

A Meta-Analysis of Social Skills Interventions for Preschoolers with or at Risk of Early Emotional and Behavioral Problems


Abstract
:1. Introduction
1.1. Social Skills
1.2. Social Skills Interventions
1.3. Previous Research
1.4. Purpose and Research Questions
- What is the overall effect of SSIs for preschoolers identified with or at risk of early emotional and/or behavioral problems?
- What are the effect sizes of SSIs on outcomes related to (1) social–cognitive skills, (2) problem behaviors, and (3) social competence?
- Are there differential effects for SSIs based on intervention tier, integration, duration, literacy component, curriculum, and treatment fidelity?
2. Method
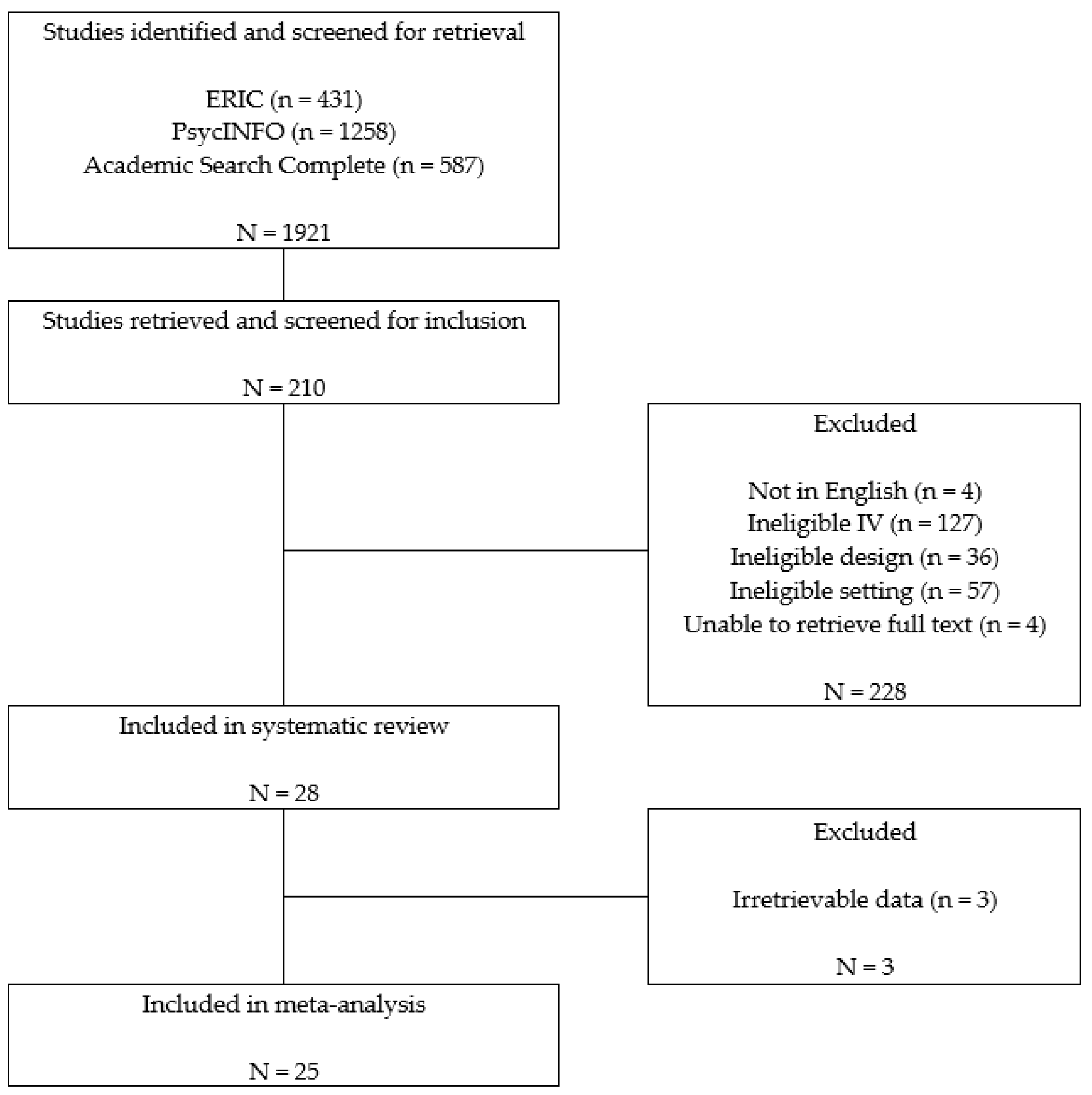
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
- Peer-reviewed journals: Studies had to be published in peer-reviewed journals to ensure the quality of the included studies was relatively high. Dissertations, presentation reports, or studies not published in peer-reviewed journals were excluded. Studies not written in English were also excluded.
