
The Mental Health Impacts of a Pandemic: A Multiaxial Conceptual Model for COVID-19



{kind=link}
Abstract
:1. Introduction
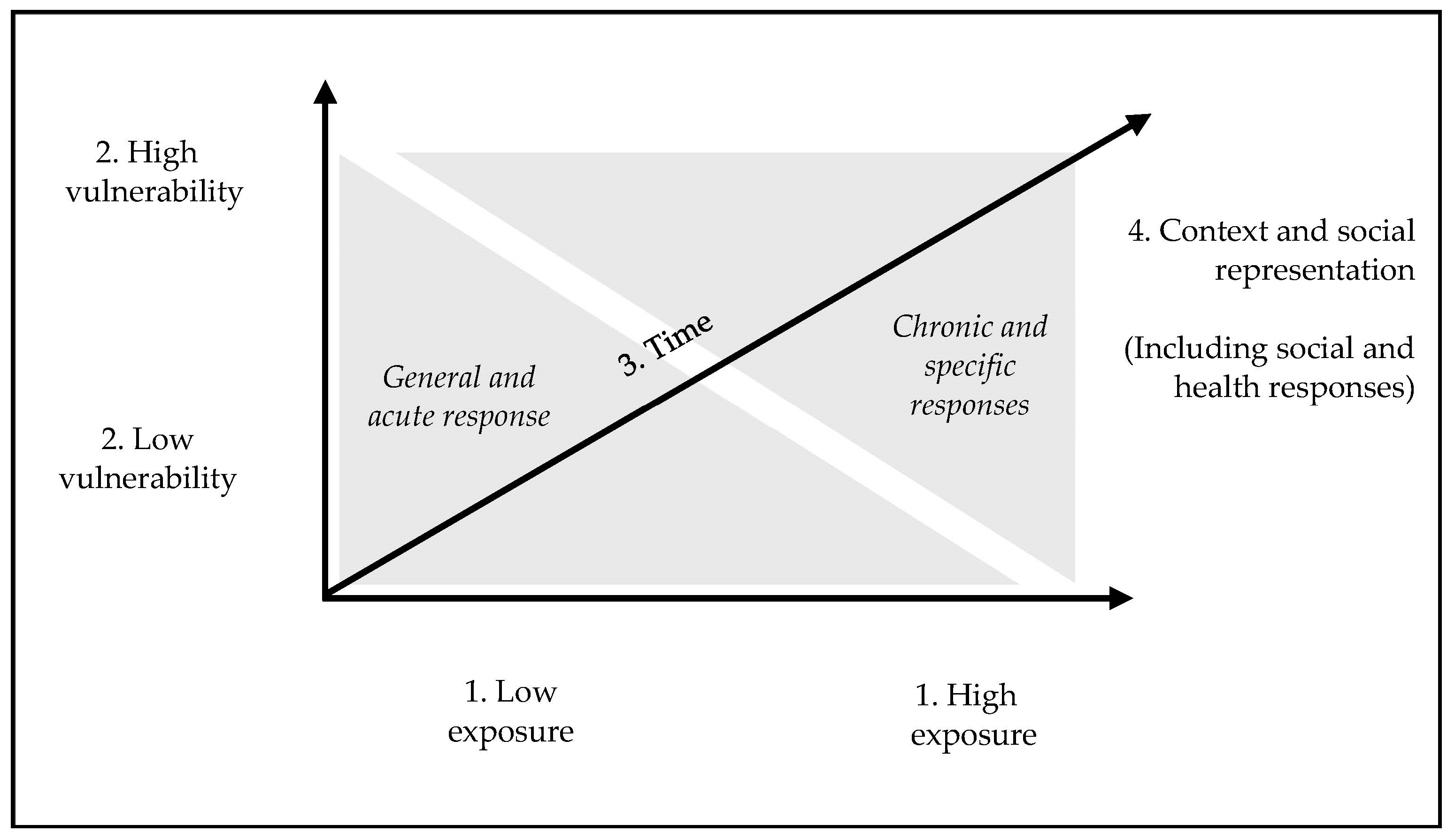
2. A Multiaxial Model for Understanding the Impacts of COVID-19 Pandemic
2.1. Axis 1: Exposure
2.2. Axis 2: Personal and Social Vulnerability
2.3. Axis 3: Time
2.4. Axis 4: Context and Social Representations
3. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ganesh, B.; Rajakumar, T.; Malathi, M.; Manikandan, N.; Nagaraj, J.; Santhakumar, A.; Elangovan, A.; Malik, Y.S. Epidemiology and pathobiology of SARS-CoV-2 (COVID-19) in comparison with SARS, MERS: An updated overview of current knowledge and future perspectives. Clin. Epidemiol. Glob. Health 2021, 10, 100694. [Google Scholar] [CrossRef]
- Şimşir, Z.; Koç, H.; Seki, T.; Griffiths, M.D. The relationship between fear of COVID-19 and mental health problems: A meta-analysis. Death Stud. 2022, 46, 515–523. [Google Scholar] [CrossRef]
- Haig, B.D. An Abductive Theory of Scientific Method. Psychol. Methods 2005, 10, 371–388. [Google Scholar] [CrossRef]
- Black, D.W.; Grant, J.E. DSM-5 Guidebook: The Essential Companion to the Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2014. [Google Scholar]
- Wakefield, J.C. DSM-5: An Overview of Changes and Controversies. Clin. Soc. Work. J. 2013, 41, 139–154. [Google Scholar] [CrossRef]
- Hannemann, J.; Abdalrahman, A.; Erim, Y.; Morawa, E.; Jerg-Bretzke, L.; Beschoner, P.; Geiser, F.; Hiebel, N.; Weidner, K.; Steudte-Schmiedgen, S.; et al. The impact of the COVID-19 pandemic on the mental health of medical staff considering the interplay of pandemic burden and psychosocial resources—A rapid systematic review. PLoS ONE 2022, 17, e0264290. [Google Scholar] [CrossRef]
- Nicolaou, C.; Menikou, J.; Lamnisos, D.; Lubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Papacostas, S.; Aydın, G.; Chong, Y.Y.; et al. Mental Health Status of Healthcare Workers during the COVID-19 Outbreak. Eur. J. Psychol. Open 2021, 80, 62–76. [Google Scholar] [CrossRef]
- Muzi, M.; Talamonti, D.; Rosa Di Prinzio, R.; Sun, X. Effects of COVID-19 Pandemic on Mental Health among Frontline Healthcare Workers: A Systematic Review and Meta-Analysis. 2019. Available online: https://www.crd.york.ac.uk/PROSPERO/ (accessed on 7 March 2023).
- Seckman, C. The impact of COVID-19 on the psychosocial well-being of older adults: A literature review. J. Nurs. Sch. 2023, 55, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Sebastião, R.; Neto, D.D.; Costa, V. Understanding Differential Stress and Mental Health Reactions to COVID-19-Related Events. Int. J. Environ. Res. Public Health 2023, 20, 5819. [Google Scholar] [CrossRef] [PubMed]
