Diagnostic Value of Endotracheal Aspirates Sonication on Ventilator-Associated Pneumonia Microbiologic Diagnosis

 ,
,  , ,
, , 
 , and
, and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Population
2.2. Collection of Samples
2.3. Microbiological Analysis
2.4. Microscopy Images Acquisition
2.5. Statistical Analysis
3. Results
3.1. Population
3.2. Samples Collected
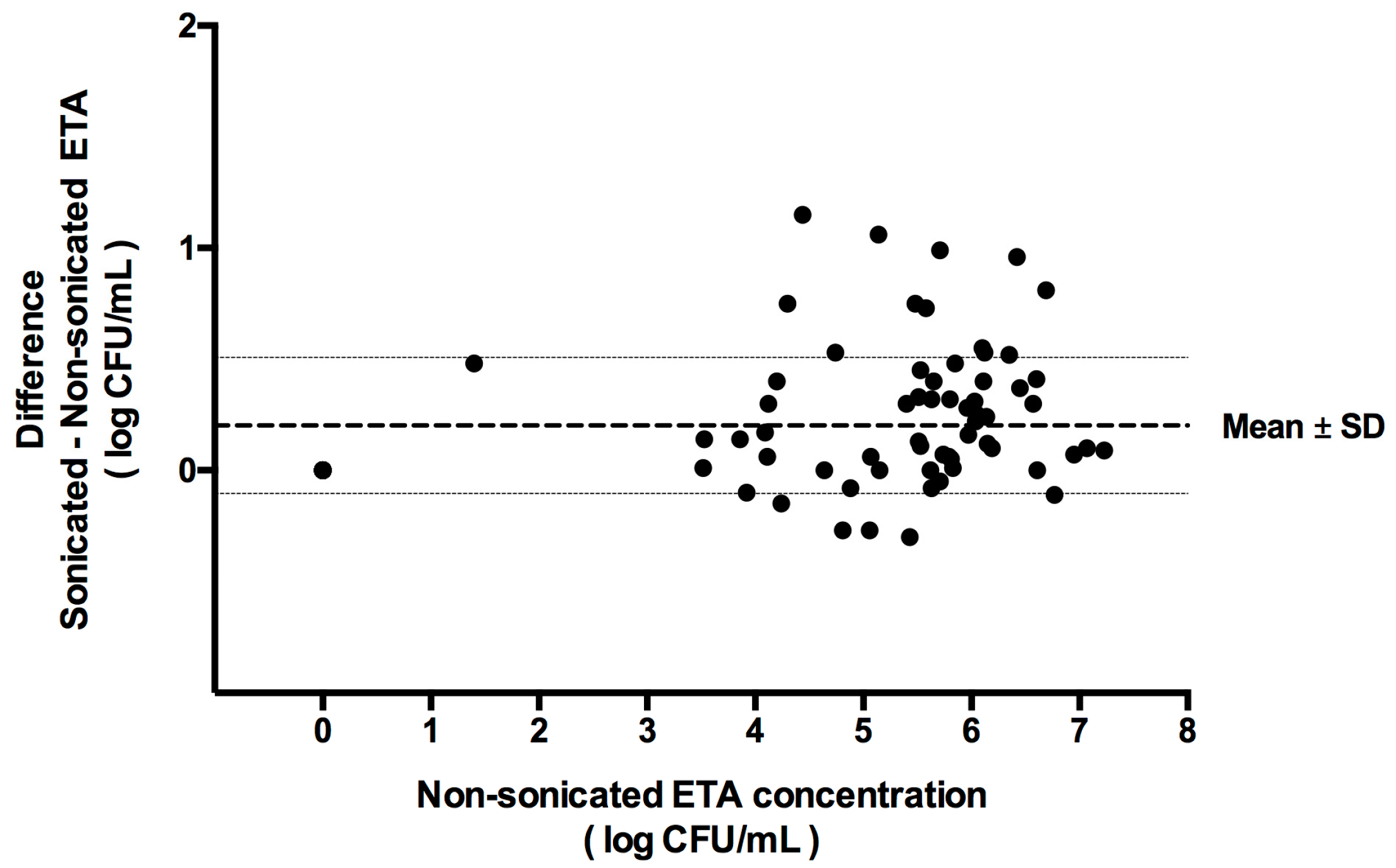
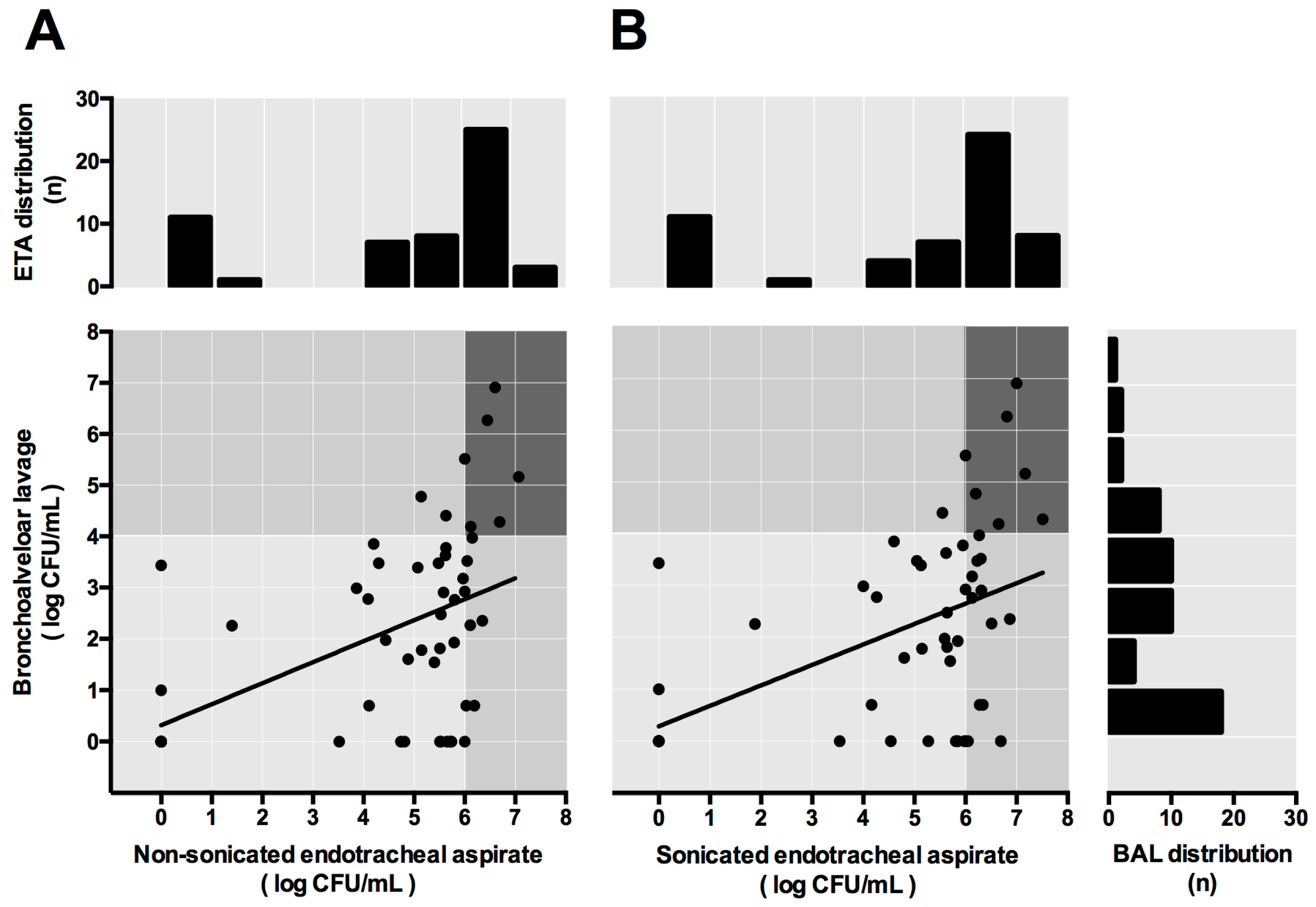
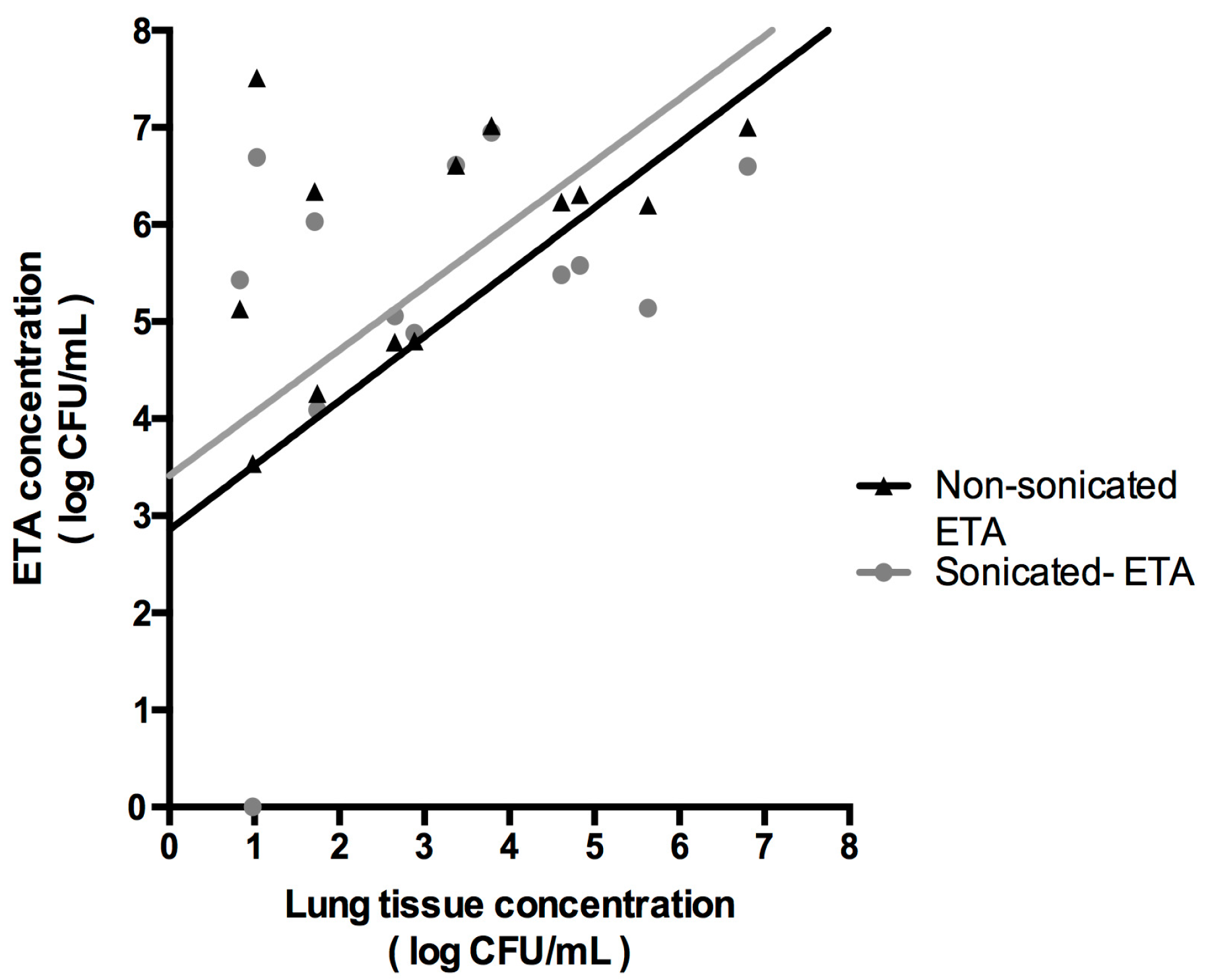
3.3. Standard Versus Sonicated Cultures
3.4. Sensitivity and Specificity
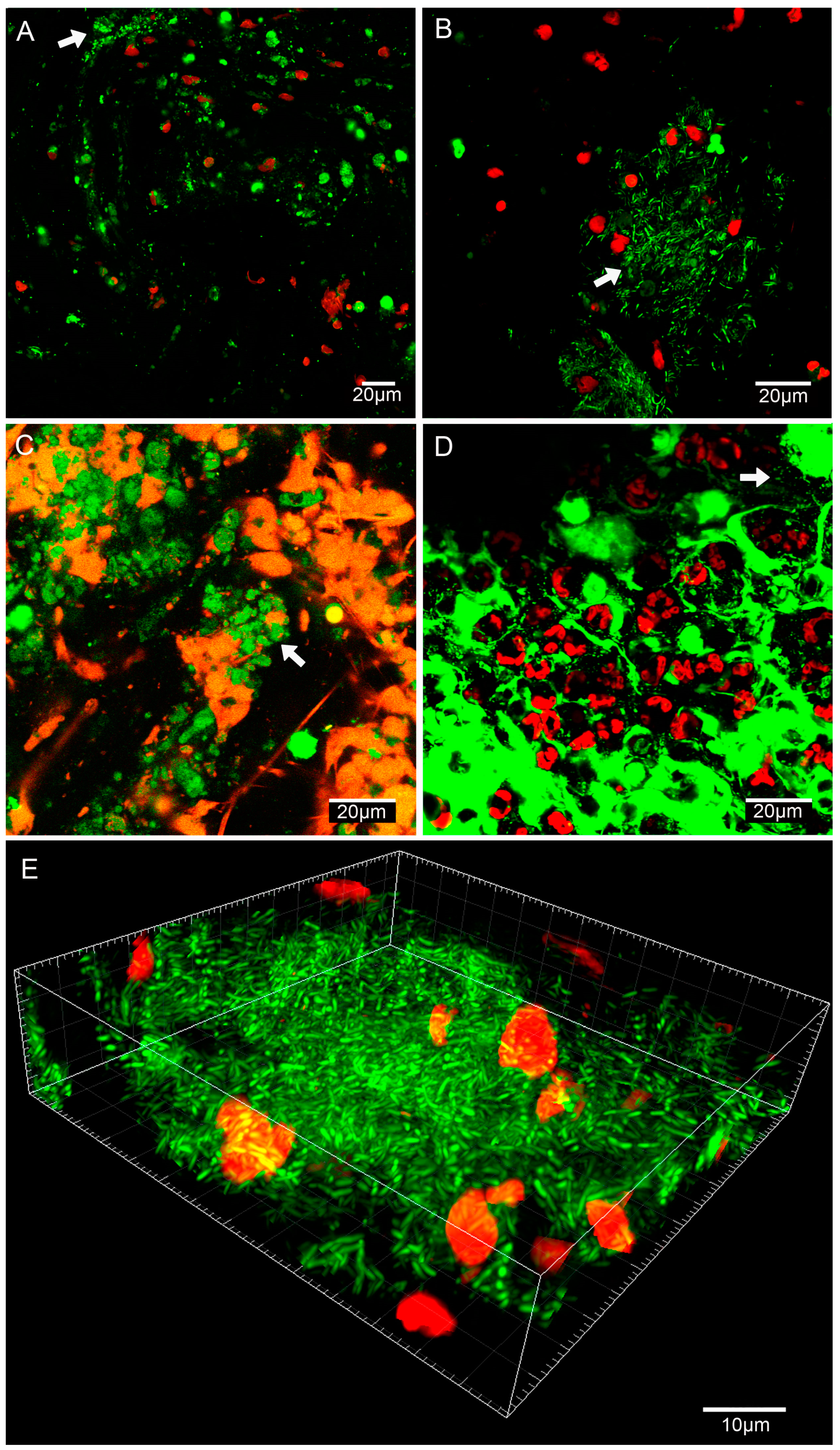
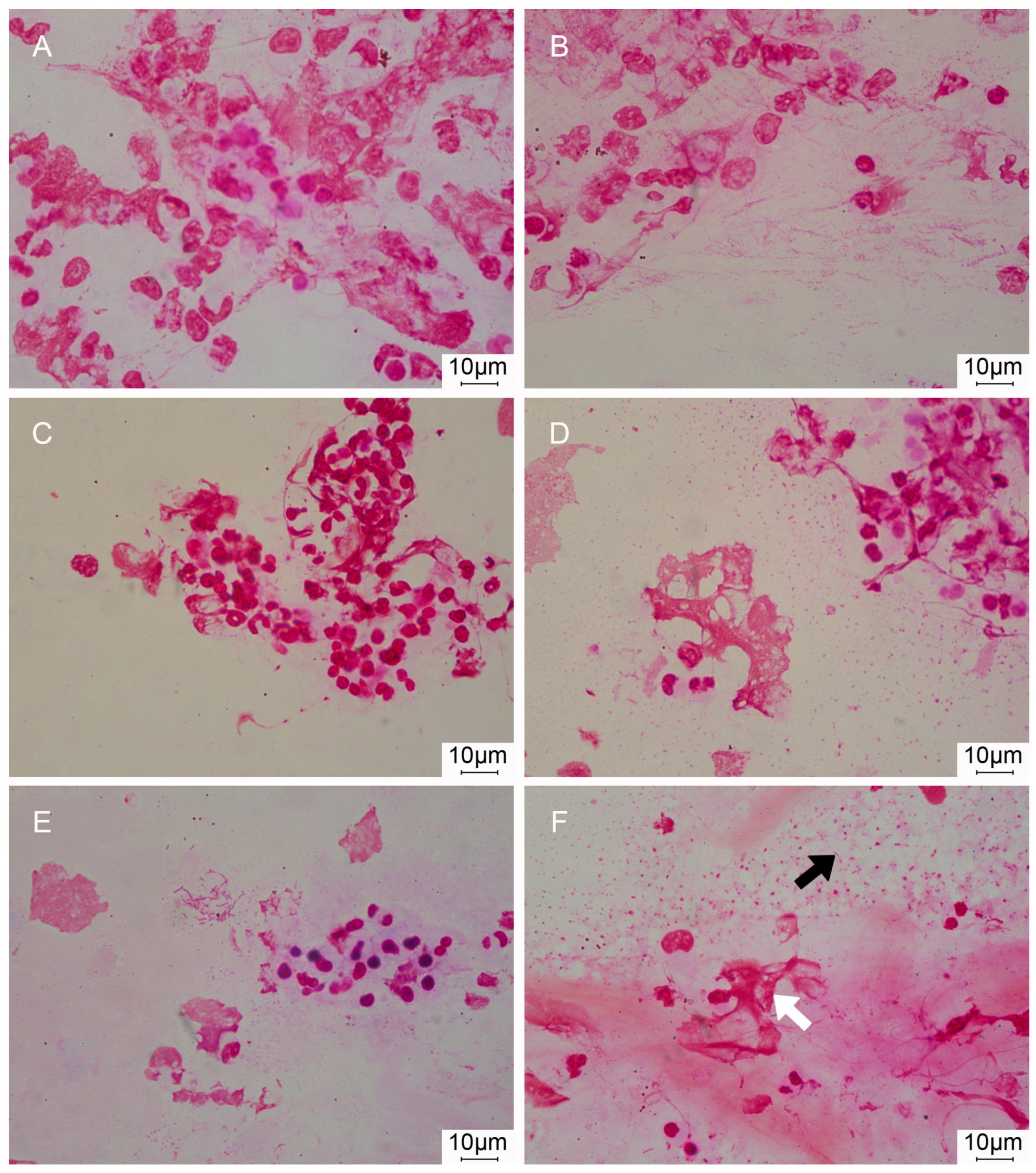
3.5. Imaging Biofilms
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Chastre, J.; Fagon, J.Y. Ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reporting on 2011 Surveillance Data and 2012 Epidemic Intelligence Data. Annual Epidemiological Report 2013. Stockholm: European Centre for Disease Prevention and Control (ECDC), 2013. Available online: https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/annual-epidemiological-report-2013.pdf (accessed on 18 September 2017).
- Planquette, B.; Timsit, J.F.; Misset, B.Y.; Schwebel, C.; Azoulay, E.; Adrie, C.; Vesin, A.; Jamali, S.; Zahar, J.R.; Allaouchiche, B.; et al. Pseudomonas aeruginosa ventilator-associated pneumonia. predictive factors of treatment failure. Am. J. Respir. Crit. Care Med. 2013, 188, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Hamilton, C.W.; Ernst, F.R. Economic impact of ventilator-associated pneumonia in a large matched cohort. Infect. Control Hosp. Epidemiol. 2012, 33, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Warren, D.K.; Shukla, S.J.; Olsen, M.A.; Kollef, M.H.; Hollenbeak, C.S.; Cox, M.J.; Cohen, M.M.; Fraser, V.J. Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit. Care Med. 2003, 31, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Burnham, C.D. Ventilator-Associated Pneumonia: The Role of Emerging Diagnostic Technologies. Semin. Respir. Crit. Care Med. 2017, 38, 253–263. [Google Scholar]
- Valencia, A.M.; Torres, M.A.; Insausti, O.J.; Alvarez, L.F.; Carrasco, J.N.; Herranz, C.M.; Tirapu Leon, J.P. Diagnostic value of quantitative cultures of endotracheal aspirate in ventilator-associated pneumonia: A Multicenter Study. Arch. Bronconeumol. 2003, 39, 394–399. [Google Scholar]
- Morris, A.C.; Kefala, K.; Simpson, A.J.; Wilkinson, T.S.; Everingham, K.; Kerslake, D.; Raby, S.; Laurenson, I.F.; Swann, D.G.; Walsh, T.S. Evaluation of the effect of diagnostic methodology on the reported incidence of ventilator-associated pneumonia. Thorax 2009, 64, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Fernandez-Barat, L. New developments in the diagnosis of VAP make bronchoalveolar lavage less useful: Some considerations. Intensive Care Med. 2014, 40, 1778–1779. [Google Scholar] [PubMed]
- Correa, R.A.; Luna, C.M.; Anjos, J.C.; Barbosa, E.A.; Rezende, C.J.; Rezende, A.P.; Pereira, F.H.; Rocha, M.O. Quantitative culture of endotracheal aspirate and BAL fluid samples in the management of patients with ventilator-associated pneumonia: A randomized clinical trial. J. Bras. Pneumol. 2014, 40, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, M. A randomized trial of diagnostic techniques for ventilator-associated pneumonia. N. Engl. J. Med. 2006, 355, 2619–2630. [Google Scholar]
