

The Impact of Physical Activity on Depressive Symptoms among Urban and Rural Older Adults: Empirical Study Based on the 2018 CHARLS Database
Abstract
:1. Introduction
1.1. Symptoms of Depression among Older Adults
1.2. Physical Activity and Depressive Symptoms
1.3. The Present Study
2. Materials and Methods
2.1. Data Source
2.2. Variable Selection
2.2.1. Depressive Symptoms
2.2.2. Physical Activity Level
2.2.3. Covariates
2.2.4. Statistical Analysis
3. Results
3.1. Descriptive Characteristics of the Sample
3.2. Factors Influencing the Level of Physical Activity among Older Adults
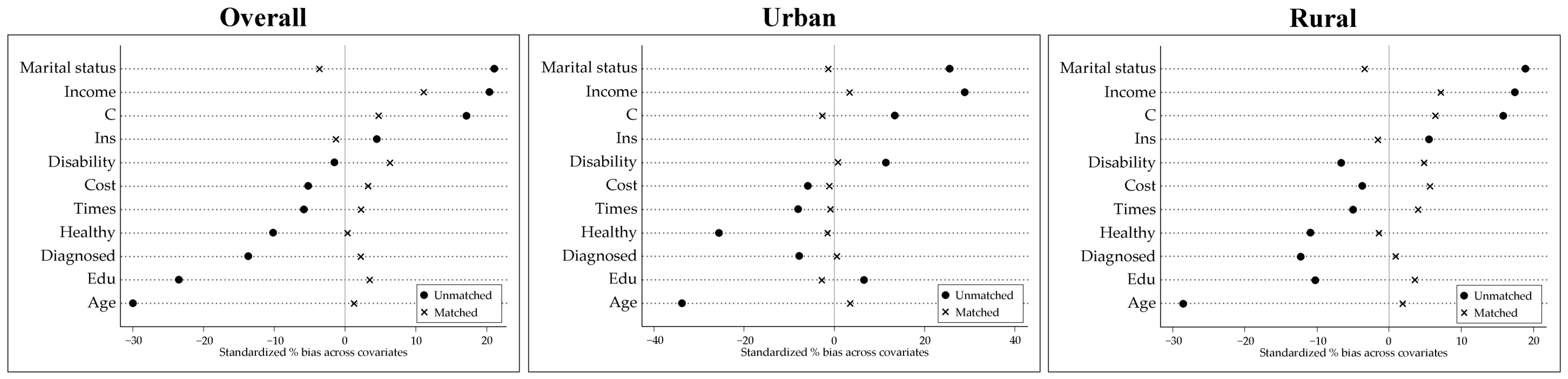
3.3. Equilibrium Test for Propensity Score Matching
3.4. Equilibrium Test for Propensity Score Matching
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seventh National Population Census Bulletin. Available online: https://www.gov.cn/guoqing/2021-05/13/content_5606149.htm (accessed on 29 August 2023).
- CHENG, L.F.; DENG, W. Study on the impact of population aging on social security expenditure in China. East China Econ. Manag. 2022, 1, 1–8. [Google Scholar]
- Tang, B.; Li, Z.; Hu, S.; Xiong, J. Economic Implications of Health Care Burden for Elderly Population. INQUIRY: J. Health Care Organ. Provis. Financ. 2022, 59, 00469580221121511. [Google Scholar] [CrossRef]
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Shao, M.; Chen, J.; Ma, C. Research on the Relationship between Chinese Elderly Health Status, Social Security, and Depression. Int. J. Environ. Res. Public Health 2022, 19, 7496. [Google Scholar] [CrossRef]
- Sun, X.; Zhou, M.; Huang, L.; Nuse, B. Depressive costs: Medical expenditures on depression and depressive symptoms among rural elderly in China. Public Health 2020, 181, 141–150. [Google Scholar] [CrossRef]
- Li, X.; Ge, T.; Dong, Q.; Jiang, Q. Social participation, psychological resilience and depression among widowed older adults in China. BMC Geriatr. 2023, 1, 454. [Google Scholar] [CrossRef]
- Jiang, C.H.; Zhu, F.; Qin, T.T. Relationships between Chronic Diseases and Depression among Middle-aged and Elderly People in China: A Prospective Study from CHARLS. Curr. Med. Sci. 2020, 5, 858–870. [Google Scholar] [CrossRef]
- Schulz, R.; Drayer, R.A.; Rollman, B.L. Depression as a risk factor for non-suicide mortality in the elderly. Biol. Psychiatry 2002, 3, 205–225. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Subramaniam, H. Prognosis of depression in old age compared to middle age: A systematic review of comparative studies. Am. J. Psychiatry 2005, 9, 1588–1601. [Google Scholar] [CrossRef]
- Hua, Y.; Wang, B.; Wallen, G.R.; Shao, P.; Ni, C.; Hua, Q. Health-promoting lifestyles and depression in urban elderly Chinese. PLoS ONE 2015, 3, e0117998. [Google Scholar] [CrossRef]
- Lee, C.T.; Yeh, C.J.; Lee, M.C.; Lin, H.S.; Chen, V.C.; Hsieh, M.H.; Yen, C.H.; Lai, T.J. Leisure activity, mobility limitation and stress as modifiable risk factors for depressive symptoms in the elderly: Results of a national longitudinal study. Arch. Gerontol. Geriatr. 2012, 2, e221-9. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.T.; Liu, C.B.; Tsai, Y.H.; Chin, Y.F.; Wong, C.H. Physical fitness exercise versus cognitive behavior therapy on reducing the depressive symptoms among community-dwelling elderly adults: A randomized controlled trial. Int. J. Nurs. Stud. 2015, 10, 1542–1552. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Barbour, K.A.; Blumenthal, J.A. Exercise training and depression in older adults. Neurobiol. Aging 2005, Suppl. 1, 119–123. [Google Scholar] [CrossRef]
