
The Relationship between Handgrip Strength, Timed Up-and-Go, and Mild Cognitive Impairment in Older People during COVID-19 Pandemic Restrictions




Abstract
:1. Introduction
2. Methods
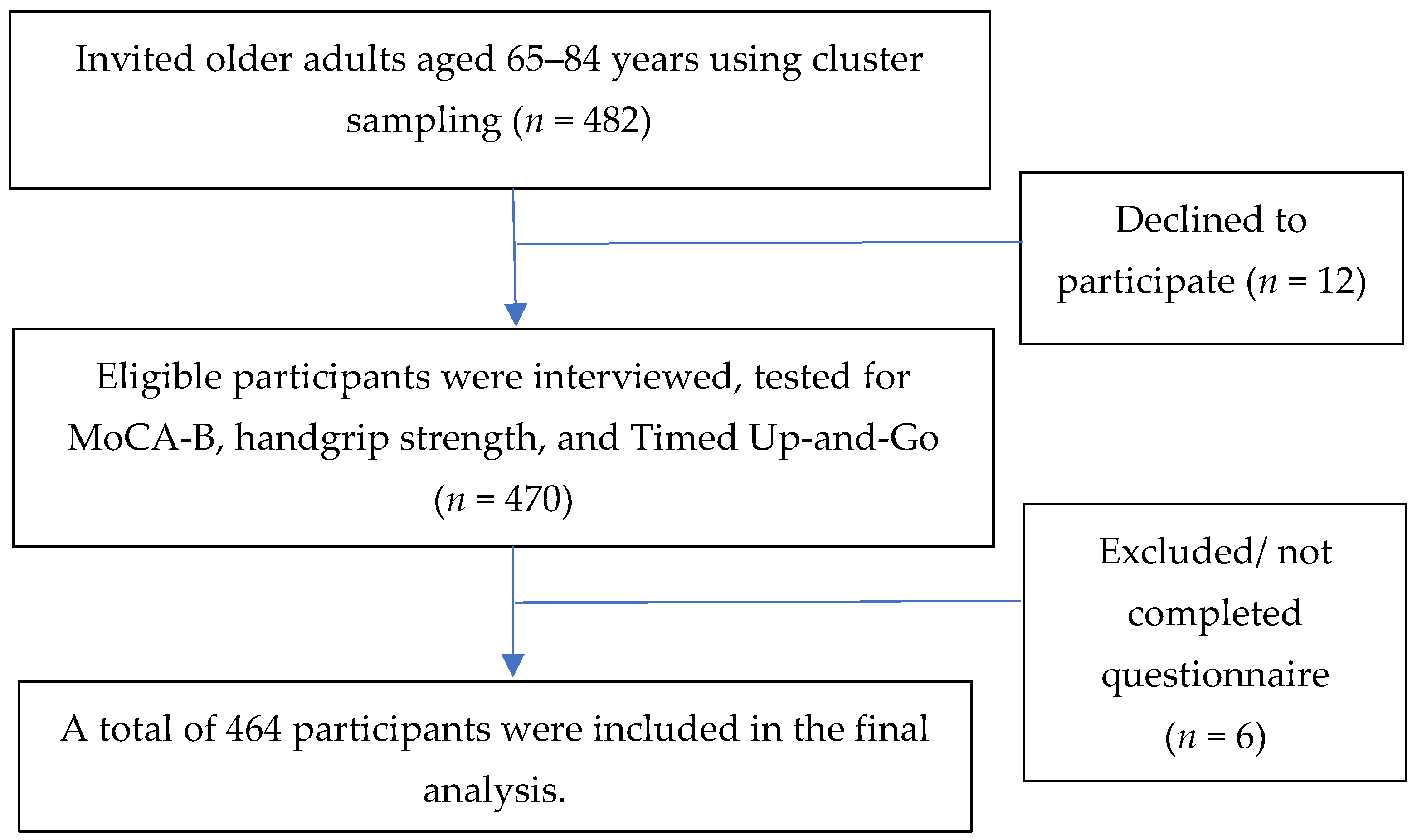
2.1. Study Design and Participants
2.2. Data Collection and Measurement
2.3. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. MoCA-B Scores and Difference between the Non-MCI and MCI Groups
3.3. Handgrip Strength and Timed Up-and-Go
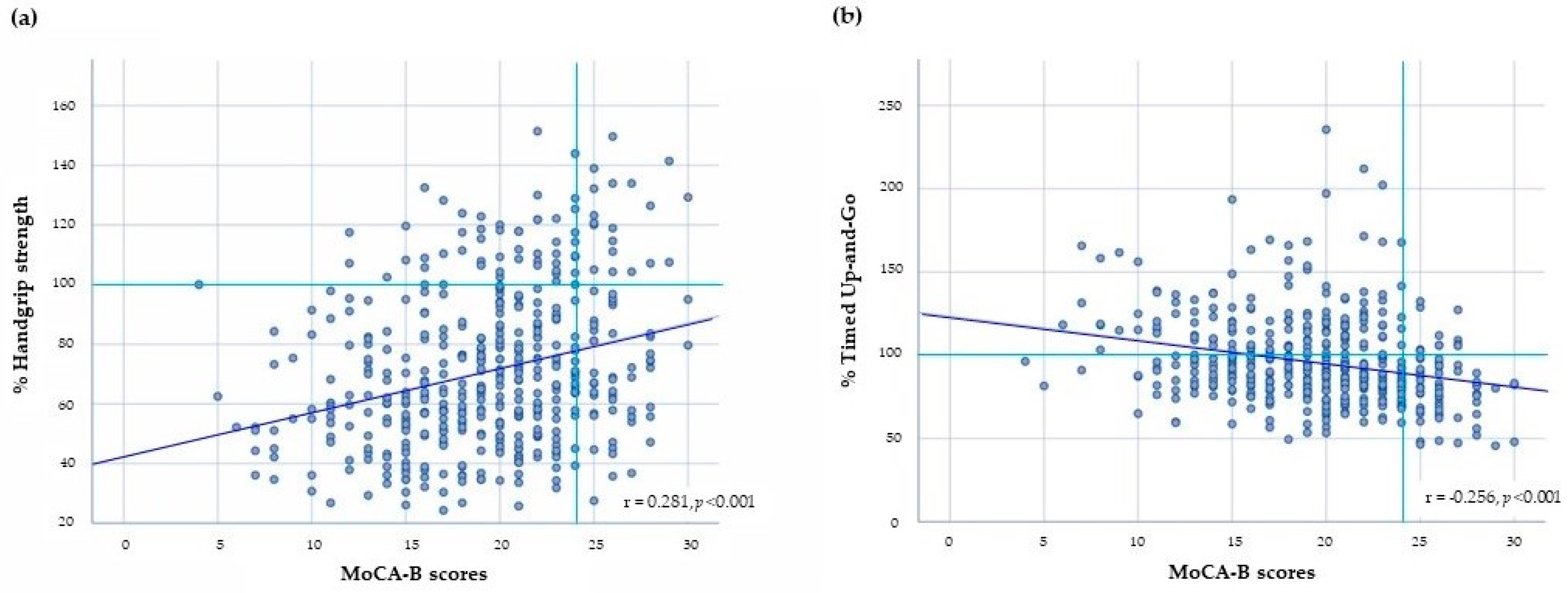
3.4. Relationship between Handgrip Strength, Timed Up-and-Go, and Mild Cognitive Impairment
3.5. The Factors Associated with MoCA-B Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jung, Y.H.; Park, S.; Jang, H.; Cho, S.H.; Kim, S.J.; Kim, J.P.; Kim, S.T.; Na, D.L.; Seo, S.W.; Kim, H.J. Frontal-executive dysfunction affects dementia conversion in patients with amnestic mild cognitive impairment. Sci. Rep. 2020, 10, 772. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Lipnicki, D.M.; Kochan, N.A.; Crawford, J.D.; Thalamuthu, A.; Andrews, G.; Brayne, C.; Matthews, F.E.; Stephan, B.C.; Lipton, R.B.; et al. The Prevalence of Mild Cognitive Impairment in Diverse Geographical and Ethnocultural regions: The COSMIC Collaboration. PLoS ONE 2015, 10, e0142388. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, J.; Thaikruea, L.; Wongpakaran, N.; Munkhetvit, P. Prevalence of Mild Cognitive Impairment in Rural Thai Older People, Associated Risk Factors and their Cognitive Characteristics. Dement. Geriatr. Cogn. Dis. Extra 2020, 10, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Jekel, K.; Damian, M.; Wattmo, C.; Hausner, L.; Bullock, R.; Connelly, P.J.; Dubois, B.; Eriksdotter, M.; Ewers, M.; Graessel, E.; et al. Mild cognitive impairment and deficits in instrumental activities of daily living: A systematic review. Alzheimer’s Res. Ther. 2015, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Brasure, M.; Desai, P.; Davila, H.; Nelson, V.A.; Calvert, C.; Jutkowitz, E.; Butler, M.; Fink, H.A.; Ratner, E.; Hemmy, L.S.; et al. Physical Activity Interventions in Preventing Cognitive Decline and Alzheimer-Type Dementia: A Systematic Review. Ann. Intern. Med. 2018, 168, 30–38. [Google Scholar] [CrossRef]
- Ciesielska, N.; Sokołowski, R.; Mazur, E.; Podhorecka, M.; Polak-Szabela, A.; Kędziora-Kornatowska, K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr. Pol. 2016, 50, 1039–1052. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Julayanont, P.; Tangwongchai, S.; Hemrungrojn, S.; Tunvirachaisakul, C.; Phanthumchinda, K.; Hongsawat, J.; Suwichanarakul, P.; Thanasirorat, S.; Nasreddine, Z.S. The Montreal Cognitive Assessment-Basic: A Screening Tool for Mild Cognitive Impairment in Illiterate and Low-Educated Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 2550–2554. [Google Scholar] [CrossRef]