- Ruiz, M.; Torres, A.; Ewig, S.; Marcos, M.A.; Alcón, A.; Lledó, R.; Asenjo, M.A.; Maldonado, A. Noninvasive versus invasive microbial investigation in ventilator-associated pneumonia: Evaluation of Outcome. Am. J. Respir. Crit. Care Med. 2000, 162, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Rea-Neto, A.; Youssef, N.C.; Tuche, F.; Brunkhorst, F.; Ranieri, V.M.; Reinhart, K.; Sakr, Y. Diagnosis of ventilator-associated pneumonia: A Systematic Review of the Literature. Crit. Care 2008, 12, R56. [Google Scholar] [CrossRef] [PubMed]
- Landry, R.M.; An, D.; Hupp, J.T.; Singh, P.K.; Parsek, M.R. Mucin-Pseudomonas aeruginosa interactions promote biofilm formation and antibiotic resistance. Mol. Microbiol. 2006, 59, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Worlitzsch, D.; Tarran, R.; Ulrich, M.; Schwab, U.; Cekici, A.; Meyer, K.C.; Birrer, P.; Bellon, G.; Berger, J.; Weiss, T.; et al. Effects of reduced mucus oxygen concentration in airway Pseudomonas infections of cystic fibrosis patients. J. Clin. Investig. 2002, 109, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Gries, D.M.; Pultz, N.J.; Donskey, C.J. Growth in cecal mucus facilitates colonization of the mouse intestinal tract by methicillin-resistant Staphylococcus aureus. J. Infect. Dis. 2005, 192, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Hall-Stoodley, L.; Stoodley, P. Evolving concepts in biofilm infections. Cell Microbiol. 2009, 11, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial biofilms: A Common Cause of Persistent Infections. Science 1999, 21, 1318–1322. [Google Scholar] [CrossRef]
- Trampuz, A.; Piper, K.E.; Jacobson, M.J.; Hanssen, A.D.; Unni, K.K.; Osmon, D.R.; Mandrekar, J.N.; Cockerill, F.R.; Steckelberg, J.M.; Greenleaf, J.F.; et al. Sonication of removed hip and knee prostheses for diagnosis of infection. N. Engl. J. Med. 2007, 357, 654–663. [Google Scholar] [CrossRef] [PubMed]
