
Space-Time Trends in Lassa Fever in Sierra Leone by ELISA Serostatus, 2012–2019

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Study Design and Inclusion Criteria
2.3. Lassa Fever Clinical Database
2.4. Lassa Fever Enzyme-Linked Immunosorbent Assay (ELISA) Diagnostics
2.5. Statistical Analysis
3. Results
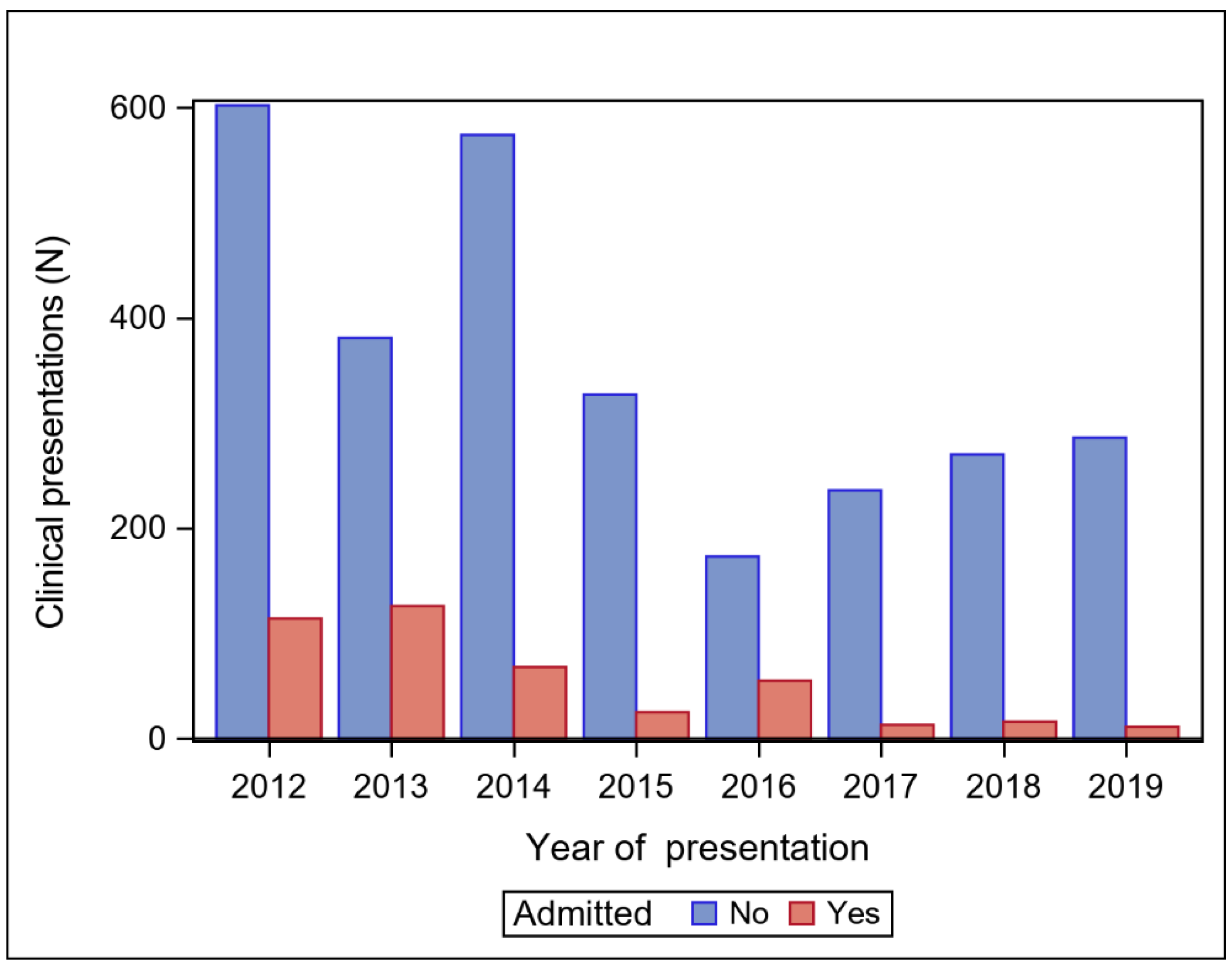
3.1. Lassa Fever Suspected Cases by Year of Clinical Presentation
3.2. Serostatus Group Comparisons
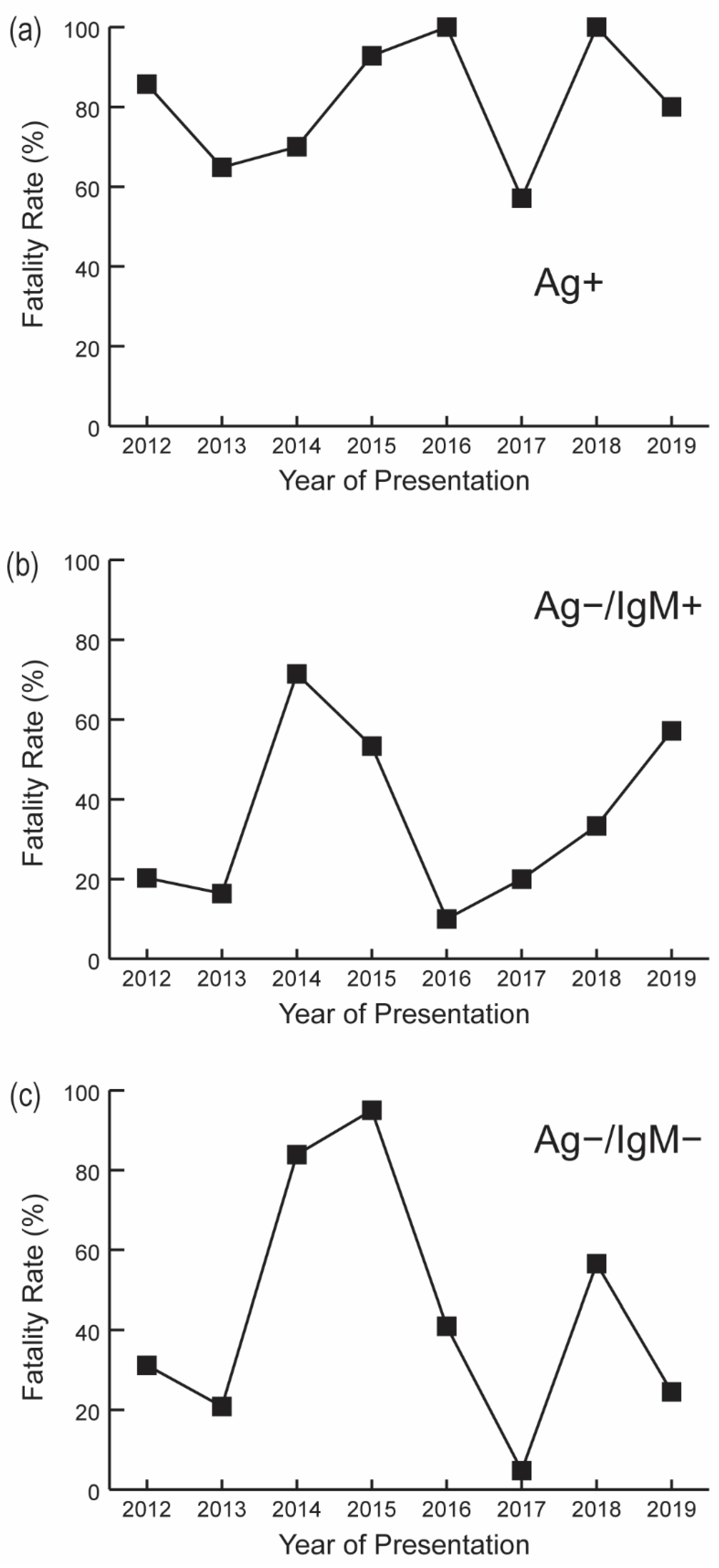
3.3. Fatality Rates by Serostatus
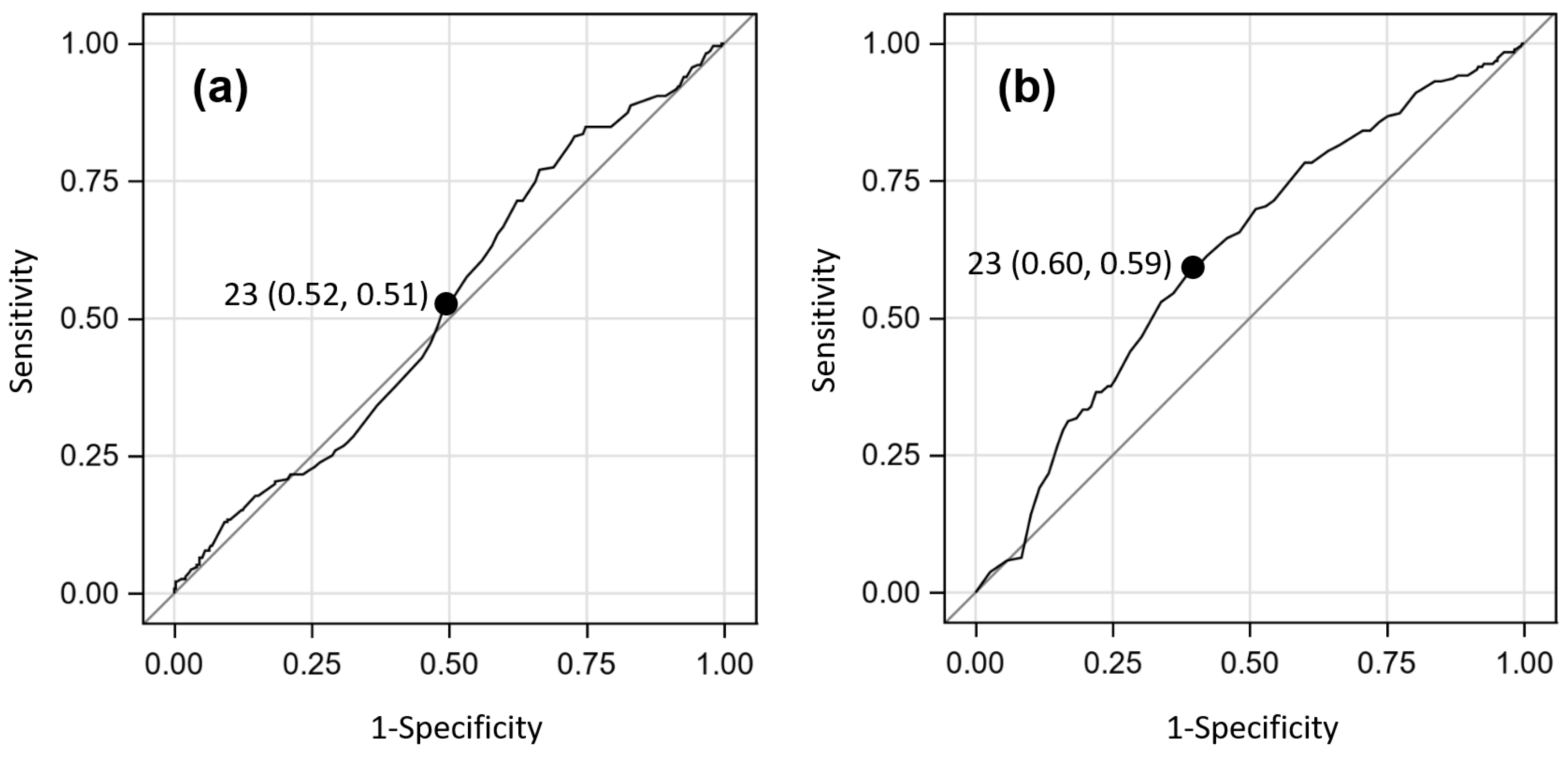
3.4. Breakpoints for Continuous Age Predictor
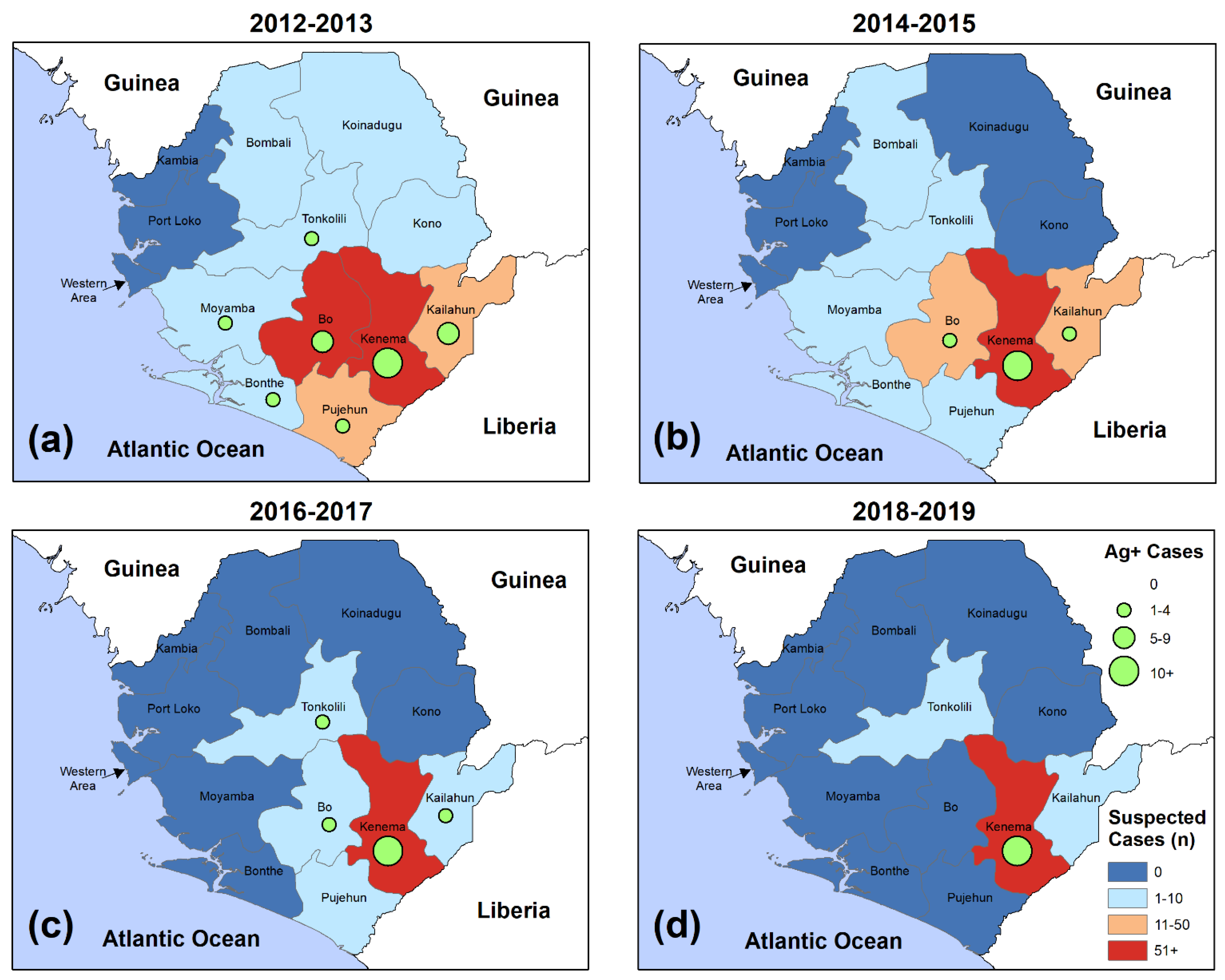
3.5. Space-Time Trends in Suspected LF Presentations and Confirmed Cases
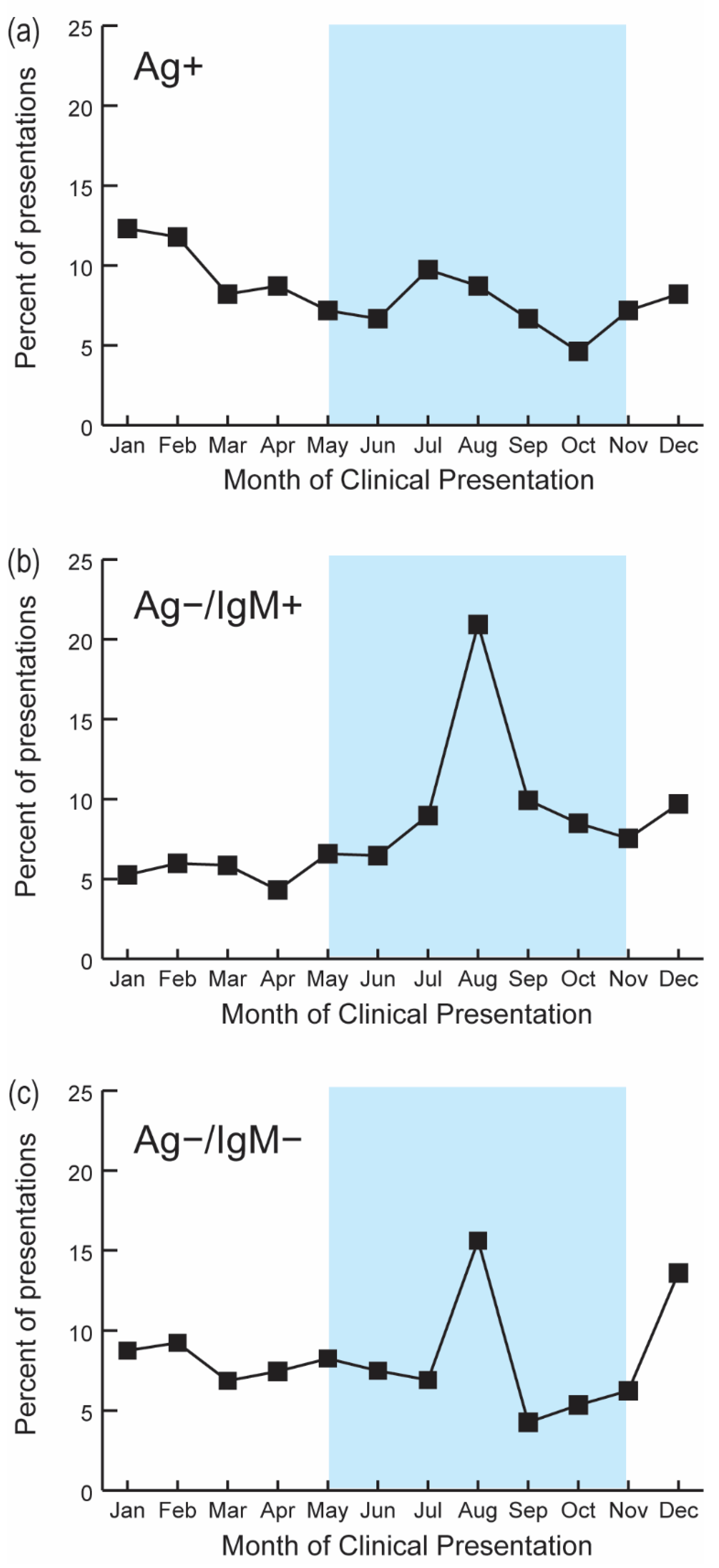
3.6. Seasonality of Lassa Fever Presentations
