
Survival Analysis of Male Patients with Brain Metastases at Initial Breast Cancer Diagnosis over the Last Decade


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giordano, S.H. Breast Cancer in Men. N. Engl. J. Med. 2018, 378, 2311–2320. [Google Scholar] [CrossRef]
- Ly, D.; Forman, D.; Ferlay, J.; Brinton, L.A.; Cook, M.B. An international comparison of male and female breast cancer incidence rates. Int. J. Cancer 2013, 132, 1918–1926. [Google Scholar] [CrossRef]
- Konduri, S.; Singh, M.; Bobustuc, G.; Rovin, R.; Kassam, A. Epidemiology of male breast cancer. Breast 2020, 54, 8–14. [Google Scholar] [CrossRef]
- Fentiman, I.S. Risk factors for male breast cancer. Am. J. Transl. Res. 2023, 15, 6918–6925. [Google Scholar]
- Hultborn, R.; Hanson, C.; Köpf, I.; Verbiené, I.; Warnhammar, E.; Weimarck, A. Prevalence of Klinefelter’s syndrome in male breast cancer patients. Anticancer Res. 1997, 17, 4293–4297. [Google Scholar]
- Ibrahim, M.; Yadav, S.; Ogunleye, F.; Zakalik, D. Male BRCA mutation carriers: Clinical characteristics and cancer spectrum. BMC Cancer 2018, 18, 179. [Google Scholar] [CrossRef]
- Hassett, M.J.; Somerfield, M.R.; Giordano, S.H. Management of Male Breast Cancer: ASCO Guideline Summary. JCO Oncol. Pract. 2020, 16, e839–e843. [Google Scholar] [CrossRef]
- Jackson, A.W.; Muldal, S.; Ockey, C.H.; O’Connor, P.J. Carcinoma of Male Breast in Association with the Klinefelter Syndrome. Br. Med. J. 1965, 1, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Watase, C.; Shiino, S.; Shimoi, T.; Noguchi, E.; Kaneda, T.; Yamamoto, Y.; Yonemori, K.; Takayama, S.; Suto, A. Breast Cancer Brain Metastasis—Overview of Disease State, Treatment Options and Future Perspectives. Cancers 2021, 13, 1078. [Google Scholar] [CrossRef] [PubMed]
- Chew, S.; Carroll, H.K.; Darwish, W.; Boychak, O.; Higgins, M.; McCaffrey, J.; Kelly, C.M. Characterization of Treatments and Disease Course for Women with Breast Cancer Brain Metastases: 5-Year Retrospective Single Institution Experience. Cancer Manag. Res. 2021, 13, 8191–8198. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.H.; Woo, C.G.; Lee, Y.J.; Park, Y.S. Brain metastasis with subtype conversion in a patient with male breast cancer: A case report. Medicine 2021, 100, e24373. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.F.; Althuis, M.D.; Brinton, L.A.; Devesa, S.S. Is male breast cancer similar or different than female breast cancer? Breast Cancer Res. Treat. 2004, 83, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.F.; Jatoi, I.; Tse, J.; Rosenberg, P.S. Male breast cancer: A population-based comparison with female breast cancer. J. Clin. Oncol. 