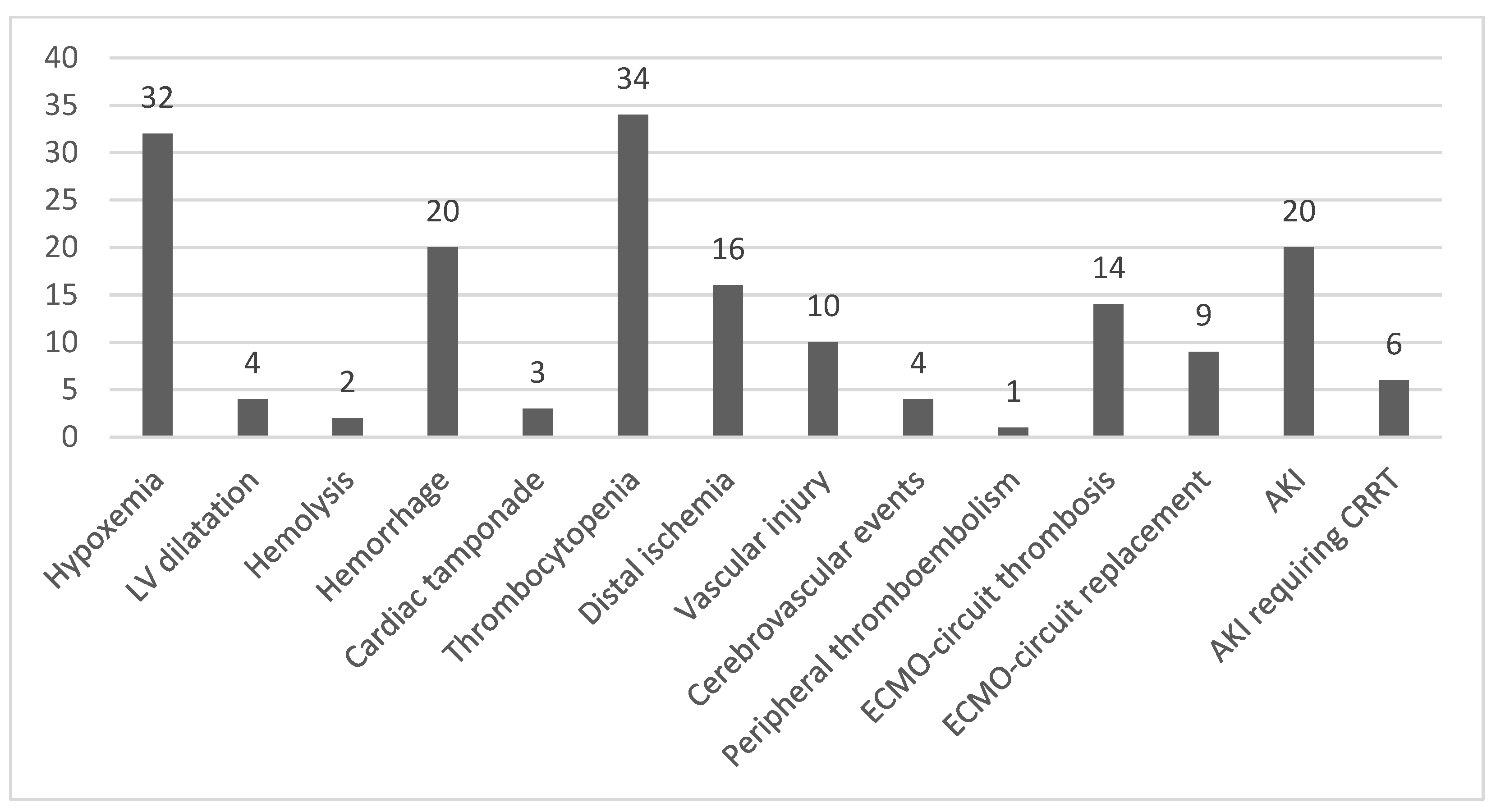
| Type of complications during ECMO (%) | ||||
| Cardiac failure | 44 (63.8) | 20 (50%) | 24 (82%) | 0.006 |
| Hypoxemia | 32 (47.8) | 17 (44.7) | 15 (51.7) | 0.627 |
| LV dilatation | 4 (6.0) | 1 (2.6) | 3 (10.3 | 0.308 |
| Hemolysis | 2 (3.0) | 1 (2.6) | 1 (3.4) | 0.999 |
| Hemorrhage | 20 (29.9) | 8 (21.1) | 12 (41.4) | 0.106 |
| Cardiac tamponade | 3 (4.5) | 2 (5.3) | 1 (3.4) | 0.999 |
| Thrombocytopenia | 34 (50.7) | 21 (55.3) | 13 (44.8) | 0.464 |
| Limb ischemia | 16 (23.9) | 9 (23.7) | 7 (24.1) | 0.966 |
| Vascular injury | 10 (14.9) | 5 (13.2) | 5 (17.2) | 0.736 |
| Cerebrovascular events | 4 (6.0) | 0 | 4 (13.8) | 0.031 |
| Peripheral thromboembolisms | 1 (1.5) | 0 | 1 (3.4) | 0.433 |
| Thrombosis of the circuit | 14 (20.9) | 5 (13.2) | 9 (31) | 0.128 |
| ECMO circuit replacement | 9 (10.8) | 4 (10.8) | 5 (17.9) | 0.483 |
| Acute kidney failure | 20 (29.4) | 12 (30.8) | 8 (27.6) | 0.796 |
| In CRRT | 6 (8.7) | 3 (7.5) | 3 (10.3) | 0.690 |
| Antiplatelet therapy (%) | 48 (72.7) | 27 (71.1) | 21 (75) | 0.785 |
| ASA | 3 (4.5) | 3 (7.9) | 0 | 0.256 |
| ASA + Clopidogrel | 3 (4.5) | 0 | 3 (10.7) | 0.072 |
| ASA + Dipiridamol | 40 (60.6) | 24 (63.2) | 16 (57.1) | 0.799 |
| Clopidogrel | 2 (3.0) | 0 | 2 (7.1) | 0.176 |
| Switch to C-ECMO (%) | 5 (7.5) | 1 (2.6) | 4 (13.8) | 0.158 |
| Lactic Acid (2 h), mg/dL, median | 5.8 (3.6–9.2) | 6.0 (6.0–9.9) | 5.3 (3.7–6.5) | 0.249 |
| Lactic Acid (4 h), mg/dL, median | 2.03 (1.5–4.0) | 2.13 (1.5–4.4) | 1.8 (1.3–3.2) | 0.670 |
| Colonization of ECMO cannula(%) | 2 (2.9) | 0 | 2 (6.9) | 0.173 |
| Outcome | ||||
| Switch from ECMO to another CV support (%) | 11 (15.9) | 5 (12.5) | 6 (20.7) | 0.507 |
| In-hospital stay, days | 20.3 (13.1–45.0) | 21.7 (11.3–45.0) | 19.3 (14.1–45.3) | 0.980 |
| ICU stay, days | 14 (9.5–25) | 12.4 (7.6–23.3) | 15.7 (10.9–34.3) | 0.860 |
| Mortality during ECMO (%) | 27 (39.1) | 18 (45) | 9 (31) | 0.319 |