3.7. Impact of the 2014–2016 Ebola Epidemic on LF Epidemiological Factors
4. Discussion
4.1. Testing Is Likely Prioritizing Subjects at Late Stages of Acute LF Infection
4.2. The Definition of Confirmed LF Cases Significantly Influences CFRs
4.3. LF Remains Endemic in Sierra Leone
4.4. LF Case-Fatality Rates Are Higher in the Dry Season and Recent, Non-Acute LF Exposures Are More Likely to Present in the Rainy Season
4.5. Suspected LF Case Frequencies Have Yet to Recover Following the 2014–2016 Ebola Epidemic
4.6. Only a Few Confirmed Cases LF Cases Are Needed to Constitute an LF Outbreak
4.7. Subjects Aged over 40 Years Are Less Frequently Observed in the Acute or Recent Serostatus Groups
4.8. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Lassa Fever. 2021. Available online: https://www.who.int/health-topics/lassa-fever#tab=tab_1 (accessed on 11 January 2021).
- World Health Organization. Lassa Fever. Available online: https://www.who.int/news-room/fact-sheets/detail/lassa-fever (accessed on 12 January 2021).
- Ogbu, O.; Ajuluchukwu, E.; Uneke, C.J. Lassa fever in West African sub-region: An overview. J. Vector Borne Dis. 2007, 44, 1–11. [Google Scholar] [PubMed]
- McCormick, J.B. Epidemiology and control of Lassa fever. Curr. Top. Microbiol. Immunol. 1987, 134, 69–78. [Google Scholar] [CrossRef]
- Garry, R.F. 50 Years of Lassa Fever Research. Curr. Top. Microbiol. Immunol. 2020. [Google Scholar] [CrossRef]
- Monath, T.P.; Newhouse, V.F.; Kemp, G.E.; Setzer, H.W.; Cacciapuoti, A. Lassa virus isolation from Mastomys natalensis rodents during an epidemic in Sierra Leone. Science 1974, 185, 263–265. [Google Scholar] [CrossRef] [PubMed]
- McCormick, J.B.; Webb, P.A.; Krebs, J.W.; Johnson, K.M.; Smith, E.S. A prospective study of the epidemiology and ecology of Lassa fever. J. Infect. Dis. 1987, 155, 437–444. [Google Scholar] [CrossRef]
- Sattler, R.A.; Paessler, S.; Ly, H.; Huang, C. Animal Models of Lassa Fever. Pathogens 2020, 9, 197. [Google Scholar] [CrossRef] [Green Version]
- Raabe, V.; Koehler, J. Laboratory Diagnosis of Lassa Fever. J. Clin. Microbiol. 2017, 55, 1629–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birmingham, K.; Kenyon, G. Lassa fever is unheralded problem in West Africa. Nat. Med. 2001, 7, 878. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Lassa Fever. 2019. Available online: https://www.cdc.gov/vhf/lassa/index.html (accessed on 9 January 2021).
