Clinical, Epidemiological, and Geospatial Characteristics of Patients Infected with Hepatitis C Virus Treated with Second-Generation Direct-Action Antivirals in a Reference Center in a Mesoregion of São Paulo State, Brazil

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Inclusion/Exclusion Criteria
2.3. Data Collection and Baseline Laboratory Parameters
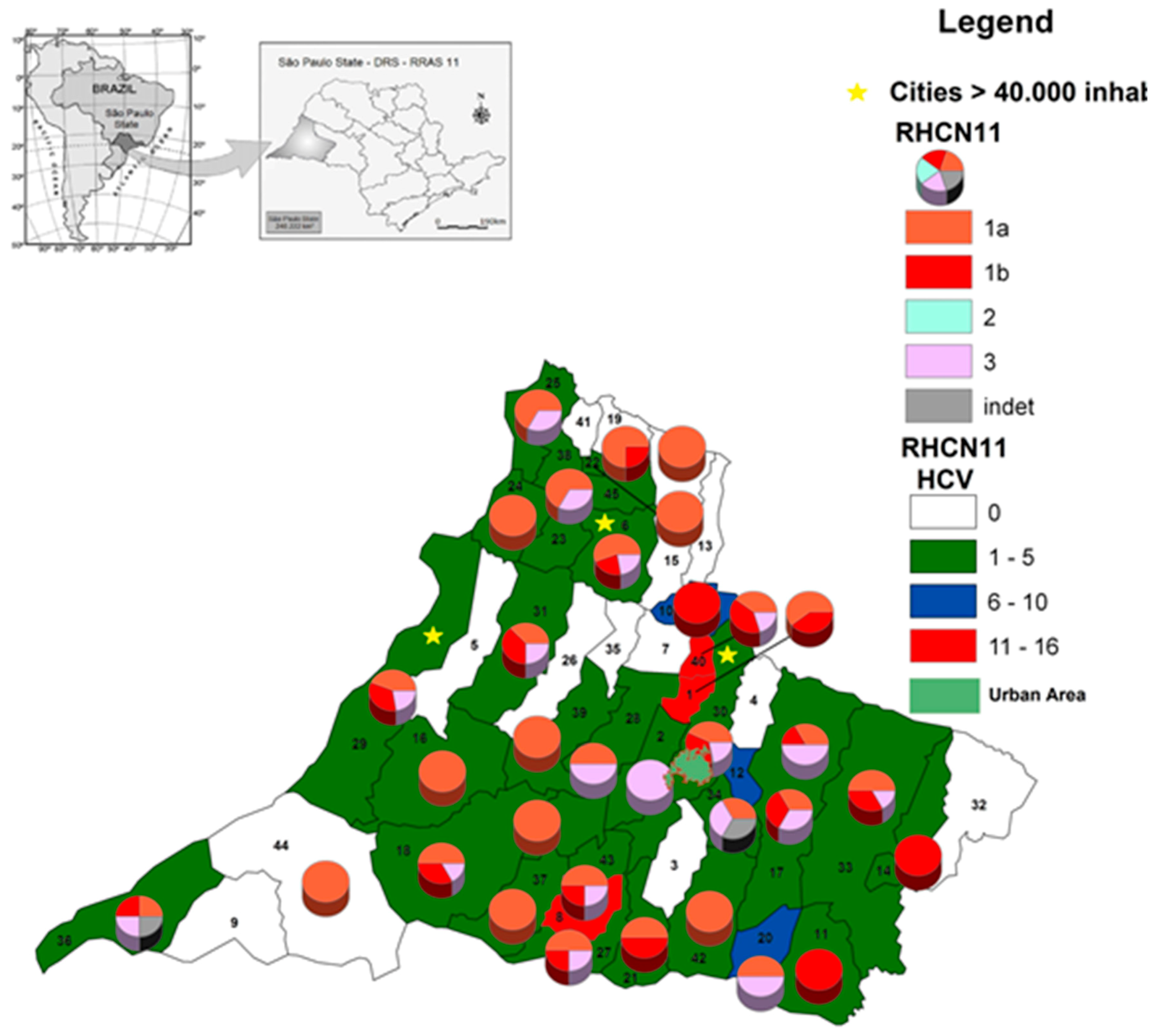
2.4. Geospatial Analysis and Construction of Maps
2.5. Statistical Analysis
2.6. Ethical Statement
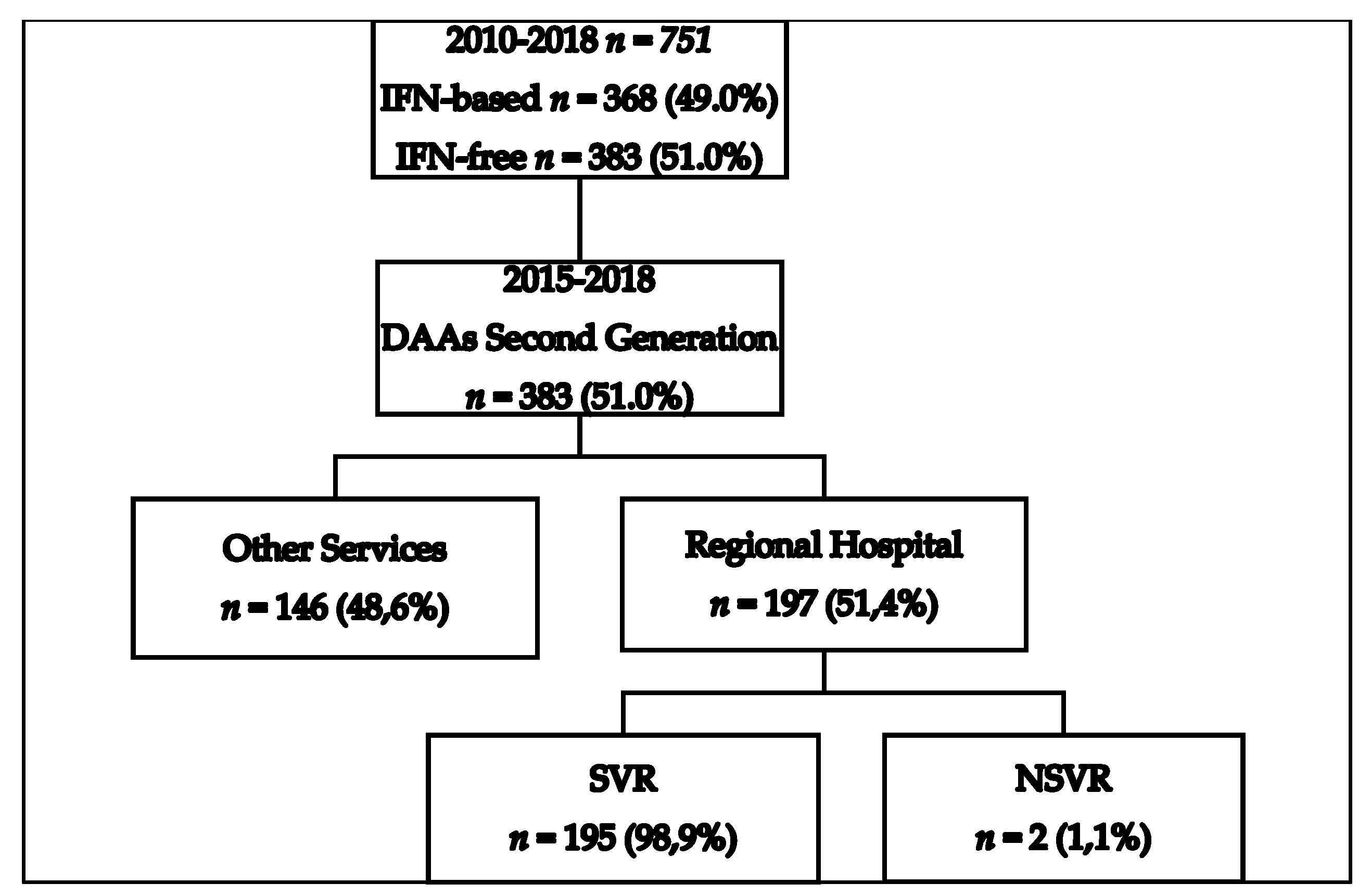
