
Comprehensive Contact Tracing, Testing and Sequencing Show Limited Transmission of SARS-CoV-2 between Children in Schools in Norway, August 2020 to May 2021

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Demographic and Exposure Data
2.3. Laboratory Data
2.4. Epidemiological Data
2.5. Mitigation Measures in Schools
| Stay at home policy for all if symptomatic Enforced classroom hygiene Defined child cohorts, limited mixing of cohorts Limit shared spaces for children indoors Limit shared spaces for children outdoors Reduce the number of staff involved in each cohort Reduce physical contact between staff Work-from-home policy for staff whenever possible |
2.6. Analyses
3. Results
3.1. Infection Rates
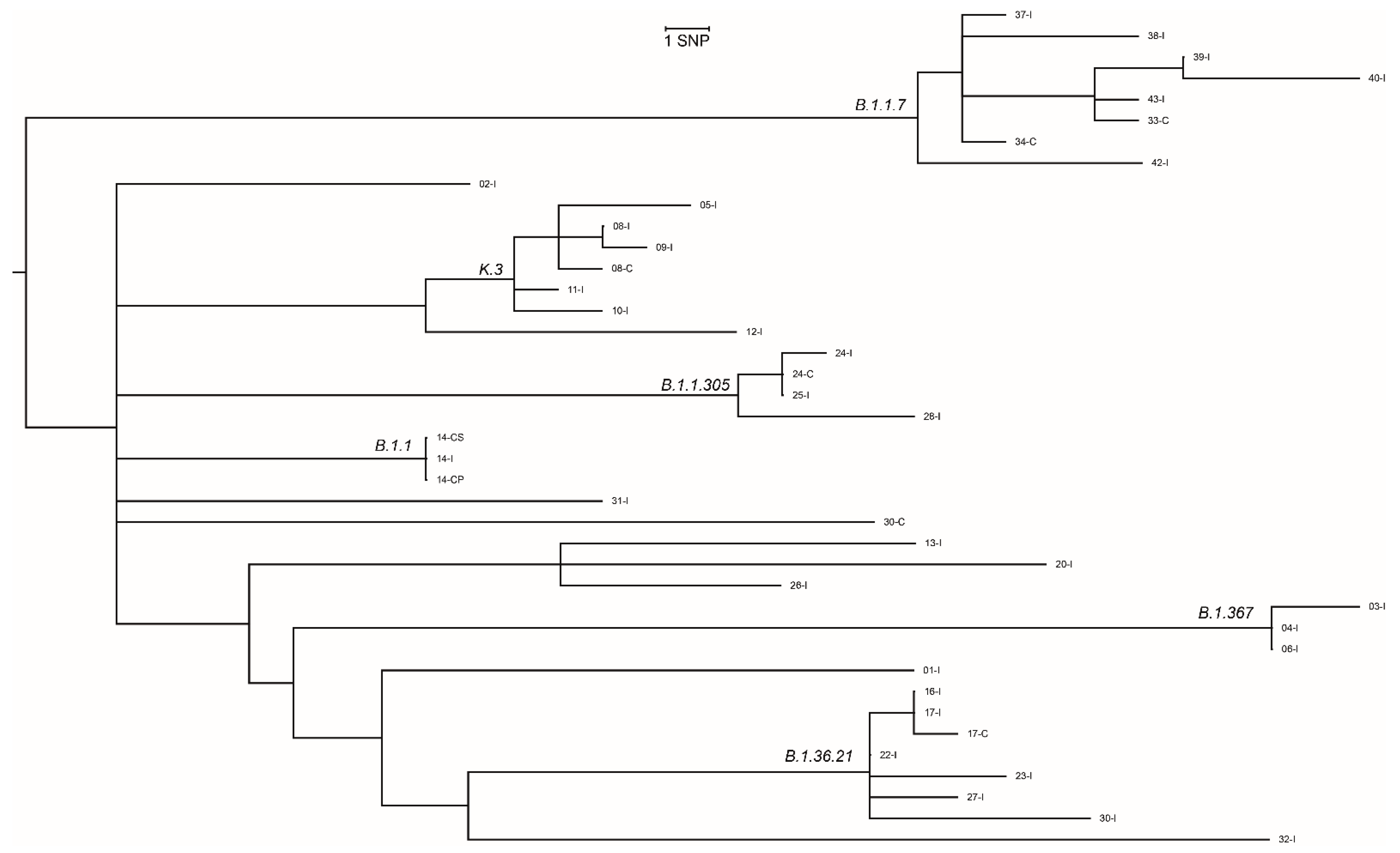
3.2. Characteristics of the Virus
3.3. Possible Transmission
3.4. Study Data Compared with Surveillance Data
3.5. Mitigation Measures in School
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Source | Level |
|---|---|
| Home-sampled saliva test, study start * | All participants |
| Home-sampled saliva test, study end * | All participants |
| Questionnaire 1—Demography and previous exposure | All participants |
| Questionnaire 2—Symptom diary | All participants |
| Questionnaire 3—Outcome and exposure | Contacts negative for SARS-CoV-2 in the first saliva sample |
| WGS data-cases * | Cases and contacts with confirmed SARS-CoV-2 |
| Linkage with MSIS laboratory database | All participants |
| Infection prevention and control measures | Participating Schools |
| Outcome of contact investigation, municipalities | Population, aggregated |
| Epidemiological data | Population, aggregated |
| ID I | Quarter/Year | Grade | County | IR (/100,000) $ | IPC II-Level | Child Contacts | Adult Contacts | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| County | Local | National # | Scores (Local) § | Total n | Included n (%) | Total n | Included n | ||||
| 1st to 4th grade | |||||||||||
| 1 * | Q3-2020 | 1–4 | Viken | 34 | 17 | 7 | 30 | 15 (50) | 12 | 3 | |