- Iacono, G.L.; Cunningham, A.A.; Fichet-Calvet, E.; Garry, R.F.; Grant, D.S.; Khan, S.H.; Leach, M.; Moses, L.M.; Schieffelin, J.S.; Shaffer, J.G.; et al. Using modelling to disentangle the relative contributions of zoonotic and anthroponotic transmission: The case of lassa fever. PLoS Negl. Trop. Dis. 2015, 9, e3398. [Google Scholar] [CrossRef] [Green Version]
- McCormick, J.B.; King, I.J.; Webb, P.A.; Johnson, K.M.; O’Sullivan, R.; Smith, E.S.; Trippel, S.; Tong, T.C. A case-control study of the clinical diagnosis and course of Lassa fever. J. Infect. Dis. 1987, 155, 445–455. [Google Scholar] [CrossRef]
- Fichet-Calvet, E.; Rogers, D.J. Risk maps of Lassa fever in West Africa. PLoS Negl. Trop. Dis. 2009, 3, e388. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Allergy and Infectious Diseases. NIAID Emerging Infectious Diseases/Pathogens. 2018. Available online: https://www.niaid.nih.gov/research/emerging-infectious-diseases-pathogens (accessed on 13 January 2021).
- McCormick, J.B.; King, I.J.; Webb, P.A.; Scribner, C.L.; Craven, R.B.; Johnson, K.M.; Elliott, L.H.; Belmont-Williams, R. Lassa fever. Effective therapy with ribavirin. N. Engl. J. Med. 1986, 314, 20–26. [Google Scholar] [CrossRef]
- Khan, S.H.; Goba, A.; Chu, M.; Roth, C.; Healing, T.; Marx, A.; Fair, J.; Guttieri, M.C.; Ferro, P.; Imes, T.; et al. New opportunities for field research on the pathogenesis and treatment of Lassa fever. Antivir. Res. 2008, 78, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Coalition for Epidemic Preparedness Innovations. Largest-Ever Lassa Fever Research Programme Launches in West Africa. Available online: https://cepi.net/news_cepi/largest-ever-lassa-fever-research-programme-launches-in-west-africa/ (accessed on 6 March 2021).
- Fraser, D.W.; Campbell, C.C.; Monath, T.P.; Goff, P.A.; Gregg, M.B. Lassa fever in the Eastern Province of Sierra Leone, 1970–1972. I. Epidemiologic studies. Am. J. Trop. Med. Hyg. 1974, 23, 1131–1139. [Google Scholar] [CrossRef]
- Shaffer, J.G.; Grant, D.S.; Schieffelin, J.S.; Boisen, M.L.; Goba, A.; Hartnett, J.N.; Levy, D.C.; Yenni, R.E.; Moses, L.M.; Fullah, M.; et al. Lassa fever in post-conflict sierra leone. PLoS Negl. Trop. Dis. 2014, 8, e2748. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, J.G.; Schieffelin, J.S.; Grant, D.S.; Goba, A.; Momoh, M.; Kanneh, L.; Levy, D.C.; Hartnett, J.N.; Boisen, M.L.; Branco, L.M.; et al. Data set on Lassa fever in post-conflict Sierra Leone. Data Brief 2019, 23, 103673. [Google Scholar] [CrossRef]
- Kangbai, J.; Kamara, F.; Lahai, R.; Gebeh, F. Lassa Fever in post-Ebola Sierra Leone. Sociodemographics and case fatality rates of in-hospital patients admitted at the Kenema Government Hospital Lassa Fever Ward between 2016–2018. J. Virol. Pathog. 2020, 1, 101. [Google Scholar]
- Samuels, R.J.; Moon, T.D.; Starnes, J.R.; Alhasan, F.; Gbakie, M.; Goba, A.; Koroma, V.; Momoh, M.; Sandi, J.D.; Garry, R.F.; et al. Lassa Fever among Children in Eastern Province, Sierra Leone: A 7-year Retrospective Analysis (2012–2018). Am. J. Trop. Med. Hyg. 2020, tpmd200773. [Google Scholar] [CrossRef]
- Kenmoe, S.; Tchatchouang, S.; Ebogo-Belobo, J.T.; Ka’e, A.C.; Mahamat, G.; Simo, R.E.G.; Bowo-Ngandji, A.; Emoh, C.P.D.; Che, E.; Ngongang, D.T.; et al. Systematic review and meta-analysis of the epidemiology of Lassa virus in humans, rodents and other mammals in sub-Saharan Africa. PLoS Negl. Trop. Dis. 2020, 14, e0008589. [Google Scholar] [CrossRef]
- Akpede, G.O.; Asogun, D.A.; Okogbenin, S.A.; Dawodu, S.O.; Momoh, M.O.; Dongo, A.E.; Ike, C.; Tobin, E.; Akpede, N.; Ogbaini-Emovon, E.; et al. Caseload and Case Fatality of Lassa Fever in Nigeria, 2001–2018: A Specialist Center’s Experience and Its Implications. Front. Public Health 2019, 7, 170. [Google Scholar] [CrossRef]
- Bagcchi, S. Lassa fever outbreak continues across Nigeria. Lancet Infect. Dis. 2020, 20, 543. [Google Scholar] [CrossRef]
