
Misleading HbA1c Measurement in Diabetic Patients with Hemoglobin Variants


Abstract
:1. Introduction
2. Materials and Methods
2.1. Blood Samples
2.2. Hemoglobin A1c Analyses
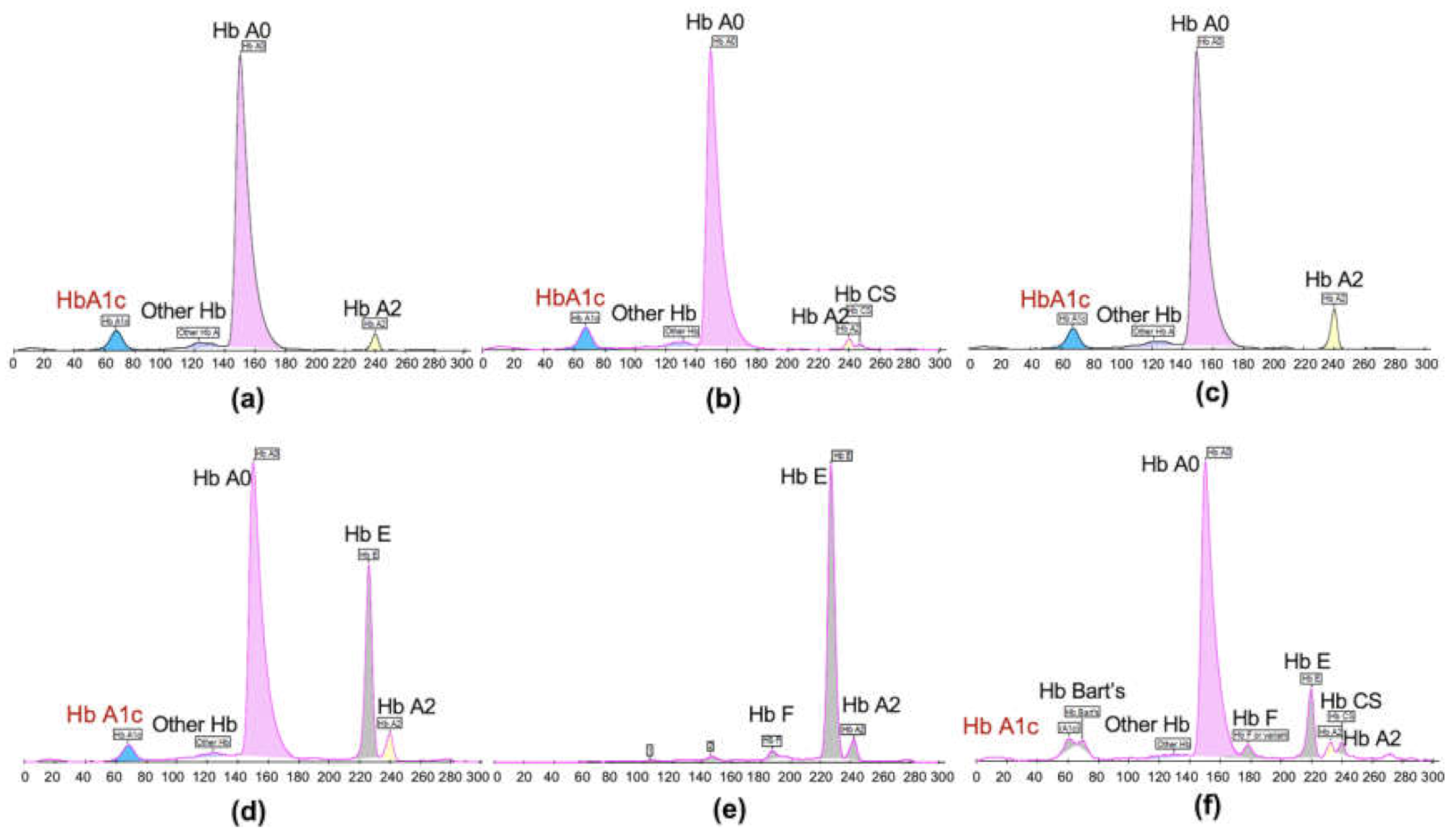
2.3. Hemoglobin Typing
2.4. Plasma Glucose and Estimated Average Glucose Analyses
2.5. Statistical Analysis
3. Results
3.1. Prevalence of Hemoglobin Variants among Patients with Diabetes
3.2. HbA1c Levels of Patients with Hemoglobinopathies
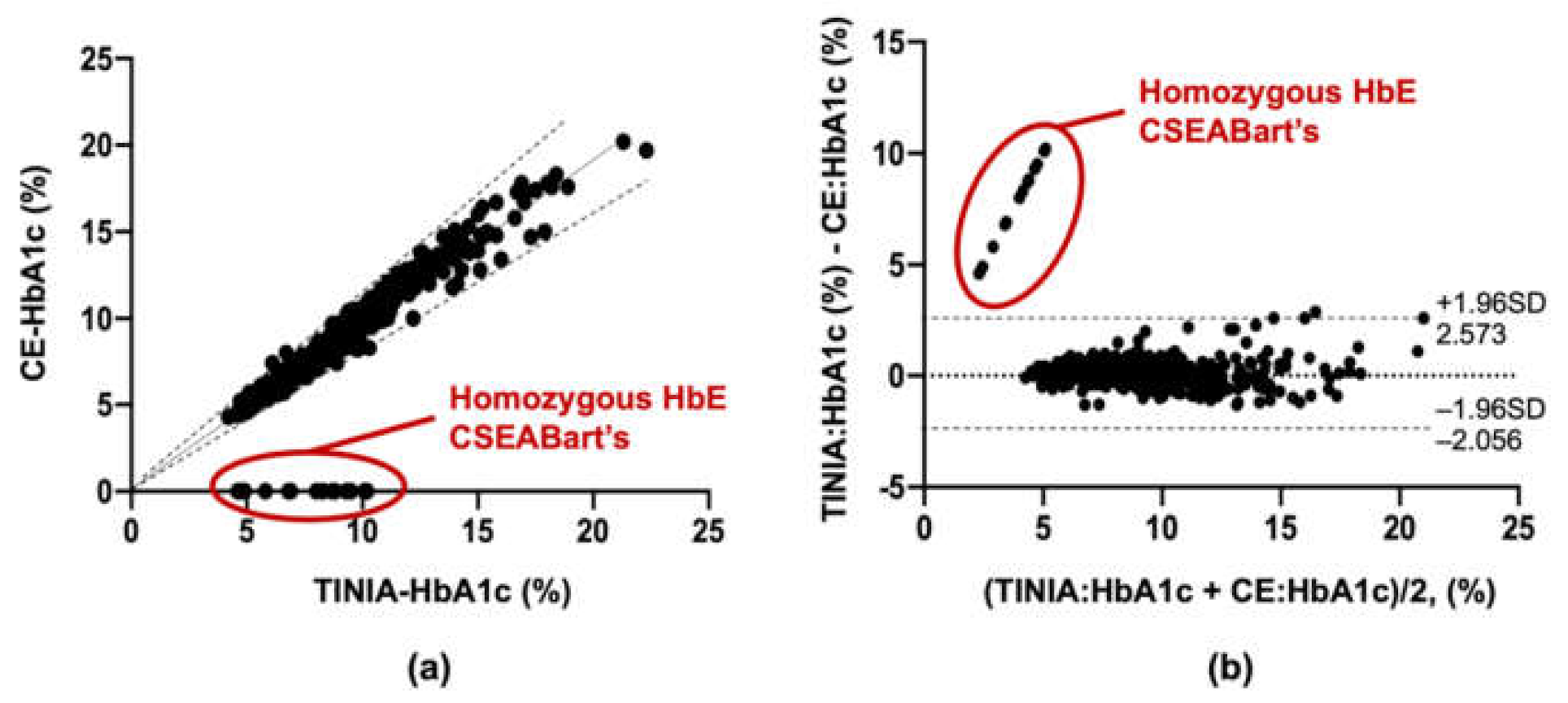
3.3. Comparison of HbA1c Levels Measured by Two Methods
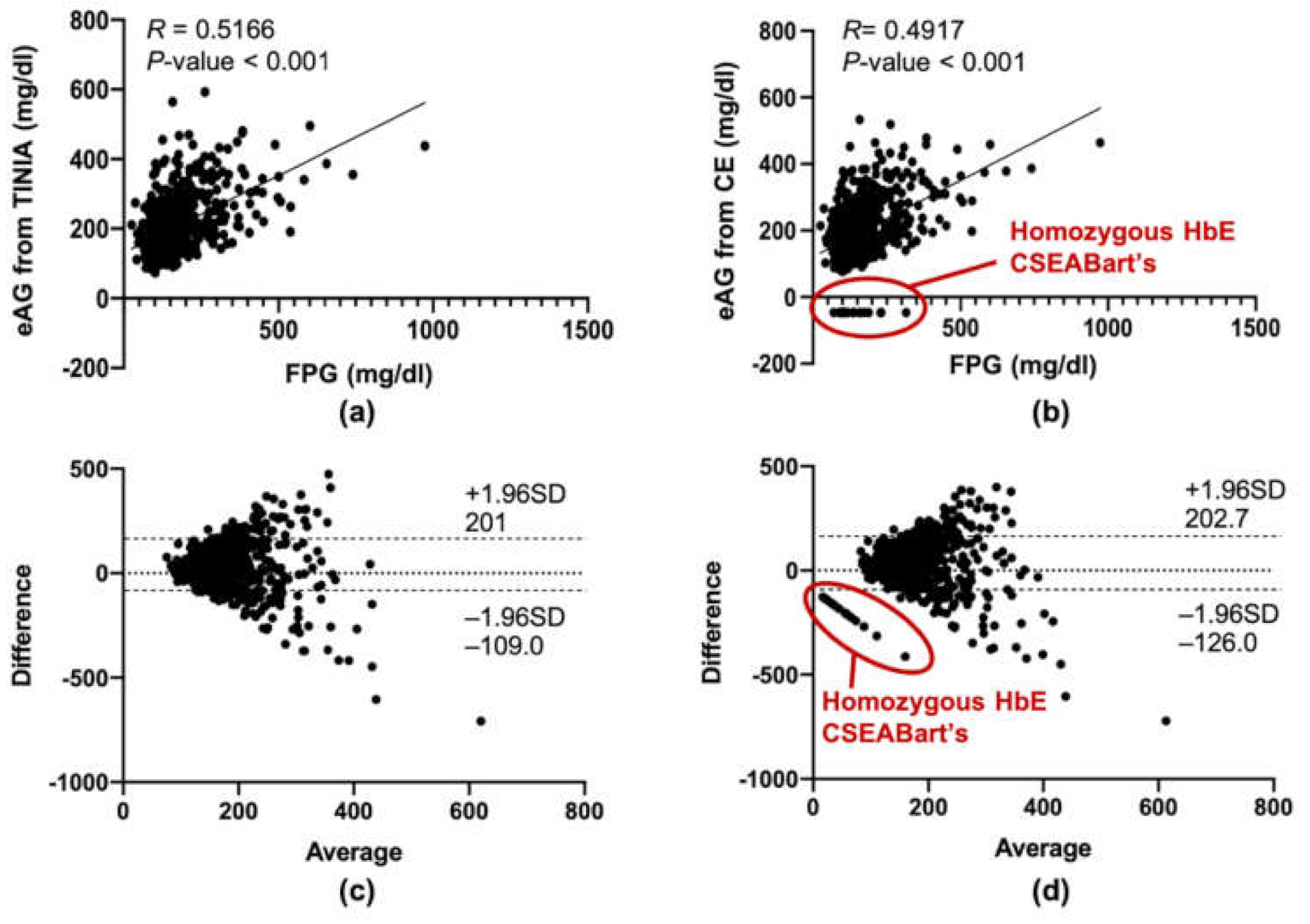
3.4. Effects of Hemoglobinopathy on Estimated Average Plasma Glucose and Fasting Blood Sugar
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes, A. Standards of medical care in diabetes--2008. Diabetes Care 2008, 31, 12–54. [Google Scholar] [CrossRef] [Green Version]
- Weykamp, C.; John, W.G.; Mosca, A. A review of the challenge in measuring hemoglobin A1c. J. Diabetes Sci. Technol. 2009, 3, 439–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weykamp, C. HbA1c: A review of analytical and clinical aspects. Ann. Lab. Med. 2013, 33, 393–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnedl, W.J.; Liebminger, A.; Roller, R.E.; Lipp, R.W.; Krejs, G.J. Hemoglobin variants and determination of glycated hemoglobin (HbA1c). Diabetes Metab. Res. Rev. 2001, 17, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Sacks, D.B. Hemoglobin variants and hemoglobin A1c analysis: Problem solved? Clin. Chem. 2003, 49, 1245–1247. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.L.; Safar-Pour, S.; De, B.K.; Rohlfing, C.L.; Weykamp, C.W.; Little, R.R. Effects of hemoglobin C and S traits on glycohemoglobin measurements by eleven methods. Clin. Chem. 2005, 51, 776–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratumvinit, B.; Reesukumal, K.; Hanyongyuth, S.; Wangchaijaroenkit, S.; Pooliam, J.; Kost, G.J.; Kamkang, P.; Loh, T.P. Hemoglobin A1c levels are slightly but significantly lower in normoglycemic subjects with the hemoglobin E phenotype. Ann. Lab. Med. 2019, 39, 209–213. [Google Scholar] [CrossRef] [Green Version]
- Kweka, B.; Lyimo, E.; Jeremiah, K.; Filteau, S.; Rehman, A.M.; Friis, H.; Manjurano, A.; Faurholt-Jepsen, D.; Krogh-Madsen, R.; PrayGod, G.; et al. Influence of hemoglobinopathies and glucose-6-phosphate dehydrogenase deficiency on diagnosis of diabetes by HbA1c among Tanzanian adults with and without HIV: A cross-sectional study. PLoS ONE 2020, 15, e0244782. [Google Scholar] [CrossRef]
- Williams, T.N.; Weatherall, D.J. World distribution, population genetics, and health burden of the hemoglobinopathies. Cold Spring Harb. Perspect. Med. 2012, 2, a011692. [Google Scholar] [CrossRef] [Green Version]