2010, 28, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, K.L.; Mainwaring, W.; Miller, A.B.; Lin, T.A.; Jethanandani, A.; Espinoza, A.F.; Piotrowski, M.; Fuller, C.D.; Stauder, M.C.; Shaitelman, S.F.; et al. Exclusion of Men from Randomized Phase III Breast Cancer Clinical Trials. Oncologist 2020, 25, e990–e992. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Bartlett, J.M.S.; Slaets, L.; van Deurzen, C.H.M.; van Leeuwen-Stok, E.; Porter, P.; Linderholm, B.; Hedenfalk, I.; Schröder, C.; Martens, J.; et al. Characterization of male breast cancer: Results of the EORTC 10085/TBCRC/BIG/NABCG International Male Breast Cancer Program. Ann. Oncol. 2018, 29, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Minisini, A.M.; Moroso, S.; Gerratana, L.; Giangreco, M.; Iacono, D.; Poletto, E.; Guardascione, M.; Fontanella, C.; Fasola, G.; Puglisi, F. Risk factors and survival outcomes in patients with brain metastases from breast cancer. Clin. Exp. Metastasis 2013, 30, 951–956. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Chao, S.T.; Shanley, R.; Luo, X.; Sneed, P.K.; Suh, J.; Weil, R.J.; Jensen, A.W.; et al. The effect of tumor subtype on the time from primary diagnosis to development of brain metastases and survival in patients with breast cancer. J. Neuro-Oncol. 2013, 112, 467–472. [Google Scholar] [CrossRef]
- Leone, J.P.; Lee, A.V.; Brufsky, A.M. Prognostic factors and survival of patients with brain metastasis from breast cancer who underwent craniotomy. Cancer Med. 2015, 4, 989–994. [Google Scholar] [CrossRef]
- Lee, S.S.; Ahn, J.H.; Kim, M.K.; Sym, S.J.; Gong, G.; Ahn, S.D.; Kim, S.B.; Kim, W.K. Brain metastases in breast cancer: Prognostic factors and management. Breast Cancer Res. Treat. 2008, 111, 523–530. [Google Scholar] [CrossRef]
- Ogawa, K.; Yoshii, Y.; Nishimaki, T.; Tamaki, N.; Miyaguni, T.; Tsuchida, Y.; Kamada, Y.; Toita, T.; Kakinohana, Y.; Tamaki, W.; et al. Treatment and prognosis of brain metastases from breast cancer. J. Neuro-Oncol. 2008, 86, 231–238. [Google Scholar] [CrossRef]
- Chen, X.; Liu, X.; Zhang, L.; Li, S.; Shi, Y.; Tong, Z. Poorer survival of male breast cancer compared with female breast cancer patients may be due to biological differences. Jpn. J. Clin. Oncol. 2013, 43, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-G.; Zhang, W.-W.; Liao, X.-L.; Sun, J.-Y.; Li, F.-Y.; Su, J.-J.; He, Z.-Y. Men and women show similar survival outcome in stage IV breast cancer. Breast 2017, 34, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Daily, K.; Douglas, E.; Romitti, P.A.; Thomas, A. Epidemiology of De Novo Metastatic Breast Cancer. Clin. Breast Cancer 2021, 21, 302–308. [Google Scholar] [CrossRef]