- Heinrich, M.L.; Boisen, M.L.; Nelson, D.K.; Bush, D.J.; Cross, R.W.; Koval, A.P.; Hoffmann, A.R.; Beddingfield, B.J.; Hastie, K.M.; Rowland, M.M.; et al. Antibodies from Sierra Leonean and Nigerian Lassa fever survivors cross-react with recombinant proteins representing Lassa viruses of divergent lineages. Sci. Rep. 2020, 10, 16030. [Google Scholar] [CrossRef]
- Sullivan, B.M.; Sakabe, S.; Hartnett, J.N.; Ngo, N.; Goba, A.; Momoh, M.; Sandi, J.D.; Kanneh, L.; Cubitt, B.; Garcia, S.D.; et al. High crossreactivity of human T cell responses between Lassa virus lineages. PLoS Pathog. 2020, 16, e1008352. [Google Scholar] [CrossRef] [PubMed]
- Monath, T.P. A short history of Lassa fever: The first 10–15 years after discovery. Curr. Opin. Virol. 2019, 37, 77–83. [Google Scholar] [CrossRef]
- Branco, L.M.; Grove, J.N.; Boisen, M.L.; Shaffer, J.G.; Goba, A.; Fullah, M.; Momoh, M.; Grant, D.S.; Garry, R.F. Emerging trends in Lassa fever: Redefining the role of immunoglobulin M and inflammation in diagnosing acute infection. Virol. J. 2011, 8, 478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boisen, M.L.; Uyigue, E.; Aiyepada, J.; Siddle, K.J.; Oestereich, L.; Nelson, D.K.; Bush, D.J.; Rowland, M.M.; Heinrich, M.L.; Eromon, P.; et al. Field evaluation of a Pan-Lassa rapid diagnostic test during the 2018 Nigerian Lassa fever outbreak. Sci. Rep. 2020, 10, 8724. [Google Scholar] [CrossRef]
- Viral Hemorrhagic Fever Consortium. Viral Hemorrhagic Fever Consortium. 2021. Available online: https://vhfc.org/ (accessed on 12 January 2021).
- Centers for Disease Control and Prevention. 2014–2016 Ebola Outbreak in West Africa. 2019. Available online: https://www.cdc.gov/vhf/ebola/history/2014-2016-outbreak/index.html#:~:text=After%20an%20initial%20declaration%20in,March%20and%20April%20of%202016 (accessed on 19 January 2021).
- Goba, A.; Khan, S.H.; Fonnie, M.; Fullah, M.; Moigboi, A.; Kovoma, A.; Sinnah, V.; Yoko, N.; Rogers, H.; Safai, S.; et al. An Outbreak of Ebola Virus Disease in the Lassa Fever Zone. J. Infect. Dis. 2016, 214 (Suppl. 3), S110–S121. [Google Scholar] [CrossRef] [PubMed]
- BBC News. Ebola Intensifies the Struggle to Cope with Lassa Fever. 2014. Available online: https://www.bbc.com/news/world-africa-29868394 (accessed on 21 January 2021).
- Check Hayden, E. Infectious disease: Ebola’s lost ward. Nature 2014, 513, 474–477. [Google Scholar] [CrossRef] [Green Version]
- Schieffelin, J.S.; Shaffer, J.G.; Goba, A.; Gbakie, M.; Gire, S.K.; Colubri, A.; Sealfon, R.S.; Kanneh, L.; Moigboi, A.; Momoh, M.; et al. Clinical illness and outcomes in patients with Ebola in Sierra Leone. N. Engl. J. Med. 2014, 371, 2092–2100. [Google Scholar] [CrossRef]
- Quaglio, G.; Tognon, F.; Finos, L.; Bome, D.; Sesay, S.; Kebbie, A.; Di Gennaro, F.; Camara, B.S.; Marotta, C.; Pisani, V.; et al. Impact of Ebola outbreak on reproductive health services in a rural district of Sierra Leone: A prospective observational study. BMJ Open 2019, 9, e029093. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.A.; Gopalakrishnan, S.; Ameh, C.A.; White, S.; van den Broek, N.R. Women and babies are dying but not of Ebola’: The effect of the Ebola virus epidemic on the availability, uptake and outcomes of maternal and newborn health services in Sierra Leone. BMJ Glob. Health 2016, 1, e000065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Statement on the End of the Ebola Outbreak in Sierra Leone. 2015. Available online: https://www.afro.who.int/news/statement-end-ebola-outbreak-sierra-leone (accessed on 19 January 2021).
- The World Bank. Sierra Leone. 2021. Available online: https://data.worldbank.org/country/SL (accessed on 20 January 2021).
- Worldometer. Sierra Leone Population. Available online: https://www.worldometers.info/world-population/sierra-leone-population/ (accessed on 20 January 2021).
- Wikipedia. Districts of Sierra Leone. 2020. Available online: https://en.wikipedia.org/wiki/Districts_of_Sierra_Leone (accessed on 29 January 2021).
