Relation of Structural and Functional Changes in Auditory and Visual Pathways after Temporal Lobe Epilepsy Surgery

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
- Patients with mTLE evaluated according to the institution’s protocols and who were candidates for resective surgery according to agreed criteria.
- Patients who met the drug-resistance criteria.
- Patients who gave their informed consent to participate in the investigation.
2.2. Electrophysiological Tests
2.3. Resection Measure
2.4. Perimetry
2.5. Diffusion Tensor Imaging (DTI)
2.6. Tractography
2.7. Brain Anatomical Connectivity
2.8. Statistics
2.9. Ethical Considerations
3. Results
3.1. Auditory Pathway
Structure-Function Relationships
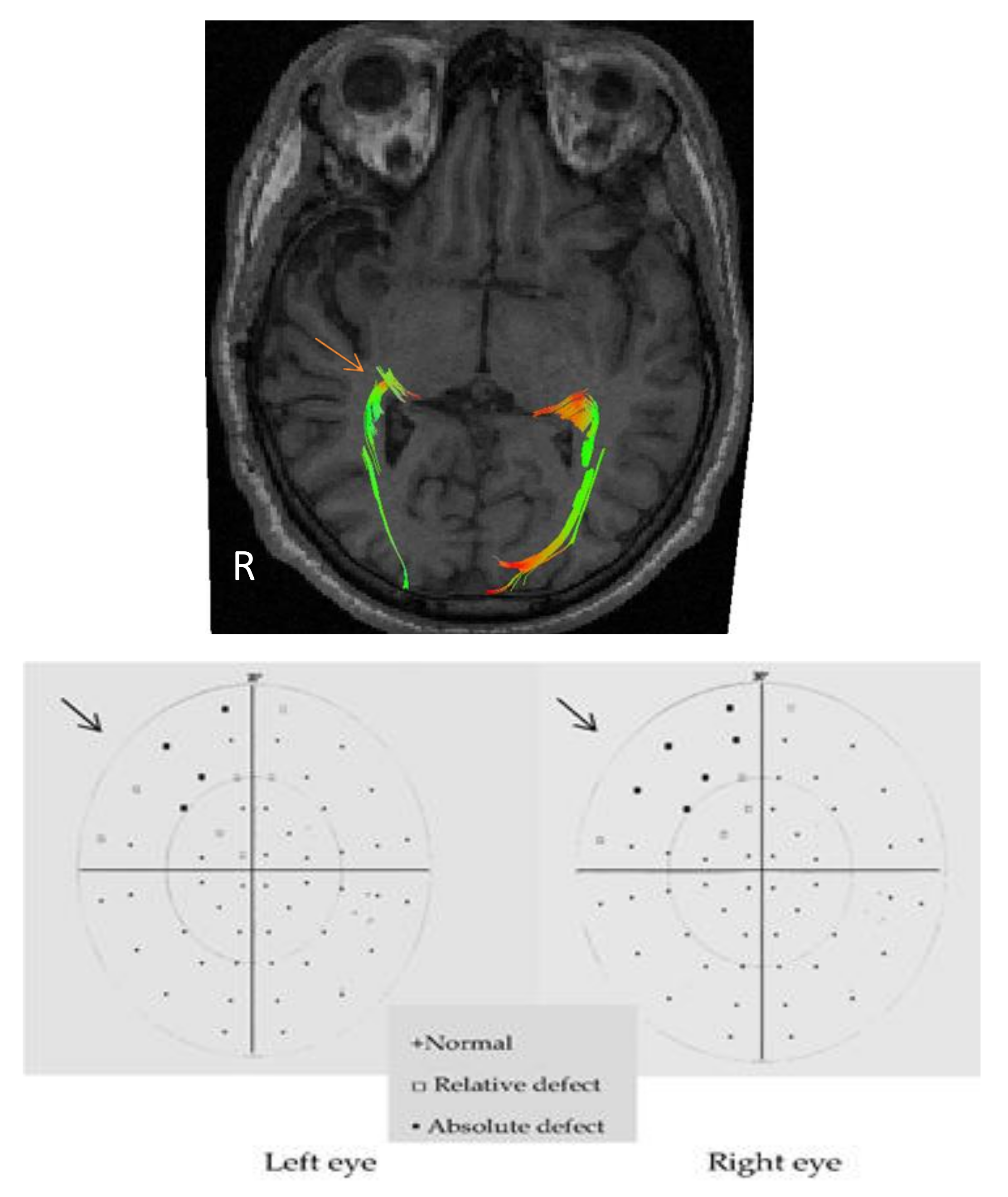
3.2. Visual Pathway
Structure-Function Relationships
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gronich, G.; Arno, L.; Dualib, K. Neurofisiologia nao-invasiva (EEG) das diferentes síndromes epilépticas. In Tratamento clínico e cirúrgico das epilepsias de dificil controle; Cukiert, A., Ed.; Lemos: Sao Paulo, Brazil, 2002; p. 157. [Google Scholar]
- Hauser, W. The natural history of temporal lobe epilepsy. In Epilepsy Surgery; Luders, H., Ed.; Raven Press: New York, NY, USA, 2000; pp. 133–141. [Google Scholar]
- Viera, O., Jr. Tratamento cirúrgico da epilepsia do lobo temporal. In Tratamento Clínico e Cirúrgico das Epilepsias de Difícil Controle; Cukiert, A., Ed.; Lemos: Sao Paulo, Brazil, 2002; pp. 269–289. [Google Scholar]
- Bonilha, L.; Marzt, G.U.; Glazier, S.S.; Edwards, J.C. Subtypes of medial temporal lobe epilepsy: Influence on temporal lobectomy outcomes? Epilepsia 2012, 53, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bazil, C.; Morrell, M.J.; Peddley, T. Epilepsy. In Merritt’s Neurology; Rowland, L., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, YSA, 2005; pp. 990–1008. [Google Scholar]
- Karceski, S.; Morrell, M. Principles of epilepsy management: Diagnosis and treatment. In Neurological Therapeutics: Principles and Practice; Noseworthy, J.H., Ed.; Informa Healthcare: Rochester, NY, USA, 2006; pp. 341–354. [Google Scholar]
- Sindou, M.; Guenot, M. Surgical anatomy of the temporal lobe for epilepsy surgery. Adv. Tech. Stand. Neurosurg. 2003, 28, 315–343. [Google Scholar] [PubMed]
- Hughes, T.S.; Abou-Khalil, B.; Lavin, P.J.; Fakhoury, T.; Blumenkopf, B.; Donahue, S.P. Visual field defects after temporal lobe resection: A prospective quantitative analysis. Neurology 1999, 53, 167–172. [Google Scholar] [CrossRef] [PubMed]