- Marques, A.; Gaspar de Matos, M.; Bordado, J.; Gouveia, É.R.; Peralta, M.; Gomez-Baya, D. Different levels of physical activity and depression symptoms among older adults from 18 countries: A population-based study from the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur. J. Sport Sci. 2021, 6, 887–894. [Google Scholar] [CrossRef]
- Lampinen, P.; Heikkinen, E. Reduced mobility and physical activity as predictors of depressive symptoms among community-dwelling older adults: An eight-year follow-up study. Aging Clin. Exp. Res. 2003, 15, 205–211. [Google Scholar] [CrossRef]
- Zhang, S.; Xiang, K.; Li, S.; Pan, H.F. Physical activity and depression in older adults: The knowns and unknowns. Psychiatry Res. 2021, 297, 113738. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Z.; Fu, C. Urban-rural differences in the association between social activities and depressive symptoms among older adults in China: A cross-sectional study. BMC Geriatr. 2021, 21, 569. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 1, 61–68. [Google Scholar] [CrossRef]
- Yu, D.S.F.; Yan, E.C.W.; Chow, C.K. Interpreting SF-12 mental component score: An investigation of its convergent validity with CESD-10. Qual. Life Res. 2015, 24, 2209–2217. [Google Scholar] [CrossRef]
- Liu, J.; Qiang, F. Psychosocial Mediation of Light-Moderate Physical Activity and Cognitive Performance among Adults Aged 60+ in China. Behav. Sci. 2022, 12, 175. [Google Scholar] [CrossRef]
- Macfarlane, D.; Chan, A.; Cerin, E. Examining the validity and reliability of the Chinese version of the International Physical Activity Questionnaire, long form (IPAQ-LC). Public Health Nutr. 2011, 3, 443–450. [Google Scholar] [CrossRef]
- Austin, P.C.; Jembere, N.; Chiu, M. Propensity score matching and complex surveys. Stat. Methods Med. Res. 2018, 4, 1240–1257. [Google Scholar] [CrossRef]
- Li, L.W.; Liu, J.; Xu, H.; Zhang, Z. Understanding Rural–Urban Differences in Depressive Symptoms Among Older Adults in China. J. Aging Health 2016, 2, 341–362. [Google Scholar] [CrossRef]
- Yuan, L.; Xu, Q.; Gui, J.; Liu, Y.; Lin, F.; Zhao, Z.; Sun, J. Decomposition and comparative analysis of differences in depressive symptoms between urban and rural older adults: Evidence from a national survey. Int. Psychogeriatr. 2023, 1–12. [Google Scholar] [CrossRef]
- Liao, J.; Wang, Q.; Huang, J.L.; Wei, Y.M. Urban-rural difference in the costs of disability and its effects on poverty among people with disabilities in China. Front. Public Health 2022, 10, 989540. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Song, S.; Sullivan, S.; Qiu, J.; Wang, W. Ageing, the urban-rural gap and disability trends: 19 years of experience in China - 1987 to 2006. PLoS ONE 2010, 8, e12129. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chi, I.; Zhang, X.; Cheng, Z.; Zhang, L.; Chen, G. Urban and rural factors associated with life satisfaction among older Chinese adults. Aging Ment. Health 2015, 10, 947–954. [Google Scholar] [CrossRef]
- Jeong, J.A.; Kim, S.A.; Yang, J.H.; Shin, M.H. Urban-Rural Differences in the Prevalence of Depressive Symptoms in Korean Adults. Chonnam Med. J. 2023, 2, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Stickley, A.; Koyanagi, A.; Roberts, B.; McKee, M. Urban-rural differences in psychological distress in nine countries of the former Soviet Union. J. Affect. Disord. 2015, 178, 142–148. [Google Scholar] [CrossRef]