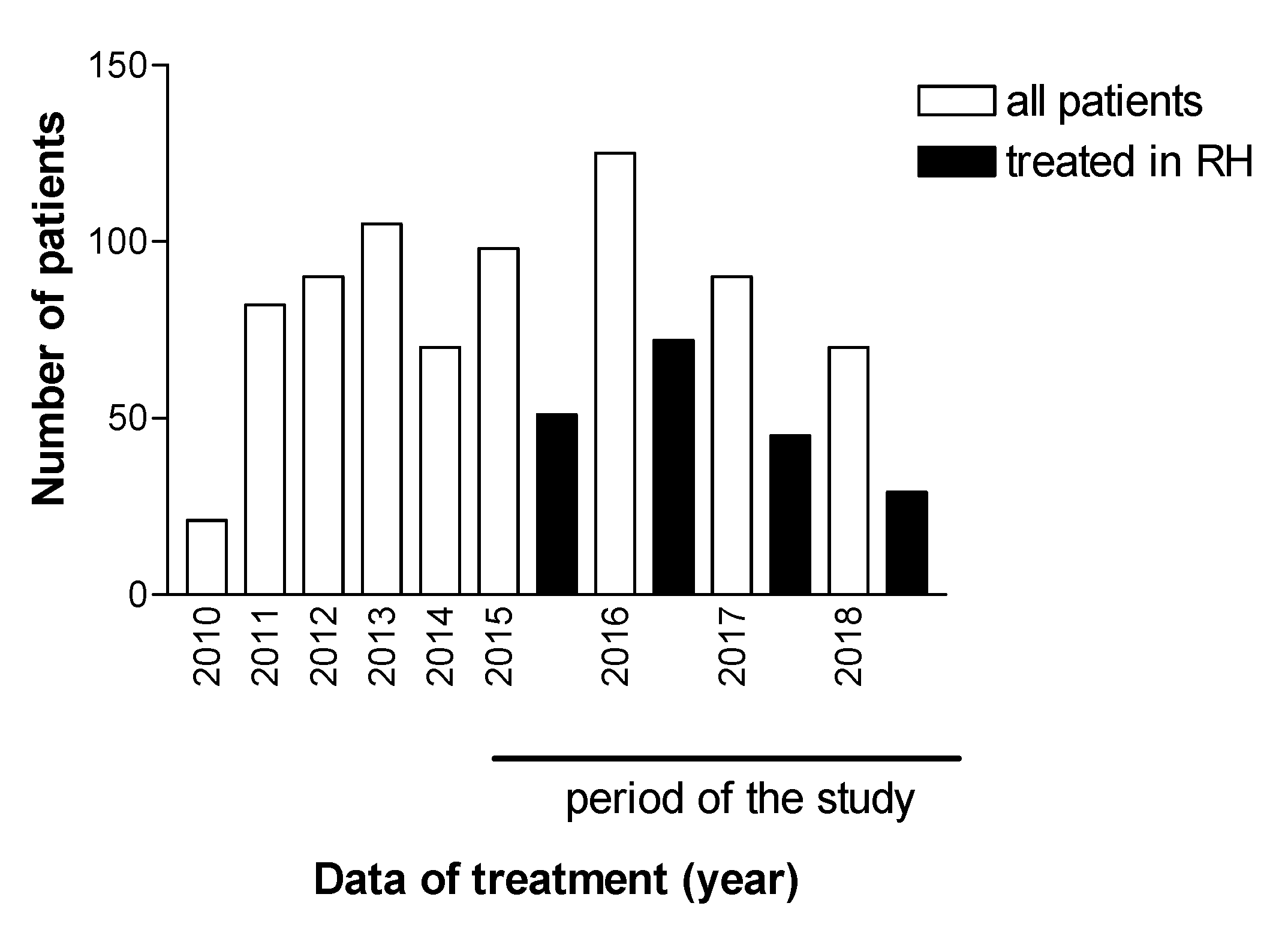
3. Results
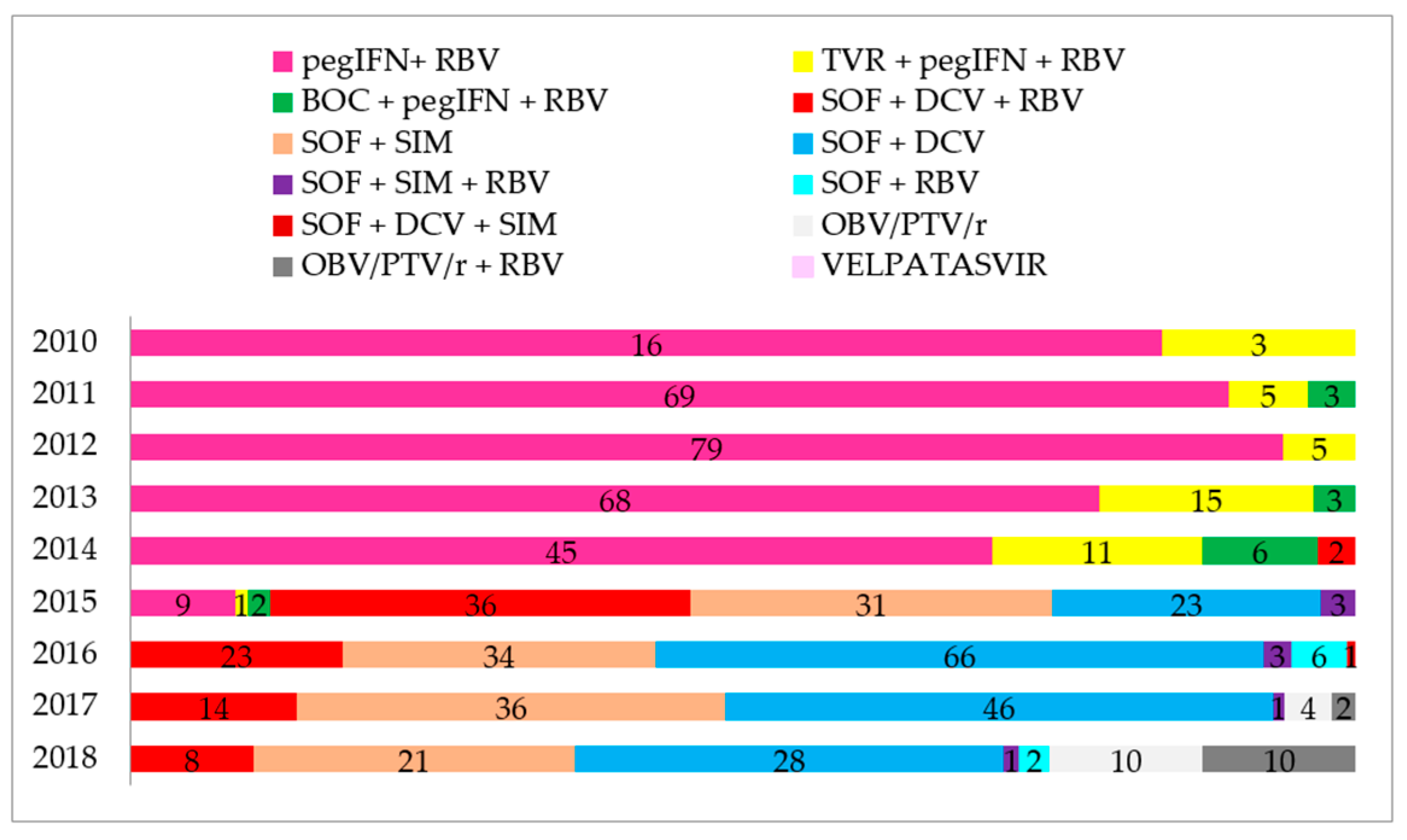
3.1. Therapeutic Regimens, Baseline Clinical, and Demographic Characteristics
3.2. Laboratory Findings
3.3. Comorbidities Associated with Chronic HCV Infection
3.4. Geographic Distribution of Genotypes and Cumulative Incidence of HCV in the RHAN11 Mesoregion
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis. Available online: https://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en/ (accessed on 19 August 2020).