| 2 * | Q3-2020 | 1–4 | Viken | 29 | 26 | 7 | 45 | 33 (73) | 9 | 4 | |
| 3 * | Q3-2020 | 1–4 | Viken | 29 | 26 | 4 | 18 | 16 (89) | 3 | 2 | |
| 4 * | Q4-2020 | 1–4 | Viken | 31 | 39 | 5 | 22 | 19 (86) | 9 | 7 | |
| 5 * | Q4-2020 | 1–4 | Viken | 31 | 51 | 7 | 22 | 17 (77) | 5 | 5 | |
| 6 * | Q4-2020 | 1–4 | Viken | 31 | 51 | 7 | 19 | 4 (21) | 5 | 2 | |
| 7 * | Q4-2020 | 1–4 | Oslo | 99 | 55 | 6 | 22 | 18 (82) | 7 | 7 | |
| 8 * | Q4-2020 | 1–4 | Oslo | 181 | 150 | 5 | 24 | 18 (71) | 4 | 3 | |
| 9 | Q4-2020 | 1–4 | Oslo | 336 | 251 | 6 | 21 | 14 (67) | 1 | 1 | |
| 10 | Q2-2021 | 1–4 | Oslo | 441 | 763 | - | 13 | 4 (31) | 1 | 1 | |
| 11 | Q2-2021 | 1–4 | Oslo | 471 | 433 | 7 | 37 | 20 (54) | 3 | 4 | |
| 12 | Q2-2021 | 1–4 | Oslo | 284 | 267 | 8 | 18 | 13 (72) | 1 | 0 | |
| 13 | Q2-2021 | 1–4 | Viken | 141 | 204 | 7 | 9 | 4 (44) | 1 | 1 | |
| 14 | Q2-2021 | 1–4 | Viken | 118 | 337 | 7 | 10 | 6 (60) | 4 | 1 | |
| 15 | Q2-2021 | 1–4 | Viken | 109 | 152 | 8 | 19 | 13(14) | 3 | 3 | |
| 5th to 7th grade | |||||||||||
| 16 * | Q3-2020 | 5–7 | Oslo | 53 | 65 | 7 | 20 | 17 (85) | 3 | 2 | |
| 17 * | Q4-2020 | 5–7 | Oslo | 99 | 55 | 6 | 25 | 20 (80) | 3 | 2 | |
| 18 * | Q4-2020 | 5–7 | Oslo | 95 | 96 | 6 | 24 | 17 (71) | 6 | 2 | |
| 19 * | Q4-2020 | 5–7 | Oslo | 111 | 111 | 6 | 25 | 8 (28) | 3 | 3 | |
| 20 * | Q4-2020 | 5–7 | Oslo | 181 | 276 | 6 | 21 | 15 (71) | 4 | 3 | |
| 21 | Q4-2020 | 5–7 | Oslo | 254 | 354 | 5 | 16 | 10 (63) | 1 | 0 | |
| 22 | Q4-2020 | 5–7 | Viken | 209 | 522 | 7 | 15 | 9 (60) | 1 | 1 | |
| 23 | Q4-2020 | 5–7 | Viken | 194 | 179 | - | 17 | 14 (82) | 2 | 1 | |
| 24 | Q4-2020 | 5–7 | Viken | 182 | 158 | 7 | 18 | 10 (56) | 0 | 0 | |
| 25 | Q1-2021 | 5–7 | Viken | 144 | 201 | 7 | 41 | 31 (76) | 2 | 1 | |
| 26 | Q1-2021 | 5–7 | Viken | 144 | 171 | 7 | 20 | 15 (70) | 5 | 2 | |
| 27 | Q2-2021 | 5–7 | Oslo | 363 | 211 | 8 | 10 | 4 (40) | 1 | 0 | |
| 28 | Q2-2021 | 5–7 | Oslo | 284 | 419 | - | 14 | 6 (43) | 3 | 1 | |
| 29 | Q2-2021 | 5–7 | Oslo | 212 | 179 | 7 | 24 | 12 (50) | 4 | 2 | |