- Vassos, E.; Agerbo, E.; Mors, O.; Pedersen, C.B. Urban-rural differences in incidence rates of psychiatric disorders in Denmark. Br. J. Psychiatry 2016, 208, 435–440. [Google Scholar] [CrossRef]
- Butterworth, P.; Handley, T.E.; Lewin, T.J.; Kelly, B. Psychological distress in rural Australia: Regional variation and the role of family functioning and social support. J. Public Health 2014, 22, 481–488. [Google Scholar] [CrossRef]
- Breslau, J.; Marshall, G.N.; Pincus, H.A.; Brown, R.A. Are mental disorders more common in urban than rural areas of the United States? J. Psychiatr. Res. 2014, 56, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Han, T.; Han, M.; Moreira, P.; Song, H.; Li, P.; Zhang, Z. Association between specific social activities and depressive symptoms among older adults: A study of urban-rural differences in China. Front. Public Health 2023, 11, 1099260. [Google Scholar] [CrossRef]
- Mumba, M.N.; Nacarrow, A.F.; Cody, S.; Key, B.A.; Wang, H.; Robb, M.; Jurczyk, A.; Ford, C.; Kelley, M.A.; Allen, R.S. Intensity and type of physical activity predicts depression in older adults. Aging Ment. Health 2021, 4, 664–671. [Google Scholar] [CrossRef]
- Kong, X.K.; Xiao, Q.L.; Li, J. Urban-rural comparison on the risk factors of geriatric depressive symptoms. Chin. Ment. Health J. 2018, 8, 648–655. [Google Scholar]
- Camacho, T.C.; Roberts, R.E.; Lazarus, N.B.; Kaplan, G.A.; Cohen, R.D. Physical activity and depression: Evidence from the Alameda County Study. Am. J. Epidemiol. 1991, 2, 20–31. [Google Scholar] [CrossRef]
- Worrall, C.; Jongenelis, M.I.; McEvoy, P.M.; Jackson, B.; Newton, R.U.; Pettigrew, S. An Exploratory Study of the Relative Effects of Various Protective Factors on Depressive Symptoms Among Older People. Front. Public Health 2020, 8, 579304. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Xi, J.; Hall, B.J.; Fu, M.; Zhang, B.; Guo, J.; Feng, X. Attitudes toward aging, social support and depression among older adults: Difference by urban and rural areas in China. J. Affect Disord. 2020, 274, 85–92. [Google Scholar] [CrossRef]
- Hussain, B.; Mirza, M.; Baines, R.; Burns, L.; Stevens, S.; Asthana, S.; Chatterjee, A. Loneliness and social networks of older adults in rural communities: A narrative synthesis systematic review. Front. Public Health 2023, 11, 1113864. [Google Scholar] [CrossRef]
- Wang, C.; Liu, Z.; Chen, T.; Wang, J.; Zhang, X.; Han, B. Intergenerational support and depressive symptoms in old age: The difference between urban and rural China. Front. Public Health 2022, 10, 1007408. [Google Scholar] [CrossRef]
- Gu, Y.; Ali, S.H.; Guo, A. Comparing the role of social connectivity with friends and family in depression among older adults in China: Evaluating the moderating effect of urban–rural status. Front. Psychiatry 2023, 14, 1162982. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, W. Does grandchild care intention, intergenerational support have an impact on the health of older adults in China? A quantitative study of CFPS data. Front. Public Health 2023, 11, 1186798. [Google Scholar] [CrossRef]