| In-hospital mortality (%) | 33 (46.4) | 18 (46.2%) | 15 (50.0%) | 0.754 |
| Number of NI Episodes during ECMO | N = 34 (%) |
|---|---|
| Ventilator-associated pneumonia-associated organisms | 19 (55.9%) |
| Gram-negative bacteria | 8 |
| Klebsiella pneumoniae | 2 |
| Proteus mirabilis | 1 |
| Serratia marcescens | 1 |
| Burkholderia cepacia | 1 |
| Enterobacter cloacae | 1 |
| Enterobacter aerogenes | 1 |
| Acinetobacter baumannii | 1 |
| Gram-positive bacteria | 5 |
| S. aureus | 3 |
| MRSA a | 1 |
| Polymicrobial b | 3 |
| Virus | 1 |
| HSV-1 c | 1 |
| Unknown etiology (negative culture) | 2 |
| Tracheobronchitis | 3 (8.8%) |
| Enterobacter aerogenes | 2 |
| Stenotrophomonas maltophilia | 1 |
| Bloodstream infections | 3 (8.8%) |
| Pseudomonas aeruginosa | 1 |
| Coagulase-negative staphylococci | 2 |
| SSTI d | 3 (8.8%) |
| Morganella morganii | 1 |
| Staphylococcus lugdunensis | 1 |
| Coagulase-negative staphylococci | 1 |
| Intra-abdominal infections (Escherichia coli) | 1 (2.9%) |
| Clostridium difficile infection | 1 (2.9%) |
| Urinary tract infection (K. pneumoniae) | 1 (2.9%) |
| CMV e disease | 3 (8.8%) |
| Variable | N (%) | Alive = 36 | Death = 33 | p |
|---|---|---|---|---|
| Sex, male | 57 (82.6%) | 31 (86.1%) | 26 (78.8%) | 0.423 |
| Age (median, IQR) | 58 (IQR 20–75) | 55 (20–75) | 61 (27–69) | 0.416 |
| Body mass index > 25 | 33 (47.8) | 14 (38.9%) | 19 (57.6%) | 0.12 |
| Underlying condition | ||||
| Cardiac disease | 52 (75.4%) | 25 (69.4%) | 27 (81.8%) | 0.23 |
| Pulmonary disease | 8 (11.6%) | 4 (11.1%) | 4 (12.1%) | 1.00 |
| Diabetes mellitus | 18 (26.1%) | 11 (30.6%) | 7 (21.2%) | 0.37 |
| Liver cirrhosis | 1 (1.4%) | 1 (2.8%) | 0 (0%) | 1.00 |
| Chronic kidney insufficiency | 8 (11.6%) | 3 (8.3%) | 5 (15.2%) | 0.466 |
| Chronic renal replacement | 0 (0%) | 0 (0%) | 0 (0%) | – |
| Immunosuppression | 16 (10.1%) | 3 (8.3%) | 4 (12.1%) | 0.70 |
| HIV infection | 0 | 0 (0%) | 0 (0%) | – |
| Solid organ tumor under CT | 0 | 0 (0%) | 0 (0%) | – |