| 8th to10th grade | |||||||||||
| 30 | Q4-2020 | 8–10 | Oslo | 181 | 150 | 5 | 21 | 16 (76) | 3 | 2 | |
| 31 | Q4-2020 | 8–10 | Oslo | 254 | 354 | 7 | 22 | 3 (14) | 1 | 0 | |
| 31 | Q4-2020 | 8–10 | Oslo | 254 | 429 | 6 | 23 | 12 (52) | 4 | 1 | |
| 33 | Q4-2020 | 8–10 | Oslo | 336 | 438 | 5 | 25 | 14 (56) | 8 | 6 | |
| 34 | Q4-2020 | 8–10 | Oslo | 336 | 415 | 5 | 28 | 19 (68) | 4 | 1 | |
| 35 | Q4-2020 | 8–10 | Oslo | 336 | 415 | 6 | 19 | 4 (16) | 5 | 3 | |
| 36 | Q4-2020 | 8–10 | Oslo | 294 | 239 | 8 | 13 | 5 (38) | 4 | 1 | |
| 37 | Q4-2020 | 8–10 | Viken | 194 | 179 | - | 18 | 10 (56) | 3 | 1 | |
| 38 | Q4-2020 | 8–10 | Oslo | 223 | 365 | 8 | 23 | 17 (74) | 2 | 2 | |
| 39 | Q1-2021 | 8–10 | Viken | 202 | 268 | 7 | 14 | 6 (50) | 1 | 2 | |
| 40 | Q1-2021 | 8–10 | Viken | 190 | 159 | 8 | 10 | 6 (60) | 5 | 1 | |
| 41 | Q1-2021 | 8–10 | Viken | 190 | 269 | 6 | 20 | 9 (45) | 1 | 1 | |
| 42 | Q1-2021 | 8–10 | Viken | 195 | 335 | 7 | 62 | 32 (52) | 6 | 3 | |
| 43 | Q1-2021 | 8–10 | Oslo | 471 | 637 | 7 | 18 | 4 (22) | 3 | 3 | |
| ID | Quarter | Grade | National Guideline/Traffic Light Model | Sum of Scores | National Guidelines | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | H | ||||||
| 1 | Q3-2020 | 1–4 | 7 | ||||||||||
| 2 | 5–7 | 7 | |||||||||||
| 3 | 1–4 | 7 | |||||||||||
| 4 | 1–4 | 4 | |||||||||||
| 5 | Q4-2020 | 1–4 | 5 | ||||||||||
| 6 | 1–4 | 7 | |||||||||||
| 7 | 1–4 | 7 | |||||||||||
| 8 | 1–4 | 6 | |||||||||||
| 9 | 5–7 | 6 | |||||||||||
| 10 | 5–7 | 6 | |||||||||||
| 11 | 5–7 | 6 | |||||||||||
| 12 | 1–4 | 5 | |||||||||||
| 13 | 8–10 | 5 | |||||||||||
| 14 | 5–7 | 6 | |||||||||||
| 15 | 5–7 | 5 | |||||||||||
| 16 | 8–10 | 7 | |||||||||||
| 17 | 8–10 | 6 | |||||||||||
| 18 | 8–10 | 5 | |||||||||||
| 19 | 1–4 | 6 | |||||||||||
| 20 | 8–10 | 5 | |||||||||||
| 21 | 8–10 | 6 | |||||||||||
| 22 | 5–7 | 7 | |||||||||||
| 23 | 8–10 | 8 | |||||||||||
| 24 | 5–7 | - | |||||||||||
| 25 | 8–10 | - | |||||||||||
| 26 | 8–10 | 8 | |||||||||||
| 27 | 5–7 | 7 | |||||||||||