- Huang, Q.; Zhao, J.; Jiang, W.; Wang, W. The Association between Physical Activity and Cognitive Function: Data from the China Health and Nutrition Survey. Behav Neurol. 2022, 2022, 3438078. [Google Scholar] [CrossRef]
- Tavares, J.; Sa-Couto, P.; Reis, J.D.; Boltz, M.; Capezuti, E. The Role of Frailty in Predicting 3 and 6 Months Functional Decline in Hospitalized Older Adults: Findings from a Secondary Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7126. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Lee, L.; Patel, T.; Costa, A.; Bryce, E.; Hillier, L.M.; Slonim, K.; Hunter, S.W.; Heckman, G.; Molnar, F. Screening for frailty in primary care: Accuracy of gait speed and hand-grip strength. Can. Fam. Physician 2017, 63, e51–e57. [Google Scholar]
- Su, H.; Sun, X.; Li, F.; Guo, Q. Association between handgrip strength and cognition in a Chinese population with Alzheimer’s disease and mild cognitive impairment. BMC Geriatr. 2021, 21, 459. [Google Scholar] [CrossRef]
- Cui, M.; Zhang, S.; Liu, Y.; Gang, X.; Wang, G. Grip Strength and the Risk of Cognitive Decline and Dementia: A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. Front. Aging Neurosci. 2021, 13, 625551. [Google Scholar] [CrossRef]
- Alfaro-Acha, A.; Al Snih, S.; Raji, M.A.; Kuo, Y.F.; Markides, K.S.; Ottenbacher, K.J. Handgrip strength and cognitive decline in older Mexican Americans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 859–865. [Google Scholar] [CrossRef]
- Auyeung, T.W.; Lee, J.S.; Kwok, T.; Woo, J. Physical frailty predicts future cognitive decline—A four-year prospective study in 2737 cognitively normal older adults. J. Nutr. Health Aging 2011, 15, 690–694. [Google Scholar] [CrossRef]
- Ansai, J.H.; Andrade, L.P.; Nakagawa, T.H.; Rebelatto, J.R. Performances on the Timed Up and Go Test and subtasks between fallers and non-fallers in older adults with cognitive impairment. Arq. Neuropsiquiatr. 2018, 76, 381–386. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Zanetti, M.; Gortan Cappellari, G.; Ratti, C.; Ceschia, G.; Murena, L.; De Colle, P.; Barazzoni, R. Poor nutritional status but not cognitive or functional impairment per se independently predict 1 year mortality in elderly patients with hip-fracture. Clin. Nutr. 2019, 38, 1607–1612. [Google Scholar] [CrossRef]
- Seesen, M.; Sirikul, W.; Ruangsuriya, J.; Griffiths, J.; Siviroj, P. Cognitive Frailty in Thai Community-Dwelling Elderly: Prevalence and Its Association with Malnutrition. Nutrients 2021, 13, 4239. [Google Scholar] [CrossRef] [PubMed]
- Pashmdarfard, M.; Azad, A. Assessment tools to evaluate Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) in older adults: A systematic review. Med. J. Islam. Repub. Iran 2020, 34, 33. [Google Scholar] [CrossRef] [PubMed]