- Tang, S.; Yang, T.; Ye, C.; Liu, M.; Gong, Y.; Yao, L.; Xu, Y.; Bai, Y.; Tang, S. Research on grandchild care and depression of chinese older adults based on CHARLS2018: The mediating role of intergenerational support from children. BMC Public Health 2022, 22, 137. [Google Scholar] [CrossRef] [PubMed]
- Blomstrand, P.; Tesan, D.; Nylander, E.M.; Ramstrand, N. Mind body exercise improves cognitive function more than aerobic- and resistance exercise in healthy adults aged 55 years and older—An umbrella review. Eur Rev Aging Phys Act 2023, 20, 15. [Google Scholar] [CrossRef]
- Smith, P.J.; Merwin, R.M. The role of exercise in management of mental health disorders: An integrative review. Annu. Rev. Med. 2021, 72, 45–62. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Fang, H.; Leng, W.; Li, J.; Chang, J. Effect of Aerobic Exercise on Mental Health in Older Adults: A Meta-Analysis of Randomized Controlled Trials. Front. Psychiatry 2021, 12, 748257. [Google Scholar] [CrossRef]
- Chen, Z.; Wu, Z.; Zheng, S.; Liu, C.; Wu, Q.; Li, S. Effect of exercise interventions on the depression of older adults. A meta-analysis. Int. J. Sport Psychol. 2022, 53, 543–568. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Variable Description | Overall | Urban | Rural |
|---|---|---|---|---|
| Sample size | n | 5055 | 1582 | 3473 |
| Gender | Male | 48.98% | 52.47% | 47.39% |
| Female | 51.02% | 47.53% | 52.61% | |
| Age | Years | 67.55 ± 5.85 | 67.86 ± 6.18 | 67.41 ± 5.68 |
| Exercise | mins/week | 434.16 ± 364.20 | 483.83 ± 395.12 | 325.10 ± 252.70 |
| CESD-10 | Scores | 19.17 ± 5.26 | 18.60 ± 4.52 | 19.43 ± 5.54 |
| Health | Scores | 2.89 ± 1.00 | 2.82 ± 0.94 | 2.93 ± 1.02 |
| Education level | No formal education | 45.52% | 25.47% | 54.65% |
| Elementary school | 23.11% | 22.19% | 23.52% | |
| Middle school | 19.11% | 27.31% | 15.38% | |
| High school | 10.62% | 20.42% | 6.16% | |
| Vocational school and above | 1.64% | 4.61% | 0.29% | |
| Disability | Yes | 13.29% | 11.00% | 14.34% |
| No | 86.71% | 89.00% | 85.66% | |
| Marital status | With spouse | 83.20% | 81.16% | 84.13% |
| Without spouse | 16.80% | 18.84% | 15.87% | |
| Diagnosed | Yes | 43.70% | 47.79% | 41.84% |
| No | 56.30% | 52.21% | 58.16% | |
| Times | <1 time for outpatient treatment/month | 92.68% | 92.04% | 92.97% |
| ≥1 time for outpatient treatment/month | 7.32% | 7.96% | 7.04% | |
| Cost | ln(spent for outpatient treatment/month) | 0.45 ± 1.63 | 0.51 ± 1.78 | 0.41 ± 1.55 |
| medical insurance | Yes/medical insurance | 97.65% | 98.55% | 97.24% |
| No/medical insurance | 2.35% | 1.45% | 2.76% | |
| Income | ln(any wage and bonus income/year) | 1.50 ± 3.40 | 1.55 ± 3.45 | 1.27 ± 3.30 |
| Variable Type | Variable | Overall | Urban | Rural |
|---|---|---|---|---|
| Covariates | Disability | 0.0121 | 0.4730 * | −0.0710 |
| (0.0816) | (0.1910) | (0.0879) | ||
| Gender | 0.3620 ** | 0.0627 | 0.4410 ** | |
| (0.0745) | (0.1780) | (0.0827) | ||
| Edu | −0.1950 ** | 0.0048 | −0.2670 ** | |
| (0.0376) | (0.0726) | (0.0445) | ||
| Area | −1.1360** | - | - | |
| (0.0918) | - | - | ||
| Marital status | 0.3540 ** | 0.5010 | 0.3390 ** | |
| (0.1060) | (0.2710) | (0.1160) | ||
| Age | −0.0480 ** | −0.0434 ** | −0.0498 ** | |
| (0.0065) | (0.0155) | (0.0071) | ||
| Healthy | −0.0773 * | −0.2480 ** | −0.0464 | |
| (0.0348) | (0.0830) | (0.0384) | ||
| Diagnosed | −0.1420 | −0.0259 | −0.1640 * | |
| (0.0727) | (0.1750) | (0.0803) | ||
| Times | −0.1340 | −0.2080 | −0.1180 | |
| (0.1130) | (0.2770) | (0.1250) | ||
