

Needs of Family Caregivers of People with Lower Limb Amputations: A Scoping Review

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Deviations from the Protocol
2.2. Inclusion Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Data Analyses and Presentation
3. Results
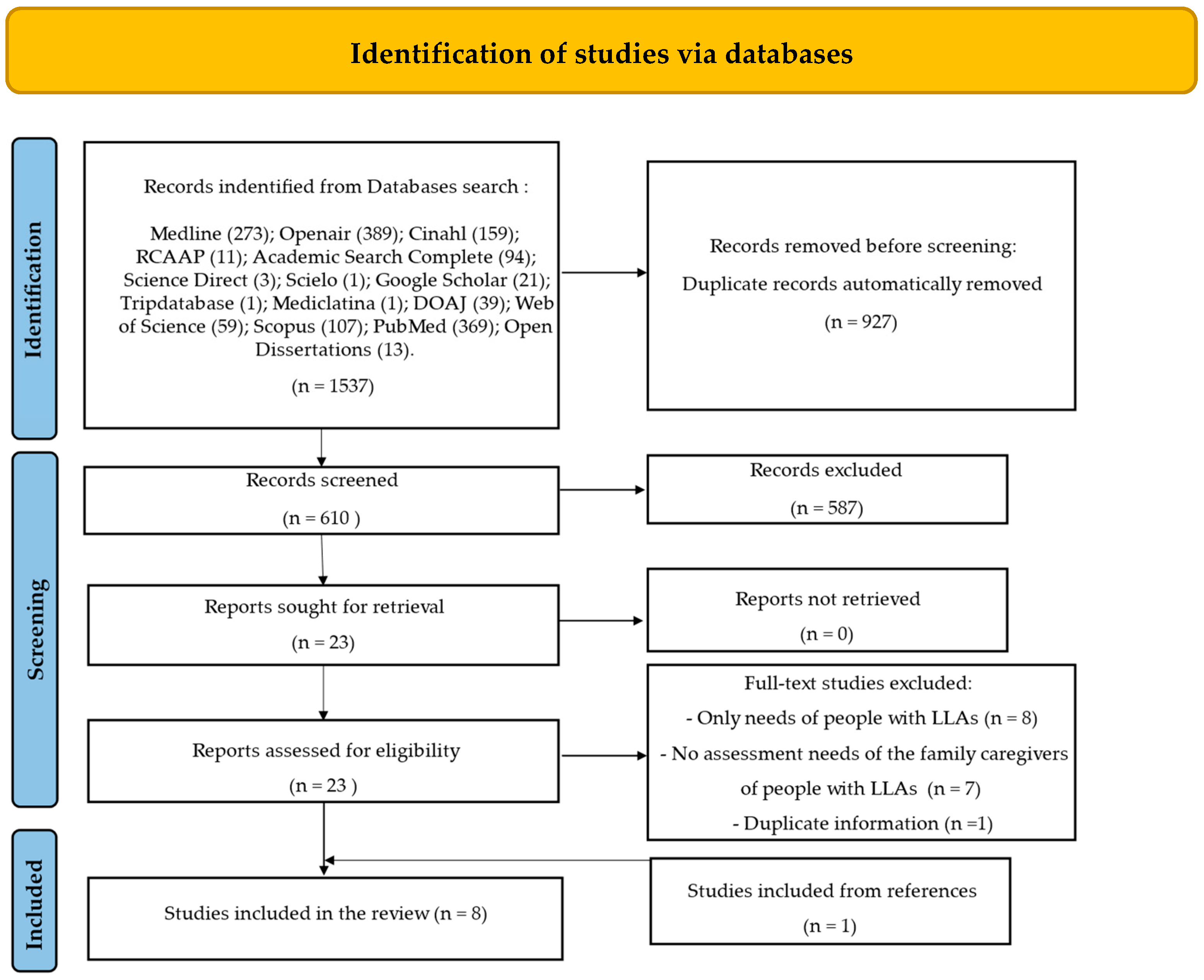
3.1. Study Inclusion
3.2. Characteristics of Included Studies
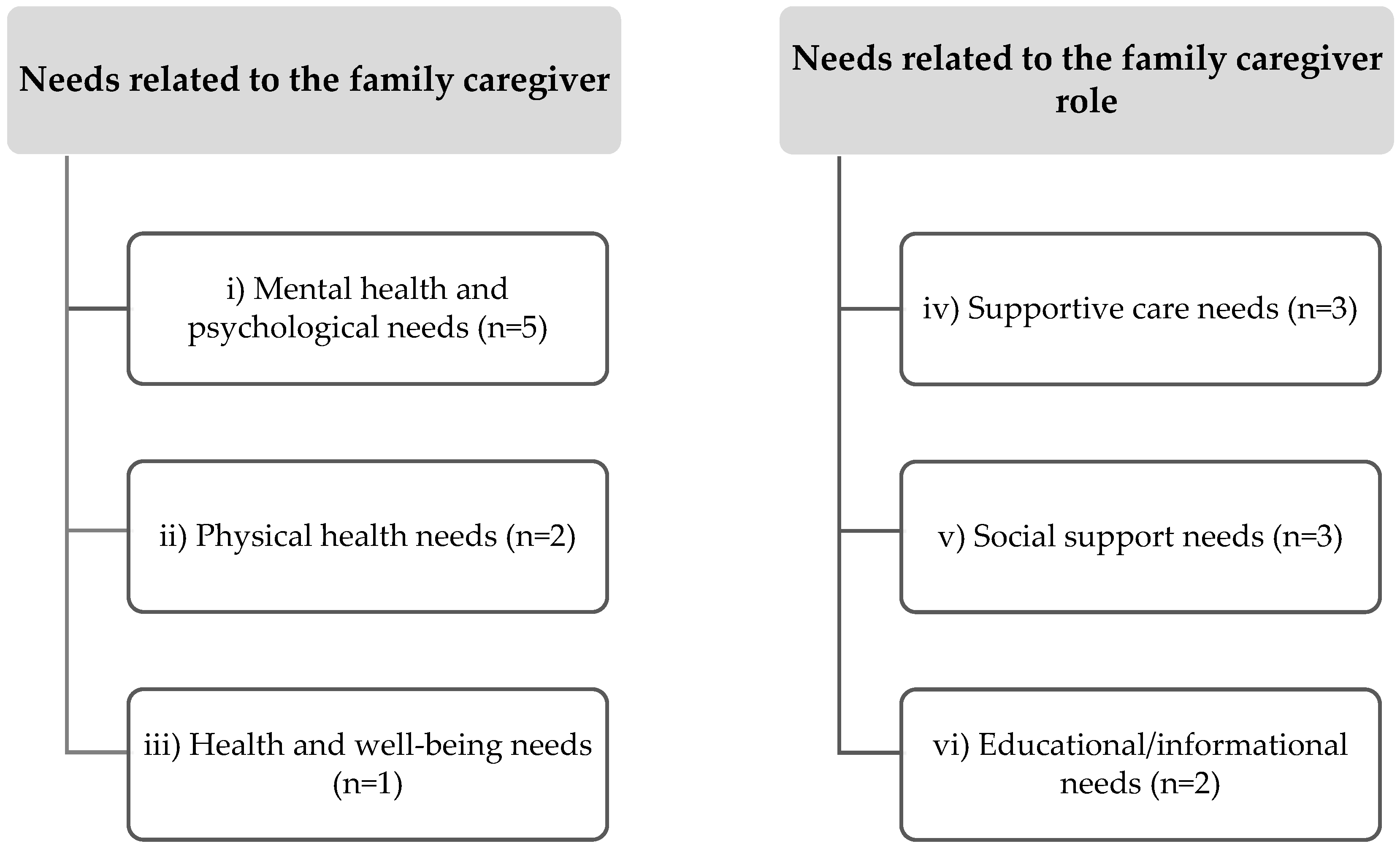
3.3. Summary of Results
3.3.1. Mental Health and Psychological Support Needs of FCs of People with LLAs
3.3.2. Physical Health Needs of FCs of People with LLAs
3.3.3. Health and Well-Being Needs of FCs of People with LLAs
3.3.4. Supportive Care Needs of Family Caregivers of People with LLAs
3.3.5. Social Support Needs of FCs of People with LLAs
3.3.6. Educational/Informational Needs of FCs of People with LLAs
4. Discussion
4.1. Limitations
4.2. Implications for Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De-Rosende Celeiro, I.; Simón Sanjuán, L.; Santos-Del-Riego, S. Activities of daily living in people with lower limb amputation: Outcomes of an intervention to reduce dependence in pre-prosthetic phase. Disabil. Rehabil. 2017, 39, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Fatima, S.Z. Life of an amputee: Predictors of quality of life after lower limb amputation. Wien. Med. Wochenschr. 2023, 173, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Alessa, M.; Alkhalaf, H.A.; Alwabari, S.S.; Alwabari, N.J.; Alkhalaf, H.; Alwayel, Z.; Almoaibed, F. The Psychosocial Impact of Lower Limb Amputation on Patients and Caregivers. Cureus 2022, 14, e31248. [Google Scholar] [CrossRef] [PubMed]
- Ousey, K.; Edward, K.L.; Lui, S. Identifying and exploring physical and psychological morbidity and patient and family caregiver resilience following acute wound development and/or wound blistering post orthopaedic surgery: A systematic review. Int. Wond J. 2015, 12, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Moradi, A.; Ebrahimzadeh, M.H.; Soroush, M.R. Quality of life of caregiver spouses of veterans with bilateral lower extremity amputations. Trauma Mon. 2015, 20, e21891. [Google Scholar] [CrossRef] [PubMed]
- Çamur, S.; Batıbay, S.G.; Bayram, S. Effect of lower extremity amputation on caregiving burden in caregivers of patients with diabetic foot: Prospective cohort study. Int. Wound J. 2020, 17, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Bom, J.; Bakx, P.; Schut, F.; Van Doorslaer, E. The impact of informal caregiving for older adults on the health of various types of caregivers: A systematic review. Gerontologist 2019, 59, e629–e642. [Google Scholar] [CrossRef] [PubMed]
- Messenger, G.; Taha, N.; Sabau, S.; Alhubail, A.; Albibbiat, A.M. Is there a Role for Informal Caregivers in the Management of Diabetic Foot Ulcers? A Narrative Review. Diabetes Ther. 2019, 10, 2025–2033. [Google Scholar] [CrossRef]
- Given, B.; Sherwood, P.R.; Given, C.W. What knowledge and skills do caregivers need? Am. J. Nurs. 2008, 108, 28–34. [Google Scholar] [CrossRef]
