Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Specimens
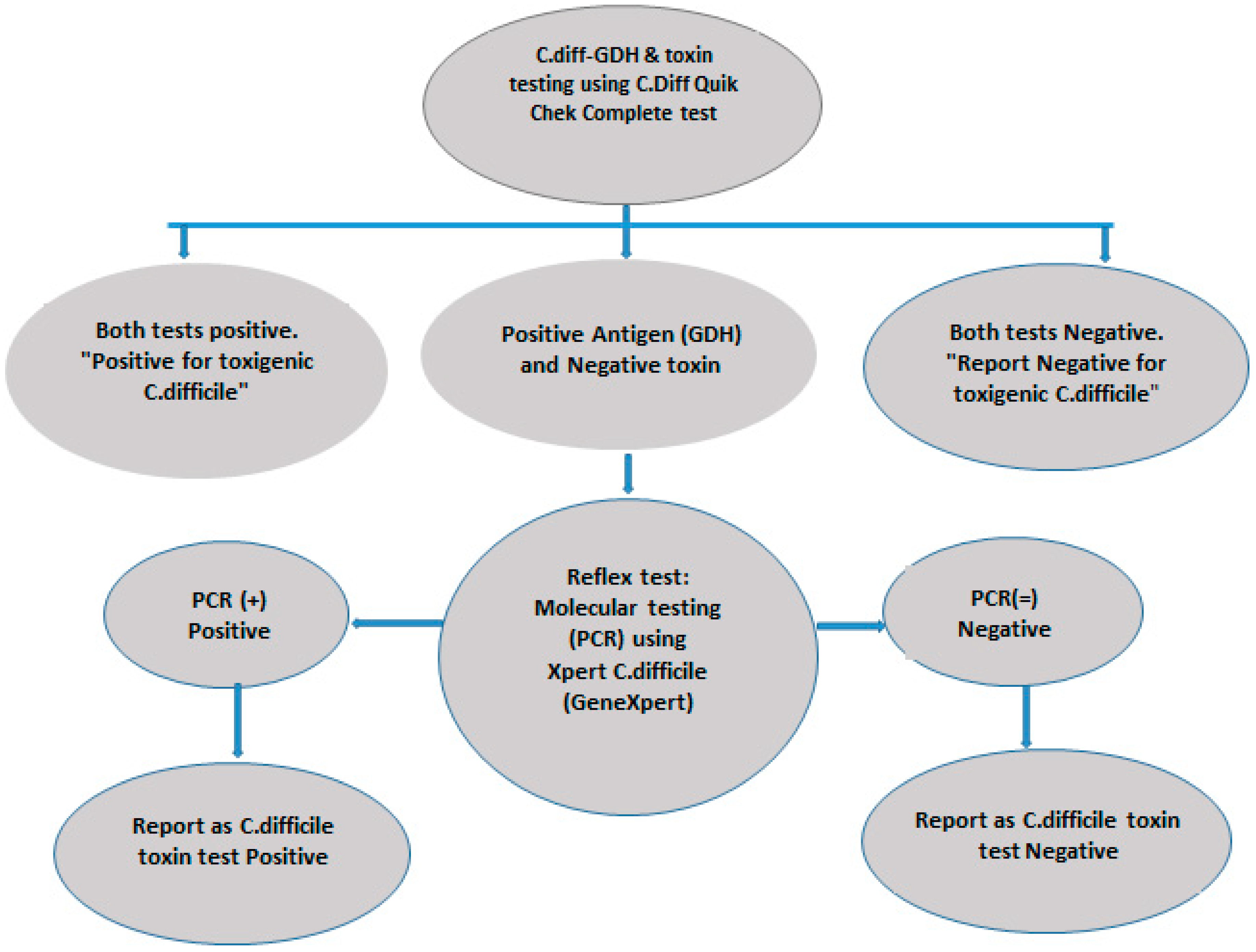
2.2. C. difficile Antigen and Toxin Assays
2.3. Xpert C. difficile PCR Assay
2.4. Data Analysis
3. Results
3.1. Phase 1
3.2. Phase 2
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Polage, C.R.; Solnick, J.V.; Cohen, S.H. Nosocomial Diarrhea: Evaluation and Treatment of Causes Other Than Clostridium difficile. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 55, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Titov, L.; Lebedkova, N.; Shabanov, A.; Tang, Y.J.; Cohen, S.H.; Silva, J. Isolation and Molecular Characterization of Clostridium difficile Strains from Patients and the Hospital Environment in Belarus. J. Clin. Microbiol. 2000, 38, 1200–1202. [Google Scholar] [PubMed]
- Martin, J.S.; Monaghan, T.M.; Wilcox, M.H. Clostridium difficile infection: Epidemiology, diagnosis and understanding transmission. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, E.C., IV; Oldfield, E.C., III; Johnson, D.A. Clinical update for the diagnosis and treatment of Clostridium difficile infection. World J. Gastrointest. Pharmacol. Ther. 2014, 5, 1–26. [Google Scholar] [PubMed]
- Tonna, I.; Welsby, P.D. Pathogenesis and treatment of Clostridium difficile infection. Postgrad. Med. J. 2005, 81, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Sayedy, L.; Kothari, D.; Richards, R.J. Toxic megacolon associated Clostridium difficile colitis. World J. Gastrointest. Endosc. 2010, 2, 293–297. [Google Scholar] [CrossRef]
- Swindells, J.; Brenwald, N.; Reading, N.; Oppenheim, B. Evaluation of diagnostic tests for Clostridium difficile infection. J. Clin. Microbiol. 2010, 48, 606–608. [Google Scholar] [CrossRef]
- Cohen, S.H.; Gerding, D.N.; Johnson, S.; Kelly, C.P.; Loo, V.G.; McDonald, L.C.; Pepin, J.; Wilcox, M.H. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America [SHEA] and the infectious diseases society of America [IDSA]. Infect. Control Hosp. Epidemiol. 2010, 31, 431–455. [Google Scholar] [CrossRef]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America [IDSA] and Society for Healthcare Epidemiology of America [SHEA]. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 66, e1–e48. [Google Scholar] [CrossRef]
- Shetty, N.; Wren, M.; Coen, P. The role of glutamate dehydrogenase for the detection of Clostridium difficile in faecal samples: A meta-analysis. J. Hosp. Infect. 2011, 77, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Fenner, L.; Widmer, A.F.; Goy, G.; Rudin, S.; Frei, R. Rapid and reliable diagnostic algorithm for detection of Clostridium difficile. J. Clin. Microbiol. 2008, 46, 328–330. [Google Scholar] [CrossRef] [PubMed]