- Ingram, R.E.; Luxton, D.D. Vulnerability-stress models. In Development of Psychopathology: A Vulnerability-Stress Perspective; Hankin, B.L., Abela, J.R.Z., Eds.; Sage: London, UK, 2005; pp. 32–46. [Google Scholar]
- Carvalho, S.; Coelho, C.G.; Kluwe-Schiavon, B.; Magalhães, J.; Leite, J. The Acute Impact of the Early Stages of COVID-19 Pandemic in People with Pre-Existing Psychiatric Disorders: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5140. [Google Scholar] [CrossRef]
- Wall, S.; Dempsey, M. The effect of COVID-19 lockdowns on women’s perinatal mental health: A systematic review. Women Birth 2022, 36, 47–55. [Google Scholar] [CrossRef]
- Racine, N.; Eirich, R.; Cooke, J.; Zhu, J.; Pador, P.; Dunnewold, N.; Madigan, S. When the Bough Breaks: A systematic review and meta-analysis of mental health symptoms in mothers of young children during the COVID-19 pandemic. Infant Ment. Health J. 2022, 43, 36–54. [Google Scholar] [CrossRef] [PubMed]
- Alarcão, V.; Virgolino, A.; Stefanovska-Petkovska, M.; Neves, J. Exploring the Effects of the COVID-19 Pandemic on Mental Health and Well-Being of Migrant Populations in Europe: An Equity-Focused Scoping Review. Behav. Sci. 2022, 12, 393. [Google Scholar] [CrossRef] [PubMed]
- El Tatary, G.; Gill, N. The impact of the COVID-19 pandemic on the mental health and wellbeing of refugees and asylum seekers-A Narrative Review of the Literature. Australas. Psychiatry 2022, 30, 728–731. [Google Scholar] [CrossRef] [PubMed]
- Abrahim, H.L.; Holman, E.A. A scoping review of the literature addressing psychological well-being of racial and ethnic minority nurses during the COVID-19 pandemic. Nurs. Outlook 2023, 71, 101899. [Google Scholar] [CrossRef] [PubMed]
- Cénat, J.M.; Farahi, S.M.M.M.; Dalexis, R.D.; Darius, W.P.; Bekarkhanechi, F.M.; Poisson, H.; Broussard, C.; Ukwu, G.; Auguste, E.; Nguyen, D.D.; et al. The global evolution of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis of longitudinal studies. J. Affect. Disord. 2022, 315, 70–95. [Google Scholar] [CrossRef]
- Natarajan, A.; Shetty, A.; Delanerolle, G.; Zeng, Y.; Zhang, Y.; Raymont, V.; Rathod, S.; Halabi, S.; Elliot, K.; Shi, J.Q.; et al. A systematic review and meta-analysis of long COVID symptoms. Syst. Rev. 2023, 12, 1–19. [Google Scholar] [CrossRef]
- Patchaikannu, G. Economic hardships during pandemics and its impact on mental health: A narrative review with special focus on the COVID-19 pandemic. Open J. Psychiatry Allied Sci. 2021, 12, 83–88. [Google Scholar] [CrossRef]