| 28 | Q1-2021 | 8–10 | 7 | ||||||||||
| 29 | 8–10 | 8 | |||||||||||
| 30 | 8–10 | 6 | |||||||||||
| 31 | 5–7 | 7 | |||||||||||
| 32 | 5–7 | 7 | |||||||||||
| 33 | 8–10 | 7 | |||||||||||
| 34 | 8–10 | 7 | |||||||||||
| 35 | Q2-2021 | 1–4 | - | ||||||||||
| 36 | 1–4 | 7 | |||||||||||
| 37 | 5–7 | 8 | |||||||||||
| 38 | 1–4 | 8 | |||||||||||
| 39 | 5–7 | - | |||||||||||
| 40 | 1–4 | 7 | |||||||||||
| 41 | 5–7 | 7 | |||||||||||
| 42 | 1–4 | 7 | |||||||||||
| 43 | 1–4 | 8 | |||||||||||
| Yellow level according to traffic light model | A | Stay at home policy for all if symptomatic | |||||||||||
| B | Enforced classroom hygiene | ||||||||||||
| Red level according to traffic light model | C | Defined child cohorts, reduced mixing of cohorts | |||||||||||
| D | Avoid shared spaces for children indoors | ||||||||||||
| IPC consistent with national guideline, score = 1 | E | Avoid shared spaces for children outdoors | |||||||||||
| F | Reduce the number of staff contacts per child | ||||||||||||
| IPC not consistent with national guideline, score = 0 | G | Reduce physical contact between staff | |||||||||||
| H | Promotion of home-office whenever possible | ||||||||||||
References
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 among Children in China. Pediatrics 2020, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Wong, G.W. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Eggo, R.M. Susceptibility to SARS-CoV-2 Infection among Children and Adolescents Compared with Adults: A Systematic Review and Meta-analysis. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.A.; Saliba, V.; Bernal, J.L.; Ramsay, M.E.; Ladhani, S.N. SARS-CoV-2 infection and transmission in educational settings: A prospective, cross-sectional analysis of infection clusters and outbreaks in England. Lancet Infect. Dis. 2021, 21, 344–353. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. COVID-19 in Children and the Role of School Settings in Transmission-Second Update; ECDC: Stockholm, Sweden, 2021.