- Avila, M.B.; Avila, N.P.; Dupont, A.W. Recent Advances in the Diagnosis and Treatment of Clostridium Difficile Infection. F1000Research 2016, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umscheid, C.A.; Mitchell, M.D.; Doshi, J.A.; Agarwal, R.; Williams, K.; Brennan, P.J. Estimating the Proportion of Healthcare-Associated Infections That Are Reasonably Preventable and the Related Mortality and Costs. Infect. Control Hosp. Epidemiol. 2015, 32, 101–114. [Google Scholar] [CrossRef] [PubMed]
- McGlone, S.M.; Bailey, R.R.; Zimmer, S.M.; Popovich, M.J.; Tian, Y.; Ufberg, P.; Muder, R.R.; Lee, B.Y. The economic burden of Clostridium difficile. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2012, 18, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Vindigni, S.M.; Surawicz, C.M. C. difficile Infection: Changing Epidemiology and Management Paradigms. Clin. Trans. Gastroenterol. 2015, 6, e99. [Google Scholar] [CrossRef] [PubMed]
- Carroll, K.C. Tests for the diagnosis of Clostridium difficile infection: The next generation. Anaerobe 2011, 17, 170–174. [Google Scholar] [CrossRef]
- Kufelnicka, A.M.; Kirn, T.J. Effective utilization of evolving methods for the laboratory diagnosis of Clostridium difficile infection. Clin. Infect. Dis. 2011, 52, 1451–1457. [Google Scholar] [CrossRef]
- Culbreath, K.; Ager, E.; Nemeyer, R.J.; Kerr, A.; Gilligan, P.H. Evolution of testing algorithms at a university hospital for detection of Clostridium difficile infections. J. Clin. Microbiol. 2012, 50, 3073–3076. [Google Scholar] [CrossRef]
- Qutub, M.O.; AlBaz, N.; Hawken, P.; Anoos, A. Comparison between the two-step and the three-step algorithms for the detection of toxigenic Clostridium difficile. Indian J. Med. Microbiol. 2011, 29, 293–296. [Google Scholar] [CrossRef]
- Khanna, S.; Pardi, D.S. The growing incidence and severity of Clostridium difficile infection in inpatient and outpatient settings. Expert Rev. Gastroenterol. Hepatol. 2010, 4, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Kato, N.; Watanabe, K.; Iwai, N.; Nakamura, H.; Yamamoto, T.; Suzuki, K.; Kim, S.M.; Chong, Y.; Wasito, E.B. Identification of toxin A-negative, toxin B-positive Clostridium difficile by PCR. J. Clin. Microbiol. 1998, 36, 2178–2182. [Google Scholar] [PubMed]