- Family Caregiver Alliance. 2020. Available online: http://www.caergiver.org/ (accessed on 12 November 2023).
- Abdallah Abdel-Mordy, M.; Abd El-Mordy Elsayed, E.; Sadek Abd El-Hammed, H.; Mohamed Sobhy Elsayed, D. Awareness of Caregivers regarding Care of Patients with Post Diabetic Foot Amputation. J. Nurs. Sci. Benha Univ. 2022, 3, 1042–1062. [Google Scholar] [CrossRef]
- Antunes, P.; Marques, P. Transition to the family caregiver role in Portugal. Porto Biomed. J. 2017, 2, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Broese van Groenou, M.I.; De Boer, A. Providing informal care in a changing society. Eur. J. Ageing 2016, 13, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Mollica, M.A.; Smith, A.W.; Kent, E.E. Caregiving tasks and unmet supportive care needs of family caregivers: A U.S. population-based study. Patient Educ. Couns. 2020, 103, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Calvó-Perxas, L.; Vilalta-Franch, J.; Litwin, H.; Turró-Garriga, O.; Mira, P.; Garre-Olmo, J. What seems to matter in public policy and the health of informal caregivers? A cross-sectional study in 12 European countries. PLoS ONE 2018, 13, e0194232. [Google Scholar] [CrossRef] [PubMed]
- Plöthner, M.; Schmidt, K.; de Jong, L.; Zeidler, J.; Damm, K. Needs and preferences of informal caregivers regarding outpatient care for the elderly: A systematic literature review. BMC Geriatr. 2019, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Dixe, M.D.A.; Soares, E.; Martinho, R.; Rijo, R.; Caroço, J.; Gomes, N.; Querido, A. Informal Caregiver Empowerment Model for Caring for the Person with Dependency, 1st ed.; ciTechCare: Leiria, Portugal, 2020; p. 52. [Google Scholar]
- Da Costa, A.F.; Lopes, M.C.B.T.; Campanharo, C.R.V.; Batista, R.E.A.; Okuno, M.F.P. Quality of life and burden of caregivers of elderly people. Texto Contexto-Enferm. 2020, 29, e20190043. [Google Scholar] [CrossRef]
- Biliunaite, I.; Kazlauskas, E.; Sanderman, R.; Andersson, G. Informal caregiver support needs and burden: A survey in Lithuania. BMJ Open 2022, 12, e054607. [Google Scholar] [CrossRef] [PubMed]
- Dixe, M.D.A.C.R.; da Conceição Teixeira, L.F.; Areosa, T.J.T.C.C.; Frontini, R.C.; de Jesus Almeida Peralta, T.; Querido, A.I.F. Needs and skills of informal caregivers to care for a dependent person: A cross-sectional study. BMC Geriatr. 2019, 19, 255. [Google Scholar] [CrossRef] [PubMed]
- Cloyes, K.G.; Hart, S.E.; Jones, A.K.; Ellington, L. Where are the family caregivers? Finding family caregiver-related content in foundational nursing documents. J. Prof. Nurs. Off. J. Am. Assoc. Coll. Nurs. 2020, 36, 76–84. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Volume 18, pp. 2119–2126. [Google Scholar]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Khalil, H.; Larsen, P.; Marnie, C.; Pollock, D.; Tricco, A.C.; Munn, Z. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid. Synth. 2022, 20, 953–968. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.; Castanheira, S.; Carvalho, L.; Barroso, C. Needs of family caregivers of the person with lower limb amputation: Scoping review protocol. Millenium-J. Educ. Technol. Health 2023, 2, e28570. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Costa, S.; Ferreira, J.; Leite, Â.; Pereira, M.G. Traumatic stress as a mediator of quality of life and burden in informal caregivers of amputees due to diabetic foot: A longitudinal study. Health Psychol. Rep. 2021, 9, 338–348. [Google Scholar] [CrossRef]
- Costa, M.S.A.; Machado, J.C.; Pereira, M.G. Longitudinal changes on the quality of life in caregivers of type 2 diabetes amputee patients. Scand. J. Caring Sci. 2020, 34, 979–988. [Google Scholar] [CrossRef]
- Costa, M.S.A.; Machado, J.C.; Pereira, M.G. Burden changes in caregivers of patients with type 2 diabetes: A longitudinal study. J. Adv. Nurs. 2018, 74, 2322–2330. [Google Scholar] [CrossRef]
- Tsoulou, V.; Karamolegou, E.; Kourakos, M.; Vasilopoulos, G.; Polikandrioti, M. Association of State and Trait Anxiety Between Patients Who Had Undergone Traumatic Amputation and Their Family Caregivers. Int. J. Low. Extrem. Wounds 2019, 18, 176–185. [Google Scholar] [CrossRef]
- Ganjparvar, Z.; Mousavi, B.; Masumi, M.; Soroush, M.; Montazeri, A. Determinants of Quality of Life in the Caregivers of Iranian War Survivors with Bilateral Lower-Limb Amputation after More than Two Decades. Iran. J. Med. Sci. 2016, 41, 257–264. [Google Scholar]
- Foss, M.H.D.; Martins, M.R.I.; Martins, M.I.D.; Godoy, J.M.P. Qualidade de vida dos cuidadores de amputados de membros inferiores. Rev. Neurociênc. 2009, 17, 8–13. [Google Scholar] [CrossRef]
- Bennett, J. Limb loss: The unspoken psychological aspect. J. Vasc. Nurs. 2016, 34, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Latlief, G.; Elnitsky, C.; Hart-Hughes, S.; Phillips, S.L.; Adams-Koss, L.; Kent, R.; Highsmith, M.J. Patient safety in the rehabilitation of the adult with an amputation. Phys. Med. Rehabil. Clin. N. Am. 2012, 23, 377–392. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Mazanec, S.R.; Voss, J.G. Needs of Informal Caregivers of Patients with Head and Neck Cancer: A Systematic Review. Oncol. Nurs. Forum 2021, 48, 11–29. [Google Scholar] [CrossRef] [PubMed]
- Hunt, G.; Longacre, M.; Kent, E.; Weber-Raley, L. Cancer caregiving in the US: An intense, episodic, and challenging care experience. Natl. Alliance Caregiving 2016, 2016, 34. [Google Scholar]
- Schulz, R.; Beach, S.R.; Friedman, E.M.; Martsolf, G.R.; Rodakowski, J.; James, A.E., III. Changing structures and processes to support family caregivers of seriously ill patients. J. Palliat. Med. 2018, 21 (Suppl. S2), S-36. [Google Scholar] [CrossRef] [PubMed]
- Amoah, P.A. The relationship between functional health literacy, self-rated health, and social support between younger and older adults in Ghana. Int. J. Environ. Res. Public Health 2019, 16, 3188. [Google Scholar] [CrossRef]