| Cost | 0.0544 | 0.0655 | 0.0501 | |
| (0.0553) | (0.1230) | (0.0632) | ||
| Ins | 0.3580 | 0.000 | 0.2710 | |
| (0.2330) | - | (0.2410) | ||
| Income | 0.0276 ** | 0.0546 * | 0.0235 * | |
| (0.0100) | (0.0217) | (0.0111) | ||
| Cons | 1.9340 ** | 0.8890 | 2.1050 ** | |
| (0.5260) | (1.0630) | (0.5760) | ||
| Statistical Testing | N | 5055 | 1559 | 3473 |
| R2 | ||||
| AIC | 5230.3 | 1058.6 | 4165.5 |
| Variable | Match | K-NNM (%bias) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Overall | Urban | Rural | Overall | Urban | Rural | ||
| Age | U | −30.0 | −33.7 | −28.5 | 0.000 | 0.710 | 0.650 |
| M | 1.3 | 3.5 | 1.9 | 0.731 | 0.716 | 0.636 | |
| Gender | U | 17.1 | 13.4 | 15.7 | 0.000 | - | - |
| M | 4.7 | −2.6 | 6.4 | 0.238 | 0.810 | 0.140 | |
| Edu | U | −23.5 | 6.4 | −10.2 | 0.000 | 1.020 | 0.930 |
| M | 3.5 | −2.5 | 3.6 | 0.358 | 0.812 | 0.393 | |
| Disability | U | −1.5 | 11.4 | −6.7 | 0.640 | 1.400 | 0.820 |
| M | 6.3 | 0.9 | 4.7 | 0.097 | 0.940 | 0.233 | |
| Marital status | U | 21.0 | 25.5 | 18.9 | 0.000 | - | - |
| M | −3.6 | −1.3 | −3.4 | 0.302 | 0.890 | 0.372 | |
| Healthy | U | −10.2 | −3.1 | −11.0 | 0.002 | 0.890 | 0.900 |
| M | 0.3 | 94.4 | −1.4 | 0.934 | 0.894 | 0.742 | |
| Diagnosed | U | −13.7 | 0.3 | −12.3 | 0.000 | - | - |
| M | 2.2 | 0.1 | 0.9 | 0.578 | 0.951 | 0.835 | |
| Times | U | −5.9 | −8.1 | −5.1 | 0.083 | 0.630 | 0.780 |
| M | 2.3 | −0.8 | 4 | 0.542 | 0.935 | 0.309 | |
| Cost | U | −5.2 | −6.0 | −3.7 | 0.121 | 0.800 | 0.850 |
| M | 3.2 | −1.2 | 5.6 | 0.382 | 0.913 | 0.155 | |
| Ins | U | 4.5 | - | 5.5 | 0.188 | - | - |
| M | −1.3 | - | −1.5 | 0.720 | 1.000 | 0.692 | |
| Income | U | 20.4 | 28.8 | 17.4 | 0.000 | 1.690 | 1.310 |
| M | 11.1 | 3.5 | 7.1 | 0.008 | 0.771 | 0.116 | |
| Matching Method | Overall | Urban | Rural | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Treatment Effect | Standard Error | p-Value | Treatment Effect | Standard Error | p-Value | Treatment Effect | Standard Error | p-Value | |
| K-NNM (k = 4) | −2.415 | 0.078 | 0.004 | −2.012 | 0.069 | 0.045 | −2.477 | 0.007 | 0.055 |
| Caliper Match (caliper = 0.02) | −2.413 | 0.072 | 0.058 | −2.012 | 0.065 | 0.177 | −2.477 | 0.004 | 0.735 |
| Nuclear Match | −2.819 | 0.037 | 0.317 | −2.612 | 0.082 | 0.038 | −2.853 | 0.043 | 0.502 |
| Average Value | −2.549 | −2.212 | −2.602 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, X.; Liu, H.; Niyomsilp, E. The Impact of Physical Activity on Depressive Symptoms among Urban and Rural Older Adults: Empirical Study Based on the 2018 CHARLS Database. Behav. Sci. 2023, 13, 864. https://doi.org/10.3390/bs13100864
Jin X, Liu H, Niyomsilp E. The Impact of Physical Activity on Depressive Symptoms among Urban and Rural Older Adults: Empirical Study Based on the 2018 CHARLS Database. Behavioral Sciences. 2023; 13(10):864. https://doi.org/10.3390/bs13100864
Chicago/Turabian StyleJin, Xueyu, Huasen Liu, and Eksiri Niyomsilp. 2023. "The Impact of Physical Activity on Depressive Symptoms among Urban and Rural Older Adults: Empirical Study Based on the 2018 CHARLS Database" Behavioral Sciences 13, no. 10: 864. https://doi.org/10.3390/bs13100864
APA StyleJin, X., Liu, H., & Niyomsilp, E. (2023). The Impact of Physical Activity on Depressive Symptoms among Urban and Rural Older Adults: Empirical Study Based on the 2018 CHARLS Database. Behavioral Sciences, 13(10), 864. https://doi.org/10.3390/bs13100864