- Participants: Studies had to include preschoolers or young children aged 3–6 years old identified as with or at risk of emotional and behavioral problems. At-risk children included the preschoolers who were identified as at risk by any reliable screening tool or nominated by teachers as demonstrating externalizing behavior patterns, including chronic problem behaviors, aggressive behaviors, oppositional–defiant behaviors, frequent tantrums, noncompliance, and rule infractions. Studies were excluded if they mainly included participants identified as with autism spectrum disorder or developmental disabilities.
- Design: Studies had to use group research designs, including an experimental design, quasi-experimental design, or partial randomized control trials with randomization among classrooms or schools. This criterion was also set to ensure the quality of the included studies was high. Studies using single-case research, descriptive studies, qualitative research, or literature reviews were excluded.
- Independent variables: The social skills interventions could be based on any of the following theoretical frameworks, including behavioral, cognitive–behavioral interventions, etc. Studies focused on inclusion policy or studies on environment rearrangement were excluded.
- Implementer: Intervention implementers had to be teachers, para-professionals, or therapists who provided services in preschool settings. Studies on parent training or interventions aimed to improve parent–child relationships and interactions were excluded.
- Settings: Interventions conducted in Head Start programs, public or private preschool programs, daycare programs, or state-funded prekindergarten programs. Because the authors intended to find some commonly applicable group social skills interventions that can be applied in any preschool setting to benefit preschoolers with diverse backgrounds. Studies that were conducted in clinic settings or psychiatric hospitals were excluded.
- Dependent variables: The interventions had to target one of three skills covered in Gresham’s framework of social skills training: social interactions, prosocial behaviors, or social–cognitive skills. Studies had to examine and report the effects of SSIs on one or more social, emotional, or behavioral outcomes.
- Results: Studies had to report enough statistics to calculate an effect size for the intervention. Enough statistics means the authors need to report the mean scores and standard deviations of the experiment and control groups that could lead to the calculation of effect size d or the authors reported the numbers of participants in the experiment and control groups and any summary effect size statistics (e.g., t, F, or chi-square) that can be converted to effect size d. Studies that did not report enough statistical information to calculate the effect sizes were excluded. For several studies, the authors were contacted to obtain more information to calculate effect sizes. The studies in which the author replied with enough information were included (e.g., [23,24]).
2.3. Coding for Descriptive Information
2.4. Inter-Rater Reliability for Coding
2.5. Data Analysis and Calculation of Effects
3. Results
3.1. Overall Effects
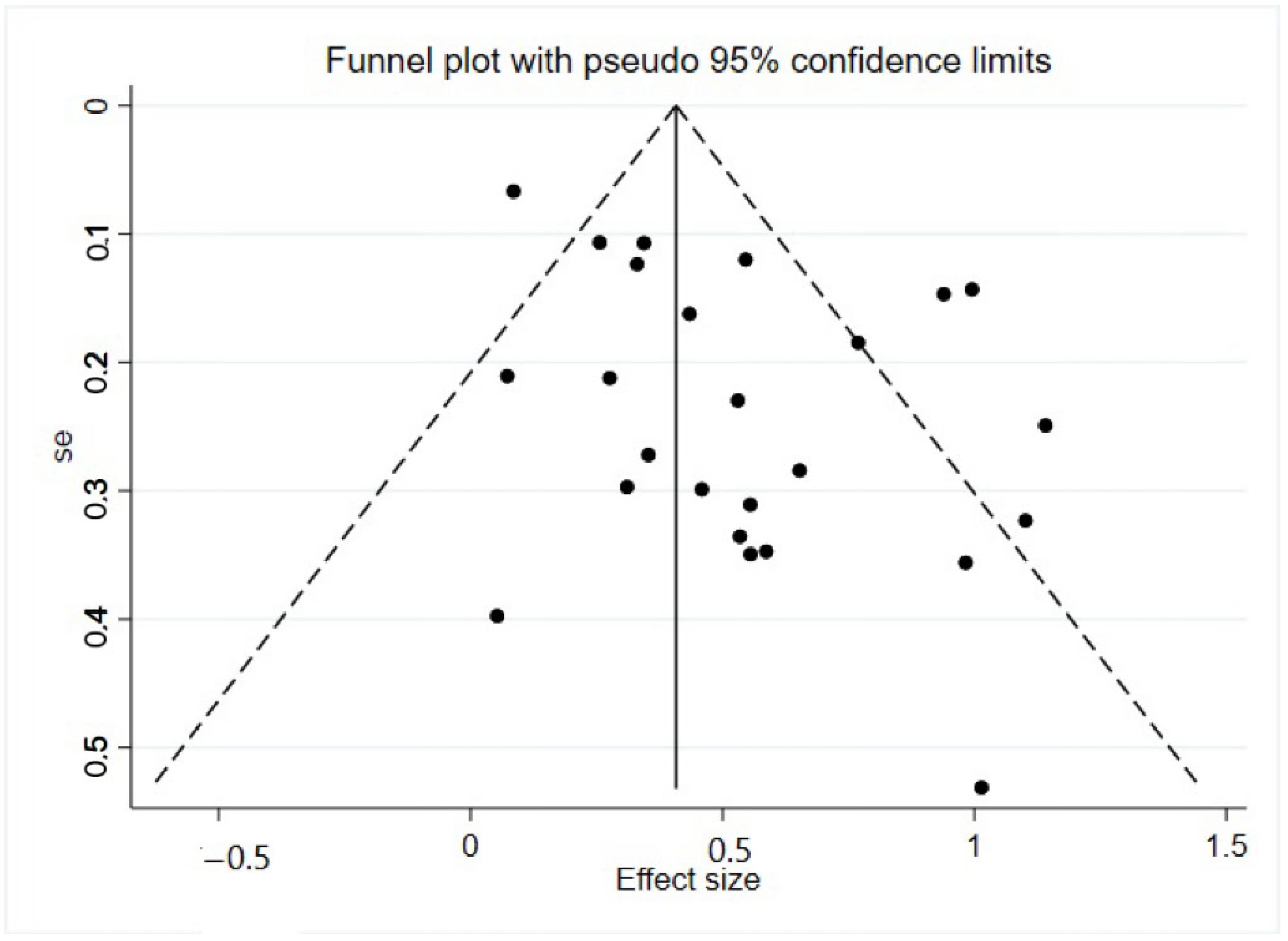
3.2. Examining for Publication Bias