- Katayama, O.; Lee, S.; Bae, S.; Makino, K.; Shinkai, Y.; Chiba, I.; Harada, K.; Shimada, H. Lifestyle changes and outcomes of older adults with mild cognitive impairment: A 4-year longitudinal study. Arch. Gerontol. Geriatr. 2021, 94, 104376. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-T.; Jang, Y.; Chang, W.-Y. How do impairments in cognitive functions affect activities of daily living functions in older adults? PLoS ONE 2019, 14, e0218112. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Ownby, R.L.; Crocco, E.; Acevedo, A.; John, V.; Loewenstein, D. Depression and risk for Alzheimer disease: Systematic review, meta-analysis, and metaregression analysis. Arch. Gen. Psychiatry 2006, 63, 530–538. [Google Scholar] [CrossRef]
- Jiang, R.; Westwater, M.L.; Noble, S.; Rosenblatt, M.; Dai, W.; Qi, S.; Sui, J.; Calhoun, V.D.; Scheinost, D. Associations between grip strength, brain structure, and mental health in >40,000 participants from the UK Biobank. BMC Med. 2022, 20, 286. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Chien, M.Y.; Chen, H.C. Poor sleep quality is independently associated with physical disability in older adults. J. Clin. Sleep Med. 2015, 11, 225–232. [Google Scholar] [CrossRef]
- Brown, L.; Mossabir, R.; Harrison, N.; Brundle, C.; Smith, J.; Clegg, A. Life in lockdown: A telephone survey to investigate the impact of COVID-19 lockdown measures on the lives of older people (≥75 years). Age Ageing 2021, 50, 341–346. [Google Scholar] [CrossRef]
- Yamada, K.; Yamaguchi, S.; Sato, K.; Fuji, T.; Ohe, T. The COVID-19 outbreak limits physical activities and increases sedentary behavior: A possible secondary public health crisis for the elderly. J. Orthop. Sci. 2020, 25, 1093–1094. [Google Scholar] [CrossRef]
- Pagano, A.F.; Brioche, T.; Arc-Chagnaud, C.; Demangel, R.; Chopard, A.; Py, G. Short-term disuse promotes fatty acid infiltration into skeletal muscle. J. Cachexia Sarcopenia Muscle 2018, 9, 335–347. [Google Scholar] [CrossRef]
- World Health Organization. WHO Health Emergengy Dash Board. WHO (COVID-19) Thailand Situation. Available online: https://covid19.who.int/region/searo/country/th (accessed on 16 December 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Center of Disease Control and Prevention. Epi Info™ for Mobile Devices. 2022. Available online: https://www.cdc.gov/epiinfo/mobile.html (accessed on 16 December 2022).
- Chye, L.; Wei, K.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.P. Strong Relationship between Malnutrition and Cognitive Frailty in the Singapore Longitudinal Ageing Studies (SLAS-1 and SLAS-2). J. Prev. Alzheimer’s Dis. 2018, 5, 142–148. [Google Scholar] [CrossRef]