- Makhtar, A.; Ab Ghani, N.N.; Syed Elias, S.M.; Mohamed Ludin, S. Social support and associated factors among family caregivers of older people in North-East Peninsular Malaysia. Belitung Nurs. J. 2023, 9, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Abu Bakar, S.H.; Weatherley, R.; Omar, N.; Abdullah, F.; Mohamad Aun, N.S. Projecting social support needs of informal caregivers in Malaysia. Health Soc. Car Community 2014, 22, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Domínguez Guedea, M.T.; Damacena, F.A.; Montiel Carbajal, M.M.; Ochoa Marcobich, P.; Álvarez Hernández, G.; Valdéz Lizárraga, L.; Ibarra Flores, E. Necessidades de apoio social em cuidadores de familiares idosos mexicanos. Psicol. Soc. 2009, 21, 242–249. [Google Scholar] [CrossRef]
- Maguire, R.; Hanly, P.; Maguire, P. Beyond care burden: Associations between positive psychological appraisals and well-being among informal caregivers in Europe. Qual. Life Res. 2019, 28, 2135–2146. [Google Scholar] [CrossRef]
- Moreira, A.C.A.; Silva, M.J.D.; Darder, J.J.T.; Coutinho, J.F.V.; Vasconcelos, M.I.O.; Marques, M.B. Effectiveness of an educational intervention on knowledge-attitude-practice of older adults’ caregivers. Rev. Bras. Enferm. 2018, 71, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Azizi, A.; Khatiban, M.; Mollai, Z.; Mohammadi, Y. Effect of informational support on anxiety in family caregivers of patients with hemiplegic stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105020. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family Caregiving for Older Adults. Annu. Rev. Psychol. 2020, 71, 635–659. [Google Scholar] [CrossRef] [PubMed]
- Araújo, O.; Lage, I.; Cabrita, J.; Teixeira, L. Training informal caregivers to care for older people after stroke: A quasi-experimental study. J. Adv. Nurs. 2018, 74, 2196–2206. [Google Scholar] [CrossRef] [PubMed]
- Farahani, M.A.; Bahloli, S.; JamshidiOrak, R.; Ghaffari, F. Investigating the needs of family caregivers of older stroke patients: A longitudinal study in Iran. BMC Geriatric 2020, 20, 313. [Google Scholar] [CrossRef] [PubMed]
- Torbjörnsson, E.; Ottosson, C.; Boström, L.; Blomgren, L.; Malmstedt, J.; Fagerdahl, A.M. Health-related quality of life and prosthesis use among patients amputated due to peripheral arterial disease—A one-year follow-up. Disabil. Rehabil. 2022, 44, 2149–2157. [Google Scholar] [CrossRef] [PubMed]
- Teo, S.P. Lower Limb Amputee patients have comorbidities and risk of complications-Findings from a hospital audit. J. Rehabil. Sci. Res. 2020, 7, 60–65. [Google Scholar]
- Pohjolainen, T.; Alaranta, H.; Kärkkäinen, M. Prosthetic use and functional and social outcome following major lower limb amputation. Prosthet. Orthot. Int. 1990, 14, 75–79. [Google Scholar] [CrossRef]
- Asano, M.; Rushton, P.; Miller, W.C.; Deathe, B.A. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet. Orthot. Int. 2008, 32, 231–243. [Google Scholar] [CrossRef]
