Latino Veterans with PTSD: A Systematic Review

Abstract
:1. Introduction
1.1. PTSD in Veterans and Latinos
1.1.1. Latino Culture and PTSD Assessment
1.1.2. Latino Culture and PTSD Treatment
1.2. Rationale and Objectives
2. Method
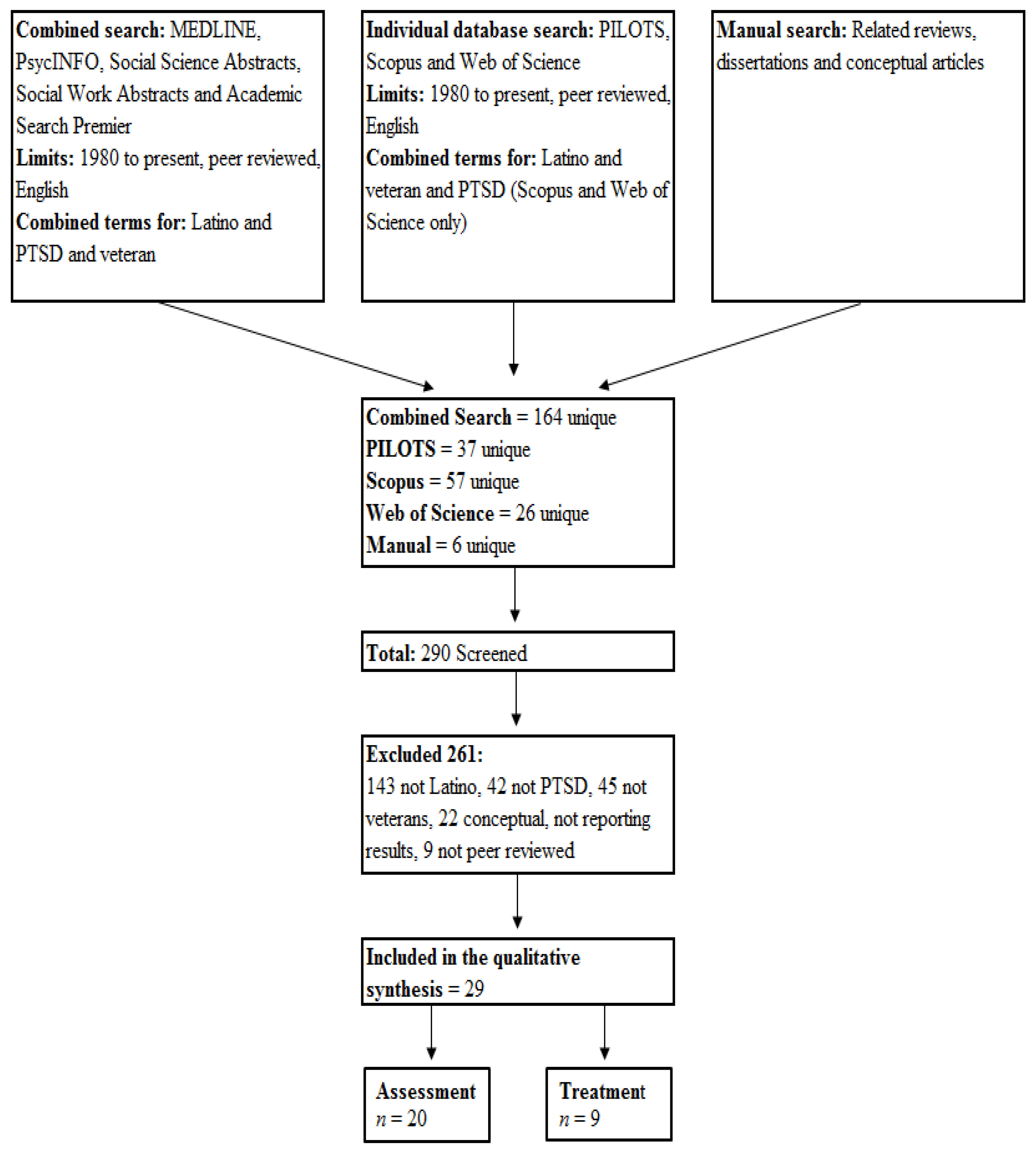
2.1. Article Selection
2.2. Data Collection Process and Data Items
3. Results
3.1. Article Selection

3.2. Article Characteristics

{kind=link}
| Article by Category | Study Design/Type | Total Sample Size (% Latino) | % Latina | Latino Subgroup (% of Total Latino) | Veteran Era | Data Source (Setting) | PTSD Measure | Cultural Considerations |
|---|---|---|---|---|---|---|---|---|
| Assessment Related | ||||||||
| C'de Baca, Castillo and Qualls, 2012 | Quan/Corr | 398 (28) | 28 | Not reported | Unknown | VA New Mexico Women's Stress Disorder Clinic | CAPS | M |
| David et al. 1999 | Quan/Corr | 53 (17) | 0 | Not reported | Multiple | VA Miami Inpatient Unit | SCID III, MS | M |
| Dohrenwend et al. 2008 | Quan/Corr | 248 (33) | 0 | 84 (MA (75), PR (18) O (7) | Vietnam | NVVRS | SCID | I |
| Escobar et al. 1983 | Quan/Corr | 41 (100) | 0 | Not reported | Vietnam | VA Los Angeles Clinic | DSM-III Symptom Checklist | I |
| Fontana and Rosenheck, 1994 | Quan/Corr | 1,198 (23) | 0 | Not reported | Vietnam | NVVRS | NVVRS Comp | NM |
| Ghafoori Heirholzer, 2010 | Quan/Corr | 96 (25) | 0 | Not reported | Unknown | Central California Vet Center | CAPS | M |
| Herrera, Owens, MallIkrodt, 2013 | Quan/Corr | 45 (100) | 0 | M (51), PR (27), CA (11), SA (7), C(4); O (13) | Unknown | Online Survey | PCL | I |
| Koopman et al. 2001 | Quan/Corr | 102 (11) | 0 | Not reported | Vietnam | VA Inpatient PTSD Program | CAPS | M |
| Kulka et al. 1990 | Quan/Corr | 1,198 (23) | Unknown | Not reported | Vietnam | NVVRS | NVVRS Comp | NM |
| Lewis-Fernández et al. 2008 | Quan/Corr | 255 (33.7) | 0 | MA (73); PR (20), O (7) | Vietnam | NVVRS | M-PTSD and SCID | I |