- Asper, M.; Osika, W.; Dalman, C.; Pöllänen, E.; Simonsson, O.; Flodin, P.; Sidorchuk, A.; Marchetti, L.; Awil, F.; Castro, R.; et al. Effects of the COVID-19 pandemic and previous pandemics, epidemics and economic crises on mental health: Systematic review. BJPsych Open 2022, 8, e181. [Google Scholar] [CrossRef]
- Duden, G.S.; Gersdorf, S.; Stengler, K. Global impact of the COVID-19 pandemic on mental health services: A systematic review. J. Psychiatr. Res. 2022, 154, 354–377. [Google Scholar] [CrossRef]
- Chong, Y.Y.; Chien, W.T.; Cheng, H.Y.; Lamnisos, D.; Ļubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; et al. Patterns of Psychological Responses among the Public during the Early Phase of COVID-19: A Cross-Regional Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4143. [Google Scholar] [CrossRef]
- Ye, Z.; Li, W.; Zhu, R. Online psychosocial interventions for improving mental health in people during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2022, 316, 120–131. [Google Scholar] [CrossRef] [PubMed]
- Li, J. Digital technologies for mental health improvements in the COVID-19 pandemic: A scoping review. BMC Public Health 2023, 23, 413. [Google Scholar] [CrossRef] [PubMed]
- Almeda, N.; Díaz-Milanés, D.; Guiterrez-Colosia, M.R.; García-Alonso, C.R. A systematic review of the international evolution of online mental health strategies and recommendations during the COVID-19 pandemic. BMC Psychiatry 2022, 22, 621. [Google Scholar] [CrossRef]
- Harrison, L.; Carducci, B.; Klein, J.D.; Bhutta, Z.A. Indirect effects of COVID-19 on child and adolescent mental health: An overview of systematic reviews. BMJ Glob. Health 2022, 7, e010713. [Google Scholar] [CrossRef]
- Viner, R.; Viner, R.; Russell, S.; Russell, S.; Saulle, R.; Saulle, R.; Croker, H.; Croker, H.; Stansfield, C.; Stansfield, C.; et al. School Closures during Social Lockdown and Mental Health, Health Behaviors, and Well-being among Children and Adolescents During the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Villarreal-Zegarra, D.; Reátegui-Rivera, C.M.; Sabastizagal-Vela, I.; Burgos-Flores, M.A.; Cama-Ttito, N.A.; Rosales-Rimache, J. Policies on mental health in the workplace during the COVID-19 pandemic: A scoping review. PLoS ONE 2022, 17, e0272296. [Google Scholar] [CrossRef]
- Rzeszutek, M.; Gruszczyńska, E.; Pięta, M.; Malinowska, P. HIV/AIDS stigma and psychological well-being after 40 years of HIV/AIDS: A systematic review and meta-analysis. Eur. J. Psychotraumatol. 2021, 12, 1990527. [Google Scholar] [CrossRef]
- Zhao, S.; Hu, S.; Zhou, X.; Song, S.; Wang, Q.; Zheng, H.; Zhang, Y.; Hou, Z. The Prevalence, Features, Influencing Factors, and Solutions for COVID-19 Vaccine Misinformation: Systematic Review. JMIR Public Health Surveill. 2023, 9, e40201. [Google Scholar] [CrossRef]