3.3. Moderator Analysis
4. Discussions
Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feil, E.G.; Frey, A.; Walker, H.M.; Small, J.W.; Seeley, J.R.; Golly, A.; Forness, S.R. The efficacy of a home-school intervention for preschoolers with challenging behaviors: A randomized controlled trial of Preschool First Step to Success. J. Early Interv. 2014, 36, 151–170. [Google Scholar] [CrossRef]
- Brown, W.H.; Conroy, M.A. Social-emotional competence in young children with developmental delays: Our reflection and vision for the future. J. Early Interv. 2011, 33, 310–320. [Google Scholar] [CrossRef]
- Forness, S.R.; Freeman, S.F.; Paparella, T.; Kauffman, J.M.; Walker, H.M. Special education implications of point and cumulative prevalence for children with emotional or behavioral disorders. J. Emot. Behav. Disord. 2012, 20, 4–18. [Google Scholar] [CrossRef]
- Kellam, S.G.; Werthamer-Larsson, L.; Dolan, L.J.; Brown, C.H.; Mayer, L.S.; Rebok, G.W.; Anthony, J.C.; Laudolff, J.; Edelsohn, G.; Wheeler, L. Developmental epidemiologically based preventive trials: Baseline modeling of early target behaviors and depressive symptoms. Am. J. Community Psychol. 1991, 19, 563–584. [Google Scholar] [CrossRef]
- McCabe, P.C.; Altamura, M. Empirically valid strategies to improve social and emotional competence of preschool children. Psychol. Sch. 2011, 48, 513–540. [Google Scholar] [CrossRef]
- Maag, J.W. Social Skills Training for Students With Emotional and Behavioral Disorders: A Review of Reviews. Behav. Disord. 2006, 32, 4–17. [Google Scholar] [CrossRef]
- Bulotsky-Shearer, R.J.; Domínguez, X.; Bell, E.R.; Rouse, H.L.; Fantuzzo, J.W. Relations between behavior problems in classroom social and learning situations and peer social competence in Head Start and kindergarten. J. Emot. Behav. Disord. 2010, 18, 195–210. [Google Scholar] [CrossRef]
- Heckman, J.J. Skill formation and the economics of investing in disadvantaged children. Science 2006, 312, 1900–1902. [Google Scholar] [CrossRef]
- Gresham, F.M. Response to intervention and emotional and behavioral disorders: Best practices in assessment for intervention. Assess. Eff. Interv. 2007, 32, 214–222. [Google Scholar] [CrossRef]
- Lösel, F.; Beelmann, A. Effects of Child Skills Training in Preventing Antisocial Behavior: A Systematic Review of Randomized Evaluations. Ann. Am. Acad. Political Soc. Sci. 2003, 587, 84–109. [Google Scholar] [CrossRef]
- Sentse, M.; Kretschmer, T.; de Haan, A.; Prinzie, P. Conduct problem trajectories between age 4 and 17 and their association with behavioral adjustment in emerging adulthood. J. Youth Adolesc. 2017, 46, 1633–1642. [Google Scholar] [CrossRef] [PubMed]
- Merrell, K.W.; Gimple, G. Social Skills of Children and Adolescents: Conceptualization, Assessment, Treatment; Psychology Press: London, UK, 2014. [Google Scholar]
- Gresham, F.M. Conceptual issues in the assessment of social competence. In Children’s Social Behavior: Development, Assessment, and Modification; Elsevier: Amsterdam, The Netherlands, 1986; pp. 143–179. [Google Scholar]
- Gresham, F. Evidence-based social skills interventions for students at risk for EBD. Remedial Spec. Educ. 2015, 36, 100–104. [Google Scholar] [CrossRef]
