Feasibility of Telephone Follow-Up after Critical Care Discharge


 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Procedure
2.3. Data Collection
2.4. Study Measures
2.4.1. Health-Related Quality of Life (HRQoL)
2.4.2. Frailty
2.4.3. Other Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vijayaraghavan, B.K.T.; Willaert, X.; Cuthbertson, B.H. Should ICU clinicians follow patients after ICU discharge? No. Intensive Care Med. 2018, 1542–1544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, A.; Tehranchi, K.M.; Needham, D.M. Critical care rehabilitation trials: The importance of ‘usual care’. Crit. Care 2013, 17, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herridge, M.S.; Cheung, A.M.; Tansey, C.M.; Matte-Martyn, A.; Diaz-Granados, N.; Al-Saidi, F.; Cooper, A.B.; Guest, C.B.; Mazer, C.D.; Mehta, S.; et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N. Engl. J. Med. 2003, 348, 683–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Needham, D.M.; Davidson, J.; Cohen, H.; Hopkins, R.O.; Weinert, C.; Wunsch, H.; Zawistowski, C.; Bemis-Dougherty, A.; Berney, S.C.; Bienvenu, O.J.; et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care Med. 2012, 40, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Pandharipande, P.P.; Girard, T.D.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Pun, B.T.; Brummel, N.E.; Hughes, C.G.; Vasilevskis, E.E.; Shintani, A.K.; et al. Long-term cognitive impairment after critical illness. N. Engl. J. Med. 2013, 369, 1306–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herridge, M.S. The challenge of designing a post-critical illness rehabilitation intervention. Crit. Care 2011, 15, 1002. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, J.; Fortune, G.; Barber, V.; Young, J.D. The prevalence of post traumatic stress disorder in survivors of ICU treatment: A systematic review. Intensive Care Med. 2007, 33, 1506–1518. [Google Scholar] [CrossRef]
- Hill, A.D.; Fowler, R.A.; Pinto, R.; Herridge, M.S.; Cuthbertson, B.H.; Scales, D.C. Long-term outcomes and healthcare utilization following critical illness–a population-based study. Crit. Care 2016, 20, 76. [Google Scholar] [CrossRef] [Green Version]