- Brurberg, K.G. The role of children in the transmission of SARS-CoV-2(COVID-19), 1st update. Nor. Inst. Public Health 2020, 3, D5140. [Google Scholar]
- Brandal, L.T.; Ofitserova, T.S.; Meijerink, H.; Rykkvin, R.; Lund, H.M.; Hungnes, O.; Winje, B.A. Minimal transmission of SARS-CoV-2 from paediatric COVID-19 cases in primary schools, Norway, August to November. Eurosurveillance 2021, 26, 2002011. [Google Scholar] [CrossRef]
- Flasche, S.; Edmunds, W.J. The role of schools and school-aged children in SARS-CoV-2 transmission. Lancet Infect. Dis. 2021, 21, 298–299. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Wahl, B.; Dudala, S.R.; Gopal, K.; Neelima, S.; Reddy, K.J.; Lewnard, J.A. Epidemiology and transmission dynamics of COVID-19 in two Indian states. Science 2020, 370, 691–697. [Google Scholar] [CrossRef]
- Johansen, T.B.; Astrup, E.; Jore, S.; Nilssen, H.; Dahlberg, B.B.; Klingenberg, C.; Greve-Isdahl, M. Infection prevention guidelines and considerations for paediatric risk groups when reopening primary schools during COVID-19 pandemic, Norway, April 2020. Eurosurveillance 2020, 25, 2000921. [Google Scholar] [CrossRef]
- Al Suwaidi, H.; Senok, A.; Varghese, R.; Deesi, Z.; Khansaheb, H.; Pokasirakath, S.; Alsheikh-Ali, A. Saliva for molecular detection of SARS-CoV-2 in school-age children. Clin. Microbiol. Infect. 2021, 27, 1330–1335. [Google Scholar] [CrossRef]
- Norwegian Institute of Public Health. Genomic Epidemiology of Novel Coronavirus-Norway All Focused Subsampling; Norwegian Institute of Public Health: Oslo, Norway, 2021; Available online: https://nextstrain.org/groups/niph/ncov/norway-all-2021-06-07?c=pango_lineage (accessed on 29 September 2021).
- World Health Organization. Protocol: Real-Time RT-PCR Assays for the Detection of SARS-CoV-2; Institut Pasteur: Paris, France; Available online: https://www.who.int/docs/default-source/coronaviruse/real-time-rt-pcr-assays-for-the-detection-of-sars-cov-2-institut-pasteur-paris.pdf (accessed on 8 June 2021).
- Lauvrak, V.; Juvet, L.K. Saliva Sample for Testing SARS-CoV-2 Infection, 1st Update Ondiagnostic Accuracy; Norwegian Institute of Public Health: Oslo, Norway, 2020; Available online: https://fhi.brage.unit.no/fhi-xmlui/handle/11250/2722753 (accessed on 13 February 2021).
- Quick, J. nCoV-2019 Sequencing Protocol v3 (LoCost) V.3. Available online: https://www.protocols.io/view/ncov-2019-sequencing-protocol-v3-locost-bh42j (accessed on 8 June 2021).