- Gresham, F.M.; Cook, C.R.; Crews, S.D.; Kern, L. Social skills training for children and youth with emotional and behavioral disorders: Validity considerations and future directions. Behav. Disord. 2004, 30, 32–46. [Google Scholar] [CrossRef]
- Krueger, R.F.; Hicks, B.M.; McGue, M. Altruism and Antisocial Behavior: Independent Tendencies, Unique Personality Correlates, Distinct Etiologies. Psychol. Sci. 2001, 12, 397–402. [Google Scholar] [CrossRef]
- Shure, M.B.; Spivack, G. Interpersonal problem solving as a mediator of behavioral adjustment in preschool and kindergarten children. J. Appl. Dev. Psychol. 1980, 1, 29–44. [Google Scholar] [CrossRef]
- Bierman, K.L.; Domitrovich, C.E.; Nix, R.L.; Gest, S.D.; Welsh, J.A.; Greenberg, M.T.; Blair, C.; Nelson, K.E.; Gill, S. Promoting academic and social-emotional school readiness: The Head Start REDI program. Child Dev. 2008, 79, 1802–1817. [Google Scholar] [CrossRef]
- Kauffman, J.M. How we prevent the prevention of emotional and behavioral disorders. In Handbook of Emotional and Behavioural Difficulties; Clough, P., Ed.; Sage: London, UK, 2005; pp. 429–440. [Google Scholar]
- Schneider, B.H.; Byrne, B.M. Children’s social skills training: A meta-analysis. In Children’s Peer Relations: Issues in Assessment and Intervention; Springer: Berlin/Heidelberg, Germany, 1985; pp. 175–192. [Google Scholar]
- Beelmann, A.; Pfingsten, U.; Lösel, F. Effects of training social competence in children: A meta-analysis of recent evaluation studies. J. Clin. Child Psychol. 1994, 23, 260–271. [Google Scholar] [CrossRef]
- Schneider, B.H. Didactic methods for enhancing children’s peer relations: A quantitative review. Clin. Psychol Rev. 1992, 12, 363–382. [Google Scholar] [CrossRef]
- Webster-Stratton, C.; Jamila Reid, M.; Stoolmiller, M. Preventing conduct problems and improving school readiness: Evaluation of the incredible years teacher and child training programs in high-risk schools. J. Child Psychol. Psychiatry 2008, 49, 471–488. [Google Scholar] [CrossRef]
- Fishbein, D.H.; Domitrovich, C.; Williams, J.; Gitukui, S.; Guthrie, C.; Shapiro, D.; Greenberg, M. Short-term intervention effects of the PATHS curriculum in young low-income children: Capitalizing on plasticity. J. Prim. Prev. 2016, 37, 493–511. [Google Scholar] [CrossRef]
- Graziano Paulo, A.; Hart, K. Beyond behavior modification: Benefits of social-emotional/self-regulation training for preschoolers with behavior problems. J. Sch. Psychol. 2016, 58, 91–111. [Google Scholar] [CrossRef] [PubMed]
- Gunter, L.; Caldarella, P.; Korth, B.B.; Young, K.R. Promoting social and emotional learning in preschool students: A study of Strong Start Pre-K. Early Child. Educ. J. 2012, 40, 151–159. [Google Scholar] [CrossRef]
- Hughes, C.; Cline, T. An evaluation of the preschool PATHS curriculum on the development of preschool children. Educ. Psychol. Pract. 2015, 31, 73–85. [Google Scholar] [CrossRef]
- Hyatt, K.J.; Filler, J.W. A comparison of the effects of two social skill training approaches on teacher and child behavior. J. Res. Child. Educ. 2007, 22, 85–96. [Google Scholar] [CrossRef]
- Sharp, K.C. Impact of interpersonal problem-solving training on preschoolers’ social competency. J. Appl. Dev. Psychol. 1981, 2, 129–143. [Google Scholar] [CrossRef]