- Akodu, B.A.; Ugochukwu, S.N.; Eyitayo, O.A.; Abiola, A. Amputation Characteristics, Caregiver Support and Psychosocial Effect of Amputation among Adult Amputees at Tertiary Hospitals in Lagos Nigeria. West Afr. J. Med. 2020, 37, 537–547. [Google Scholar]
- Fard, B.; Geertzen, J.H.B.; Dijkstra, P.U. Return home after dysvascular major amputation of the lower limb: A multicentre observational study in the Netherlands. J. Rehabil. Med. 2020, 52, jrm00008. [Google Scholar] [CrossRef]
- Zhu, X.; Lee, M.; Chew, E.A.; Goh, L.J.; Dong, L.; Bartlam, B. “When nothing happens, nobody is afraid!” beliefs and perceptions around self-care and health-seeking behaviours: Voices of patients living with diabetic lower extremity amputation in primary care. Int. Wound J. 2021, 18, 850–861. [Google Scholar] [CrossRef]
- Zambrano Vásquez, J.L. Fisioterapia en la Calidad de Vida y Discapacidad de Pacientes Con Prótesis Por Amputación de Miembro Inferior. Master’s Thesis, Universidade da Coruña, A Coruña, Spain, 2021. [Google Scholar]
- Brier, M.J.; Williams, R.M.; Turner, A.P.; Henderson, A.W.; Roepke, A.M.; Norvell, D.C.; Henson, H.; Czerniecki, J.M. Quality of Relationships with Caregivers, Depression, and Life Satisfaction After Dysvascular Lower Extremity Amputation. Arch. Phys. Med. Rehabil. 2018, 99, 452–458. [Google Scholar] [CrossRef]
- Donohue, S.J. Lower limb amputation. 3: The role of the nurse. Br. J. Nurs. 1997, 6, 1171–1191. [Google Scholar] [CrossRef]
- Køberl, S.; Schrøder, K.; Dall-Hansen, D.; Abrahamsen, C. From hospital to home following a lower limb amputation: A focus group study of healthcare professionals’ views and experiences with transitioning. Int. J. Orthop. Trauma Nurs. 2023, 49, 101003. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.; Andrews, L.; Engward, H. Examining the effects of acquired limb loss on the family network: A grounded theory study. Disabil. Rehabil. 2020, 44, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.S.A. Qualidade de Vida Nos Cuidadores de Pacientes Diabéticos Tipo 2 Amputados: Um Estudo Longitudinal. Ph.D. Thesis, Universidade do Minho, Braga, Portugal, 2017. [Google Scholar]



{kind=link}
{kind=link}
| Author(s) (Year), Country | Methodology | Participants Study Context | Identified Needs | Main Conclusions |
|---|---|---|---|---|
| Costa et al. (2021) [28], Portugal | Longitudinal Study (Quantitative) | 110 family caregivers of people with diabetic foot amputations (1 month after amputation); 101 family caregivers (7 months after amputation); 84 family caregivers (up to 10 months after amputation); Living at home | (i) Mental health and psychological needs (iv) Supportive care needs (v) Social support needs | Family caregivers show signs of stress during the first month after patient’s amputation. Traumatic stress mediates the relationship between caregiver stress and mental QoL, emphasizing the importance of mental health in the family caregiver. Family caregivers need help in caregiving, especially 1 month after amputation, because of the increase in caregiving burden. Between 1 and 7 months after amputation, family caregivers show signs of traumatic stress with negative consequences in caregiving, needing social support in caregiving to help them with the increase traumatic stress in this period. |