- Hoiby, N.; Bjarnsholt, T.; Moser, C.; Bassi, G.L.; Coenye, T.; Donelli, G.; Hall-Stoodley, L.; Hola, V.; Imbert, C.; Kirketerp-Moller, K.; et al. ESCMID guideline for the diagnosis and treatment of biofilm infections. Clin. Microbiol. Infect. 2015, 21, S1–S25. [Google Scholar] [CrossRef] [PubMed]
- Marsh, R.L.; Thornton, R.B.; Smith-Vaughan, H.C.; Richmond, P.; Pizzutto, S.J.; Chang, A.B. Detection of biofilm in bronchoalveolar lavage from children with non-cystic fibrosis bronchiectasis. Pediatr. Pulmonol. 2015, 50, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Barat, L.; Li, B.G.; Ferrer, M.; Bosch, A.; Calvo, M.; Vila, J.; Gabarrus, A.; Martinez-Olondris, P.; Rigol, M.; Esperatti, M.; et al. Direct analysis of bacterial viability in endotracheal tube biofilm from a pig model of methicillin-resistant Staphylococcus aureus pneumonia following antimicrobial therapy. FEMS Immunol. Med. Microbiol. 2012, 65, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Li, B.G.; Fernandez-Barat, L.; Saucedo, L.; Giunta, V.; Marti, J.D.; Tavares, R.O.; Aguilera, X.E.; Rigol, M.; Roca, I.; Munoz, L.; et al. Endotracheal tube biofilm translocation in the lateral Trendelenburg position. Crit. Care 2015, 19, 59. [Google Scholar]
- Martinez-Olondris, P.; Sibila, O.; Agusti, C.; Rigol, M.; Soy, D.; Esquinas, C.; Piner, R.; Luque, N.; Guerrero, L.; Quera, M.A.; et al. An experimental model of pneumonia induced by methicillin-resistent Staphylococcus aureus in ventilated piglets. Eur. Respir. J. 2010, 36, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Li, B.G.; Rigol, M.; Marti, J.D.; Saucedo, L.; Ranzani, O.T.; Roca, I.; Cabanas, M.; Munoz, L.; Giunta, V.; Luque, N.; et al. A novel porcine model of ventilator-associated pneumonia caused by oropharyngeal challenge with Pseudomonas aeruginosa. Anesthesiology 2014, 120, 1205–1215. [Google Scholar]