- Shure, M.B.; Spivack, G.; Gordon, R. Problem-solving thinking: A preventive mental health program for preschool children. Lit. Res. Instr. 1972, 11, 259–273. [Google Scholar] [CrossRef]
- Olson, S.L. Assessment of impulsivity in preschoolers: Cross-measure convergences, longitudinal stability, and relevance to social competence. J Clin Child Psychol 1989, 18, 176–183. [Google Scholar] [CrossRef]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Wilson, S.J.; Lipsey, M.W. School-based interventions for aggressive and disruptive behavior: Update of a meta-analysis. Am. J. Prev. Med. 2007, 33, S130–S143. [Google Scholar] [CrossRef]
- Hedges, L.V.; Tipton, E.; Johnson, M.C. Robust variance estimation in meta-regression with dependent effect size estimates. Res. Synth. Methods 2010, 1, 39–65. [Google Scholar] [CrossRef]
- Tanner-Smith, E.E.; Tipton, E. Robust variance estimation with dependent effect sizes: Practical considerations including a software tutorial in Stata and SPSS. Res. Synth. Methods 2014, 5, 13–30. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Feil, E.G.; Small, J.W.; Seeley, J.R.; Walker, H.M.; Golly, A.; Frey, A.; Forness, S.R. Early intervention for preschoolers at risk for attention-deficit/hyperactivity disorder: Preschool first step to success. Behav. Disord. 2016, 41, 95–106. [Google Scholar] [CrossRef]
- Çelik, S.; Diken, I.; Çolak, A.; Arikan, A.; Aksoy, F.; Tomris, G. Effectiveness of the preschool version of the First Step to Success early intervention program for preventing antisocial behaviors. Educ. Sci.-Theory Pract. 2016, 16, 511–535. [Google Scholar]
- Denham, S.A.; Burton, R. A social-emotional intervention for at-risk 4-year-olds. J. Sch. Psychol. 1996, 34, 225–245. [Google Scholar] [CrossRef]
- Hart, K.C.; Graziano, P.A.; Kent, K.M.; Kuriyan, A.; Garcia, A.; Rodriguez, M.; Pelham, W.E., Jr. Early intervention for children with behavior problems in summer settings: Results from a pilot evaluation in head start preschools. J. Early Interv. 2016, 38, 92–117. [Google Scholar] [CrossRef]
- Hemmeter, M.L.; Snyder, P.A.; Fox, L.; Algina, J. Evaluating the implementation of the Pyramid Model for promoting social-emotional competence in early childhood classrooms. Top. Early Child. Spec. Educ. 2016, 36, 133–146. [Google Scholar] [CrossRef]
- Koglin, U.; Petermann, F. The effectiveness of the behavioural training for preschool children. Eur. Early Child. Educ. Res. J. 2011, 19, 97–111. [Google Scholar] [CrossRef]
- Nix, R.L.; Bierman, K.L.; Domitrovich, C.E.; Gill, S. Promoting children’s social-emotional skills in preschool can enhance academic and behavioral functioning in kindergarten: Findings from Head Start REDI. Early Educ. Dev. 2013, 24, 1000–1019. [Google Scholar] [CrossRef]
- Reinke, W.M.; Stormont, M.; Herman, K.C.; Wang, Z.; Newcomer, L.; King, K. Use of coaching and behavior support planning for students with disruptive behavior within a universal classroom management program. J. Emot. Behav. Disord. 2014, 22, 74–82. [Google Scholar] [CrossRef]
- Serna, L.; Nielsen, E.; Lambros, K.; Forness, S. Primary prevention with children at risk for emotional or behavioral disorders: Data on a universal intervention for Head Start classrooms. Behav. Disord. 2000, 26, 70–84. [Google Scholar] [CrossRef]