| Hematol. neoplasia/HSCT (<5 yrs) | 3 (4.3%) | 2 (5.6%) | 1 (3.0%) | 1.00 |
| Solid organ transplant | 2 (2.9%) | 1 (2.8%) | 1 (3.0%) | 1.00 |
| Immunosuppressive therapy/CCS * | 6 (8.7%) | 2 (5.6%) | 4 (12.1%) | 0.41 |
| Autoimmune disease | 5 (7.2%) | 3 (8.3%) | 2 (6.1%) | 1.00 |
| ECMO indication | ||||
| Cardiocirculatory failure | 60 (87.0%) | 35 (97.2%) | 25 (75.8%) | 0.008 |
| As bridge to heart Tx | 9 (13%) | 9 (25%) | 0 (0%) | 0.002 |
| Respiratory failure | 4 (5.8%) | 0 (0%) | 4 (12.1%) | 0.047 |
| Cardiorespiratory failure | 5 (7.2%) | 1 (2.8%) | 4 (12.1%) | 0.18 |
| Type of cannulation | ||||
| Veno-venous | 2 (2.9%) | 0 | 2 (6.7%) | 0.18 |
| Venous artery | 66 (95.7%) | 38 (97.4%) | 28 (93.3%) | 0.57 |
| Other | 1 (1.4%) | 1 (2.6%) | 0 | 1.00 |
| Femoral cannulation | 66 (95.7%) | 39 (100%) | 27 (90%) | 0.70 |
| Days on ECMO | 6 (5–35) | 6 (2–26) | 7 (2–35) | 0.14 |
| Renal replacement therapy | 6 (8.7%) | 1(2.8%) | 5(15.2%) | 0.097 |
| Days of MV before ECMO | 1 (1–20) | 1 (1–6) | 1 (1–20) | 0.28 |
| Total days of MV | 1 (1–2.7) | 1 (1–6) | 1 (1–20) | 0.28 |
| SOFA score | 8 (2–17) | 7.5 (2–13) | 9 (13–17) | 0.051 |
| Charlson score | 3 (0–7) | 2 (0–6) | 3 (0–7) | 0.14 |
| Colonization before ECMO | 21 (30.4%) | 10 (27.8%) | 11 (33.3%) | 0.61 |
| MDR colonization | 1 (1.4%) | 0 (0%) | 1 (3.0%) | 0.47 |
| Infections due to the same microorganisms during ECMO | 0 | 0 (0%) | 0 (0%) | |
| ECMO cannula colonization | 2 (2.9%) | 2 (5.6%) | 0 (0%) | 0.49 |
| Microorganism | ||||
| Propionibacterium | 1 (1.4%) | |||
| Enterobacter cloacae | 1 (1.4%) | |||
| Other VAD requirement | 4 (5.8%) | |||
| Antibiotics > 24 h before ECMO | 6 (8.7%) | 2 (5.6%) | 4 (12.1%) | 0.41 |
| Adequate empirical antimicrobial therapy | 12 (17.4%) | 6 (16.7%) | 6 (18.2%) | 0.86 |
| Endpoints | ||||
| Length of in-hospital stay | 20 (4–411) | 36 (9–411) | 14 (4–78) | 0.01 |
| Length of CICU stay | 14 (2–405) | 15 (5–405) | 12 (2–49) | 0.15 |