- Tantiritsak, T. (Ed.) Clinical Practice Guidelines: Dementia; Tana Press: Bangkok, Thailand, 2014. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T. Prevalence of major depressive disorders in long-term care facilities: A report northern Thailand. Psychogeriatrics 2012, 12, 11–17. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Methipisit, T.; Mungthin, M.; Saengwanitch, S.; Ruangkana, P.; Chinwarun, Y.; Ruangkanchanasetr, P.; Panichkul, S.; Ukritchon, S.; Mahakit, P.; Sithinamsuwan, P. The Development of Sleep Questionnaires Thai Version (ESS, SA-SDQ, and PSQI): Linguistic Validation, Reliability Analysis and Cut-Off Level to Determine Sleep Related Problems in Thai Population. J. Med. Assoc. Thai 2016, 99, 893–903. [Google Scholar]
- Fox, B.; Henwood, T.; Schaap, L.; Bruyère, O.; Reginster, J.Y.; Beaudart, C.; Buckinx, F.; Roberts, H.; Cooper, C.; Cherubini, A. Adherence to a standardized protocol for measuring grip strength and appropriate cut-off values in adults over 65 years with sarcopenia: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 50–59. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.T.; Bloch, M.L.; Jønsson, L.R.; Jakobsen, T.L. Interrater reliability of the standardized Timed Up and Go Test when used in hospitalized and community-dwelling older individuals. Physiother. Res. Int. 2019, 24, e1769. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Dunne, R.A.; Aarsland, D.; O’Brien, J.T.; Ballard, C.; Banerjee, S.; Fox, N.C.; Isaacs, J.D.; Underwood, B.R.; Perry, R.J.; Chan, D.; et al. Mild Cognitive Impairment: The Manchester consensus. Age Ageing 2020, 50, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef]
- Cooper, C.; Hardy, R.; Aihie Sayer, A.; Ben-Shlomo, Y.; Birnie, K.; Cooper, C.; Kuh, D.; Craig, L.; Deary, I.J.; Demakakos, P.; et al. Age and gender differences in physical capability levels from mid-life onwards: The harmonisation and meta-analysis of data from eight UK cohort studies. PLoS ONE 2011, 6, e27899. [Google Scholar] [CrossRef]
- Ma, L. Depression, Anxiety, and Apathy in Mild Cognitive Impairment: Current Perspectives. Front. Aging Neurosci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Fastame, M.C.; Mulas, I.; Putzu, V.; Asoni, G.; Viale, D.; Mameli, I.; Pau, M. Executive and Motor Functions in Older Individuals with Cognitive Impairment. Behav. Sci. 2022, 12, 214. [Google Scholar] [CrossRef]
- Kim, K.H.; Park, S.K.; Lee, D.R.; Lee, J. The Relationship between Handgrip Strength and Cognitive Function in Elderly Koreans over 8 Years: A Prospective Population-Based Study Using Korean Longitudinal Study of Ageing. Korean J. Fam. Med. 2019, 40, 9–15. [Google Scholar] [CrossRef]
- Jang, J.Y.; Kim, J. Association between handgrip strength and cognitive impairment in elderly Koreans: A population-based cross-sectional study. J. Phys. Ther. Sci. 2015, 27, 3911–3915. [Google Scholar] [CrossRef]
- Zammit, A.R.; Piccinin, A.M.; Duggan, E.C.; Koval, A.; Clouston, S.; Robitaille, A.; Brown, C.L.; Handschuh, P.; Wu, C.; Jarry, V.; et al. A Coordinated Multi-study Analysis of the Longitudinal Association Between Handgrip Strength and Cognitive Function in Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 229–241. [Google Scholar] [CrossRef]
