
Cutibacterium avidum: A Potent and Underestimated Pathogen in Prosthetic Hip Joint Infections

 and
and
Abstract
:1. Introduction
2. Case Presentations
2.1. Case 1
2.2. Case 2
2.3. Case 3
2.4. Case 4
3. Methods
3.1. Bacterial Isolates
3.2. Antibiotic Susceptibility Testing
3.3. Genome Sequencing and Analysis
4. Results
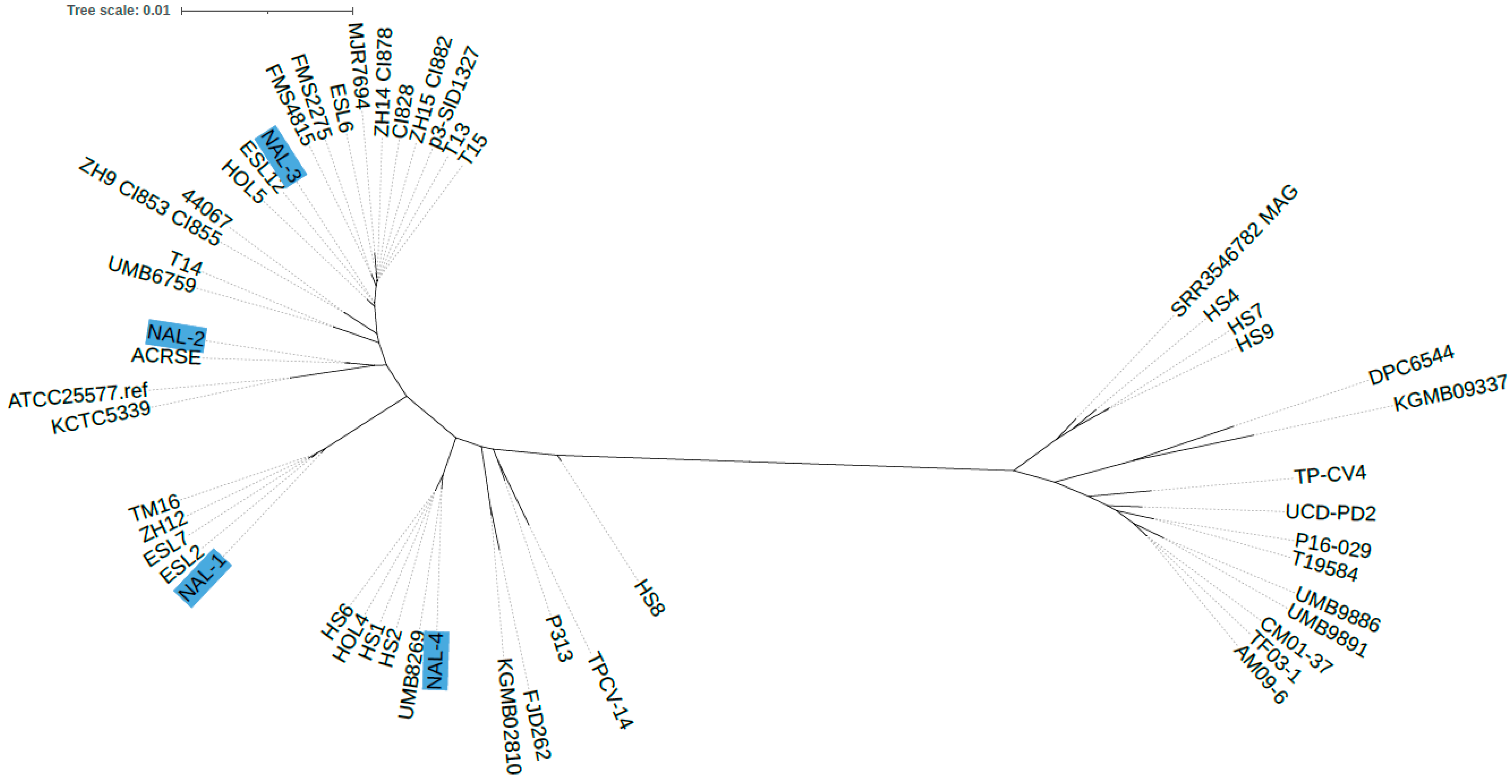
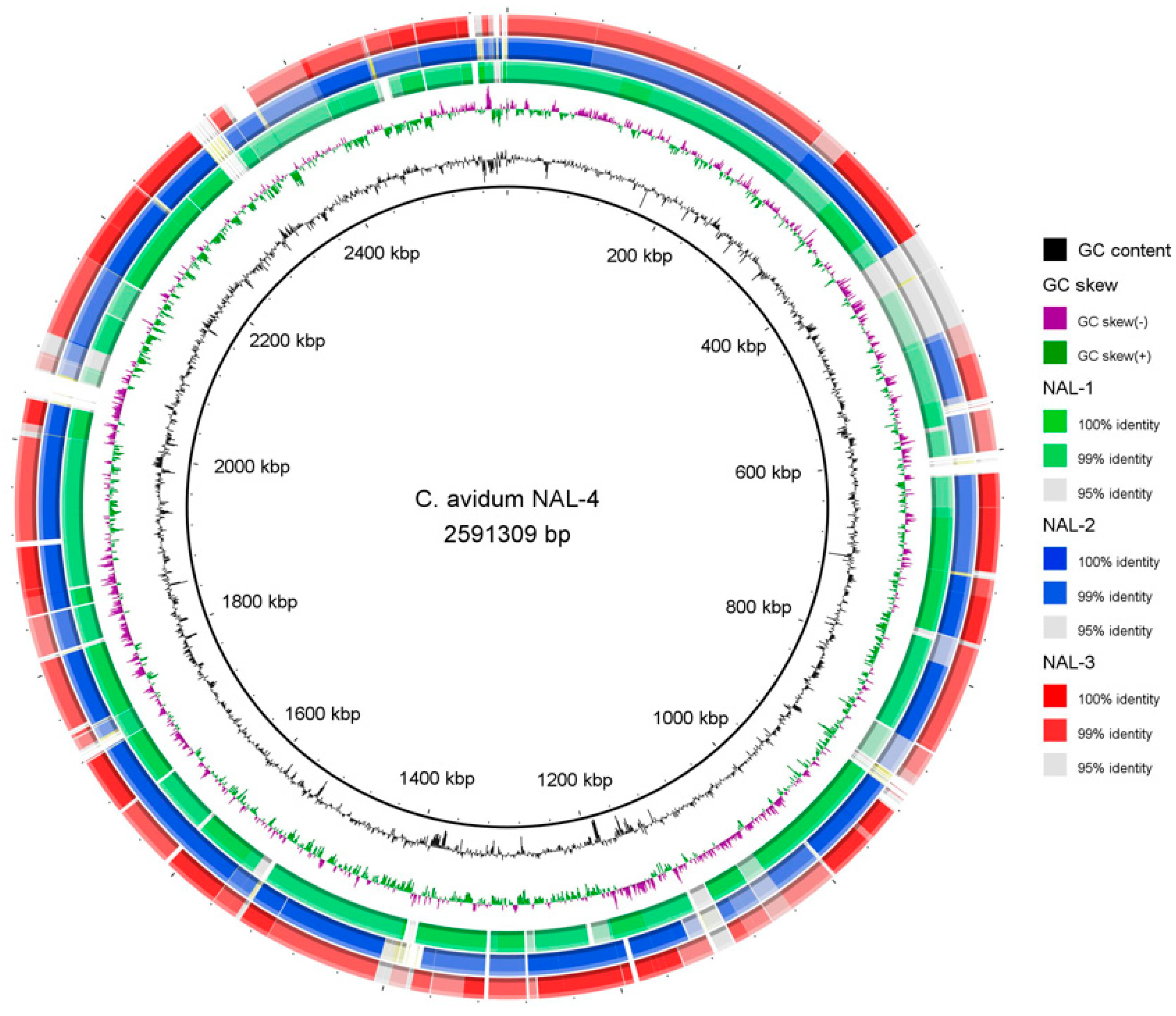
4.1. Genome Sequencing of C. avidum Isolates
4.2. Antibiotic Susceptibility Testing
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wildeman, P.; Rolfson, O.; Söderquist, B.; Wretenberg, P.; Lindgren, V. What Are the Long-Term Outcomes of Mortality, Quality of Life, and Hip Function after Prosthetic Joint Infection of the Hip? A 10-Year Follow-up from Sweden. Clin. Orthop. Relat. Res. 2021, 479, 2203–2213. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [PubMed]
- Flurin, L.; Greenwood-Quaintance, K.E.; Patel, R. Microbiology of Polymicrobial Prosthetic Joint Infection. Diagn. Microbiol. Infect. Dis. 2019, 94, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Lutz, M.-F.; Berthelot, P.; Fresard, A.; Cazorla, C.; Carricajo, A.; Vautrin, A.-C.; Fessy, M.-H.; Lucht, F. Arthroplastic and Osteosynthetic Infections Due to Propionibacterium acnes: A Retrospective Study of 52 Cases, 1995–2002. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 739–744. [Google Scholar] [CrossRef]
- Zeller, V.; Ghorbani, A.; Strady, C.; Leonard, P.; Mamoudy, P.; Desplaces, N. Propionibacterium acnes: An Agent of Prosthetic Joint Infection and Colonization. J. Infect. 2007, 55, 119–124. [Google Scholar] [CrossRef]
- Nodzo, S.R.; Westrich, G.H.; Henry, M.W.; Miller, A.O. Clinical Analysis of Propionibacterium acnes Infection After Total Knee Arthroplasty. J. Arthroplast. 2016, 31, 1986–1989. [Google Scholar] [CrossRef]
- Renz, N.; Mudrovcic, S.; Perka, C.; Trampuz, A. Orthopedic Implant-Associated Infections Caused by Cutibacterium Spp.—A Remaining Diagnostic Challenge. PLoS ONE 2018, 13, e0202639. [Google Scholar] [CrossRef] [PubMed]