- Benzaken, A.; Catapan, E.; Girade, R.; Razavi, R.; Schmelzer, J.; Pessoa, M.; Ferraz, M.L.; Ferreira, P.; Martinelli, A.; Correa, M.C.M. Hepatitis C elimination by 2030 is feasible in Brazil: A mathematical modelling approach. J. Hepatol. 2018. [Google Scholar] [CrossRef]
- Parise, E.R. 25 years of Hepatitis C. Arq. Gastroenterol. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiffman, M.L. Use of high dose interferon in the treatment of chronic hepatitis C. Semin. Liver Dis. 1999, 19 (Suppl. 1), 25–33. [Google Scholar]
- AASLD/IDSA HCV Guidance Panel. Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology 2015. [Google Scholar] [CrossRef] [Green Version]
- BRAZIL Ministry of Health. Clinical Protocol and Therapeutics Guidelines for Hepatitis C and Co-Infections. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_clinico_diretrizes_hepatite_co_coinfeccoes.pdf (accessed on 25 July 2019).
- Brazil Ministry of Health. Plan for the Elimination of Hepatitis C in Brazil. Available online: http://www.aids.gov.br/system/tdf/pub/2016/66284/plano_para_eliminacao_hepatite_c_no_brasil_170119.pdf?file=1&type=node&id=66284&force=1 (accessed on 19 August 2020).
- WHO. Hepatitis C. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 18 July 2019).
- Cooper, C.L.; Galanakis, C.; Donelle, J.; Kwong, J.; Boyd, R.; Boucher, L.; Kendall, C.E. HCV-infected individuals have higher prevalence of comorbidity and multimorbidity: A retrospective cohort study. BMC Infect. Dis. 2019. [Google Scholar] [CrossRef] [Green Version]
- Laskus, T.; Radkowski, M.; Adair, D.M.; Wilkinson, J.; Scheck, A.C.; Rakela, J. Emerging evidence of hepatitis C virus neuroinvasion. AIDS 2005. [Google Scholar] [CrossRef]
- Cacoub, P.; Comarmond, C.; Domont, F.; Savey, L.; Desbois, A.C.; Saadoun, D. Extrahepatic manifestations of chronic hepatitis C virus infection. Ther. Adv. Infect. Dis. 2016. [Google Scholar] [CrossRef]
- Prestes-Carneiro, L.E.; Daniel, L.A.F.; Almeida, L.C.; D’Andrea, L.Z.; Vieira, A.G.; Anjolete, I.R.; André, L.; Flores, E.F. Spatiotemporal analysis and environmental risk factors of visceral leishmaniasis in an urban setting in São Paulo State, Brazil. Parasit. Vectors 2019. [Google Scholar] [CrossRef] [Green Version]
- Pereira, D.H.P.; Primo, L.S.; Pelizari, G.; Flores, F.; Moraes-Vasconcelos, D.; Condino-Neto, A.; Prestes-Carneiro, L.E. Primary immunodeficiencies in a mesoregion of São Paulo, Brazil: Epidemiologic, clinical, and geospatial approach. Front. Immunol. 2020. [Google Scholar] [CrossRef]
- Prestes-Carneiro, L.E.; Vieira, J.T.M.; Isaac, L.B.; Portelinha-Filho, A.M. Clinical, demographic, and epidemiologic characteristics of hepatitis B virus-infected patients at a tertiary public hospital in Presidente Prudente, State of São Paulo. Rev. Soc. Bras. Med. Trop. 2016. [Google Scholar] [CrossRef] [Green Version]
- Portelinha-Filho, A.M.; Nascimento, C.U.; Tannouri, T.N.; Troiani, C.; Ascêncio, E.L.; Bonfim, R.; D’Andrea, L.A.Z.; Prestes-Carneiro, L.E. Seroprevalence of HBV, HCV and HIV co-infection in selected individuals from state of São Paulo, Brazil. Mem. Inst. Oswaldo Cruz 2009. [Google Scholar] [CrossRef] [PubMed]