- Tyson, J.R.; James, P.; Stoddart, D.; Sparks, N.; Wickenhagen, A.; Hall, G.; Quick, J. Improvements to the ARTIC multiplex PCR method for SARS-CoV-2 genome sequencing using nanopore. bioRxiv 2020. [Google Scholar] [CrossRef]
- Rambaut, A.; Holmes, E.C.; O’Toole, Á.; Hill, V.; McCrone, J.T.; Ruis, C.; Pybus, O.G. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat. Microbiol. 2020, 5, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Minh, B.Q.; Schmidt, H.A.; Chernomor, O.; Schrempf, D.; Woodhams, M.D.; Von Haeseler, A.; Lanfear, R. IQ-TREE 2: New Models and Efficient Methods for Phylogenetic Inference in the Genomic Era. Mol. Biol. Evol. 2020, 37, 1530–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- San, J.E.; Ngcapu, S.; Kanzi, A.M.; Tegally, H.; Fonseca, V.; Giandhari, J.; de Oliveira, T. Transmission dynamics of SARS-CoV-2 within-host diversity in two major hospital outbreaks in South Africa. Virus Evol. 2021, 7, veab041. [Google Scholar] [CrossRef]
- Larosa, E.; Djuric, O.; Cassinadri, M.; Cilloni, S.; Bisaccia, E.; Vicentini, M. Secondary transmission of COVID-19 in preschool and school settings in northern Italy after their reopening in September 2020: A population-based study. Eurosurveillance 2020, 25, 2001911. [Google Scholar] [CrossRef] [PubMed]
- Heavey, L.; Casey, G.; Kelly, C.; Kelly, D.; McDarby, G. No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020. Eurosurveillance 2020, 25, 2000903. [Google Scholar] [CrossRef]
- Yung, C.F.; Kam, K.Q.; Nadua, K.D.; Chong, C.Y.; Tan, N.W.H.; Li, J. Novel Coronavirus 2019 Transmission Risk in Educational Settings. Clin. Infect. Dis. 2021, 72, 1055–1058. [Google Scholar] [CrossRef]
- Viner, R.M.; Waddington, C.; Mytton, O.; Booy, R.; Ladhan, S.; Panovska-Griffiths, J.; Bonnel, J.; Melendez-Torres, G.J. Children and Young People in Households and Schools: A Meta-Analysis of Population-Based and Contact-Tracing Studies. Lancet 2021. [Google Scholar]
- Macartney, K.; Quinn, H.E.; Pillsbury, A.J.; Koirala, A.; Deng, L.; Winkler, N. Transmission of SARS-CoV-2 in Australian educational settings: A prospective cohort study. Lancet Child. Adolesc. Health 2020, 4, 807–816. [Google Scholar] [CrossRef]
- Macartney, K. COVID-19 in Schools and Early Childhood Education and Care Services-the Term 4 Experience in NSW; National Centre for Immunisation Research and Surveillance: Sydney, Australia, 2021; Available online: https://www.ncirs.org.au/sites/default/files/2021-03/NCIRS%20NSW%20Schools%20COVID_Summary_Term%204%202020%20Report.pdf (accessed on 13 September 2021).
- Schoeps, A.H.D.; Tamm, C. COVID-19 transmission in educational institutions August to December 2020 Germany: A study of index cases and close contact cohorts. medRxiv 2021. [Google Scholar] [CrossRef]
- Gandini, S.; Rainisio, M.; Iannuzzo, M.L. A cross-sectional and prospective cohort study of the role of schools in the SARS-CoV-2 second wave in Italy. Lancet Reg. Health Eur. 2021, 5, 100092. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. SARS-CoV-2 Variants of Concern and Variants under Investigation in England-Technical Briefing 14. 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/991343/Variants_of_Concern_VOC_Technical_Briefing_14.pdf (accessed on 16 September 2021).
- Southall, E.; Holmes, A.; Hill, E.M.; Atkins, B.D.; Leng, T.; Thompson, R.N. An analysis of school absences in England during the COVID-19 pandemic. BMC Med. 2021, 19, 137. [Google Scholar] [CrossRef] [PubMed]
- Willeit, P.; Krause, R.; Lamprecht, B. Prevalence of RT-qPCR-detected SARS-CoV-2 infection at schools: First results from the Austrian School-SARS-CoV-2 prospective cohort study. Lancet Reg. Health Eur. 2021, 5, 100086. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. SARS-CoV-2 Variants of Concern as of 23 September 2021; ECDC: Stockholm, Sweden, 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 29 September 2021).