| Ortega and Rosenheck, 2000 | Quan/Corr | 1,195 (23) | 0 | MA (63), PR (23), C (2), CSA (3), O (9) | Vietnam | NVVRS | MS, NVVRS Comp | I |
| Penk et al. 1989 | Quan/Corr | 770 (12.8) | 0 | Not reported | Vietnam | VA Dallas Substance Program | MMPI with PTSD Finley’s PTSD Checklist | M |
| Ruef, Litz, and Schlenger, 2000 | Quan/Corr | 3,016 (48.9) | 0 | MA (63), PR (23), C (2), CSA (3), O (9) | Vietnam | NVVRS | MS | I |
| Schlenger et al. 1992 | Quan/Corr | 3,016 (48.9) | Unknown | MA (63), PR (23), C (2), CSA (3), O (9) | Vietnam | NVVRS | MS, MMPI, SCID | I |
| Schnurr et al. 2003 | Quan/Corr | 482 (9.5) | 0 | Not reported | Vietnam | NVVRS and HVVP | SCID | NM |
| Schnurr, Lunney, and Sengupta, 2004 | Quan/Corr | 482 (9.5) | 0 | Not reported | Vietnam | NVVRS and HVVP | SCID | NM |
| Tanielian et al. 2008 | Quan/Corr | 1,965 (8.3) | Unknown | Not reported | OEF/OIF | Random Sample of those Deployed to OEF/OIF | PCL | NM |
| Wilcox, Briones, and Suess, 1991a | Quan/Corr | 59 (not reported) | 0 | Not reported | Multiple | VA El Paso PTSD Clinic | Dx | M |
| Wilcox, Briones, and Suess, 1991b | Quan/Corr | 59 (61) | 0 | MA (77), PR (23) | Unknown | VA El Paso PTSD Clinic | Dx | M |
| Zatzick et al. 1994 | Quan/Corr | 225 (33) | 0 | Not reported | Vietnam | NVVRS | SCID | M |
| Bauer et al. 2013 | Quan/Corr | 732,085 (4.2) | Unknown | Not reported | Multiple | VA Austin Data Center | Dx | NM |
| Brinker et al. 2007 | Quan/Corr | 255 (46.3) | 0 | Not reported | Unknown | Southwest and Northeast U.S. Community | PCL | M |
| Greenawalt et al. 2011 | Quan/Corr | 148 (27) | Unknown | Not reported | OEF/OIF | VA Central Texas (3 Sites) | PCL | M |
| Jeffreys et al. 2013 | Quan/Caus | 263 (55.8) | Unknown | Not reported | Multiple | VA Texas Outpatient | CAPS, PCL, MINI PTSD | NM |