- Bunthupanich, R.; Karnpean, R.; Pinyachat, A.; Jiambunsri, N.; Prakobkaew, N.; Pakdee, N.; Fucharoen, S.; Fcharoen, S. Micromapping of thalassemia and hemoglobinopathies among Laos, Khmer, Suay and Yer ethnic groups residing in lower northeastern Thailand. Hemoglobin 2020, 44, 3–162. [Google Scholar] [CrossRef]
- Fucharoen, S.; Winichagoon, P. Thalassemia and abnormal hemoglobin. Int. J. Hematol. 2002, 76 (Suppl. 2), 83–89. [Google Scholar] [CrossRef]
- Goh, L.P.W.; Chong, E.T.J.; Lee, P.C. Prevalence of Alpha(α)-Thalassemia in Southeast Asia (2010–2020): A Meta-Analysis Involving 83,674 Subjects. Int. J. Environ. Res. Public Health 2020, 17, 7354. [Google Scholar] [CrossRef] [PubMed]
- Kattamis, A.; Forni, G.L.; Aydinok, Y.; Viprakasit, V. Changing patterns in the epidemiology of β-thalassemia. Eur. J. Haematol. 2020, 105, 692–703. [Google Scholar] [CrossRef]
- Nathan, D.M.; Kuenen, J.; Borg, R.; Zheng, H.; Schoenfeld, D.; Heine, R.J.; for the A1c-Derived Average Glucose (ADAG) Study Group. Translating the A1C assay into estimated average glucose values. Diabetes Care 2008, 31, 1473–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, R.R.; La’ulu, S.L.; Hanson, S.E.; Rohlfing, C.L.; Schmidt, R.L. Effects of 49 different rare Hb variants on HbA1c measurement in eight methods. J. Diabetes Sci. Technol. 2015, 9, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Sae-ung, N.; Fucharoen, G.; Sanchaisuriya, K.; Fucharoen, S. Alpha (0)-thalassemia and related disorders in northeast Thailand: A molecular and hematological characterization. Acta Haematol. 