- Wikipedia. Geography of Sierra Leone. 2020. Available online: https://en.wikipedia.org/wiki/Geography_of_Sierra_Leone#:~:text=Physical%20geography,-Sierra%20Leone%20is&text=Sierra%20Leone%20has%20four%20distinct,1%2C948%20meters%20(6%2C391%20ft) (accessed on 23 January 2021).
- Senga, M.; Pringle, K.; Ramsay, A.; Brett-Major, D.M.; Fowler, R.A.; French, I. Factors Underlying Ebola Virus Infection Among Health Workers, Kenema, Sierra Leone, 2014–2015. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, 454–459. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, J.G.; Schieffelin, J.S.; Gbakie, M.; Alhasan, F.; Roberts, N.B.; Goba, A.; Randazzo, J.; Momoh, M.; Moon, T.D.; Kanneh, L.; et al. A medical records and data capture and management system for Lassa fever in Sierra Leone: Approach, implementation, and challenges. PLoS ONE 2019, 14, e0214284. [Google Scholar] [CrossRef] [PubMed]
- Boisen, M.L.; Hartnett, J.N.; Shaffer, J.G.; Goba, A.; Momoh, M.; Sandi, J.D.; Fullah, M.; Nelson, D.K.; Bush, D.J.; Rowland, M.M.; et al. Field validation of recombinant antigen immunoassays for diagnosis of Lassa fever. Sci Rep. 2018, 8, 5939. [Google Scholar] [CrossRef]
- SAS Institute Inc. Pharmaceutical Statistics Using SAS; SAS Institute, Inc.: Cary, NC, USA, 2007. [Google Scholar]
- Wilhelm, J.A.; Helleringer, S. Utilization of non-Ebola health care services during Ebola outbreaks: A systematic review and meta-analysis. J. Glob. Health 2019, 9, 010406. [Google Scholar] [CrossRef] [PubMed]
- Bolkan, H.A.; van Duinen, A.; Samai, M.; Gassama, I.; Waalewijn, B.; Wibe, A.; von Schreeb, J. Admissions and surgery as indicators of hospital functions in Sierra Leone during the west-African Ebola outbreak. BMC Health Serv. Res. 2018, 18, 846. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, B.H.; Augusto, O.; Beste, J.; Toomay, S.J.; Wickett, E.; Dunbar, N.; Bawo, L.; Wesseh, C.S. The 2014–2015 Ebola virus disease outbreak and primary healthcare delivery in Liberia: Time-series analyses for 2010–2016. PLoS Med. 2018, 15, e1002508. [Google Scholar] [CrossRef] [Green Version]
- Camara, B.S.; Delamou, A.; Diro, E.; Béavogui, A.H.; El Ayadi, A.M.; Sidibé, S.; Grovogui, F.M.; Takarinda, K.C.; Bouedouno, P.; Sandouno, S.D.; et al. Effect of the 2014/2015 Ebola outbreak on reproductive health services in a rural district of Guinea: An ecological study. Trans. R. Soc. Trop. Med. Hyg. 2017, 111, 22–29. [Google Scholar] [CrossRef]
- Roberts, L. Nigeria hit by unprecedented Lassa fever outbreak. Science 2018, 359, 1201–1202. [Google Scholar] [CrossRef]
- Purushotham, J.; Lambe, T.; Gilbert, S.C. Vaccine platforms for the prevention of Lassa fever. Immunol. Lett. 2019, 215, 1–11. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Serostatus | p Value d | ||
|---|---|---|---|---|
| Ag+ (n = 195) | Ag−/IgM+ (n = 838) | Ag−/IgM− (n = 2244) | ||
| Admission status | ||||
| Admitted | 106 (54) | 159 (19) | 163 (7) | <0.001 |
| Not admitted | 89 (46) | 679 (81) | 2081 (93) | |
| Gender | ||||
| Female | 101 (52) | 435 (57) | 1071 (56) | 0.471 |
| Male | 92 (48) | 326 (43) | 850 (44) | |
| Age in years | ||||
| <5 | 35 (19) | 84 (13) | 180 (12) | <0.001 |
| 5–14 | 33 (17) | 97 (14) | 175 (11) | |
| 15–40 | 103 (55) | 363 (55) | 890 (57) | |
| >40 | 17 (9) | 117 (18) | 307 (20) | |
| District of residence | ||||
| Bo | 12 (9) | 42 (12) | 79 (12) | 0.712 |
| Kenema | 104 (79) | 265 (75) | 506 (77) | |
| Other | 16 (12) | 47 (13) | 72 (11) | |
| Survival outcome a | ||||
| Died | 106 (79) | 67 (31) | 259 (54) | <0.001 |
| Discharged | 29 (21) | 149 (69) | 222 (46) | |
| Time since illness onset | ||||
| <7 days | 47 (43) | 145 (43) | 357 (66) | <0.001 |
| ≥7 days | 62 (57) | 192 (57) | 184 (34) | |
| IgG serostatus b | ||||
| Positive | 42 (23) | 291 (37) | 682 (33) | 0.001 |
| Negative | 140 (77) | 492 (63) | 1369 (67) | |
| Season of presentation c | ||||
| Dry | 110 (56) | 323 (39) | 1162 (52) | <0.001 |
| Rainy | 85 (44) | 513 (61) | 1067 (48) | |