- Sibila, O.; Agusti, C.; Torres, A.; Baquero, S.; Gando, S.; Patron, J.R.; Morato, J.G.; Goffredo, D.H.; Bassi, N.; Luna, C.M. Experimental Pseudomonas aeruginosa pneumonia: Evaluation of the associated inflammatory response. Eur. Respir. J. 2007, 30, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- American Association for Respiratory Care. Endotracheal suctioning of mechanically ventilated patients with artificial airways. Respir. Care 2010, 55, 758–764. [Google Scholar]
- Fernandez-Barat, L.; Ciofu, O.; Kragh, K.N.; Pressler, T.; Johansen, U.; Motos, A.; Torres, A.; Hoiby, N. Phenotypic shift in Pseudomonas aeruginosa populations from cystic fibrosis lungs after 2-week antipseudomonal treatment. J. Cyst. Fibros. 2017, 16, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Ciofu, O.; Fussing, V.; Bagge, N.; Koch, C.; Hoiby, N. Characterization of paired mucoid/non-mucoid Pseudomonas aeruginosa isolates from Danish cystic fibrosis patients: Antibiotic resistance, beta-lactamase activity and RiboPrinting. J. Antimicrob. Chemother. 2001, 48, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Hola, V.; Ruzicka, F.; Horka, M. Microbial diversity in biofilm infections of the urinary tract with the use of sonication techniques. FEMS Immunol. Med. Microbiol. 2010, 59, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Stickler, D.J. Bacterial biofilms in patients with indwelling urinary catheters. Nat. Clin. Pract. Urol. 2008, 5, 598–608. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Barat, L.; Ferrer, M.; Sierra, J.M.; Soy, D.; Guerrero, L.; Vila, J.; Li, B.G.; Cortadellas, N.; Martinez-Olondris, P.; Rigol, M.; et al. Linezolid limits burden of methicillin-resistant Staphylococcus aureus in biofilm of tracheal tubes. Crit. Care Med. 2012, 40, 2385–2389. [Google Scholar] [CrossRef] [PubMed]