- Duchowny, K.A.; Ackley, S.F.; Brenowitz, W.D.; Wang, J.; Zimmerman, S.C.; Caunca, M.R.; Glymour, M.M. Associations Between Handgrip Strength and Dementia Risk, Cognition, and Neuroimaging Outcomes in the UK Biobank Cohort Study. JAMA Netw. Open 2022, 5, e2218314. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Isiozor, N.M.; Voutilainen, A.; Laukkanen, J.A. Handgrip strength and risk of cognitive outcomes: New prospective study and meta-analysis of 16 observational cohort studies. GeroScience 2022, 44, 2007–2024. [Google Scholar] [CrossRef]
- Herold, F.; Labott, B.K.; Grässler, B.; Halfpaap, N.; Langhans, C.; Müller, P.; Ammar, A.; Dordevic, M.; Hökelmann, A.; Müller, N.G. A Link between Handgrip Strength and Executive Functioning: A Cross-Sectional Study in Older Adults with Mild Cognitive Impairment and Healthy Controls. Healthcare 2022, 10, 230. [Google Scholar] [CrossRef]
- Williams, J.M.; Nyman, S.R. Association between the instrumented timed up and go test and cognitive function, fear of falling and quality of life in community dwelling people with dementia. J. Frailty Sarcopenia Falls 2018, 3, 185–193. [Google Scholar] [CrossRef]
- Ibrahim, A.; Singh, D.K.A.; Shahar, S. ‘Timed Up and Go’ test: Age, gender and cognitive impairment stratified normative values of older adults. PLoS ONE 2017, 12, e0185641. [Google Scholar] [CrossRef]
- Muir, S.W.; Beauchet, O.; Montero-Odasso, M.; Annweiler, C.; Fantino, B.; Speechley, M. Association of executive function impairment, history of falls and physical performance in older adults: A cross-sectional population-based study in eastern France. J. Nutr. Health Aging 2013, 17, 661–665. [Google Scholar] [CrossRef]
- Van Uem, J.M.T.; Walgaard, S.; Ainsworth, E.; Hasmann, S.E.; Heger, T.; Nussbaum, S.; Markus, A.; Hobert, M.A.; Encarnación, M.; Micó-Amigo, E.M.; et al. Quantitative Timed-Up-and-Go Parameters in Relation to Cognitive Parameters and Health-Related Quality of Life in Mild-to-Moderate Parkinson’s Disease. PLoS ONE 2016, 11, e0151997. [Google Scholar] [CrossRef]
- Doi, T.; Makizako, H.; Shimada, H.; Yoshida, D.; Ito, K.; Kato, T.; Ando, H.; Suzuki, T. Brain atrophy and trunk stability during dual-task walking among older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 790–795. [Google Scholar] [CrossRef]
- Kilgour, A.H.M.; Todd, O.M.; Starr, J.M. A systematic review of the evidence that brain structure is related to muscle structure and their relationship to brain and muscle function in humans over the lifecourse. BMC Geriatr. 2014, 14, 85. [Google Scholar] [CrossRef]
- Holtzer, R.; Epstein, N.; Mahoney, J.R.; Izzetoglu, M.; Blumen, H.M. Neuroimaging of mobility in aging: A targeted review. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1375–1388. [Google Scholar] [CrossRef] [PubMed]