2007, 117, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Fucharoen, G.; Sanchaisuriya, K.; Sae-ung, N.; Dangwibul, S.; Fucharoen, S. A simplified screening strategy for thalassaemia and haemoglobin E in rural communities in south-east Asia. Bull. World Health Organ. 2004, 82, 364–372. [Google Scholar] [PubMed]
- Weykamp, C.; Waenink-Wieggers, H.; Kemna, E.; Siebelder, C. HbA1c: Performance of the Sebia Capillarys 2 Flex Piercing. Clin. Chem Lab. Med. 2013, 51, e129–e131. [Google Scholar] [CrossRef]
- Dessi, M.; Pieri, M.; Pignalosa, S.; Martino, F.G.; Zenobi, R. Performances of capillary electrophoresis and HPLC methods in HbA1c determination: Diagnostic accuracy in HbS and HbD-Iran variants’ presence. J. Clin. Lab. Anal. 2015, 29, 57–60. [Google Scholar] [CrossRef]
- Wong, S.C.; Aw, T.C. HbE1c as an indicator for the presence of Hb AE phenotype in diabetic patients. Clin. Chem. 1998, 44, 660–662. [Google Scholar] [CrossRef]
- Singer, S.T.; Olivieri, N.E.; Sweeters, N.; Rodwell, C.; Oliver, C.; Vichinsky, E.P.; Kuypers, F.A. Biotin-labeled RBC survival in thalassemia and impact of treatment. Blood 2004, 104, 3616–3616. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Hemoglobin Typing | N | Prevalence (%) | FPG (mg/dL) | HbA1c (%) | ||
|---|---|---|---|---|---|---|
| TINIA | CE | p-Value | ||||
| Normal | ||||||
| A2A | 555 | 65.7 | 154.0 ± 85.55 | 8.62 ± 2.47 | 8.49 ± 2.41 | 0.351 |
| Hemoglobin variants | ||||||