- Stefan, C.A. Short-term efficacy of a primary prevention program for the development of social-emotional competencies in preschool children. Cogn. Brain Behav. 2008, 12, 285. [Google Scholar]
- Ştefan, C.A.; Miclea, M. Effects of a multifocused prevention program on preschool children’s competencies and behavior problems. Psychol. Sch. 2013, 50, 382–402. [Google Scholar] [CrossRef]
- Tankersley, M.; Kamps, D.; Mancina, C.; Weidinger, D. Social interventions for Head Start children with behavioral risks: Implementation and outcomes. J. Emot. Behav. Disord. 1996, 4, 171–181. [Google Scholar] [CrossRef]
- Tucker, C.; Schieffer, K.; Wills, T.J.; Hull, C.; Murphy, Q. Enhancing social-emotional skills in at-risk preschool students through Theraplay based groups: The Sunshine Circle Model. Int. J. Play Ther. 2017, 26, 185. [Google Scholar] [CrossRef]
- Xu, Y. Examining the effects of adapted peer tutoring on social and language skills of young English language learners. Early Child Dev. Care 2015, 185, 1587–1600. [Google Scholar] [CrossRef]
- Wheeler, J.J.; Mayton, M.R.; Ton, J.; Reese, J.E. Evaluating treatment integrity across interventions aimed at social and emotional skill development in learners with emotional and behaviour disorders. J. Res. Spec. Educ. Needs 2014, 14, 164–169. [Google Scholar] [CrossRef]
- Rosenthal, R.; DiMatteo, M.R. Meta-analysis: Recent developments in quantitative methods for literature reviews. Annu Rev. Psychol. 2001, 52, 59–82. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Fisher, Z.; Tipton, E. Robumeta: An R-package for robust variance estimation in meta-analysis. arXiv 2015, arXiv:1503.02220. [Google Scholar]
- Gresham, F.M.; Van, M.B.; Cook, C.R. Social skills training for teaching replacement behaviors: Remediating, acquisition deficits in at-risk students. Behav. Disord. 2006, 31, 363–377. [Google Scholar] [CrossRef]
- Rubin, K.H.; Asendorpj, J.B. Social withdrawal, inhibition, and shyness in childhood: Conceptual and definitional issues. In Social Withdrawal, Inhibition, and Shyness in Childhood; Psychology Press: London, UK, 2014; pp. 13–28. [Google Scholar]



{kind=link}
{kind=link}
| Methodological Features | N | % | Intervention Features | N | % | Intervention Features | N | % |
|---|---|---|---|---|---|---|---|---|
| Research design | Intervention tier | Setting | ||||||
| Experimental design | 10 | 40 | Primary intervention | 10 | 40 | Head Start | 6 | 24 |
| Quasi-experimental design | 6 | 24 | Secondary intervention | 7 | 28 | Public or private preschool | 15 | 60 |
| Partial randomized | 9 | 36 | Tertiary intervention | 1 | 4 | Inclusive preschool | 1 | 4 |
| Randomization | Combined | 7 | 28 | Combination of the above | 3 | 12 | ||
| Yes | 21 | 84 | Integration of intervention | Literacy component | ||||
| No | 4 | 16 | Integrated full-day | 14 | 56 | Yes | 6 | 24 |
| Curriculum | Scheduled time period | 11 | 44 | No | 19 | 76 | ||
| Yes | 16 | 64 | Implementer | Coaching | ||||
| No | 9 | 36 | Researcher | 2 | 8 | Yes | 13 | 52 |
| Trained teacher or staff | 15 | 60 | No | 12 | 48 | |||
| Collaboration | 8 | 32 |
| ID | Study | Design | N | n Exp | n Con | Gender | Ethnicity | Disability | Intervention | Duration | Tier | Parent | Coach | T.F. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Bierman et al., 2008 [18] | Exp. | 356 | 192 | 164 | 54% F | 17% H, 25% AA | At risk, low income | The Head Start REDI program and PATHS Curriculum | 33 wks | 1st | 2 | Y | Y |