- Sun, M.S.; Yun, Y.Y.; Liu, H.J.; Yu, Z.H.; Yang, F.; Xu, L. Brain metastasis in de novo breast cancer: An updated population-level study from SEER database. Asian J. Surg. 2022, 45, 2259–2267. [Google Scholar] [CrossRef]
- Doll, K.M.; Rademaker, A.; Sosa, J.A. Practical Guide to Surgical Data Sets: Surveillance, Epidemiology, and End Results (SEER) Database. JAMA Surg. 2018, 153, 588–589. [Google Scholar] [CrossRef]
- White, M.C.; Babcock, F.; Hayes, N.S.; Mariotto, A.B.; Wong, F.L.; Kohler, B.A.; Weir, H.K. The history and use of cancer registry data by public health cancer control programs in the United States. Cancer 2017, 123 (Suppl. 24), 4969–4976. [Google Scholar] [CrossRef] [PubMed]
- Aversa, C.; Rossi, V.; Geuna, E.; Martinello, R.; Milani, A.; Redana, S.; Valabrega, G.; Aglietta, M.; Montemurro, F. Metastatic breast cancer subtypes and central nervous system metastases. Breast 2014, 23, 623–628. [Google Scholar] [CrossRef]
- Leone, J.P.; Leone, J.; Zwenger, A.O.; Iturbe, J.; Vallejo, C.T.; Leone, B.A. Prognostic significance of tumor subtypes in male breast cancer: A population-based study. Breast Cancer Res. Treat. 2015, 152, 601–609. [Google Scholar] [CrossRef]
- Leone, J.; Freedman, R.A.; Lin, N.U.; Tolaney, S.M.; Vallejo, C.T.; Leone, B.A.; Winer, E.P.; Leone, J.P. Tumor subtypes and survival in male breast cancer. Breast Cancer Res. Treat. 2021, 188, 695–702. [Google Scholar] [CrossRef]
- Chavez-Macgregor, M.; Clarke, C.A.; Lichtensztajn, D.; Hortobagyi, G.N.; Giordano, S.H. Male breast cancer according to tumor subtype and race: A population-based study. Cancer 2013, 119, 1611–1617. [Google Scholar] [CrossRef]
- He, D.J.; Yu, D.Q.; Wang, Q.M.; Yu, Z.Y.; Qi, Y.H.; Shao, Q.J.; Chang, H. Breast Cancer Subtypes and Mortality of Breast Cancer Patients with Brain Metastasis at Diagnosis: A Population-Based Study. Inq. J. Health Care Organ. Provis. Financ. 2021, 58, 469580211055636. [Google Scholar] [CrossRef]
- Aizer, A.A.; Chen, M.-H.; McCarthy, E.P.; Mendu, M.L.; Koo, S.; Wilhite, T.J.; Graham, P.L.; Choueiri, T.K.; Hoffman, K.E.; Martin, N.E.; et al. Marital Status and Survival in Patients with Cancer. J. Clin. Oncol. 2013, 31, 3869–3876. [Google Scholar] [CrossRef]
- Zhu, S.; Lei, C. Association between marital status and all-cause mortality of patients with metastatic breast cancer: A population-based study. Sci. Rep. 2023, 13, 9067. [Google Scholar] [CrossRef] [PubMed]