- Piper, K.E.; Jacobson, M.J.; Cofield, R.H.; Sperling, J.W.; Sanchez-Sotelo, J.; Osmon, D.R.; McDowell, A.; Patrick, S.; Steckelberg, J.M.; Mandrekar, J.N.; et al. Microbiologic Diagnosis of Prosthetic Shoulder Infection by Use of Implant Sonication. J. Clin. Microbiol. 2009, 47, 1878–1884. [Google Scholar] [CrossRef]
- Nystrom, L.M.; Wyatt, C.M.; Noiseux, N.O. Arthroplasty Infection by Priopionibacterium granulosum Treated with Reimplantation despite Ongoing Purulent-Appearing Fluid Collection. J. Arthroplast. 2013, 28, 198.e5–198.e8. [Google Scholar] [CrossRef]
- Wildeman, P.; Brüggemann, H.; Scholz, C.F.P.; Leimbach, A.; Söderquist, B. Propionibacterium avidum as an Etiological Agent of Prosthetic Hip Joint Infection. PLoS ONE 2016, 11, e0158164. [Google Scholar] [CrossRef]
- Zeller, V.A.; Letembet, V.-A.; Meyssonnier, V.A.; Heym, B.; Ziza, J.-M.; Marmor, S.D. Cutibacterium (Formerly Propionibacterium) avidum: A Rare but Avid Agent of Prosthetic Hip Infection. J. Arthroplast. 2018, 33, 2246–2250. [Google Scholar] [CrossRef]
- Achermann, Y.; Liu, J.; Zbinden, R.; Zingg, P.O.; Anagnostopoulos, A.; Barnard, E.; Sutter, R.; Li, H.; McDowell, A.; Zinkernagel, A.S. Propionibacterium avidum: A Virulent Pathogen Causing Hip Periprosthetic Joint Infection. Clin. Infect. Dis. 2018, 66, 54–63. [Google Scholar] [CrossRef]
- Aichmair, A.; Frank, B.J.H.; Singer, G.; Simon, S.; Dominkus, M.; Hofstaetter, J.G. Differential Microbiological Spectrum and Resistance Pattern in Periprosthetic Hip Joint Infections: A Matched-Cohort Analysis Comparing Direct Anterior versus Lateral Approach. BMC Musculoskelet. Disord. 2022, 23, 72. [Google Scholar] [CrossRef] [PubMed]
- Corvec, S. Clinical and Biological Features of Cutibacterium (Formerly Propionibacterium) avidum, an Underrecognized Microorganism. Clin. Microbiol. Rev. 2018, 31, e00064-17. [Google Scholar] [CrossRef] [PubMed]