- Belghali, M.; Chastan, N.; Cignetti, F.; Davenne, D.; Decker, L.M. Loss of gait control assessed by cognitive-motor dual-tasks: Pros and cons in detecting people at risk of developing Alzheimer’s and Parkinson’s diseases. Geroscience 2017, 39, 305–329. [Google Scholar] [CrossRef] [PubMed]
- Buracchio, T.; Dodge, H.H.; Howieson, D.; Wasserman, D.; Kaye, J. The trajectory of gait speed preceding mild cognitive impairment. Arch. Neurol. 2010, 67, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Lekamwasam, R.; Lekamwasam, S. Effects of COVID-19 Pandemic on Health and Wellbeing of Older People: A Comprehensive Review. Ann. Geriatr. Med. Res. 2020, 24, 166–172. [Google Scholar] [CrossRef]
- Lebrasseur, A.; Fortin-Bédard, N.; Lettre, J.; Raymond, E.; Bussières, E.L.; Lapierre, N.; Faieta, J.; Vincent, C.; Duchesne, L.; Ouellet, M.C.; et al. Impact of the COVID-19 Pandemic on Older Adults: Rapid Review. JMIR Aging 2021, 4, e26474. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | n (%) | p-Value | ||
|---|---|---|---|---|
| Total (n = 464) | Non-MCI (n = 66) | MCI (n = 398) | ||
| Age (years), mean ±SD | 70.67 ± 5.59 | 68.18 ± 3.10 | 71.09 ± 5.81 | |
| 65–69 | 245 (53.0) | 52 (78.8) | 193 (48.7) | <0.001 a |
| 70–79 | 170 (36.8) | 14 (12.2) | 156 (39.4) | |
| ≥80 | 47 (10.2) | 0 (0.0) | 47 (11.9) | |
| Sex | ||||
| Male | 193 (41.6) | 31 (47.0) | 162 (40.7) | 0.348 a |
| Female | 271 (58.4) | 35 (53.0) | 236 (59.3) | |
| Marital status | ||||
| Married | 283 (61.0) | 49 (74.2) | 234 (58.8) | 0.020 a |
| Single/divorced/widowed | 181 (39.0) | 17 (25.8) | 164 (41.2) | |
| Education level | ||||
| No education | 13 (2.8) | 2 (3.0) | 11 (2.8) | <0.001 a |
| Primary school (1–3 years) | 170 (36.6) | 18 (27.3) | 152 (38.2) | |
| Primary school (4–6 years) | 231 (49.8) | 22 (33.3) | 209 (45.0) | |
| Secondary school (12 years) | 34 (7.3) | 15 (22.7) | 19 (4.8) | |
| Bachelor’s degree (>12 years) | 16 (3.4) | 9 (13.6) | 7 (1.8) | |
| Living status, alone | 58 (12.5) | 7 (10.6) | 51 (12.8) | 0.693 a |
| Current smoking | 32 (6.9) | 4 (6.1) | 28 (7.1) | 0.713 a |
| Current drinking | 69 (14.9) | 15 (22.7) | 54 (13.6) | 0.062 a |
| Numbers of chronic diseases | ||||
| 0 | 134 (28.9) | 19 (28.8) | 115 (85.8) | 0.944 a |
| 1–2 | 275 (59.3) | 40 (60.6) | 235 (85.5) | |
| ≥3 | 55 (11.8) | 7 (10.6) | 48 (12.1) | |
| Hypertension | 237 (51.1) | 31 (47.0) | 206 (51.8) | 0.508 a |
| Dyslipidemia | 79 (17.0) | 12 (18.2) | 67 (16.8) | 0.860 a |
| Type 2 Diabetes mellitus | 78 (16.8) | 13 (19.7) | 65 (16.3) | 0.594 a |
| Gout | 20 (4.3) | 4 (6.1) | 16 (4.0) | 0.507 a |
| Coronary heart disease | 18 (3.9) | 3 (4.5) | 15 (3.8) | 0.762 a |
| Asthma | 15 (3.2) | 2 (3.0) | 13 (3.3) | 1.000 a |
| Stroke | 14 (3.0) | 2 (3.0) | 12 (3.0) | 1.000 a |
| Chronic kidney disease | 12 (2.6) | 1 (1.5) | 11 (2.8) | 0.708 a |
| COPD | 7 (1.5) | 0 (0.0) | 7 (1.5) | 0.600 a |