| Costa et al. (2020) [29], Portugal | Longitudinal Study (Quantitative) | 110 family caregivers of people with diabetic foot amputations (1 month after amputation); 101 family caregivers (7 months after amputation); 84 family caregivers (up to 10 months after amputation); Living at home | (i) Mental health and psychological needs (ii) Physical health needs (iv) Supportive care needs | Between 1 and 7 months after surgery appears to be a critical period, given the increase in physical symptoms; caregivers who presented high levels of physical symptomatology showed low levels of mental QoL over time. Seven months after the amputation, caregivers experience a greater number of physical symptoms, due to the strain of caring for patients with reduced mobility. In the period between 1 and 7 months after amputation, an increase occurs in the physical symptomatology of the family caregivers due to exhaustion, needing support in caregiving tasks to help deal with physical exhaustion. |
| Costa et al. (2018) [30], Portugal | Longitudinal Study (Quantitative) | 110 family caregivers of people with diabetic foot amputations (1 month after amputation); 101 family caregivers (7 months after amputation); 84 family caregivers (up to 10 months after amputation); Living at home | (iv) Supportive care needs (v) Social support needs | Family caregivers need increasing help with caregiving activities up to 10 months after amputation, to prevent the burden and stress of care from increasing over time. Caregiver burden increases in the first seven months after amputation and family or social support are needed to prevent the development of caregiving burden and other symptoms. |
| Tsoulou et al. (2019) [31], Grece | Cross-sectional Study (Quantitative) | 50 hospitalized patients who had undergone traumatic amputations (lower limb, fingers) and 50 family caregivers; Hospital discharge/returning home | (i) Mental health and psychological needs | Caregivers frequently put others’ needs before their own and sacrifice leisure time. Patients’ and caregivers’ psychological state is of great importance for effective treatment. After hospital discharge, 80% of the caregivers were referred for psychological counseling. |
| Ganjparvar et al. (2016) [32], Iran | Cross-sectional Study (Quantitative) | 232 amputees with LLA due to different injuries during war and 232 family caregivers (wives); Living at home | (i) Mental health and psychological needs (ii) Physical health needs (iii) Health and well-being needs (v) social support needs | Caregivers need to assess care and service to maintain physical and mental health and help to promote their QoL. Caregivers responsible for the care