- Mak, T.N.; Schmid, M.; Brzuszkiewicz, E.; Zeng, G.; Meyer, R.; Sfanos, K.S.; Brinkmann, V.; Meyer, T.F.; Brüggemann, H. Comparative Genomics Reveals Distinct Host-Interacting Traits of Three Major Human-Associated Propionibacteria. BMC Genom. 2013, 14, 640. [Google Scholar] [CrossRef] [PubMed]
- McGinley, K.J.; Webster, G.F.; Leyden, J.J. Regional Variations of Cutaneous Propionibacteria. Appl. Environ. Microbiol. 1978, 35, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Böni, L.; Kuster, S.P.; Bartik, B.; Zbinden, R.; Zingg, P.O.; Achermann, Y. Association of Cutibacterium avidum Colonization in the Groin with Obesity: A Potential Risk Factor for Hip Periprosthetic Joint Infection. Clin. Infect. Dis. 2018, 67, 1878–1882. [Google Scholar] [CrossRef] [PubMed]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A Flexible Trimmer for Illumina Sequence Data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef] [PubMed]
- Bankevich, A.; Nurk, S.; Antipov, D.; Gurevich, A.A.; Dvorkin, M.; Kulikov, A.S.; Lesin, V.M.; Nikolenko, S.I.; Pham, S.; Prjibelski, A.D.; et al. SPAdes: A New Genome Assembly Algorithm and Its Applications to Single-Cell Sequencing. J. Comput. Biol. 2012, 19, 455–477. [Google Scholar] [CrossRef]
- García-Alcalde, F.; Okonechnikov, K.; Carbonell, J.; Cruz, L.M.; Götz, S.; Tarazona, S.; Dopazo, J.; Meyer, T.F.; Conesa, A. Qualimap: Evaluating next-generation sequencing alignment data. Bioinformatics 2012, 28, 2678–2679. [Google Scholar] [CrossRef]
- Aziz, R.K.; Bartels, D.; Best, A.A.; DeJongh, M.; Disz, T.; Edwards, R.A.; Formsma, K.; Gerdes, S.; Glass, E.M.; Kubal, M.; et al. The RAST Server: Rapid Annotations Using Subsystems Technology. BMC Genom. 2008, 9, 75. [Google Scholar] [CrossRef]
- Treangen, T.J.; Ondov, B.D.; Koren, S.; Phillippy, A.M. The Harvest Suite for Rapid Core-Genome Alignment and Visualization of Thousands of Intraspecific Microbial Genomes. Genome Biol. 2014, 15, 524. [Google Scholar] [CrossRef]
- Price, M.N.; Dehal, P.S.; Arkin, A.P. FastTree 2—Approximately Maximum-Likelihood Trees for Large Alignments. PLoS ONE 2010, 5, e9490. [Google Scholar] [CrossRef]