- James, J.S.; Radhakrishnan, A.; Thomas, B.; Madhusoodanan, M.; Kesavadas, C.; Abraham, M.; Menon, R.; Rathore, C.; Vilanilam, G. Diffusion tensor imaging tractography of Meyer’s loop in planning resective surgery for drug-resistant temporal lobe epilepsy. Epilepsy Res. 2015, 110, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Jeelani, N.U.; Jindahra, P.; Tamber, M.S.; Poon, T.L.; Kabasele, P.; James-Galton, M.; Stevens, J.; Duncan, J.; McEvoy, A.W.; Harkness, W.; et al. ‘Hemispherical asymmetry in the Meyer’s Loop’: A prospective study of visual-field deficits in 105 cases undergoing anterior temporal lobe resection for epilepsy. J. Neurol. Neurosurg. Psychiatry 2010, 81, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, D.; Malmgren, K.; Rydenhag, B.; Frisen, L. Visual field defects after temporal lobectomy—Comparing methods and analysing resection size. Acta Neurol. Scand. 2004, 110, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Pathak-Ray, V.; Ray, A.; Walters, R.; Hatfield, R. Detection of visual field defects in patients after anterior temporal lobectomy for mesial temporal sclerosis-establishing eligibility to drive. Eye (Lond.) 2002, 16, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Mandelstam, S.A. Challenges of the Anatomy and Diffusion Tensor Tractography of the Meyer Loop. AJNR Am. J. Neuroradiol. 2012, 33, 1204–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japaridze, G.; Kvernadze, D.; Geladze, T.; Kevanishvili, Z. Auditory brain-stem response, middle-latency response, and slow cortical potential in patients with partial epilepsy. Seizure 1997, 6, 449–456. [Google Scholar] [CrossRef]
- Baez-Martin, M.M.; Morales Chacon, L.M.; Garcia-Maeso, I.; Estupiñan-Diaz, B.; Lorigados-Pedre, L.; Garcia, M.E.; Galvizu, R.; Bender, J.E.; Cabrera-Abreu, I.; Perez-Tellez, Y.; et al. Temporal lobe epilepsy surgery modulates the activity of auditory pathway. Epilepsy Res. 2014, 108, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Baez Martin, M.M.; del Carmen Perez, T.Y.; Morales Chacon, L.M.; Diaz, B.E.; Trapaga-Quincoses, O.; Maeso, I.G.; Bender, J.E.; Galvizu, R.; Garcia, M.E.; Abreu, I.C.; et al. Innovative evaluation of visual field defects in epileptic patients after standard anterior temporal lobectomy, using partial field visual evoked potentials. Epilepsy Res. 2010, 90, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Blumcke, I.; Aronica, E.; Urbach, H.; Alexopoulos, A.; Gonzalez-Martinez, J.A. A neuropathology-based approach to epilepsy surgery in brain tumors and proposal for a new terminology use for long-term epilepsy-associated brain tumors. Acta Neuropathol. 