| Characteristic | Season of Presentation e | p Value f | |
|---|---|---|---|
| Rainy (n = 1665) | Dry (n = 1595) | ||
| Admission status | |||
| Admitted | 209 (13) | 219 (14) | 0.320 |
| Not admitted | 1456 (87) | 1376 (86) | |
| Gender | |||
| Female | 769 (58) | 834 (54) | 0.073 |
| Male | 562 (42) | 698 (46) | |
| Age, years | |||
| <5 | 177 (15) | 121 (10) | 0.005 |
| 5–14 | 141 (12) | 163 (14) | |
| 15–40 | 663 (55) | 691 (58) | |
| >40 | 219 (18) | 220 (18) | |
| District of residence | |||
| Bo | 70 (12) | 63 (11) | 0.335 |
| Kenema | 427 (77) | 446 (76) | |
| Other | 59 (11) | 76 (13) | |
| Survival outcome a | |||
| Died | 136 (42) | 295 (58) | <0.001 |
| Discharged | 187 (58) | 212 (42) | |
| Time since illness onset | |||
| <7 days | 267 (54) | 280 (57) | 0.347 |
| ≥7 days | 227 (46) | 211 (43) | |
| Ag serostatus b | |||
| Positive | 85 (5) | 110 (7) | 0.031 |
| Negative | 1580 (95) | 1485 (93) | |
| IgM serostatus c | |||
| Positive | 559 (34) | 356 (22) | <0.001 |
| Negative | 1106 (66) | 1239 (78) | |
| IgG serostatus d | |||
| Positive | 541 (34) | 467 (33) | 0.763 |
| Negative | 1057 (66) | 934 (67) | |
| Characteristic | Time Period | p Value f | ||
|---|---|---|---|---|
| Pre-Ebola n = 1384 | Ebola e n = 783 | Post-Ebola n = 1110 | ||
| Admission status | ||||
| Admitted | 306 (22) | 24 (3) | 98 (9) | <0.001 |
| Not admitted | 1078 (78) | 759 (97) | 1012 (91) | |
| Gender | ||||
| Female | 811 (59) | 213 (49) | 583 (55) | 0.036 |
| Male | 564 (41) | 222 (51) | 482 (45) | |
| Age, years | ||||
| <5 | 158 (13) | 17 (7) | 124 (13) | 0.346 |
| 5–14 | 171 (14) | 27 (11) | 107 (11) | |
| 15–40 | 676 (56) | 141 (57) | 539 (58) | |
| >40 | 212 (17) | 61 (25) | 168 (18) | |
| District | ||||
| Bo | 131 (16) | 0 (0) | 2 (1) | <0.001 |
| Kenema | 569 (69) | 18 (95) | 288 (96) | |
| Other | 124 (15) | 1 (5) | 10 (3) | |
| Survival outcome a | ||||
| Died | 131 (34) | 215 (96) | 86 (40) | 0.120 |
| Discharged | 260 (66) | 10 (4) | 130 (60) | |
| Serostatus b | ||||
| Ag+ | 85 (6) | 21 (3) | 89 (8) | <0.001 |
| Ag−/IgM+ | 504 (36) | 151 (19) | 183 (16) | |
| Ag−/IgM− | 795 (58) | 611 (78) | 838 (76) | |
| Time since illness onset | ||||
| <7 days | 314 (46) | 7 (44) | 228 (80) | <0.001 |
| ≥7 days | 373 (54) | 9 (56) | 56 (20) | |
| IgG serostatus c | ||||
| Positive | 295 (22) | 342 (44) | 378 (43) | <0.001 |
| Negative | 1070 (78) | 430 (56) | 501 (57) | |
| Season of presentation d | ||||
| Rainy | 767 (55) | 470 (60) | 428 (39) | <0.001 |
| Dry | 617 (45) | 309 (40) | 669 (61) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaffer, J.G.; Schieffelin, J.S.; Momoh, M.; Goba, A.; Kanneh, L.; Alhasan, F.; Gbakie, M.; Engel, E.J.; Bond, N.G.; Hartnett, J.N.; et al. Space-Time Trends in Lassa Fever in Sierra Leone by ELISA Serostatus, 2012–2019. Microorganisms 2021, 9, 586. https://doi.org/10.3390/microorganisms9030586
Shaffer JG, Schieffelin JS, Momoh M, Goba A, Kanneh L, Alhasan F, Gbakie M, Engel EJ, Bond NG, Hartnett JN, et al. Space-Time Trends in Lassa Fever in Sierra Leone by ELISA Serostatus, 2012–2019. Microorganisms. 2021; 9(3):586. https://doi.org/10.3390/microorganisms9030586
Chicago/Turabian StyleShaffer, Jeffrey G., John S. Schieffelin, Mambu Momoh, Augustine Goba, Lansana Kanneh, Foday Alhasan, Michael Gbakie, Emily J. Engel, Nell G. Bond, Jessica N. Hartnett, and et al. 2021. "Space-Time Trends in Lassa Fever in Sierra Leone by ELISA Serostatus, 2012–2019" Microorganisms 9, no. 3: 586. https://doi.org/10.3390/microorganisms9030586
APA StyleShaffer, J. G., Schieffelin, J. S., Momoh, M., Goba, A., Kanneh, L., Alhasan, F., Gbakie, M., Engel, E. J., Bond, N. G., Hartnett, J. N., Nelson, D. K. S., Bush, D. J., Boisen, M. L., Heinrich, M. L., Rowland, M. M., Branco, L. M., Samuels, R. J., Garry, R. F., Grant, D. S., & the Viral Hemorrhagic Fever Consortium. (2021). Space-Time Trends in Lassa Fever in Sierra Leone by ELISA Serostatus, 2012–2019. Microorganisms, 9(3), 586. https://doi.org/10.3390/microorganisms9030586