| Rosenheck and Fontana, 1996 | Quan/Caus | 5,475 (8.1) | Unknown | PR (56), MA (44) | Vietnam | VA PTSD Program (53 Sites) | SCID-III | M |
| Rosenheck and Fontana, 2002 | Quan/Caus | 12,447 (5.3) | 0.06 | Not reported | Vietnam | VA Inpatient PTSD Program (49 Sites) | MS, PC-PTSD | M |
| Spoont et al. 2009 | Quan/Corr | 20,284 (5) | Unknown | Not reported | Multiple | VA National Patient Care Database | Dx | M |
| Wanner, Long, and Tang, 2010 | Quan/Case Study | 1 (100) | 0 | Not reported | Vietnam | Large VA Medical Center | PCL | NM |
| Zappert and Westrup, 2008 | Quan/Caus | 18 (5.6) | 5.6 | Not reported | Unknown | Palo Alto VA Woman’s Trauma Recovery Program | PCL, Dx | NM |
3.3. Assessment Related (n = 20)
3.3.1. Assessment Related Symptoms and Comorbidity
3.3.2. Cultural Factors
3.4. Treatment Related (n = 9)
3.4.1. Treatment Outcomes
3.4.2.Cultural Factors
4. Discussion
4.1. Overall Limitations and Gaps
4.2. Assessment Related
4.3. Treatment Related
4.4. Limitations
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Humes, K.; Jones, N.A.; Ramirez, R.R. Overview of Race and Hispanic Origin, 2010; US Department of Commerce, Economics and Statistics Administration, US Census Bureau: Suitland, MD, USA, 2011. [Google Scholar]
- U.S. Bureau of the Census, Population Estimates Program. State and Country Quick Facts: Hispanic Origin. Available online: http://quickfacts.census.gov/qfd/meta/long_RHI825212.htm (accessed on 2 March 1014).
- Office of the Under Secretary of Defense, Personnel and Readiness. Population Representation in the Military Services; Fiscal Year 2011; Summary Report. Available online: http://prhome.defense.gov/RFM/MPP/AP/POPREP.aspx (accessed on 2 March 1014).
- U.S. Department of Veterans Affairs. Department of Veterans Affairs FY 2014–2020 Strategic Plan. Available online: http://www.va.gov/op3/docs/StrategicPlanning/VA2014-2020strategicPlan.PDF (accessed on 2 March 1014).