- Nutini, M.F.R.; Hunter, J.; Giron, L.; Pires, A.F.N.P.C.; Kohiyama, I.M.; Camargo, M.; Sucupira, M.C.A.; Benzaken, A.S.; Ferreira, P.A.; Truong, H.M.; et al. HCV genotype profile in Brazil of mono-infected and HIV co-infected individuals: A survey representative of an entire country. PLoS ONE 2020. [Google Scholar] [CrossRef] [PubMed]
- Petruzziello, A.; Marigliano, S.; Loquercio, G.; Cacciapuoti, C. Hepatitis C virus (HCV) genotypes distribution: An epidemiological up-date in Europe. Infect. Agent Cancer 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botheju, W.S.P.; Zghyer, F.; Mahmud, S.; Terlikbayeva, A.; El-Bassel, N.; Abu-Raddad, L.J. The epidemiology of hepatitis C virus in Central Asia: Systematic review, meta-analyses, and meta-regression analyses. Sci. Rep. 2019. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Pogorzelska, J.; Flisiak-Jackiewicz, M. Hepatitis C: Efficacy and safety in real life. Liver Int. 2017. [Google Scholar] [CrossRef] [Green Version]
- Lobato, C.M.O.; Codes, L.; Silva, G.F.; Souza, A.F.M.; Coelho, H.S.M.; Pedroso, M.L.A.; Parise, E.R.; Lima, L.M.S.T.B.; Borba, L.A.; Evangelista, A.S.; et al. Direct antiviral therapy for treatment of hepatitis C: A real-world study from Brazil. Ann. Hepatol. 2019. [Google Scholar] [CrossRef]
- Sette, H., Jr.; Cheinquer, H.; Wolff, F.H.; Araujo, A.; Coelho-Borges, S.; Soares, S.R.P.; Barros, M.F.A. Treatment of chronic HCV infection with the new direct acting antivirals (DAA): First report of a real world experience in Southern Brazil. Ann. Hepatol. 2017. [Google Scholar] [CrossRef]
- Calleja, J.L.; Crespo, J.; Rincón, D.; Ruiz-Antorán, B.; Fernandez, I.; Perelló, C.; Gea, F.; Lens, S.; Garcia-Samaniego, J.; Sacristán, B.; et al. Effectiveness, safety and clinical outcomes of direct-acting antiviral therapy in HCV genotype 1 infection: Results from a Spanish real-world cohort. J. Hepatol. 2017. [Google Scholar] [CrossRef]
- Hajarizadeh, B.; Lamoury, F.M.; Feld, J.J.; Amin, J.; Keoshkerian, E.; Matthews, G.V.; Hellard, M.; Dore, G.J.; Lloyd, A.R.; Grebely, J.; et al. Alanine aminotransferase, HCV RNA levels and pro-inflammatory and pro-fibrogenic cytokines/chemokines during acute hepatitis C virus infection. Virol. J. 2016. [Google Scholar] [CrossRef] [Green Version]
- Roshan, B.; Guzman, G. Histological and clinical characteristics of patients with chronic hepatitis C and persistently normal alanine aminotransferase levels. Hepat. Res. Treat. 2014. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.T.; Qiu, M.J.; Yang, S.L.; Fang, X.; He, X.X.; Wang, M.M.; Li, Y.N.; Xiong, Z.F.; Huang, S. Alpha-fetoprotein regulates the expression of immune-related proteins through the NF-κB (P65) pathway in hepatocellular carcinoma cells. J. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ozgor, D.; Otan, E. HCC and tumor biomarkers: Does one size fits all? J. Gastrointest. Cancer 2020. [Google Scholar] [CrossRef] [PubMed]
- Manuc, D.; Preda, C.M.; Sandra, I.; Baicus, C.; Cerban, R.; Constantinescu, I.; Olteanu, A.O.; Ciora, C.A.; Manuc, T.; Chiriac, D.E.; et al. Signification of Serum Alpha-Fetoprotein Levels in Cases of Compensated Cirrhosis and Hepatitis C Virus without Hepatocellular Carcinoma. J. Med. Life 2020. [Google Scholar] [CrossRef]