| 2. | Celik et al., 2016 [38] | Exp. | 22 | 11 | 11 | 9% F | NR | At risk of antisocial | preschool FSS | 30 days | 3rd | 1 | Y | Y |
| 3. | Denham et al., 1996 [39] | Quasi | 105 | 63 | 42 | NR | 76% min | 69 at risk | High Scope model, PATHS, Prosocial Activity Guide, and ICPS | 32 wks | 1st + 2nd | 3 | Y | Y |
| 4. | Feil et al., 2014 [1] | Exp. | 126 | 65 | 61 | 35% F | 31% AA, 44% C, 13% H | Ext. problems | preschool FSS | 30 days | 2nd | 1 | Y | Y |
| 5. | Feil et al., 2016 [37] | Exp. | 45 | 26 | 19 | 16% F | 16% AA, | 12% have disability | preschool FSS | 30 days | 1st + 2nd | 1 | Y | Y |
| 6. | Fishbein et al., 2016 [24] | Exp. | 327 | 154 | 173 | NR | Most AA | NR | PATHS, universal social–emotional program | 22 wks | 1st | 2 | Y | Y |
| 7. | Graziano et al., 2016 [25] | Exp. | 41~ | 15 | 11 | 24% F | 84% H | Ext. problems | School readiness parenting program and STP-PreK | 8 wks | 2nd | 1 | N | Y |
| 8. | Gunter et al., 2012 [26] | Quasi | 84~ | 28 | 32 | 50% F | 66.7% H, 26.2% C, 2.4% AA, | Int. problems | Strong Start Pre-K | 6 wks | 1st | 3 | N | Y |
| 9. | Hart et al., 2016 [40] | Exp. | 46 * | 22 | 24 | 22% F | 98% min, 52% H | Ext. problems | Kindergarten summer readiness classroom | 4 wks | 2nd | 1 | Y | Y |
| 10. | Hemmeter et al., 2016 [41] | Exp. | 97 * | 54 | 43 | NR | 42.3% C, 37.5% AA, 18.3% H | 72% with IEP | Pyramid Model for Promoting Young Children’s Social–Emotional Competence | 1 school year | 1st + 2nd + 3rd | 3 | Y | Y |
| 11. | Hughes et al., 2015 [27] | Quasi | 57~ | 20 | 17 | 50.8% F | NR | NR | PATHS | 9 months | 1st | 3 | N | N |
| 12. | Hyatt, 2007 [28] | Exp. | 24~ | 8 | 8 | 50% F | NR | 6 have disability | Adaptation from Skill streaming in Early Childhood | 8 days | 2nd | 3 | N | N |
| 13. | Koglin et al., 2011 [42] | Quasi | 90 | 48 | 42 | 47.4% F | NR | Ext. or Int. behavior | Behavior training for preschool children | 13 wks | 1st | 3 | N | Y |
| 14. | Nix et al., 2013 [43] | Exp. | 356 | 192 | 164 | 54% F | 25% AA, 17% L | At risk, low income | REDI and preschool PATHS | 1 year | 1st | 3 | Y | Y |
| 15. | Reinke et al., 2014 [44] | Exp. | 46 | 23 | 23 | 30% F | 91.3% AA, 8% C | 15% with disruptive behaviors | IY Teacher Classroom Management, | NR | 1st + 2nd | 3 | Y | Y |
| 16. | Serna et al., 2000 [45] | Exp. | 84 | 53 | 31 | 56% F | 71.4% H, 12% AA | NR | Self-determination program | 12 wks | 1st | 1 | N | N |
| 17. | Sharp, 1981 [29] | Exp. | 54~ | 18 | 19 | 46% F | All AA | NR | ICPS | 11 wks | 2nd | 3 | N | N |
| 18. | Shure et al., 1980 [17] | Exp. | 219 | 113 | 106 | 55.7% F | All AA | NR | ICPS | 3 months | 2nd | 3 | N | N |
| 19. | Shure et al., 1972 [30] | Exp. | 54~ | 22 | 21 | 48% F | NR | NR | ICPS | 10 wks | 2nd | 3 | N | N |
| 20. | Stefan, 2008 [46] | Quasi | 52 | 26 | 26 | 50% F | NR | NR | A 5-step social–emotional program | 5 months | 1st | 3 | N | N |
| 21. | Stefan et al., 2013 [47] | Exp. | 158 | 89 | 69 | 55% F | All C | 20% Ext. problem | Social–emotional prevention program | NR | 1st + 2nd | 1 | Y | Y |
| 22. | Tankersley et al., 1996 [48] | Exp. | 45 | 34 | 11 | 37.8% F | 64% AA, 33% C, 2% H | At risk, with Ext. problems | Affection activities, social skills instructions, | 10 wks | 2nd | 1 | N | N |