- Institute of Medicine (IOM). eturning home from Iraq and Afghanistan: Preliminary assessment of readjustment needs of veterans, service members, and their families; The National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Richardson, L.K.; Frueh, B.C.; Acierno, R. Prevalence estimates of combat-related post-traumatic stress disorder: Critical review. Austr. N. Zeal. J. Psychiatry 2010, 44, 4–19. [Google Scholar] [CrossRef]
- Campbell, D.G.; Felker, B.L.; Liu, C.F.; Yano, E.M.; Kirchner, J.E.; Chan, D.; Rubenstein, L.V.; Chaney, E.F. Prevalence of depression–PTSD comorbidity: Implications for clinical practice guidelines and primary care-based interventions. J. Gener. Intern. Med. 2007, 22, 711–718. [Google Scholar]
- Erbes, C.; Westermeyer, J.; Engdahl, B.; Johnsen, E. Post-traumatic stress disorder and service utilization in a sample of service members from Iraq and Afghanistan. Milit. Med. 2007, 172, 359–363. [Google Scholar]
- Pittman, J.O.E.; Goldsmith, A.A.; Lemmer, J.A.; Kilmer, M.T.; Baker, D.G. Post-traumatic stress disorder, depression, and health-related quality of life in OEF/OIF veterans. Qual. Life Res. 2012, 21, 99–103. [Google Scholar]
- Tanielian, T.L.; Jaycox, L. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery; Rand Corporation: Santa Monica, CA, USA, 2008. [Google Scholar]
- Institute of Medicine (IOM). Treatment for Posttraumatic Stress Disorder in military and Veteran Populations: Initial Assessment; The National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Hough, R.L.; Canino, G.J.; Abueg, F.R.; Gusman, F.D. PTSD and related stress disorders among Hispanics. In Ethnocultural Aspects of Posttraumatic Stress Disorder: Issues, Research, and Clinical Applications; Marsella, A.J., Friedman, M.J., Gerrity, E.T., Scurfield, R.M., Eds.; American Psychological Association: Washington, DC, USA, 1996; pp. 301–338. [Google Scholar]
- Joyce, P.A.; Berger, R. Which language does PTSD speak? The “westernization” of Mr. Sanchez. J.Trauma Pract. 2007, 5, 53–67. [Google Scholar] [CrossRef]
- Marsella, A.; Friedman, M.; Spain, E.H. A selective review of the literature on ethnocultural aspects of PTSD. PTSD Res. Q. 1992, 3, 1–7. [Google Scholar]
- Marsella, A.J. Ethnocultural aspects of PTSD: An overview of concepts, issues, and treatments. Traumatology 2010, 16, 17–26. [Google Scholar] [CrossRef]
- Berberich, D.A. Posttraumatic stress disorder: Gender and cross-cultural clinical issues. Psychother. Priv. Pract. 1998, 17, 29–41. [Google Scholar] [CrossRef]
- Adams, R.E.; Boscarino, J.A. Differences in mental health outcomes among Whites, African Americans, and Hispanics following a community disaster. Psychiatry 2005, 68, 250. [Google Scholar]
- Alarcón, R.D. Culture, cultural factors and psychiatric diagnosis: review and projections. World Psychiatry 2009, 8, 131–139. [Google Scholar]
- Alcántara, C.; Casement, M.D.; Lewis-Fernández, R. Conditional risk for PTSD among Latinos: A systematic review of racial/ethnic differences and sociocultural explanations. Clin. Psychol. Rev. 2013, 33, 107–119. [Google Scholar]
- Alegría, M.; Mulvaney-Day, N.; Woo, M.; Torres, M.; Gao, S.; Oddo, V. Correlates of past-year mental health service use among Latinos: Results from the National Latino and Asian American Study. Am. J. Public Health 2007, 97, 76–83. [Google Scholar] [CrossRef]
- Eisenman, D.P.; Meredith, L.S.; Rhodes, H.; Green, B.L.; Kaltman, S.; Cassells, A.; Tobin, J.N. PTSD in Latino patients: Illness beliefs, treatment preferences, and implications for care. J. Gener. Intern. Med. 2008, 23, 1386–1392. [Google Scholar] [CrossRef]
- Fierros, M.; Smith, C. The Relevance of Hispanic Culture to the Treatment of a Patient with Posttraumatic Stress Disorder (PTSD). Psychiatry (Edgmont) 2006, 3, 49–56. [Google Scholar]
- Frueh, B.C.; Brady, K.L.; de Arellano, M.A. Racial differences in combat-related PTSD: Empirical findings and conceptual issues. Clin. Psychol. Rev. 1998, 18, 287–305. [Google Scholar] [CrossRef]
- Greenwell, A.N.; Cosden, M. The relationship between fatalism, dissociation, and trauma symptoms in Latinos. J. Trauma Dissoc. 2009, 10, 334–345. [Google Scholar] [CrossRef]