- Rehabilitation after Critical Illness in Adults NICE Quality Standard 158 2017, 7th Sep. Available online: https://www.nice.org.uk/guidance/qs158 (accessed on 8 September 2019).
- Meyer, J.; Brett, S.J.; Waldmann, C. Should ICU clinicians follow patients after ICU discharge? Yes. Intensive Care Med. 2018, 44, 1539–1541. [Google Scholar] [CrossRef] [Green Version]
- Walker, W.; Wright, J.; Danjoux, G.; Howell, S.J.; Martin, D.; Bonner, S. Project Post Intensive Care exercise (PIX): A qualitative exploration of intensive care unit survivors’ perceptions of quality of life post-discharge and experience of exercise rehabilitation. J. Intensive Care Soc. 2015, 16, 37–44. [Google Scholar]
- Ramsay, P.; Huby, G.; Merriweather, J.; Salisbury, L.; Rattray, J.; Grifth, D.; Walsh, T. Patient and carer experience of hospital based rehabilitation from intensive care to hospital discharge: Mixed methods process evaluation of the RECOVER randomised clinical trial. BMJ Open 2016, 6, e012041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.; Sherbourne, C. The MOS 36-Item Short-Form Health Survey (SF-36). Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 30, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Howlett, S.E.; MacKnight, C.; Beattie, B.L.; Bergman, H.; Hébert, R.; Hogan, D.B.; Wolfson, C.; McDowell, I. Prevalence, attributes, and outcomes of fitness and frailty in community-dwelling older adults: Report from the Canadian study of health and aging. J. Gerontol. A. Biol. Sci. Med. Sci. 2004, 59, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- McDermid, R.C.; Stelfox, H.T.; Bagshaw, S.M. Frailty in the critically ill: A novel concept. Crit. Care 2011, 15, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onerup, A.; Angerås, U.; Bock, D.; Börjesson, M.; Fagevik Olsen, M.; Gellerstedt, M.; Haglind, E.; Nilsson, H.; Angenete, E. The preoperative level of physical activity is associated to the postoperative recovery after elective cholecystectomy–A cohort study. Int. J. Surg. 2015, 19, 35–41. [Google Scholar] [CrossRef]
- Ware, K.E.; Snow, K.K.; Kosinski, M. SF-36 Health Survey: Manual and Interpretation Guide; Health Institute, New England Medical Center: Boston, MA, USA, 1993. [Google Scholar]