- Krishnaratne, S.; Pfadenhauer, L.M.; Coenen, M.; Geffert, K.; Jung-Sievers, C.; Klinger, C. Measures implemented in the school setting to contain the COVID-19 pandemic: A scoping review. Cochrane Database Syst. Rev. 2020, 12, CD013812. [Google Scholar] [CrossRef] [PubMed]
- Lessler, J.; Grabowski, M.K.; Grantz, K.H.; Badillo-Goicoechea, E.; Metcalf, C.J.E. Household COVID-19 risk and in-person schooling. Science 2021, 4, 1092–1097. [Google Scholar] [CrossRef]

| Whole Study Period | Pre-Alpha | Alpha | |
|---|---|---|---|
| Number of contact investigations, all (n, %) | 43 | 32 | 11 |
| 1–4th grade | 15 (35) | 9 (28) | 6 (55) |
| 5–7th grade | 14 (33) | 11 (34) | 3 (27) |
| 8–10th grade | 14 (33) | 12 (38) | 2 (18) |
| Number of child contacts, all (n, %) | 599 | 441 | 118 |
| 1–4th grade | 214 (36) | 154 (35) | 60 (51) |
| 5–7th grade | 188 (31) | 166 (38) | 22 (19) |
| 8–10th grade | 157 (26) | 121 (27) | 36 (31) |
| Number of adult contacts, all (n, %) | 100 | 81 | 19 |
| 1–4th grade | 53 (53) | 43 (53) | 10 (53) |
| 5–7th grade | 20 (20) | 17 (21) | 3 (16) |
| 8–10th grade | 27 (27) | 21 (26) | 6 (32) |
| Number of child contacts per index case (median, range) # | 13 (3–33) | 15 (4–33) | 6 (4–32) |
| Participation child contacts (median, range) # | 60 (14–89) | 68 (14–89) | 44 (14–72) |
| Number of adult contacts per index case (median, range) # | 2 (0–12) | 2 (0–12) | 1 (0–3) |
| Participation adult contacts (median, range) # | 67 (0–100) | 67 (0–100) | 50 (0–100) |
| IPC-score (median, range) | 7 (6–8) | 6 (5–8) | 7 (6–8) |
| Number of Contacts, n (n) # | Primary I Cases, n (%, 95% CI) | Secondary II Cases, n (%, 95% CI) | All Infected Cases III n (%, 95% CI) | |
|---|---|---|---|---|
| All child contacts | 559 (537) | 4 (0.7, 0.20–1.82) | 4 (0.7, 0.20–1.90) | 8 (1.4, 0.62–2.80) |
| pre-Alpha * | 441 (426) | 3 (0.7, 0.14–1.97) | 3 (0.7, 0.15–2.04) | 6 (1.4, 0.50–2.94) |
| Alpha * | 118 (111) | 1 (0.9, 0.02–4.63) | 1 (0.9, 0.02–4.92) | 2 (1.7, 0.21–5.99) |
| Child contacts by school grade | ||||
| Child contacts, grade 1–4 (all) | 214 (206) | 1 (0.5, 0.01–2.58) | 0 | 1 (0.5, 0.01–2.58) |
| pre-Alpha | 154 (148) | 1 (0.7, 0.02–3.56) | 0 | 1 (0.7, 0.02–3.56) |
| Alpha | 60 (58) | 0 | 0 | 0 |
| Child contacts, grade 5–7 (all) | 188 (183) | 1 (0.5, 0.01–2.93) | 2 (1.1, 0.13–3.89) | 3 (1.6, 0.33–4.59) |
| pre-Alpha | 166 (163) | 1 (0.6, 0.02–3.31) | 1 (0.6, 0.02–3.37) | 2 (1.2, 0.15–4.28) |
| Alpha | 22 (20) | 0 | 1 (5.0, 0.13–22.87) | 1 (4.5, 0.12–22.84) |
| Child contacts, grade 8–10 (all) | 157 (148) | 2 (1.3, 0.15–4.53) | 2 (1.4, 0.16–4.58) | 4 (2.6, 0.70–6.39) |
| pre-Alpha | 121 (115) | 1 (0.8, 0.02–4.52) | 2 (1.8, 0.20–6.14) | 3 (2.5 0.51–7.07) |
| Alpha | 36 (33) | 1 (2.8, 0.07–14.5) | 0 | 1 (2.8, 0.07–14.53) |