- Pole, N.; Best, S.R.; Metzler, T.; Marmar, C.R. Why are Hispanics at greater risk for PTSD? Cult. Divers. Ethn. Minor. Psychol. 2005, 11, 144–161. [Google Scholar] [CrossRef]
- Galea, S.; Ahern, J.; Resnick, H.; Kilpatrick, D.; Bucuvalas, M.; Gold, J.; Vlahov, D. Psychological sequelae of the September 11 terrorist attacks in New York City. N. Engl. J. Med. 2002, 346, 982–987. [Google Scholar] [CrossRef]
- Perilla, J.L.; Norris, F.H.; Lavizzo, E.A. Ethnicity, culture, and disaster response: Identifying and explaining ethnic differences in PTSD six months after Hurricane Andrew. J. Soc. Clin. Psychol. 2002, 21, 20–45. [Google Scholar]
- Williams, A.E.; Smith, W.R.; Starr, A.J.; Webster, D.C.; Martinez, R.J.; Vojir, C.P.; Sakalys, J.A.; Morgan, S.J. Ethnic differences in posttraumatic stress disorder after musculoskeletal trauma. J. Trauma-Injury Infect. Crit. Care 2008, 65, 1054–1065. [Google Scholar] [CrossRef]
- Dassori, A.M.; Silva, J.A. PTSD and ethnic violence. Psychiatr. Serv. 1998, 49, 108–108. [Google Scholar]
- Duke, M.R.; Moore, R.S.; Ames, G.M. PTSD treatment-seeking among rural Latino combat veterans: A review of the literature. J. Rur. Soc. Sci. 2011, 26, 157–180. [Google Scholar]
- Ruef, A.M.; Litz, B.T.; Schlenger, W.E. Hispanic ethnicity and risk for combat-related posttraumatic stress disorder. Cult. Divers. Ethn. Minor. Psychol. 2000, 6, 235–251. [Google Scholar] [CrossRef]
- Antshel, K.M. Integrating culture as a means of improving treatment adherence in the Latino population. Psychol. Health Med. 2002, 7, 435–449. [Google Scholar] [CrossRef]
- Norris, F.H.; Alegría, M. Promoting disaster recovery in ethnic-minority individuals and communities. In Ethnocultural Perspectives on Disaster and Trauma; Springer: New York, NY, USA, 2008; pp. 15–35. [Google Scholar]
- Cánive, J.M.; Castillo, D. Hispanic veterans diagnosed with PTSD: Assessment and treatment issues. NC-PTSD Clin. Q. 1997, 7, 12–14. [Google Scholar]
- Penk, W.E.; Allen, I.M. Clinical assessment of post-traumatic stress disorder (PTSD) among American minorities who served in Vietnam. J. Traum. Stress 1991, 4, 41–66. [Google Scholar] [CrossRef]
- Marin, G.; Sabogal, F.; Marin, B.V.; Otero-Sabogal, R.; Perez-Stable, E.J. Development of a short acculturation scale for Hispanics. Hispan. J. Behav. Sci. 1987, 9, 183–205. [Google Scholar]
- Felix-Ortiz, M.; Newcomb, M.D.; Myers, H. A multidimensional measure of cultural identity for Latino and Latina adolescents. Hispan. J. Behav. Sci. 1994, 16, 99–115. [Google Scholar] [CrossRef]
- Cervantes, R.C.; Castro, F.G. Stress, coping, and Mexican American mental health: A systematic review. Hispan. J. Behav. Sci. 1985, 7, 1–73. [Google Scholar] [CrossRef]
- Ruiz, P. Assessing, diagnosing and treating culturally diverse individuals: A Hispanic perspective. Psychiatr. Q. 1995, 66, 329–341. [Google Scholar] [CrossRef]
- Kichic, R.; Vera, M.; Reyes-Rabanillo, M. Commentary: Challenges in the dissemination and implementation of exposure-based CBT for the treatment of Hispanics with PTSD. In Posttraumatic Stress Disorder; Stein, D.J., Friedman, M.J., Blanco, C., Eds.; John and Sons, Ltd.: Oxford, UK, 2011; pp. 205–207. [Google Scholar]
- Roberts, A.L.; Gilman, S.E.; Breslau, J.; Breslau, N.; Koenen, K.C. Race/ethnic differences in exposure to traumatic events, development of post-traumatic stress disorder, and treatment-seeking for post-traumatic stress disorder in the United States. Psychol. Med. 2011, 41, 71–83. [Google Scholar] [CrossRef] [Green Version]
- Hinton, D.E.; Lewis-Fernández, R. The cross-cultural validity of posttraumatic stress disorder: Implications for DSM-5. Depress. Anxiety 2011, 28, 783–801. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; American Psychiatric Association: Washington, DC, USA, 1980. [Google Scholar]
- Spitzer, R.L.; Williams, J.B.; Gibbon, M.; First, M.B. The Structured Clinical Interview for DSM-III-R (SCID) I: History, rationale, and description. Arch. Gener. Psychiatry 1992, 49, 624–629. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. In Proceedings of the Annual Meeting of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 29 October 1993.