- Marquette, C.H.; Copin, M.C.; Wallet, F.; Neviere, R.; Saulnier, F.; Mathieu, D.; Duroche, A.; Ramon, P.; Tonnel, A.B. Diagnostic tests for pneumonia in ventilated patients: Prospective evaluation of diagnostic accuracy using histology as a diagnostic gold standard. Am. J. Respir. Crit. Care Med. 1995, 151, 1878–1888. [Google Scholar] [CrossRef] [PubMed]
- Jourdain, B.; Joly-Guillou, M.L.; Dombret, M.C.; Calvat, S.; Trouillet, J.L.; Gibert, C.; Chastre, J. Usefulness of quantitative cultures of BAL fluid for diagnosing nosocomial pneumonia in ventilated patients. Chest 1997, 111, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Burillo, A.; Marin, M.; Cercenado, E.; Ruiz-Carrascoso, G.; Perez-Granda, M.J.; Oteo, J.; Bouza, E. Evaluation of the Xpert Carba-R (Cepheid) Assay Using Contrived Bronchial Specimens from Patients with Suspicion of Ventilator-Associated Pneumonia for the Detection of Prevalent Carbapenemases. PLoS ONE 2016, 11, e0168473. [Google Scholar] [CrossRef] [PubMed]
- Souza, L.C.D.; Mota, V.B.R.D.; Carvalho, A.V.D.S.; Correa, R.D.G.C.; Liberio, S.A.; Lopes, F.F. Association between pathogens from tracheal aspirate and oral biofilm of patients on mechanical ventilation. Braz. Oral Res. 2017, 31, e38. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Nunez, M.; Marti, S.; Puig, C.; Perez-Brocal, V.; Millares, L.; Santos, S.; Ardanuy, C.; Moya, A.; Linares, J.; Monso, E. Bronchial microbiome, PA biofilm-forming capacity and exacerbation in severe COPD patients colonized by P. aeruginosa. Future Microbiol. 2017, 12, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratala, J.; et al. Management of Adults With Hospital-Acquired and Ventilator-Associated Pneumonia: Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Pigs (n) | Inoculated Microorganism | Bacterial Instillation | ETA (n) | BAL (n) | Treatment |