- Jenkinson, C.; Coulter, A.; Wright, A. Short-form 36 (SF-36) health survey questionnaire: Normative data for adults of working age. Br. Med. J. 1993, 29, 1437–1440. [Google Scholar] [CrossRef] [Green Version]
- Audureau, E.; Rican, S.; Coste, J. Worsening trends and increasing disparities in health-related quality of life: Evidence from two French population-based cross-sectional surveys, 1995–2003. Qual. Life Res. 2013, 22, 13–26. [Google Scholar] [CrossRef]
- Ribu, L.; Hanestad, B.R.; Moum, T.; Birkeland, K.; Rustoen, T. A comparison of the health- related quality of life in patients with diabetic foot ulcers, with a diabetes group and a nondiabetes group from the general population. Qual. Life Res. 2007, 16, 179–189. [Google Scholar] [CrossRef]
- Underwood, S.; Campbell, S.; Deasy, C. Telephone Follow-Up of Mild Traumatic Brain Injury; A Feasibility Study. Ir. Med. J. 2019, 112, 984. [Google Scholar]
- Ma, O.J.; Tanski, M.; Burns, B.; Spizman, E.F.; Heilman, J.A. Development and implementation of an emergency department telephone follow-up system. J. Healthc. Risk Manag. 2017, 37, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Myhren, H.; Ekeberg, Ø.; Stokland, O. Health-related quality of life and return to work after critical illness in general intensive care unit patients: A 1-year follow-up study. Crit. Care Med. 2010, 38, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, J.; Hatch, R.A.; Bishop, J.; Morgan, K.; Jenkinson, C.; Cuthbertson, B.H.; Brett, S.J. An exploration of social and economic outcome and associated health-related quality of life after critical illness in general intensive care unit survivors: A 12-month follow-up study. Crit. Care 2013, 28, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuthbertson, B.H.; Rattray, J.; Campbell, M.K.; Gager, M.; Roughton, S.; Smith, A.; Hull, A.; Breeman, S.; Norrie, J.; Jenkinson, D.; et al. The PRaCTICaL study of nurse led, intensive care follow-up programmes for improving long term outcomes from critical illness: A pragmatic randomised controlled trial. BMJ 2009, 339, b3723. [Google Scholar] [CrossRef] [Green Version]