- Keane, T.M.; Caddell, J.M.; Taylor, K.L. Mississippi Scale for Combat-Related Posttraumatic Stress Disorder: three studies in reliability and validity. J. Consult. Clin. Psychol. 1988, 56, 85–90. [Google Scholar] [CrossRef]
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a clinician-administered PTSD scale. J. Traum. Stress 1995, 8, 75–90. [Google Scholar]
- C’de Baca, J.; Castillo, D.; Qualls, C. Ethnic differences in symptoms among female veterans diagnosed with PTSD. J. Traum. Stress 2012, 25, 353–357. [Google Scholar]
- Ghafoori, B.; Hierholzer, R.W. Personality patterns among Black, White, and Hispanic combat veterans. Psychol. Trauma: Theory Res. Pract. Policy 2010, 2, 12–18. [Google Scholar] [CrossRef]
- Jeffreys, M.D.; Reinfeld, C.; Nair, P.V.; Garcia, H.A.; Mata-Galan, E.; Rentz, T.O. Evaluating treatment of posttraumatic stress disorder with cognitive processing therapy and prolonged exposure therapy in a VHA specialty clinic. J. Anxiety Disord. 2014, 28, 108–114. [Google Scholar] [CrossRef]
- Koopman, C.; Drescher, K.; Bowles, S.; Gusman, F.; Blake, D.; Dondershine, H.; Chang, V.; Butler, L.D.; Spiegel, D. Acute dissociative reactions in veterans with PTSD. J. Trauma Dissoc. 2001, 2, 91–111. [Google Scholar] [CrossRef]
- Dohrenwend, B.P.; Turner, J.B.; Turse, N.A.; Lewis-Fernandez, R.; Yager, T.J. War-related posttraumatic stress disorder in Black, Hispanic, and majority White Vietnam veterans: The roles of exposure and vulnerability. J. Traum. Stress 2008, 21, 133–141. [Google Scholar] [CrossRef]
- Fontana, A.; Rosenheck, R. Posttraumatic Stress Disorder Among Vietnam Theater Veterans A Causal Model of Etiology in a Community Sample. J. Nerv. Ment. Dis. 1994, 182, 677–684. [Google Scholar] [CrossRef]
- Kulka, R.A.; Schlenger, W.E.; Fairbank, J.A.; Hough, R.L.; Jordan, B.K.; Marmar, C.R.; Weiss, D.S. Contractual Report of Findings from the National Vietnam Veterans Readjustment Study; Research Triangle Institute: Raleigh, NC, USA, 1988; Volumes 1–4. [Google Scholar]
- Lewis-Fernández, R.; Turner, J.B.; Marshall, R.; Turse, N.; Neria, Y.; Dohrenwend, B.P. Elevated rates of current PTSD among Hispanic veterans in the NVVRS: True prevalence or methodological artifact? J. Traum. Stress 2008, 21, 123–132. [Google Scholar] [CrossRef]
- Ortega, A.N.; Rosenheck, R. Posttraumatic stress disorder among Hispanic Vietnam veterans. Am. J. Psychiatry 2000, 157, 615–619. [Google Scholar] [CrossRef]
- Schlenger, W.E.; Kulka, R.A.; Fairbank, J.A.; Hough, R.L.; Kathleen Jordan, B.; Marmar, C.R.; Weiss, D.S. The prevalence of post-traumatic stress disorder in the Vietnam generation: A multimethod, multisource assessment of psychiatric disorder. J. Traum. Stress 1992, 5, 333–363. [Google Scholar] [CrossRef]
- Schnurr, P.P.; Lunney, C.A.; Sengupta, A.; Waelde, L.C. A descriptive analysis of PTSD chronicity in Vietnam veterans. J. Traum. Stress 2003, 16, 545–553. [Google Scholar] [CrossRef]
- Schnurr, P.P.; Lunney, C.A.; Sengupta, A. Risk factors for the development versus maintenance of posttraumatic stress disorder. J. Traum. Stress 2004, 17, 85–95. [Google Scholar] [CrossRef]