- Elalfy, H.; Elsherbiny, W.; Abdel-Rahman, A.; Elhammady, D.; Shaltout, S.W.; Elsamanoudy, A.Z.; El-Deek, B. Diagnostic non-invasive model of large risky esophageal varices in cirrhotic hepatitis C virus patients. World J. Hepatol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Park, H.; Henry, L.; Adeyemi, A.; Stepanova, M. Extrahepatic Manifestations of Hepatitis C: A meta-analysis of prevalence, quality of life, and economic burden. Gastroenterology 2016. [Google Scholar] [CrossRef] [PubMed]
- Batista-Neves, S.C.; Quarantini, L.C.; Almeida, A.G.; Bressan, R.A.; Lacerda, A.L.; de-Oliveira, I.R.; Paraná, R.; Miranda-Scippa, A. High frequency of unrecognized mental disorders in HCV-infected patients. Gen. Hosp. Psychiatry. 2008. [Google Scholar] [CrossRef]
- Adinolfi, L.E.; Nevola, R.; Lus, G.; Restivo, L.; Guerrera, B.; Romano, C.; Zampino, R.; Rinaldi, L.; Sellitto, A.; Giordano, M.; et al. Chronic hepatitis C virus infection and neurological and psychiatric disorders: An overview. World J. Gastroenterol. 2015. [Google Scholar] [CrossRef]
- Yarlott, L.; Heald, E.; Forton, D. Hepatitis C virus infection and neurological and psychiatric disorders. J. Adv. Res. 2017. [Google Scholar] [CrossRef] [Green Version]
- Hanus, J.S.; Ceretta, L.B.; Simões, P.W.; Tuon, L. Incidence of hepatitis C in Brazil. Rev. Soc. Bras. Med. Trop. 2015. [Google Scholar] [CrossRef] [Green Version]
- Payne, E.; Totten, S.; Archibald, C. Hepatitis C surveillance in Canada. Can. Commun. Dis. Rep. 2014. [Google Scholar] [CrossRef]
- Han, R.; Zhou, J.; François, C.; Toumi, M. Prevalence of hepatitis C infection among the general population and high-risk groups in the EU/EEA: A systematic review update. BMC Infect. Dis. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prestes-Carneiro, L.E.; Spir, P.R.N.; Fontanesi, M.; Garcia, K.G.P.; Silva, F.A.; Flores, E.F.; Vasconcelos, D.M. Unusual manifestations of visceral leishmaniasis in children: A case series and its spatial dispersion in the western region of São Paulo state, Brazil. BMC Infect. Dis. 2019. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number (%) |
|---|---|
| Genotype | |
| 1a | 93 (47.2) |
| 1b | 56 (28.5) |
| 2 | 2 (1.0) |
| 3 | 44 (22.3) |
| Indeterminate | 2 (1.0) |
| Therapeutic regimen | |
| SOF/DCV | 71 (36.0) |
| SOF/DCV/RBV | 40 (20.3) |
| SOF/RBV | 3 (1.5) |
| SOF/SIM | 78 (39.6) |
| SOF/SIM/RBV | 5 (2.5) |
| Treatment duration | |
| 12 weeks | 153 (77.7) |
| 24 weeks | 44 (22.3) |
| Liver fibrosis | |
| F0 | 5 (2.5) |
| F1 | 40 (20.3) |
| F2 | 31 (15.7) |
| F3 | 21 (10.6) |
| F4 | 47 (23.9) |
| Unknown | 53 (26.9) |
| Previous treatment | |
| Previous failed treatments | 65 (33) |
| Naive | 132 (67) |
| Viral response | |
| SVR | 195 (98.9) |
| NSVR | 2 (1.0) |
| Average viral load (IU/mL) | 1,218,994 |
| Parameters | Number | Mean ± SD | 95% CI | Normal Range |
|---|---|---|---|---|
| Hemoglobin (g/dL), women | 80 | 13.26 ± 1.75 | 12.87–13.65 | 12.0–15.5 |
| Hemoglobin (g/dL), men | 113 | 14.64 ± 0.33 | 13.98–15.31 | 13.5–17.5 |
| Hematocrit (%) women | 80 | 40.04 ± 0.51 | 39.00–41.07 | 36–48 |