| Heterozygous HbE | 255 | 30.2 | 156.2 ± 87.19 | 8.64 ± 2.75 | 8.57 ± 2.79 | 0.788 |
| Homozygous HbE CSEA Bart’s | 16 2 | 1.9 0.2 | 144.1 ± 62.93 | 7.67 ± 1.98 | Undetectable | - |
| Hb CS trait β-thalassemia trait | 12 5 | 1.4 0.6 | 152.4 ± 45.27 | 7.75 ± 2.89 | 7.81 ± 2.89 | 0.953 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitchai, M.; Suwansaksri, N.; Seanseeha, S.; Saenboonsiri, J.; Kraitree, P.; Piyapromdee, J.; Silsirivanit, A. Misleading HbA1c Measurement in Diabetic Patients with Hemoglobin Variants. Med. Sci. 2021, 9, 43. https://doi.org/10.3390/medsci9020043
Mitchai M, Suwansaksri N, Seanseeha S, Saenboonsiri J, Kraitree P, Piyapromdee J, Silsirivanit A. Misleading HbA1c Measurement in Diabetic Patients with Hemoglobin Variants. Medical Sciences. 2021; 9(2):43. https://doi.org/10.3390/medsci9020043
Chicago/Turabian StyleMitchai, Manthana, Nattakarn Suwansaksri, Suphakdee Seanseeha, Jindamanee Saenboonsiri, Putthichai Kraitree, Jirasak Piyapromdee, and Atit Silsirivanit. 2021. "Misleading HbA1c Measurement in Diabetic Patients with Hemoglobin Variants" Medical Sciences 9, no. 2: 43. https://doi.org/10.3390/medsci9020043
APA StyleMitchai, M., Suwansaksri, N., Seanseeha, S., Saenboonsiri, J., Kraitree, P., Piyapromdee, J., & Silsirivanit, A. (2021). Misleading HbA1c Measurement in Diabetic Patients with Hemoglobin Variants. Medical Sciences, 9(2), 43. https://doi.org/10.3390/medsci9020043