2014, 128, 39–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daga, P.; Winston, G.; Modat, M.; White, M.; Mancini, L.; Cardoso, M.J.; Symms, M.; Stretton, J.; McEvoy, A.W.; Thornton, J.; et al. Accurate localization of optic radiation during neurosurgery in an interventional MRI suite. IEEE Trans. Med. Imaging 2012, 31, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Basser, P.J.; Mattiello, J.; LeBihan, D. Estimation of the effective self-diffusion tensor from the NMR spin echo. J. Magn. Reson. B 1994, 103, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Iturria-Medina, Y.; Canales-Rodriguez, E.J.; Melie-Garcia, L.; Valdés-Hernández, P.A.; Martínez-Montes, E.; Alemán-Gómez, Y.; Sánchez-Bornot, J.M. Characterizing brain anatomical connections using diffusion weighted MRI and graph theory. Neuroimage 2007, 36, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Khalfa, S.; Bougeard, R.; Morand, N.; Veuillet, E.; Isnard, J.; Guenot, M.; Ryvlin, P.; Fischer, C.; Collet, L. Evidence of peripheral auditory activity modulation by the auditory cortex in humans. Neuroscience 2001, 104, 347–358. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Weigel, D.; Ganslandt, O.; Buchfelder, M.; Nimsky, C. Prediction of visual field deficits by diffusion tensor imaging in temporal lobe epilepsy surgery. Neuroimage 2009, 45, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Egan, R.A.; Shults, W.T.; So, N.; Burchiel, K.; Kellogg, J.X.; Salinsky, M. Visual field deficits in conventional anterior temporal lobectomy versus amygdalohippocampectomy. Neurology 2000, 55, 1818–1822. [Google Scholar] [CrossRef] [PubMed]
- Guenot, M.; Krolak-Salmon, P.; Mertens, P.; Isnard, J.; Ryvlin, P.; Fischer, C.; Vighetto, A.; Mauguiere, F.; Sindou, M. MRI assessment of the anatomy of optic radiations after temporal lobe epilepsy surgery. Stereotact. Funct. Neurosurg. 1999, 73, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Hervas-Navidad, R.; Altuzarra-Corral, A.; Lucena-Martin, J.A.; Castaneda-Guerrero, M.; Vela-Yebra, R.; Sanchez, A. Defects in the visual field in resective surgery for temporal lobe epilepsy. Rev. Neurol. 2002, 34, 1025–1030. [Google Scholar] [PubMed]
- McDonald, C.R.; Hagler, D.J., Jr.; Girard, H.M.; Pung, C.; Ahmadi, M.E.; Holland, D.; Patel, R.H.; Barba, D.; Tecoma, E.S.; Iragui, V.J.; et al. Changes in fiber tract integrity and visual fields after anterior temporal lobectomy. Neurology 2010, 75, 1631–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mengesha, T.; Abu-Ata, M.; Haas, K.F.; Lavin, P.J.; Sun, D.A.; Konrad, P.E.; Pearson, M.; Wang, L.; Song, Y.; Abou-Khalil, B.W. Visual field defects after selective amygdalohippocampectomy and standard temporal lobectomy. J. Neuroophthalmol. 