- Penk, W.E.; Robinowitz, R.; Black, J.; Dolan, M.; Bell, W.; Dorsett, D.; Ames, M.; Noriega, L. Ethnicity: Post-Traumatic Stress Disorder (PTSD) differences among black, white, and Hispanic veterans who differ in degrees of exposure to combat in Vietnam. J. Clin. Psychol. 1989, 45, 729–735. [Google Scholar] [CrossRef]
- David, D.; Kutcher, G.S.; Jackson, E.I.; Mellman, T.A. Psychotic symptoms in combat-related posttraumatic stress disorder. J. Clin. Psychiatry 1999, 60, 29–32. [Google Scholar] [CrossRef]
- Wilcox, J.; Briones, D.; Suess, L. Auditory hallucinations, posttraumatic stress disorder, and ethnicity. Compr. Psychiatry 1991, 32, 320–323. [Google Scholar] [CrossRef]
- Zatzick, D.F.; Marmar, C.R.; Weiss, D.S.; Metzler, T. Does trauma-linked dissociation vary across ethnic groups? J. Nerv. Ment. Dis. 1994, 182, 576–582. [Google Scholar] [CrossRef]
- Wilcox, J.A.; Briones, D.F.; Suess, L. Substance abuse, post-traumatic stress, and ethnicity. J. Psychoact. Drugs 1991, 23, 83–84. [Google Scholar] [CrossRef]
- Escobar, J.I.; Randolph, E.T.; Puente, G.; Spiwak, F.; Asamen, J.K.; Hill, M.; Hough, R.L. Post-traumatic stress disorder in Hispanic Vietnam veterans: Clinical phenomenology and sociocultural characteristics. J. Nerv. Ment. Dis. 1983, 171, 585–596. [Google Scholar] [CrossRef]
- Herrera, C.J.; Owens, G.P.; Mallinckrodt, B. Traditional Machismo and Caballerismo as Correlates of Posttraumatic Stress Disorder, Psychological Distress, and Relationship Satisfaction in Hispanic Veterans. J. Multicul. Couns. Dev. 2013, 41, 21–35. [Google Scholar] [CrossRef]
- Greenawalt, D.S.; Tsan, J.Y.; Kimbrel, N.A.; Meyer, E.C.; Kruse, M.I.; Tharp, D.F.; Gulliver, S.B.; Morissette, S.B. Mental health treatment involvement and religious coping among African American, Hispanic, and white veterans of the wars of Iraq and Afghanistan. Depress. Res. Treat. 2011, 2011, 1–10. [Google Scholar]
- Spoont, M.R.; Hodges, J.; Murdoch, M.; Nugent, S. Race and ethnicity as factors in mental health service use among veterans with PTSD. J. Traum. Stress 2009, 22, 648–653. [Google Scholar]
- Bauer, M.S.; Lee, A.; Li, M.; Bajor, L.; Rasmusson, A.; Kazis, L.E. Off-label use of second generation antipsychotics for post-traumatic stress disorder in the Department of Veterans Affairs: Time trends and sociodemographic, comorbidity, and regional correlates. Pharmacoepidemiol. Drug Saf. 2014, 23, 77–86. [Google Scholar] [CrossRef]
- Rosenheck, R.; Fontana, A. Ethnocultural variations in service use among veterans suffering from PTSD. In Ethnocultural Aspects of Posttraumatic Stress Disorder: Issues, Research, and Clinical Applications; Marsella, A.J., Friedman, M.J., Gerrity, E.T., Scurfield, R.M., Eds.; American Psychological Association: Washington, DC, USA, 1996; pp. 483–504. [Google Scholar]
- Rosenheck, R.; Fontana, A. Black and Hispanic veterans in intensive VA treatment programs for posttraumatic stress disorder. Med. Care 2002, 40, I-52–I-61. [Google Scholar] [CrossRef]
- Brinker, M.; Westermeyer, J.; Thuras, P.; Canive, J. Severity of combat-related posttraumatic stress disorder versus noncombat-related posttraumatic stress disorder: A community-based study in American Indian and Hispanic veterans. J. Nerv. Ment. Dis. 2007, 195, 655–661. [Google Scholar] [CrossRef]
- Wanner, J.; Long, M.E.; Teng, E.J. Multi-component treatment for posttraumatic nightmares in Vietnam veterans: Two case studies. J. Psychiatr. Pract. 2010, 16, 243–249. [Google Scholar] [CrossRef]