- Figueiras, M.J.; Neto, D.D.; Maroco, J.; de Castro, E.K. Is my risk lower than yours? The role of compared risk, illness perceptions, and self-efficacy as determinants of perceived risk for COVID-19. Health Risk Soc. 2022, 24, 54–66. [Google Scholar] [CrossRef]
- Neto, D.D.; da Silva, A.N.; Roberto, M.S.; Lubenko, J.; Constantinou, M.; Nicolaou, C.; Lamnisos, D.; Papacostas, S.; Höfer, S.; Presti, G.; et al. Illness Perceptions of COVID-19 in Europe: Predictors, Impacts and Temporal Evolution. Front. Psychol. 2021, 12, 640955. [Google Scholar] [CrossRef]
- Chong, Y.Y.; Chien, W.T.; Cheng, H.Y.; Lamnisos, D.; Ļubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; et al. Predictors of changing patterns of adherence to containment measures during the early stage of COVID-19 pandemic: An international longitudinal study. Glob. Health 2023, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Kassianos, A.P.; Georgiou, A.; Kyprianidou, M.; Lamnisos, D.; Ļubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; et al. Mental Health and Adherence to COVID-19 Protective Behaviors among Cancer Patients during the COVID-19 Pandemic: An International, Multinational Cross-Sectional Study. Cancers 2021, 13, 6294. [Google Scholar] [CrossRef] [PubMed]
- Haller, E.; Lubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; Aydın, G.; Chong, Y.Y.; Chien, W.T.; et al. To Help or Not to Help? Prosocial Behavior, Its Association with Well-Being, and Predictors of Prosocial Behavior During the Coronavirus Disease Pandemic. Front. Psychol. 2022, 12, 775032. [Google Scholar] [CrossRef] [PubMed]
- Neto, D.D.; Figueiras, M.J.; Campos, S.; Tavares, P. Impact of economic crisis on the social representation of mental health: Analysis of a decade of newspaper coverage. Int. J. Soc. Psychiatry 2017, 63, 736–743. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neto, D.D.; Silva, A.N.d. The Mental Health Impacts of a Pandemic: A Multiaxial Conceptual Model for COVID-19. Behav. Sci. 2023, 13, 912. https://doi.org/10.3390/bs13110912
Neto DD, Silva ANd. The Mental Health Impacts of a Pandemic: A Multiaxial Conceptual Model for COVID-19. Behavioral Sciences. 2023; 13(11):912. https://doi.org/10.3390/bs13110912
Chicago/Turabian StyleNeto, David Dias, and Ana Nunes da Silva. 2023. "The Mental Health Impacts of a Pandemic: A Multiaxial Conceptual Model for COVID-19" Behavioral Sciences 13, no. 11: 912. https://doi.org/10.3390/bs13110912
APA StyleNeto, D. D., & Silva, A. N. d. (2023). The Mental Health Impacts of a Pandemic: A Multiaxial Conceptual Model for COVID-19. Behavioral Sciences, 13(11), 912. https://doi.org/10.3390/bs13110912