- Akinyemiju, T.; Sakhuja, S.; Waterbor, J.; Pisu, M.; Altekruse, S.F. Racial/ethnic disparities in de novo metastases sites and survival outcomes for patients with primary breast, colorectal, and prostate cancer. Cancer Med. 2018, 7, 1183–1193. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.X.; Gong, Y.; Ling, H.; Hu, X.; Shao, Z.M. Racial/ethnic differences in the outcomes of patients with metastatic breast cancer: Contributions of demographic, socioeconomic, tumor and metastatic characteristics. Breast Cancer Res. Treat. 2019, 173, 225–237. [Google Scholar] [CrossRef]
- Wang, R.; Zhu, Y.; Liu, X.; Liao, X.; He, J.; Niu, L. The Clinicopathological features and survival outcomes of patients with different metastatic sites in stage IV breast cancer. BMC Cancer 2019, 19, 1091. [Google Scholar] [CrossRef] [PubMed]
- Kyeong, S.; Cha, Y.J.; Ahn, S.G.; Suh, S.H.; Son, E.J.; Ahn, S.J. Subtypes of breast cancer show different spatial distributions of brain metastases. PLoS ONE 2017, 12, e0188542. [Google Scholar] [CrossRef] [PubMed]
- Co, M.; Lee, A.; Kwong, A. Delayed presentation, diagnosis, and psychosocial aspects of male breast cancer. Cancer Med. 2020, 9, 3305–3309. [Google Scholar] [CrossRef]
- Li, H.; Zhang, Y.; Teh, M.-S.; Limaye, S.; Cavalcante, F.P.; Shen, J.-B. Analysis of the distinct features of metastasis male breast cancer and its effect on overall survival based on the SEER database compared with female breast cancer. Transl. Cancer Res. 2023, 12, 2371–2378. [Google Scholar] [CrossRef]
- Xie, J.; Ying, Y.Y.; Xu, B.; Li, Y.; Zhang, X.; Li, C. Metastasis pattern and prognosis of male breast cancer patients in US: A population-based study from SEER database. Ther. Adv. Med. Oncol. 2019, 11, 1758835919889003. [Google Scholar] [CrossRef]
- Altiner, S.; Altiner, Ö.T.; Büyükkasap, Ç.; Uğraş Dikmen, A.; Pekcici, M.R.; Erel, S. Analysis of Knowledge about Male Breast Cancer among Patients at Tertiary Medical Center. Am. J. Men’s Health 2023, 17, 15579883231165626. [Google Scholar] [CrossRef] [PubMed]
- Miao, H.; Verkooijen, H.M.; Chia, K.-S.; Bouchardy, C.; Pukkala, E.; Larønningen, S.; Mellemkjær, L.; Czene, K.; Hartman, M. Incidence and Outcome of Male Breast Cancer: An International Population-Based Study. J. Clin. Oncol. 2011, 29, 4381–4386. [Google Scholar] [CrossRef] [PubMed]
- Leone, J.P.; Leone, J.; Zwenger, A.O.; Iturbe, J.; Leone, B.A.; Vallejo, C.T. Prognostic factors and survival according to tumour subtype in women presenting with breast cancer brain metastases at initial diagnosis. Eur. J. Cancer 2017, 74, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Di Lauro, L.; Pizzuti, L.; Barba, M.; Sergi, D.; Sperduti, I.; Mottolese, M.; Del Medico, P.; Belli, F.; Vici, P.; De Maria, R.; et al. Efficacy of chemotherapy in metastatic male breast cancer patients: A retrospective study. J. Exp. Clin. Cancer Res. 2015, 34, 26. [Google Scholar] [CrossRef]