2009, 29, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Manji, H.; Plant, G.T. Epilepsy surgery, visual fields, and driving: A study of the visual field criteria for driving in patients after temporal lobe epilepsy surgery with a comparison of Goldmann and Esterman perimetry. J. Neurol. Neurosurg. Psychiatry 2000, 68, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Taoka, T.; Sakamoto, M.; Nakagawa, H.; Nakase, H.; Iwasaki, S.; Takayama, K.; Taoka, K.; Hoshida, T.; Sakaki, T.; Kichikawa, K. Diffusion tensor tractography of the Meyer loop in cases of temporal lobe resection for temporal lobe epilepsy: Correlation between postsurgical visual field defect and anterior limit of Meyer loop on tractography. AJNR Am. J. Neuroradiol. 2008, 29, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Winston, G.P.; Daga, P.; Stretton, J.; Modat, M.; Symms, M.R.; McEvoy, A.W.; Ourselin, S.; Duncan, J.S. Optic radiation tractography and vision in anterior temporal lobe resection. Ann. Neurol. 2012, 71, 334–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winston, G.P. Epilepsy surgery, vision, and driving: What has surgery taught us and could modern imaging reduce the risk of visual deficits? Epilepsia 2013, 54, 1877–1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.; Rigolo, L.; O’Donnell, L.J.; Norton, I.; Shriver, S.; Golby, A.J. Visual pathway study using in vivo diffusion tensor imaging tractography to complement classic anatomy. Neurosurgery 2012, 70, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.X.; Zhu, X.L.; Deng, M.; Siu, D.Y.; Leung, J.C.; Chan, Q.; Chan, D.T.; Mak, C.H.; Poon, W.S. The use of diffusion tensor tractography to measure the distance between the anterior tip of the Meyer loop and the temporal pole in a cohort from Southern China. J. Neurosurg. 2010, 113, 1144–1151. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | Sex | Age Years μ (SD) | Duration of Illness Years μ (SD) | Temporo-Mesial Sclerosis N | Focal Cortical Dysplasia | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | F | IIIa | IIIb | No | ||||||
| Patients | ||||||||||
| Left lobectomy | 14 | 5 | 9 | 33.07 (9.06) | 21.14 (9.08) | 14 | 8 | 2 | 4 | |
| Right lobectomy | 13 | 7 | 6 | 34.69 (5.28) | 22.53 (12.14) | 13 | 9 | 1 | 3 | |
| Healthy subjects | 16 | 8 | 8 | 33.68 (7.96) | - | - | - | |||
| Parameters | ABR | MLR | VEP |
|---|---|---|---|
| Analysis time (ms) | 10 | 100 | 300 |
| Filters (Hz) | 100–3000 | 20–1000 | 1–100 |
| Stimulus frequency (Hz) | 10 | 5 | 1 |
| Maximal intensity (dBnHL) | 105 | 90 | - |
| Average responses | 2000 | 500 | 30 |
| Sensibility (μV/div) | 5 | 20 | 20 |
| Recording electrodes | A1, A2 | Cz | O1, Oz, O2 |
| Reference electrode | Cz | A1-A2 | Fz |
| Ground electrode | Fpz | Fpz | A1 |
| Stimulation mode | Monoaural | Binaural | Quadrants |
| Variables | Ipsilateral Auditory Radiation | Contralateral Auditory Radiation | |||
|---|---|---|---|---|---|
| µ | SD | µ | SD | p | |
| Density of connection | 0.193 | 0.0773 | 0.251 | 0.0660 | 0.026 * |
| Density of connection (FA) | 0.068 | 0.0293 | 0.093 | 0.0189 | 0.0800 |