| 23 | Tucker et al., 2017 [49] | Exp. | 206 | 107 | 99 | NR | 40% AA, 22%NA, 20% H | 9 have disability | Sunshine circles (group therapy) | 1 year | 1st | 3 | Y | N |
| 24. | Webster-Stratton et al., 2008 [23] | Exp. | 1768 | 1096 | 672 | 50% F | 18% L, 18% AA, 20% A, 27% C | At risk, low income | IY social–emotional and problem-solving curriculum | 1 year | 1st + 2nd | 3 | Y | Y |
| 25. | Xu, 2015 [50] | Exp. | 75 | 39 | 36 | 52% F | 83% H | NR | Adapted peer tutoring | 1 semester | 1st | 3 | N | Y |
| Outcome | |||||
|---|---|---|---|---|---|
| Social–Cognitive Skills | Problem Behavior | Social Competence | Effect Size | ||
| Respondent | Teacher | 0.51 1 (0.35, 0.67) 2.00 (24:12) | 0.53 1 (0.38, 0.69) 3.18 (54:17) | 0.23 2 (0.03, 0.42) 1.50 (6:4) | 0.48 1 (0.35, 0.62) 4.67 (84:18) |
| Parent | 0.37 2 (0.05, 0.70) 1.25 (5:4) | 0.24 (−0.03, 0.51) 1.71 (12:7) | 0.08 (−0.41, 0.56) 1.50 (3:2) | 0.26 2 (0.04, 0.48) 2.86 (20:7) | |
| Child | 0.69 (0.43, 0.94) 3.00 (24:8) | no effect size estimates | no effect size estimates | 0.69 1 (0.43, 0.94) 3.00 (24:8) | |
| Other | 0.63 2 (0.13, 1.13) 2.50 (15:6) | 0.58 (−0.24, 1.40) 1.75 (7:4) | 0.26 (0.05 to 0.47) (single effect size) | 0.51 2 (0.16, 0.86) 2.88 (23:8) | |
| Overall Summary | 0.54 1 (0.42, 0.66) 2.96 (68:23) | 0.54 1 (0.39, 0.70) 3.84 (73:19) | 0.20 (−0.01, 0.41) 2.50 (10:4) | 0.54 1 (0.42, 0.67) 6.04 (151:25) | |
| Legend | Effect Size (95% Confidence Interval) Average number of Effect Size per Study (number of Effect Size: number of Studies). | ||||
| Meta-Regression Models | Coeff. | p-Value | 95% CI | I2 tau2 |
|---|---|---|---|---|
| Intercept | 0.75 | <0.01 | 0.48, 1.02 | 69.86 |
| Curriculum | −0.30 | <0.05 | −0.58, −0.03 | 0.0923 |
| Intercept | 0.72 | <0.01 | 0.51, 0.93 | 68.88 |
| Integration | −0.29 | <0.05 | −0.52, −0.06 | 0.0877 |
| Intercept | 0.74 | <0.01 | 0.56, 0.92 | 69.22 |
| Treatment fidelity | −0.28 | <0.05 | −0.50, −0.06 | 0.0891 |
| Intercept | 0.33 | <0.10 * | −0.00, 0.65 | 73.46 |
| Randomization | 0.26 | <0.10 | −0.07, 0.59 | 0.1067 |
| Intercept | 0.55 | <0.01 | 0.39 0.72 | 74.23 |
| Intervention tier | −0.02 | ns | −0.27, 0.22 | 0.1154 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, X.; Burke, M.D.; Ramirez, G.; Xu, Z.; Bowman-Perrott, L. A Meta-Analysis of Social Skills Interventions for Preschoolers with or at Risk of Early Emotional and Behavioral Problems. Behav. Sci. 2023, 13, 940. https://doi.org/10.3390/bs13110940
Dong X, Burke MD, Ramirez G, Xu Z, Bowman-Perrott L. A Meta-Analysis of Social Skills Interventions for Preschoolers with or at Risk of Early Emotional and Behavioral Problems. Behavioral Sciences. 2023; 13(11):940. https://doi.org/10.3390/bs13110940
Chicago/Turabian StyleDong, Xin, Mack D. Burke, Gilbert Ramirez, Zhihong Xu, and Lisa Bowman-Perrott. 2023. "A Meta-Analysis of Social Skills Interventions for Preschoolers with or at Risk of Early Emotional and Behavioral Problems" Behavioral Sciences 13, no. 11: 940. https://doi.org/10.3390/bs13110940
APA StyleDong, X., Burke, M. D., Ramirez, G., Xu, Z., & Bowman-Perrott, L. (2023). A Meta-Analysis of Social Skills Interventions for Preschoolers with or at Risk of Early Emotional and Behavioral Problems. Behavioral Sciences, 13(11), 940. https://doi.org/10.3390/bs13110940