- Anelli, T.F.; Anelli, A.; Tran, K.N.; Lebwohl, D.E.; Borgen, P.I. Tamoxifen administration is associated with a high rate of treatment-limiting symptoms in male breast cancer patients. Cancer 1994, 74, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, M.J.; Thompson, C.K.; Zibecchi, L.T.; Lee, M.K.; Streja, E.; Berkowitz, J.S.; Wenziger, C.M.; Baker, J.L.; DiNome, M.L.; Attai, D.J. How patients experience endocrine therapy for breast cancer: An online survey of side effects, adherence, and medical team support. J. Cancer Surviv. 2021, 15, 29–39. [Google Scholar] [CrossRef]
- Trusson, D.; Quincey, K. Breast Cancer and Hair Loss: Experiential Similarities and Differences in Men’s and Women’s Narratives. Cancer Nurs. 2021, 44, 62–70. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Summary Report on the Graded Prognostic Assessment: An Accurate and Facile Diagnosis-Specific Tool to Estimate Survival for Patients with Brain Metastases. J. Clin. Oncol. 2012, 30, 419–425. [Google Scholar] [CrossRef]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A.; Lin, N.U.; Borges, V.; Abramson, V.; Anders, C.; et al. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2020, 382, 597–609. [Google Scholar] [CrossRef]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B.; et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N. Engl. J. Med. 2021, 384, 1529–1541. [Google Scholar] [CrossRef]
- Cortés, J.; Kim, S.B.; Chung, W.P.; Im, S.A.; Park, Y.H.; Hegg, R.; Kim, M.H.; Tseng, L.M.; Petry, V.; Chung, C.F.; et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine for Breast Cancer. N. Engl. J. Med. 2022, 386, 1143–1154. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| All patients | 22 | 100% | |
| Age | <50 | 7 | 31.8% |
| 50–64 | 7 | 31.8% | |
| >64 | 8 | 36.4% | |
| Race | Non-Hispanic White | 15 | 68.2% |
| Non-Hispanic Black | 3 | 13.6% | |
| NHAPI | 2 | 9.1% | |
| Hispanic (All Races) | 2 | 9.1% | |
| Tumor subtype | HR+/HER2− | 9 | 40.9% |
| HR+/HER2+ | 5 | 22.7% | |
| HR−/HER2+ | 1 | 4.5% | |
| Triple negative | 3 | 13.6% | |
| Unknown | 4 | 18.2% | |
| Grade | I | 0 | 0% |
| II | 5 | 22.7% | |
| III/IV | 11 | 50% | |
| Unknown | 6 | 27.3% | |
| Histology | Ductal | 22 | 100% |
| Lobular | 0 | 0% | |
| Ductal and lobular | 0 | 0% | |
| Other | 0 | 0% | |
| Bone metastases | No | 6 | 27.3% |
| Yes | 16 | 72.7% | |
| Liver metastases | No | 17 | 77.3% |
| Yes | 4 | 18.2% | |
| Unknown | 1 | 4.5% | |
| Lung metastases | No | 9 | 40.9% |
| Yes | 12 | 54.5% | |
| Unknown | 1 | 4.5% | |