| Density of connection (MD) | 0.080 | 0.0306 | 0.112 | 0.0261 | 0.0652 |
| Anatomical Connection probability | 0.422 | 0.1613 | 0.498 | 0.1172 | 0.3981 |
| Anatomical Connection probability (FA) | 0.181 | 0.0992 | 0.210 | 0.0372 | 0.4783 |
| Anatomical Connection probability (MD) | 0.193 | 0.0965 | 0.230 | 0.0565 | 0.4317 |
| Anatomical connection strength | 726.900 | 402.7487 | 1214.176 | 330.9955 | 0.0346 * |
| Anatomical connection strength (FA) | 257.677 | 149.3024 | 449.342 | 100.6329 | 0.020 * |
| Anatomical connection strength (MD) | 302.172 | 161.8940 | 542.212 | 135.5526 | 0.0214 * |
| Na Latency | Pa Latency | Nb Latency | Na Amplitude | |
|---|---|---|---|---|
| Mesial length of resection | +0.13 | +0.51 * | +0.48 * | −0.39 |
| Neocortical length of resection ** | +0.61 * | +0.31 | +0.21 | +0.16 |
| Anatomical connection probability (FA) ** | −0.88 * | −0.86 | −0.89 * | +0.92 * |
| Anatomical connection strength (FA) * | −0.87 | −0.89 * | −0.89 * | 0.83 |
| Ipsilateral | Contralateral | |||||
|---|---|---|---|---|---|---|
| µ | SD | µ | SD | p | ||
| OR | Number of tracts ** | 356.625 | 185.997 | 578.500 | 155.902 | 0.0041 * |
| Length of tracts | 19.671 | 7.139 | 26.870 | 7.557 | 0.0307 * | |
| Volume of tracts | 3167.500 | 1339.976 | 4368.750 | 1462.917 | 0.1988 | |
| FA | 0.403 | 0.127 | 0.499 | 0.031 | 0.0587 | |
| ADC | 0.001 | 0.000 | 0.001 | 0.000 | 0.1448 | |
| AD | 0.001 | 0.000 | 0.001 | 0.000 | 0.3502 | |
| RD | 0.001 | 0.000 | 0.001 | 0.000 | 0.1228 | |
| OC | Number of tracts | 1961.87 | 832.04 | 2971.25 | 661.71 | 0.0017 * |
| Length of tracts | 14.986 | 4.748 | 18.190 | 2.669 | 0.1127 | |
| Volume of tracts | 7396.25 | 3425.97 | 9145.00 | 2655.12 | 0.0499 * | |
| FA | 0.348 | 0.083 | 0.388 | 0.099 | 0.0026 * | |
| ADC | 0.001 | 0.000 | 0.001 | 0.000 | 0.1062 | |
| AD | 0.001 | 0.000 | 0.001 | 0.000 | 0.7131 | |
| RD | 0.001 | 0.000 | 0.001 | 0.000 | 0.0741 | |
| Ipsilateral | Contralateral | ||||
|---|---|---|---|---|---|
| µ | SD | µ | SD | p | |
| Anatomical connection density | 0.155 | 0.0733 | 0.174 | 0.0757 | 0.6104 |
| Anatomical connection density (FA) | 0.050 | 0.0271 | 0.069 | 0.0323 | 0.2115 |
| Anatomical connection density (MD) | 0.059 | 0.0306 | 0.075 | 0.0305 | 0.3426 |
| Anatomical connection probability | 0.387 | 0.1810 | 0.404 | 0.1292 | 0.8029 |
| Anatomical connection probability (FA) | 0.134 | 0.0711 | 0.174 | 0.0512 | 0.2581 |
| Anatomical connection probability (MD) | 0.178 | 0.0885 | 0.181 | 0.0537 | 0.9418 |
| Anatomical connection strength | 890.987 | 450.569 | 1239.440 | 610.7670 | 0.2174 |
| Anatomical connection strength (FA) | 290.970 | 171.595 | 487.988 | 260.4703 | 0.0958 |