| Hematocrit (%) men | 113 | 42.26 ± 0.54 | 41.18–43.35 | 41–50 |
| Platelets < 150 (mm3) | 192 | 157.60 ± 76.21 | 146.80–168.50 | 150–400 |
| TAP (seconds) | 171 | 12.23 ± 4.95 | 11.48–12.98 | 10–14 |
| INR | 174 | 1.15 ± 0.76 | 1.03–1.26 | 0.8–1.0 |
| Albumin (mg/dL) | 177 | 4.121 ± 2.45 | 3.75–4.48 | 3.4–5.4 |
| Globulins (mg/dL) | 126 | 3.60 ± 0.61 | 3.49–3.71 | 2.3–3.5 |
| Total bilirubin (mg/dL) | 189 | 0.97 ± 0.86 | 0.85–1.10 | 0.1–1.2 |
| ALT (IU/dL) | 194 | 91.73 ± 67.04 | 82.24–101.2 | 7–56 |
| AST (IU/dL) | 194 | 78.47 ± 55.22 | 70.65–86.29 | 10–40 |
| Alkaline phosphatase (IU/L) | 108 | 107.60 ± 62.62 | 95.68–119.6 | 44–147 |
| γ-GT (IU/L) | 159 | 130.2 ± 136.3 | 108.8–151.8 | 85 |
| α-Fetoproteín (ng/mL) | 167 | 12.78 ± 28.48 | 8.42–17.13 | <10 |
| Urea (mg/dL) | 157 | 29.09 ± 15.64 | 26.62–31.56 | 16–40 |
| Creatinine (mg/dL) | 190 | 0.85 ± 0.60 | 0.76–0.93 | 0.6–1.2 |
| Comorbidities | Number (n = 197) | % |
|---|---|---|
| Coronary artery disorders | 76 | 38.6 |
| Gastrointestinal | 74 | 37.5 |
| Hormonal and metabolic disorders | 40 | 20.3 |
| Psychiatric disorders | 39 | 19.8 |
| Ophthalmic disorders | 32 | 16.2 |
| Thyroid disorders | 19 | 9.7 |
| Kidney disorders | 13 | 6.6 |
| Neurologic disorders | 8 | 4.0 |
| Hematologic disorders | 8 | 4.0 |
| Autoimmune disorders | 8 | 4.0 |
| Tumors disorders | 6 | 3.0 |
| Lung disorders | 2 | 1.0 |
| Skin allergy | 2 | 1.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pena, D.Z.; Anadão, M.F.; Flores, E.F.; Okada, M.N.; Filho, A.M.P.; Ferro, R.S.; Prestes-Carneiro, L.E. Clinical, Epidemiological, and Geospatial Characteristics of Patients Infected with Hepatitis C Virus Treated with Second-Generation Direct-Action Antivirals in a Reference Center in a Mesoregion of São Paulo State, Brazil. Microorganisms 2020, 8, 1575. https://doi.org/10.3390/microorganisms8101575
Pena DZ, Anadão MF, Flores EF, Okada MN, Filho AMP, Ferro RS, Prestes-Carneiro LE. Clinical, Epidemiological, and Geospatial Characteristics of Patients Infected with Hepatitis C Virus Treated with Second-Generation Direct-Action Antivirals in a Reference Center in a Mesoregion of São Paulo State, Brazil. Microorganisms. 2020; 8(10):1575. https://doi.org/10.3390/microorganisms8101575
Chicago/Turabian StylePena, Danilo Zangirolami, Murilo Fernandes Anadão, Edilson Ferreira Flores, Mayara Namimatsu Okada, Alexandre Martins Portelinha Filho, Rodrigo Sala Ferro, and Luiz Euribel Prestes-Carneiro. 2020. "Clinical, Epidemiological, and Geospatial Characteristics of Patients Infected with Hepatitis C Virus Treated with Second-Generation Direct-Action Antivirals in a Reference Center in a Mesoregion of São Paulo State, Brazil" Microorganisms 8, no. 10: 1575. https://doi.org/10.3390/microorganisms8101575
APA StylePena, D. Z., Anadão, M. F., Flores, E. F., Okada, M. N., Filho, A. M. P., Ferro, R. S., & Prestes-Carneiro, L. E. (2020). Clinical, Epidemiological, and Geospatial Characteristics of Patients Infected with Hepatitis C Virus Treated with Second-Generation Direct-Action Antivirals in a Reference Center in a Mesoregion of São Paulo State, Brazil. Microorganisms, 8(10), 1575. https://doi.org/10.3390/microorganisms8101575