- Zappert, L.N.; Westrup, D. Cognitive processing therapy for posttraumatic stress disorder in a residential treatment setting. Psychother.: Theory Res. Pract. Train 2008, 45, 361–476. [Google Scholar] [CrossRef]
- Anastas, J.W. Research Design for Social Work and the Human Services; Columbia University Press: New York, NY, USA, 2000. [Google Scholar]
- Loo, C.M. Race-related PTSD: The Asian American Vietnam veteran. J. Traum. Stress 1994, 7, 637–656. [Google Scholar]
- Leal, D.L. The multicultural military: Military service and the acculturation of Latinos and Anglos. Arm. Forces Soc. 2003, 29, 205–226. [Google Scholar] [CrossRef]
- Hinton, D.E.; Hofmann, S.G.; Rivera, E.; Otto, M.W.; Pollack, M.H. Culturally adapted CBT (CA-CBT) for Latino women with treatment-resistant PTSD: A pilot study comparing CA-CBT to applied muscle relaxation. Behav. Res. Therapy 2011, 49, 275–280. [Google Scholar] [CrossRef]
- Foa, E.; Hembree, E.; Rothbaum, B.O. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences Therapist Guide; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Monson, C.M.; Schnurr, P.P.; Resick, P.A.; Friedman, M.J.; Young-Xu, Y.; Stevens, S.P. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. J. Consult. Clin. Psychol. 2006, 74, 898–907. [Google Scholar] [CrossRef]
- Comas-Díaz, L. Latino healing: The integration of ethnic psychology into psychotherapy. Psychother.: Theory Res. Pract. Train 2006, 43, 436–453. [Google Scholar]
- Elsass, P. Individual and collective traumatic memories: A qualitative study of post-traumatic stress disorder symptoms in two Latin American localities. Transcult. Psychiatry 2001, 38, 306–316. [Google Scholar]
- Gafner, G.; Benson, S. Indirect ego-strengthening in treating PTSD in immigrants from Central America. Contemp. Hypnosis 2001, 18, 135–144. [Google Scholar] [CrossRef]
- Shapiro, F.E. EMDR As an Integrative Psychotherapy Approach: Experts of Diverse Orientations Explore the Paradigm Prism; American Psychological Association: Washington, DC, USA, 2002. [Google Scholar]
- Schottenbauer, M.A.; Glass, C.R.; Arnkoff, D.B.; Gray, S.H. Contributions of psychodynamic approaches to treatment of PTSD and trauma: A review of the empirical treatment and psychopathology literature. Psychiatry: Interpers. Biol. Process 2008, 71, 13–34. [Google Scholar] [CrossRef]
- Stein, H.; Allen, J.G. Mentalizing as a framework for integrating therapeutic exposure and relationship repair in the treatment of a patient with complex posttraumatic psychopathology. Bull. Menn. Clin. 2007, 71, 273–290. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pittman, J.O.E. Latino Veterans with PTSD: A Systematic Review. Behav. Sci. 2014, 4, 320-340. https://doi.org/10.3390/bs4030320
Pittman JOE. Latino Veterans with PTSD: A Systematic Review. Behavioral Sciences. 2014; 4(3):320-340. https://doi.org/10.3390/bs4030320
Chicago/Turabian StylePittman, James O. E. 2014. "Latino Veterans with PTSD: A Systematic Review" Behavioral Sciences 4, no. 3: 320-340. https://doi.org/10.3390/bs4030320
APA StylePittman, J. O. E. (2014). Latino Veterans with PTSD: A Systematic Review. Behavioral Sciences, 4(3), 320-340. https://doi.org/10.3390/bs4030320