| Anatomical connection strength (MD) | 342.933 | 188.255 | 531.343 | 253.9019 | 0.1243 |
| (A) Optic Radiations | P100 Latency | P100 Amplitude | Perimetry (VFD-I) | ||||
| Electrodes | O1 | Oz | O2 | O1 | Oz | O2 | |
| Perimetry | +0.53 | +0.50 | +0.50 | ||||
| Neocortical length of resection | +0.61 | +0.60 | +0.59 | +0.72 | |||
| FA * | −0.96 | −0.98 | −0.97 | −0.73 | |||
| ADC * | +0.98 | +0.97 | +0.98 | ||||
| Axial diffusivity * | +0.99 | +0.99 | +0.99 | ||||
| Radial diffusivity * | +0.99 | +0.99 | +0.99 | ||||
| Connection density | −0.79 | −0.78 | −0.78 | +0.76 | |||
| Connection probability | −0.89 | −0.87 | −0.86 | ||||
| Connection strength | −0.88 | −0.88 | −0.89 | +0.74 | |||
| (B) Occipital Cortex | P100 Latency | P100 Amplitude | Perimetry (VFD-I) | ||||
| Electrodes | O1 | Oz | O2 | O1 | Oz | O2 | |
| Number of tracts | +0.86 | ||||||
| Volume of tracts | +0.87 | +0.94 | +0.80 | ||||
| FA | +0.82 | −0.71 | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Báez-Martín, M.M.; Morales-Chacón, L.M.; García-Maeso, I.; Estupiñán-Díaz, B.; García-Navarro, M.E.; Pérez Téllez, Y.; Lorigados-Pedre, L.; Quintanal-Cordero, N.; Valdés-Llerena, R.; González González, J.; et al. Relation of Structural and Functional Changes in Auditory and Visual Pathways after Temporal Lobe Epilepsy Surgery. Behav. Sci. 2018, 8, 92. https://doi.org/10.3390/bs8100092
Báez-Martín MM, Morales-Chacón LM, García-Maeso I, Estupiñán-Díaz B, García-Navarro ME, Pérez Téllez Y, Lorigados-Pedre L, Quintanal-Cordero N, Valdés-Llerena R, González González J, et al. Relation of Structural and Functional Changes in Auditory and Visual Pathways after Temporal Lobe Epilepsy Surgery. Behavioral Sciences. 2018; 8(10):92. https://doi.org/10.3390/bs8100092
Chicago/Turabian StyleBáez-Martín, Margarita Minou, Lilia Maria Morales-Chacón, Iván García-Maeso, Bárbara Estupiñán-Díaz, María Eugenia García-Navarro, Yamila Pérez Téllez, Lourdes Lorigados-Pedre, Nelson Quintanal-Cordero, Ricardo Valdés-Llerena, Judith González González, and et al. 2018. "Relation of Structural and Functional Changes in Auditory and Visual Pathways after Temporal Lobe Epilepsy Surgery" Behavioral Sciences 8, no. 10: 92. https://doi.org/10.3390/bs8100092
APA StyleBáez-Martín, M. M., Morales-Chacón, L. M., García-Maeso, I., Estupiñán-Díaz, B., García-Navarro, M. E., Pérez Téllez, Y., Lorigados-Pedre, L., Quintanal-Cordero, N., Valdés-Llerena, R., González González, J., Garbey-Fernández, R., Cabrera-Abreu, I., Alarcón-Calaña, C., Bender del Busto, J. E., Rodríguez Rojas, R., Batista García-Ramó, K., & Galvizu Sánchez, R. (2018). Relation of Structural and Functional Changes in Auditory and Visual Pathways after Temporal Lobe Epilepsy Surgery. Behavioral Sciences, 8(10), 92. https://doi.org/10.3390/bs8100092