- Walsh, T.S.; Salisbury, L.G.; Merriweather, J.L.; Boyd, J.A.; Grifth, D.M.; Huby, G.; Elliott, D.; McKinley, S.; Alison, J.; Aitken, L.M.; et al. Increased hospital-based physical rehabilitation and information provision after intensive care unit discharge, the recover randomized clinical trial. JAMA Intern. Med. 2015, 175, 901–910. [Google Scholar] [CrossRef]
- Elliott, D.; McKinley, S.; Alison, J.; Aitken, L.M.; King, M.; Leslie, G.D.; Kenny, P.; Taylor, P.; Foley, R.; Burmeister, E. Health related quality of life and physical recovery after critical illness: A multicentre randomised controlled trial of a home-based physical rehabilitation program. Crit. Care 2011, 15, R142. [Google Scholar] [CrossRef] [Green Version]
- Jensen, J.F.; Egerod, I.; Bestle, M.H.; Christensen, D.F.; Elklit, A.; Hansen, R.L.; Knudsen, H.; Grode, L.B.; Overgaard, D. A recovery program to improve quality of life, sense of coherence and psychological health in ICU survivors: A multicentre randomized controlled trial, the RAPIT study. Intensive Care Med. 2016, 42, 1733–1743. [Google Scholar] [CrossRef]
- Morris, P.E.; Berry, M.J.; Files, C.; Thompson, C.; Hauser, J.; Flores, L.; Dhar, S.; Chmelo, E.; Lovato, J.; Case, D.; et al. Standardized rehabilitation and hospital length of stay among patients with acute respiratory failure: A randomized clinical trial. JAMA 2016, 315, 2694–2702. [Google Scholar] [CrossRef]
- Moss, M.; Nordon-Croft, A.; Malone, D.; Van Pelt, D.; Frankel, S.K.; Warner, M.L. A randomized trial of an intensive physical therapy program for patients with acute respiratory failure. Am. J. Respir. Crit. Care Med. 2016, 193, 1101–1110. [Google Scholar] [CrossRef] [Green Version]
- Bahr, S.J.; Solverson, S.; Schlidt, A.; Hack, D.; Smith, J.L.; Ryan, P. Integrated literature review of postdischarge telephone calls. West. J. Nurs. Res. 2014, 36, 84–104. [Google Scholar] [CrossRef]
- Mistiaen, P.; Poot, E. Telephone follow-up, initiated by a hospital-based health professional, for postdischarge problems in patients discharged from hospital to home. Cochrane Database Syst. Rev 2006, CD004510. [Google Scholar] [CrossRef] [PubMed]