| Mayor surgery before ECMO | 4 (5.8%) | 1 (2.8%) | 3 (9.1%) | 0.34 |
| BSI or VAP related mortality | 5 (7.2%) | – | – | – |
| Mortality after ECMO weaning | 28 (40.6%) | – | – | – |
| In-hospital mortality | 33 (47.8%) | – | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mornese Pinna, S.; Sousa Casasnovas, I.; Olmedo, M.; Machado, M.; Juàrez Fernández, M.; Devesa-Cordero, C.; Galar, A.; Alvarez-Uria, A.; Fernández-Avilés, F.; García Carreño, J.; et al. Nosocomial Infections in Adult Patients Supported by Extracorporeal Membrane Oxygenation in a Cardiac Intensive Care Unit. Microorganisms 2023, 11, 1079. https://doi.org/10.3390/microorganisms11041079
Mornese Pinna S, Sousa Casasnovas I, Olmedo M, Machado M, Juàrez Fernández M, Devesa-Cordero C, Galar A, Alvarez-Uria A, Fernández-Avilés F, García Carreño J, et al. Nosocomial Infections in Adult Patients Supported by Extracorporeal Membrane Oxygenation in a Cardiac Intensive Care Unit. Microorganisms. 2023; 11(4):1079. https://doi.org/10.3390/microorganisms11041079
Chicago/Turabian StyleMornese Pinna, Simone, Iago Sousa Casasnovas, María Olmedo, Marina Machado, Miriam Juàrez Fernández, Carolina Devesa-Cordero, Alicia Galar, Ana Alvarez-Uria, Francisco Fernández-Avilés, Jorge García Carreño, and et al. 2023. "Nosocomial Infections in Adult Patients Supported by Extracorporeal Membrane Oxygenation in a Cardiac Intensive Care Unit" Microorganisms 11, no. 4: 1079. https://doi.org/10.3390/microorganisms11041079
APA StyleMornese Pinna, S., Sousa Casasnovas, I., Olmedo, M., Machado, M., Juàrez Fernández, M., Devesa-Cordero, C., Galar, A., Alvarez-Uria, A., Fernández-Avilés, F., García Carreño, J., Martínez-Sellés, M., De Rosa, F. G., Corcione, S., Bouza, E., Muñoz, P., & Valerio, M. (2023). Nosocomial Infections in Adult Patients Supported by Extracorporeal Membrane Oxygenation in a Cardiac Intensive Care Unit. Microorganisms, 11(4), 1079. https://doi.org/10.3390/microorganisms11041079