| MNA-SF (points), median [IQR] | 10.15 ± 2.04 | 10.48 ± 1.73 | 10.18 ± 2.04 | |
| Normal | 138 (29.7) | 21 (31.8) | 117 (29.4) | 0.527 a |
| At risk of malnutrition | 271 (58.4) | 40 (60.6) | 231 (58.0) | |
| Malnourished | 55 (11.9) | 5 (7.6) | 50 (12.6) | |
| BMI, median [IQR] | 22.75 ± 3.92 | 23.63 ± 4.46 | 22.61 ± 3.80 | |
| Underweight (<18.5 kg/m2) | 54 (12.2) | 5 (7.6) | 49 (13.0) | 0.402 a |
| Normal weight (18.5–22.9 kg/m2) | 191 (43.0) | 27 (40.9) | 164 (43.4) | |
| Overweight (23.0–24.9 kg/m2) | 89 (20.0) | 13 (19.7) | 76 (20.1) | |
| Obese (>25.0 kg/m2) | 110 (24.8) | 21 (31.8) | 89 (23.5) | |
| ADL (points), median [IQR] | 20.0 [0.0] | 20.0 [0.0] | 20.0 [0.0] | 0.147 b |
| TGDS (points), median [IQR] | 2.0 [2.0] | 1.0 [3.0] | 2.0 [2.0] | |
| Depression | 61 (13.1) | 4 (6.6) | 57 (93.4) | 1.000 a |
| PSQI (points), median [IQR] | 5.0 [3.0] | 8.0 [2.5] | 8.0 [3.0] | |
| Sleep quality, bad | 231 (49.8) | 34 (14.7) | 197 (85.3) | 0.865 a |
| Parameters | Mean ±SD, Median [IQR] | p-Value | |||||
|---|---|---|---|---|---|---|---|
| n | Total (n = 464) | n | Non-MCI (n = 66, 14.2%) | n | MCI (n = 398, 85.8%) | ||
| MoCA-B scores | 464 | 19.35 ± 4.86 20.00 [7.00] | 26.41 ± 1.40 26.00 [2.25] | 18.18 ± 4.19 19.0 [6.00] | <0.001 a | ||
| HGS (kg) | 461 | 19.91 ± 7.26, 18.60 [9.70] | 66 | 23.42 ± 8.32, 22.50 [12.52] | 395 | 19.33 ± 6.90, 17.90 [9.30] | <0.001 b |
| Male | 193 | 24.70 ± 7.49, 25.40 [11.00] | 31 | 29.80 ± 7.03, 30.00 [9.00] | 162 | 23.73 ± 7.20, 24.05 [11.20] | <0.001 b |
| Female | 268 | 16.46 ± 4.67, 16.15 [6.60] | 35 | 17.78 ± 4.36, 17.60 [5.90] | 233 | 16.26 ± 4.69, 16.00 [6.45] | 0.034 a |
| Percent HGS | 459 | 71.12 ± 25.92, 66.43 [34.64] | 66 | 83.65 ± 29.73, 80.34 [44.73] | 395 | 69.02 ± 24.66, 63.93 [33.21] | <0.001 b |
| Male | 193 | 88.23 ± 26.76, 90.71 [32.29] | 31 | 106.42 ± 25.10, 107.22 [32.14] | 162 | 84.75 ± 25.71, 85.89 [40.0] | <0.001 b |
| Female | 268 | 58.79 ± 16.69, 57.68 [23.57] | 35 | 63.49 ± 15.59, 62.85 [21.07] | 233 | 58.09 ± 16.77, 57.14 [23.04] | 0.034 a |
| TUG (s) | 459 | 12.20 ± 3.33, 11.58 [3.73] | 66 | 10.36 ± 2.53, 10.26 [3.40] | 393 | 12.50 ± 3.35, 11.79 [4.03] | <0.001 b |
| 65–69 years old | 244 | 11.38 ± 2.70, 11.03 [3.06] | 52 | 10.35 2.50, 10.26 [3.31] | 192 | 11.65 ± 2.69, 11.21 [2.95] | 0.003 a |
| 70–79 years old | 169 | 12.83 ± 3.65, 12.07 [3.96] | 14 | 10.38 ± 2.74, 10.38 [5.21] | 155 | 13.06 ± 3.65, 12.26 [4.12] | 0.012 a |
| ≥80 years old | 44 | 14.20 ± 3.61, 13.86 [4.24] | 0 | - | 44 | 14.20 ± 3.61, 13.86 [4.24] | - |
| Percent TUG | 459 | 96.03 ± 26.21, 91.18 [29.37] | 66 | 81.54 ± 19.95, 80.83 [26.77] | 393 | 98.46 ± 26.37, 92.83 [31.69] | <0.001 b |
| 65–69 years old | 244 | 89.58 ± 21.27, 86.85 [24.11] | 52 | 81.49 ± 19.71, 80.83 [26.04] | 192 | 91.77 ± 21.19, 88.31 [23.27] | 0.003 a |
| 70–79 years old | 169 | 101.06 ± 28.74, 95.04 [31.14] | 14 | 81.72 ± 21.60, 81.77 [40.98] | 155 | 102.81 ± 28.72, 96.53 [32.44] | 0.012 a |