| SARS-CoV-2 Variant I | Number of Contact Investigations | Time of Contact-Investigation | Period # |
|---|---|---|---|
| B.1.1.7 | 7 | April 2021–May 2021 | Alpha |
| B.1.36.21 | 6 | November 2020–January 2021 | pre-Alpha |
| K.3 | 5 | October 2020 | pre-Alpha |
| B.1.367 | 3 | September 2020–October 2020 | pre-Alpha |
| B.1.1.305 | 3 | December 2020–January 2021 | pre-Alpha |
| B.1.1 | 2 | November 2020–January 2021 | pre-Alpha |
| Other * | 7 | September 2020–January 2021 | pre-Alpha |
| ID | Period | School-Grade | SARS-CoV-2 Variant | SNP Difference | ||
|---|---|---|---|---|---|---|
| Index Case I | Primary Case II | Secondary Case III | ||||
| 08 | pre-Alpha | 1–4 | K.3 | K.3 | 2 SNPs | |
| 14 | pre-Alpha | 5–7 | B.1.1 | B.1.1 | B.1.1 | 0 SNP |
| 17 | pre-Alpha | 8–10 | B.1.36.21 | B.1.36.21 | 1 SNP | |
| 24 | pre-Alpha | 5–7 | B.1.1.305 | B.1.1.305 | 1 SNP | |
| 28 | pre-Alpha | 8–10 | B.1.1.305 | WGS failed | na | |
| 30 | pre-Alpha | 8–10 | B.1.36.21 | B.1.1.333 | na | |
| 33 | Alpha | 8–10 | B.1.1.7 | na | ||
| 41 | Alpha | 5–7 | B.1.1.7 | WGS failed | na | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winje, B.A.; Ofitserova, T.S.; Brynildsrud, O.B.; Greve-Isdahl, M.; Bragstad, K.; Rykkvin, R.; Hungnes, O.; Lund, H.M.; Nygård, K.; Meijerink, H.; et al. Comprehensive Contact Tracing, Testing and Sequencing Show Limited Transmission of SARS-CoV-2 between Children in Schools in Norway, August 2020 to May 2021. Microorganisms 2021, 9, 2587. https://doi.org/10.3390/microorganisms9122587
Winje BA, Ofitserova TS, Brynildsrud OB, Greve-Isdahl M, Bragstad K, Rykkvin R, Hungnes O, Lund HM, Nygård K, Meijerink H, et al. Comprehensive Contact Tracing, Testing and Sequencing Show Limited Transmission of SARS-CoV-2 between Children in Schools in Norway, August 2020 to May 2021. Microorganisms. 2021; 9(12):2587. https://doi.org/10.3390/microorganisms9122587
Chicago/Turabian StyleWinje, Brita Askeland, Trine Skogset Ofitserova, Ola Brønstad Brynildsrud, Margrethe Greve-Isdahl, Karoline Bragstad, Rikard Rykkvin, Olav Hungnes, Hilde Marie Lund, Karin Nygård, Hinta Meijerink, and et al. 2021. "Comprehensive Contact Tracing, Testing and Sequencing Show Limited Transmission of SARS-CoV-2 between Children in Schools in Norway, August 2020 to May 2021" Microorganisms 9, no. 12: 2587. https://doi.org/10.3390/microorganisms9122587
APA StyleWinje, B. A., Ofitserova, T. S., Brynildsrud, O. B., Greve-Isdahl, M., Bragstad, K., Rykkvin, R., Hungnes, O., Lund, H. M., Nygård, K., Meijerink, H., & Brandal, L. T. (2021). Comprehensive Contact Tracing, Testing and Sequencing Show Limited Transmission of SARS-CoV-2 between Children in Schools in Norway, August 2020 to May 2021. Microorganisms, 9(12), 2587. https://doi.org/10.3390/microorganisms9122587