of the person with amputations from the beginning of their condition have a lower quality of life (QoL) in the domain of physical functioning with limitations in physical activity. Caregivers of the person with bilateral LLAs have unfulfilled health and well-being needs and a poor QoL. Caregivers have lower scores in the domain of general health when compared with the general population. Compared with the general population, family caregivers of people with LLAs have lower scores in social function and mental health. Social support helps to mitigate the effect of caregivers’ burden. |
| Foss et al. (2009) [33], Brazil | Descriptive Cross-sectional Study (Quantitative) | 87 family caregivers of people with dysvascular LLAs; Living at home | (i) Mental health and psychological needs | The emotional aspect of LLA caregivers associated with general tension, isolation, disappointment, and environment is significant. LLAs’ caregivers need guidance and psychological support. |
| Bennett, J. (2016) [34], USA | Literature Review | Amputees with LLAs due to diabetes; Hospital discharge/returning home | (vi) Educational/Informational needs | Communication is essential for consistency in the planning of care for the patient and their caregivers. Postoperative care along with communication among health providers, patients, and their families are essential for a successful transition to a new life. |
| Latlief et al. (2012) [35], USA | Literature Review | Amputees with LLAs due to dysvascular conditions or traumatic events; Returning home | (vi) Educational/Informational needs | There is a greater risk of injury in family caregivers of the person with amputation, transferring into/out of chairs, cars, beds, bathtubs, and other environments, given that most of them are untrained. Families of the person with a LLA need to be educated on issues such as skin monitoring, stump sock management, donning and doffing prosthesis, residual limb hygiene, and componentry inspection and maintenance. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, D.; Silva, R.; Castanheira, S.; Carvalho, L.; Pinto, C. Needs of Family Caregivers of People with Lower Limb Amputations: A Scoping Review. Behav. Sci. 2024, 14, 326. https://doi.org/10.3390/bs14040326
Rodrigues D, Silva R, Castanheira S, Carvalho L, Pinto C. Needs of Family Caregivers of People with Lower Limb Amputations: A Scoping Review. Behavioral Sciences. 2024; 14(4):326. https://doi.org/10.3390/bs14040326
Chicago/Turabian StyleRodrigues, Diana, Rosa Silva, Sofia Castanheira, Luís Carvalho, and Cristina Pinto. 2024. "Needs of Family Caregivers of People with Lower Limb Amputations: A Scoping Review" Behavioral Sciences 14, no. 4: 326. https://doi.org/10.3390/bs14040326
APA StyleRodrigues, D., Silva, R., Castanheira, S., Carvalho, L., & Pinto, C. (2024). Needs of Family Caregivers of People with Lower Limb Amputations: A Scoping Review. Behavioral Sciences, 14(4), 326. https://doi.org/10.3390/bs14040326