- Quinn, C.D.; Sefers, S.E.; Babiker, W.; He, Y.; Alcabasa, R.; Stratton, C.W.; Carroll, K.C.; Tang, Y.W. C. Diff Quik Chek Complete Enzyme Immunoassay Provides a Reliable First-Line Method for Detection of Clostridium difficile in Stool Specimens. J. Clin. Microbiol. 2010, 48, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Sharp, S.E.; Ruden, L.O.; Pohl, J.C.; Hatcher, P.A.; Jayne, L.M.; Ivie, W.M. Evaluation of the C.Diff Quik Chek Complete Assay, a New Glutamate Dehydrogenase and A/B Toxin Combination Lateral Flow Assay for Use in Rapid, Simple Diagnosis of Clostridium difficile Disease. J. Clin. Microbiol. 2010, 48, 2082–2086. [Google Scholar] [CrossRef] [PubMed]
- Luna, R.A.; Boyanton, B.L.; Mehta, S.; Courtney, E.M.; Webb, C.R.; Revell, P.A.; Versalovic, J. Rapid Stool-Based Diagnosis of Clostridium difficile Infection by Real-Time PCR in a Children’s Hospital. J. Clin. Microbiol. 2011, 49, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.Y.; Jeong, J.H.; Kim, K.H.; Ahn, J.Y.; Park, P.W.; Seo, Y.H. Laboratory diagnosis of Clostridium difficile infection: Comparison of Techlab C. diff Quik Chek Complete, Xpert C. difficile, and multistep algorithmic approach. J. Clin. Lab. Anal. 2017, 31, e22135. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.S.; Lee, M. Evaluation of the performance of C. DIFF QUIK CHEK COMPLETE and its usefulness in a hospital setting with a high prevalence of Clostridium difficile infection. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2017, 65, 88–92. [Google Scholar]
- Martínez-Meléndez, A.; Camacho-Ortiz, A.; Morfin-Otero, R.; Maldonado-Garza, H.J.; Villarreal-Treviño, L.; Garza-González, E. Current knowledge on the laboratory diagnosis of Clostridium difficile infection. World J. Gastroenterol. 2017, 23, 1552–1567. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Xpert C. difficile PCR | Sensitivity | Specificity | PPV | NPV | |||
|---|---|---|---|---|---|---|---|
| Positive | Negative | % | % | % | % | ||
| Quik Chek | Positive | 7 | 0 | ||||
| 46.7 | 100 | 100 | 91.7 | ||||
| Complete EIA | Negative | 8 * | 88 | ||||
| 95% Confidence interval | (21.3–73.4%) | (95.9–100%) | 100% | (87.3–94.6%) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qutub, M.; Govindan, P.; Vattappillil, A. Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia. Med. Sci. 2019, 7, 6. https://doi.org/10.3390/medsci7010006
Qutub M, Govindan P, Vattappillil A. Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia. Medical Sciences. 2019; 7(1):6. https://doi.org/10.3390/medsci7010006
Chicago/Turabian StyleQutub, Mohammed, Prasanth Govindan, and Anupama Vattappillil. 2019. "Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia" Medical Sciences 7, no. 1: 6. https://doi.org/10.3390/medsci7010006
APA StyleQutub, M., Govindan, P., & Vattappillil, A. (2019). Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia. Medical Sciences, 7(1), 6. https://doi.org/10.3390/medsci7010006