|---|---|---|---|---|---|---|
| Study 1 | 15 | P. aeruginosa | Lungs | 39 | 23 | Untreated controls vs. Nebulized aminoglycoside vs. IV carbapenem |
| Study 2 | 4 | MRSA | Oropharynx | 10 | 0 | Untreated controls vs. Monoclonal antibody |
| Study 3 | 7 | P. aeruginosa | Lungs | 16 | 14 | Untreated controls vs. IV cephalosporin |
| Study 4 | 5 | P. aeruginosa | Oropharynx | 14 | 12 | Untreated controls vs. Monoclonal antibody |
| Study 5 | 2 | MRSA | Lungs | 6 | 6 | Untreated controls vs. IV lipoglycopeptide |
| Non-Sonicated ETA (log CFU/mL) | Sonicated ETA (log CFU/mL) | p-Value | ||
|---|---|---|---|---|
| Inoculated microorganism | P. aeruginosa (n = 69) | 4.03 ± 2.58 | 4.25 ± 2.79 | p < 0.001 |
| MRSA (n = 16) | 4.82 ± 2.04 | 5.17 ± 1.52 | 0.159 | |
| Bacterial instillation | Lungs (n = 61) | 4.10 ± 2.50 | 4.35 ± 2.65 | p < 0.001 |
| Oropharynx (n = 24) | 4.37 ± 2.53 | 4.61 ± 2.42 | 0.156 | |
| Time of assessment (hours after bacterial challenge) | 24 h (n = 33) | 5.24 ± 1.65 | 5.45 ± 1.71 | p < 0.001 |
| 48 h (n = 25) | 3.67 ± 2.69 | 3.79 ± 2.82 | 0.019 | |
| 72 h (n = 27) | 3.30 ± 2.84 | 3.62 ± 2.89 | 0.052 |
| ETA cut-off | Se | Sp | PPV | NPV | PLR | NLR | |
|---|---|---|---|---|---|---|---|
| (95%CI) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | ||
| Non-sonicated ETA | ≥5 log CFU/mL | 100 | 46.8 | 24.2 | 100 | 1.88 | Undefined |
| (100–100) | (32.5–61.1) | (9.6–38.9) | (100–100) | (1.44–2.46) | |||
| ≥6 log CFU/mL | 75.0 | 83.0 | 42.9 | 95.1 | 4.41 | 0.30 | |
| (65.6–100) | (72.2–93.7) | (16.9–68.8) | (88.5–100) | (2.09–9.3) | (0.09–1.01) | ||
| Sonicated ETA | ≥5 log CFU/mL | 100 | 40.4 | 22.2 | 100 | 1.68 | Undefined |