| ≥80 years old | 44 | 111.83 ± 28.44, 109.13 [33.37] | 0 | - | 44 | 111.83 ± 28.44, 109.13 [33.37] | - |
| Variables | β | 95% CI | p-Value |
|---|---|---|---|
| Age ≥80 years | −2.987 | −4.424 to −1.550 | <0.001 ** |
| Sex, Female | −0.630 | −1.529 to 0.268 | 0.169 |
| Marital status, single/divorced/widowed | −1.004 | −1.909 to −0.99 | 0.030 * |
| Education level, above secondary school | 4.139 | 2.759 to 5.519 | <0.001 ** |
| Living status, alone | −0.495 | −1.836 to 0.846 | 0.468 |
| Number of chronic diseases | 0.066 | −0.343 to 0.474 | 0.752 |
| Mini Nutritional Assessment-Short Form, MNA-SF (score) | 0.137 | 0.110 to 0.541 | 0.003 * |
| Activities of Daily Living, ADL (score) | 0.351 | −0.155 to 0.856 | 0.174 |
| Thai Geriatric Depression Scale, TGDS (score) | −0.404 | −0.607 to −0.202 | <0.001 ** |
| Global Pittsburgh Sleep Quality Index, PSQI (score) | 0.001 | −0.180 to 0.183 | 0.990 |
| Percent Handgrip Strength, %HGS | 0.053 | 0.036 to 0.069 | < 0.001 ** |
| Percent Timed Up-and-Go, %TUG | −0.047 | −0.063 to −0.031 | <0.001 ** |
| Variables | β | 95% CI | p-Value |
|---|---|---|---|
| Percent Handgrip strength, % HGS | 0.032 | 0.015 to 0.048 | <0.001 ** |
| Education level, above secondary school | 2.801 | 1.464 to 4.138 | <0.001 ** |
| Percent Timed Up-and-Go, %TUG | −0.022 | −0.039 to −0.005 | 0.013 * |
| Thai Geriatric Depression Scale, TGDS (point) | −0.248 | −0.440 to −0.057 | 0.011 * |
| Age ≥80 years | −1.677 | −3.080 to −0.273 | 0.019 * |
| Constant: Beta = 18.642; 95% CI = 15.514 to 21.770; p < 0.001 ** | |||
| R squared = 0.164; Adjusted R squared = 0.155; F = 17.627; p < 0.001 ** | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griffiths, J.; Seesen, M.; Sirikul, W.; Siviroj, P. The Relationship between Handgrip Strength, Timed Up-and-Go, and Mild Cognitive Impairment in Older People during COVID-19 Pandemic Restrictions. Behav. Sci. 2023, 13, 410. https://doi.org/10.3390/bs13050410
Griffiths J, Seesen M, Sirikul W, Siviroj P. The Relationship between Handgrip Strength, Timed Up-and-Go, and Mild Cognitive Impairment in Older People during COVID-19 Pandemic Restrictions. Behavioral Sciences. 2023; 13(5):410. https://doi.org/10.3390/bs13050410
Chicago/Turabian StyleGriffiths, Jiranan, Mathuramat Seesen, Wachiranun Sirikul, and Penprapa Siviroj. 2023. "The Relationship between Handgrip Strength, Timed Up-and-Go, and Mild Cognitive Impairment in Older People during COVID-19 Pandemic Restrictions" Behavioral Sciences 13, no. 5: 410. https://doi.org/10.3390/bs13050410
APA StyleGriffiths, J., Seesen, M., Sirikul, W., & Siviroj, P. (2023). The Relationship between Handgrip Strength, Timed Up-and-Go, and Mild Cognitive Impairment in Older People during COVID-19 Pandemic Restrictions. Behavioral Sciences, 13(5), 410. https://doi.org/10.3390/bs13050410