- Letunic, I.; Bork, P. Interactive Tree Of Life (iTOL) v5: An Online Tool for Phylogenetic Tree Display and Annotation. Nucleic Acids Res. 2021, 49, W293–W296. [Google Scholar] [CrossRef]
- Alikhan, N.-F.; Petty, N.K.; Ben Zakour, N.L.; Beatson, S.A. BLAST Ring Image Generator (BRIG): Simple Prokaryote Genome Comparisons. BMC Genom. 2011, 12, 402. [Google Scholar] [CrossRef]
- Cunningham, S.A.; Rodriguez, C.; Woerther, P.-L.; Menigaux, C.; Bauer, T.; Herrmann, J.-L.; Rottman, M.; Roux, A.-L.; Gaillard, J.-L.; Patel, R.; et al. In Vivo Emergence of Dual Resistance to Rifampin and Levofloxacin in Osteoarticular Cutibacterium avidum. Microbiol. Spectr. 2023, 11, e0368722. [Google Scholar] [CrossRef]
- Simon, S.; Frank, B.J.H.; Hartmann, S.; Hinterhuber, L.; Reitsamer, M.; Aichmair, A.; Dominkus, M.; Söderquist, B.; Hofstaetter, J.G. Dalbavancin in Gram-Positive Periprosthetic Joint Infections. J. Antimicrob. Chemother. 2022, 77, 2274–2277. [Google Scholar] [CrossRef]
- Grice, E.A.; Segre, J.A. The Skin Microbiome. Nat. Rev. Microbiol. 2011, 9, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Maurer, S.M.; Kursawe, L.; Rahm, S.; Prinz, J.; Zinkernagel, A.S.; Moter, A.; Kuster, S.P.; Zbinden, R.; Zingg, P.O.; Achermann, Y. Cutibacterium avidum Resists Surgical Skin Antisepsis in the Groin—A Potential Risk Factor for Periprosthetic Joint Infection: A Quality Control Study. Antimicrob. Resist. Infect. Control 2021, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Ilchmann, T.; Zimmerli, W.; Bolliger, L.; Graber, P.; Clauss, M. Risk of Infection in Primary, Elective Total Hip Arthroplasty with Direct Anterior Approach or Lateral Transgluteal Approach: A Prospective Cohort Study of 1104 Hips. BMC Musculoskelet. Disord. 2016, 17, 471. [Google Scholar] [CrossRef] [PubMed]
- Swedish Artroplasty Register. Annunal Report. 2022. Available online: Https://Registercentrum.Blob.Core.Windows.Net/Sar/r/SAR-Annual-Report-2022_EN-HkgQE89Nus.Pdf (accessed on 28 October 2020).