| (100–100) | (26.4–54.5) | (8.6–35.8) | (100–100) | (1.33–2.12) | |||
| ≥6 log CFU/mL | 87.5 | 70.2 | 33.3 | 97.1 | 2.94 | 0.18 | |
| (64.6–100) | (57.1–83.3) | (13.2–53.5) | (91.4–100) | (1.76–4.90) | (0.03–1.12) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Barat, L.; Motos, A.; Ranzani, O.T.; Bassi, G.L.; Aguilera Xiol, E.; Senussi, T.; Travierso, C.; Chiurazzi, C.; Idone, F.; Muñoz, L.; et al. Diagnostic Value of Endotracheal Aspirates Sonication on Ventilator-Associated Pneumonia Microbiologic Diagnosis. Microorganisms 2017, 5, 62. https://doi.org/10.3390/microorganisms5030062
Fernández-Barat L, Motos A, Ranzani OT, Bassi GL, Aguilera Xiol E, Senussi T, Travierso C, Chiurazzi C, Idone F, Muñoz L, et al. Diagnostic Value of Endotracheal Aspirates Sonication on Ventilator-Associated Pneumonia Microbiologic Diagnosis. Microorganisms. 2017; 5(3):62. https://doi.org/10.3390/microorganisms5030062
Chicago/Turabian StyleFernández-Barat, Laia, Ana Motos, Otavio T. Ranzani, Gianluigi Li Bassi, Elisabet Aguilera Xiol, Tarek Senussi, Chiara Travierso, Chiara Chiurazzi, Francesco Idone, Laura Muñoz, and et al. 2017. "Diagnostic Value of Endotracheal Aspirates Sonication on Ventilator-Associated Pneumonia Microbiologic Diagnosis" Microorganisms 5, no. 3: 62. https://doi.org/10.3390/microorganisms5030062
APA StyleFernández-Barat, L., Motos, A., Ranzani, O. T., Bassi, G. L., Aguilera Xiol, E., Senussi, T., Travierso, C., Chiurazzi, C., Idone, F., Muñoz, L., Vila, J., Ferrer, M., Pelosi, P., Blasi, F., Antonelli, M., & Torres, A. (2017). Diagnostic Value of Endotracheal Aspirates Sonication on Ventilator-Associated Pneumonia Microbiologic Diagnosis. Microorganisms, 5(3), 62. https://doi.org/10.3390/microorganisms5030062