| Distant lymph node metastases | No | 5 | 22.7% |
| Yes | 1 | 4.5% | |
| Unknown | 16 | 72.7% | |
| Other metastases | No | 5 | 22.7% |
| Yes | 2 | 9.1% | |
| Unknown | 15 | 68.2% | |
| Surgery (mastectomy or lumpectomy) | No | 18 | 81.8% |
| Yes | 4 | 18.2% | |
| Radiation | No or Unknown | 9 | 40.9% |
| Yes | 13 | 59.1% | |
| Chemotherapy | No or Unknown | 6 | 27.3% |
| Yes | 16 | 72.7% | |
| Marital status at diagnosis | Single | 6 | 27.3% |
| Married | 12 | 54.5% | |
| Other (Separated/Divorced/Widowed) | 3 | 13.6% | |
| Unknown | 1 | 4.5% | |
| Median household income | ≥USD 75,000 | 8 | 36.4% |
| USD 65,000–74,999 | 5 | 22.7% | |
| USD 55,000–64,999 | 5 | 22.7% | |
| USD 45,000–54,999 | 3 | 13.6% | |
| USD 35,000–44,999 | 1 | 4.5% |
| Variable | Median OS (Months) | Log-Rank p |
|---|---|---|
| Age at diagnosis | ||
| <50 years | 9 | <0.53 |
| 50–64 years | 8 | |
| >64 years | 4 | |
| Grade | ||
| II | 6 | 0.9 |
| III/IV | 10 | |
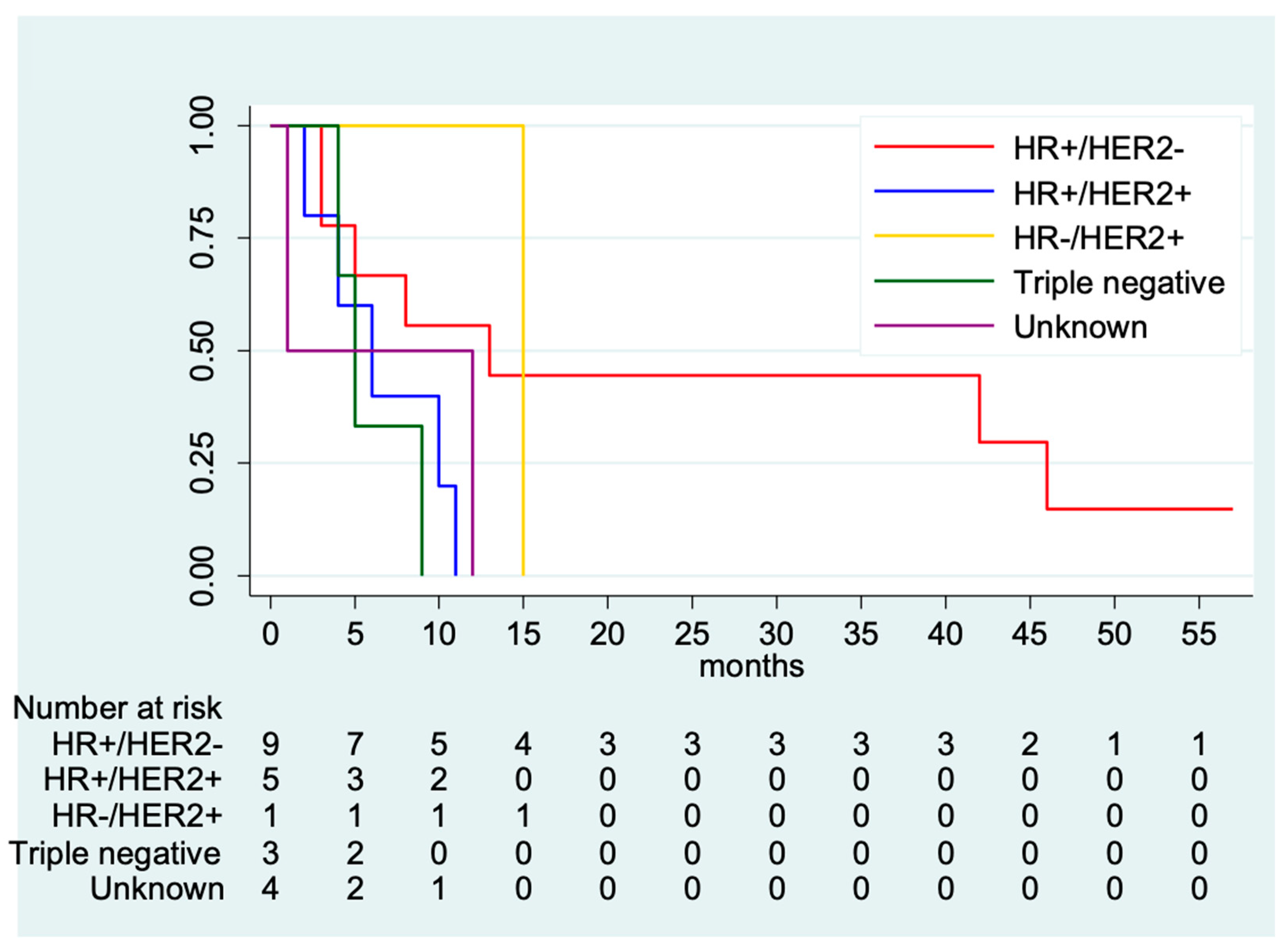
| Tumor subtype | ||
| HR+/Her2- | 13 | 0.19 |
| HR+/Her2+ | 6 | |
| HR-/Her2+ | - | |
| Triple negative | 5 | |
| Unknown | 1 | |
| Race | ||
| NHW | 9 | 0.59 |
| NHB | 5 | |
| NHAPI | 1 | |
| Hispanic | 8 | |
| Surgery | ||
| No | 8 | 0.14 |
| Yes | 5 | |
| Radiation | ||
| No/Unknown | 10 | 0.24 |
| Yes | 5 | |
| Chemotherapy | ||
| No/Unknown | 3 | 0.004 |
| Yes | 10 | |
| Liver metastases | ||
| No | 8 | 0.04 |
| Yes | 2 | |
| Lung metastases | ||
| No | 6 | 0.65 |
| Yes | 8 | |
| Other metastases | ||
| No | 5 | 0.71 |
| Yes | 8 | |
| Marital Status | ||
| Single | 5 | 0.25 |
| Married | 8 | |
| Other | 4 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avila, J.; Leone, J.; Vallejo, C.T.; Leone, J.P. Survival Analysis of Male Patients with Brain Metastases at Initial Breast Cancer Diagnosis over the Last Decade. Med. Sci. 2024, 12, 15. https://doi.org/10.3390/medsci12010015
Avila J, Leone J, Vallejo CT, Leone JP. Survival Analysis of Male Patients with Brain Metastases at Initial Breast Cancer Diagnosis over the Last Decade. Medical Sciences. 2024; 12(1):15. https://doi.org/10.3390/medsci12010015
Chicago/Turabian StyleAvila, Jorge, Julieta Leone, Carlos T. Vallejo, and José P. Leone. 2024. "Survival Analysis of Male Patients with Brain Metastases at Initial Breast Cancer Diagnosis over the Last Decade" Medical Sciences 12, no. 1: 15. https://doi.org/10.3390/medsci12010015
APA StyleAvila, J., Leone, J., Vallejo, C. T., & Leone, J. P. (2024). Survival Analysis of Male Patients with Brain Metastases at Initial Breast Cancer Diagnosis over the Last Decade. Medical Sciences, 12(1), 15. https://doi.org/10.3390/medsci12010015