- Ridberg, S.; Hellmark, B.; Nilsdotter, Å.; Söderquist, B. Cutibacterium acnes (Formerly Propionibacterium acnes) Isolated from Prosthetic Joint Infections Is Less Susceptible to Oxacillin than to Benzylpenicillin. J. Bone Jt. Infect. 2019, 4, 106–110. [Google Scholar] [CrossRef]
- Dettmer, A.; Melander, M.; Hallgren, H.C.B.; Adolfsson, L.E.; Salomonsson, B. The Choice of Antibiotic Prophylaxis Influences the Infection Reoperation Rate in Primary Shoulder Arthroplasty: Analysis from the Swedish Shoulder Arthroplasty Register. Clin. Orthop. Relat. Res. 2023, 481, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, J.; Nakase, K.; Hayashi, N.; Nasu, Y.; Hirai, Y.; Nakaminami, H. Multidrug-Resistant Cutibacterium avidum Isolated from Patients with Acne Vulgaris and Other Infections. J. Glob. Antimicrob. Resist. 2022, 28, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, J.; Nakase, K.; Nakaminami, H. Emergence of Cutibacterium avidum with erm(X) on a Mobile Genetic Element Identical to that of Cutibacterium acnes. Microbiol. Resour. Announc. 2023, 12, e0017823. [Google Scholar] [CrossRef] [PubMed]
- Legaria, M.C.; Barberis, C.; Camporro, J.; Traglia, G.M.; Famiglietti, A.; Stecher, D.; Vay, C.A. Intra-Peritoneal Abscess after an Abdominal Hysterectomy Involving Cutibacterium avidum (Former Propionibacterium avidum) Highly Resistant to Clindamycin. Anaerobe 2019, 59, 176–183. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Antibiotics | Case 1 | Case 2 | Case 3 | Case 4 |
|---|---|---|---|---|
| Penicillin G | 0.125 | 0.064 | 0.064 | 0.125 |
| Piperacillin/Tazobactam | 1.0 | 1.0 | 1.0 | 2 |
| Meropenem | 0.125 | 0.125 | 0.064 | 0.125 |
| Moxifloxacin | 0.125 | 0.125 | 0.125 | 0.125 |
| Vancomycin | 1 | 1 | 0.5 | 1 |
| Erytromycin | 0.032 | 0.032 | 0.032 | 0.016 |
| Clindamycin | 0.032 | 0.032 | 0.032 | 0.032 |
| Rifampicin | 0.008 | 0.004 | 0.004 | 0.004 |
| Metronidazole | >256 | >256 | >256 | >256 |
| Strain | Coverage | Contigs | GC | CDS | Length (bp) | GenBank Accession |
|---|---|---|---|---|---|---|
| NAL-1 | 212 | 18 | 63.4 | 2405 | 2,506,293 | JAXCLG000000000 |
| NAL-2 | 333 | 17 | 63.4 | 2385 | 2,510,992 | JAXCLH000000000 |
| NAL-3 | 323 | 16 | 63.4 | 2413 | 2,503,367 | JAXCLI000000000 |
| NAL-4 | 290 | 32 | 63.4 | 2468 | 2,591,309 | JAXCLJ000000000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karlsson, J.; Kamenska, N.; Matuschek, E.; Brüggemann, H.; Söderquist, B. Cutibacterium avidum: A Potent and Underestimated Pathogen in Prosthetic Hip Joint Infections. Microorganisms 2024, 12, 432. https://doi.org/10.3390/microorganisms12030432
Karlsson J, Kamenska N, Matuschek E, Brüggemann H, Söderquist B. Cutibacterium avidum: A Potent and Underestimated Pathogen in Prosthetic Hip Joint Infections. Microorganisms. 2024; 12(3):432. https://doi.org/10.3390/microorganisms12030432
Chicago/Turabian StyleKarlsson, Johanna, Nina Kamenska, Erika Matuschek, Holger Brüggemann, and Bo Söderquist. 2024. "Cutibacterium avidum: A Potent and Underestimated Pathogen in Prosthetic Hip Joint Infections" Microorganisms 12, no. 3: 432. https://doi.org/10.3390/microorganisms12030432
APA StyleKarlsson, J., Kamenska, N., Matuschek, E., Brüggemann, H., & Söderquist, B. (2024). Cutibacterium avidum: A Potent and Underestimated Pathogen in Prosthetic Hip Joint Infections. Microorganisms, 12(3), 432. https://doi.org/10.3390/microorganisms12030432