- Braun, E.; Baidusi, A.; Alroy, G.; Azzam, Z.S. Telephone follow-up improves patients satisfaction following hospital discharge. Eur. J. Intern. Med. 2009, 20, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, P.; Pipitone, O.; Franklin, A.; Jackson, D.R.; Moore, E.A.; Dubuque, C.R.; Peralta, C.A.; De Mory, A.C. A Virtual Multidisciplinary Care Program for Management of Advanced Chronic Kidney Disease: Matched Cohort Study. J. Med. Internet Res. 2020, 12, e17194. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
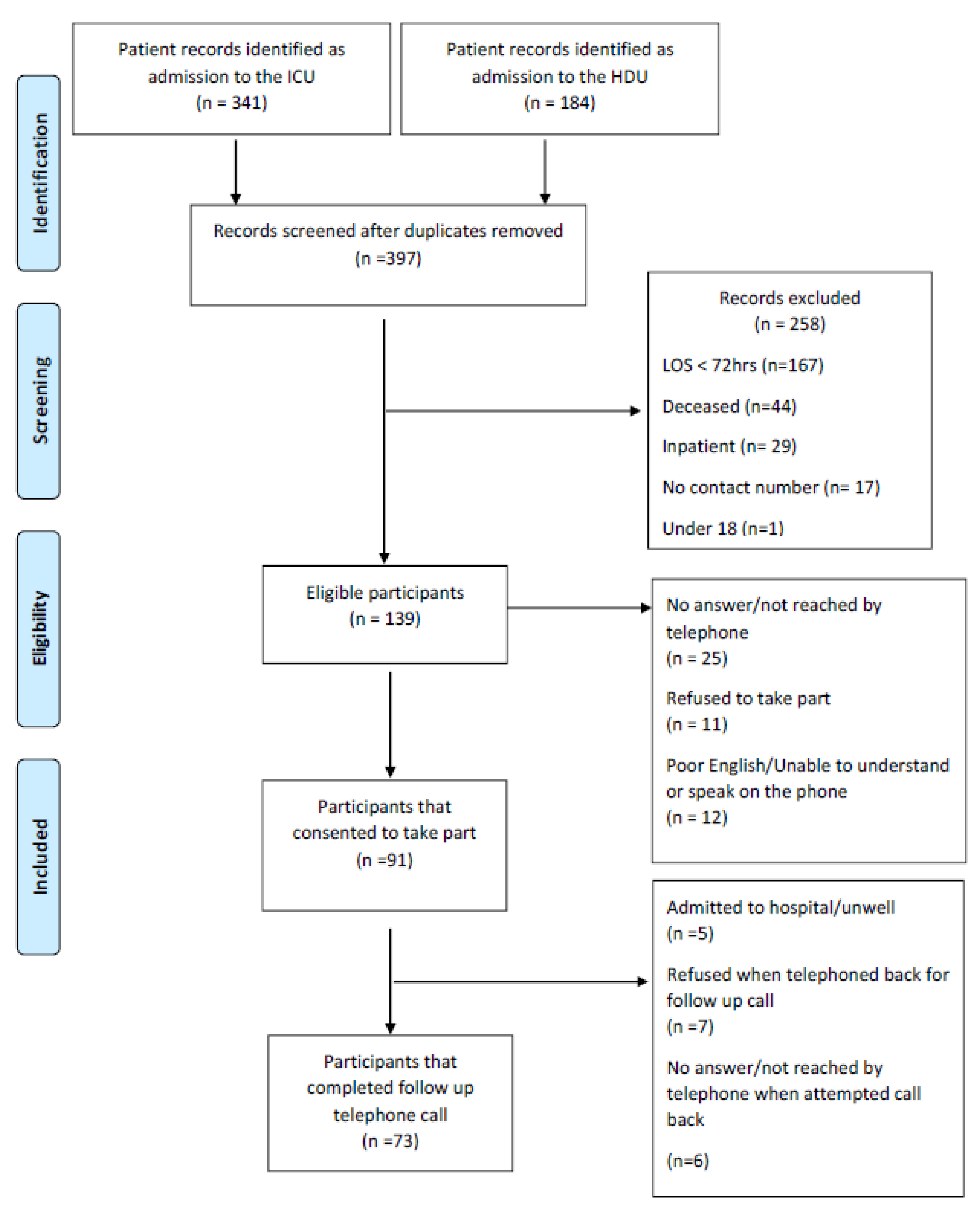
| Variable | n = 73 |
|---|---|
| Female, n (%) | 33 (45) |
| Age, mean years (SD) | 61.7 (15.7) |
| LOS critical care, mean days (SD) | 8 (5.5) |
| LOS hospital, mean days (SD) | 34 (24.4) |
| Reason for admission to critical care, n (%) | |
| Post-operative follow-up | 34 (47) |
| Respiratory-related complications sepsis, MOF | 24 (33) |
| Kidney-related complications | 6 (8) |
| Trauma, epilepsy, other | 9 (12) |
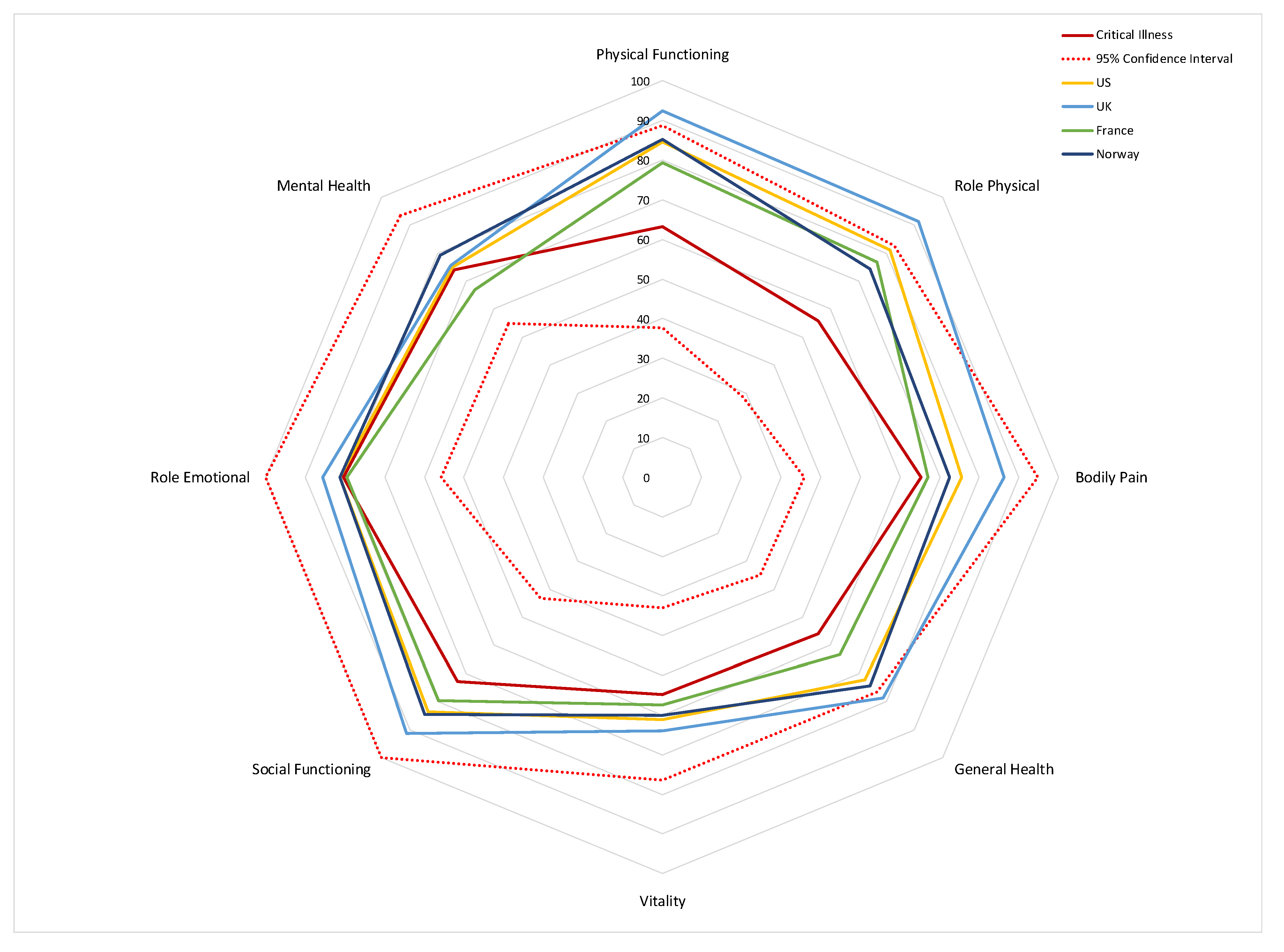
| Domain | n = 71 |
|---|---|
| Physical functioning | 63.3 (25.5) |
| Role physical | 55.7 (27.0) |
| General health | 55.8 (20.9) |
| Vitality | 54.7 (21.8) |
| Social functioning | 72.9 (30.0) |
| Role emotional | 80.4 (24.6) |
| Mental health | 74.1 (19.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hodalova, S.; Moore, S.; Dowds, J.; Murphy, N.; Martin-Loeches, I.; Broderick, J. Feasibility of Telephone Follow-Up after Critical Care Discharge. Med. Sci. 2020, 8, 16. https://doi.org/10.3390/medsci8010016
Hodalova S, Moore S, Dowds J, Murphy N, Martin-Loeches I, Broderick J. Feasibility of Telephone Follow-Up after Critical Care Discharge. Medical Sciences. 2020; 8(1):16. https://doi.org/10.3390/medsci8010016
Chicago/Turabian StyleHodalova, Sofia, Sarah Moore, Joanne Dowds, Niamh Murphy, Ignacio Martin-Loeches, and Julie Broderick. 2020. "Feasibility of Telephone Follow-Up after Critical Care Discharge" Medical Sciences 8, no. 1: 16. https://doi.org/10.3390/medsci8010016
APA StyleHodalova, S., Moore, S., Dowds, J., Murphy, N., Martin-Loeches, I., & Broderick, J. (2020). Feasibility of Telephone Follow-Up after Critical Care Discharge. Medical Sciences, 8(1), 16. https://doi.org/10.3390/medsci8010016