A Study on Technology Acceptance of Digital Healthcare among Older Korean Adults Using Extended Tam (Extended Technology Acceptance Model)




Abstract
:1. Introduction
2. Literature Review
2.1. Elderly Perception and Their Acceptability of Technology Use in Healthcare
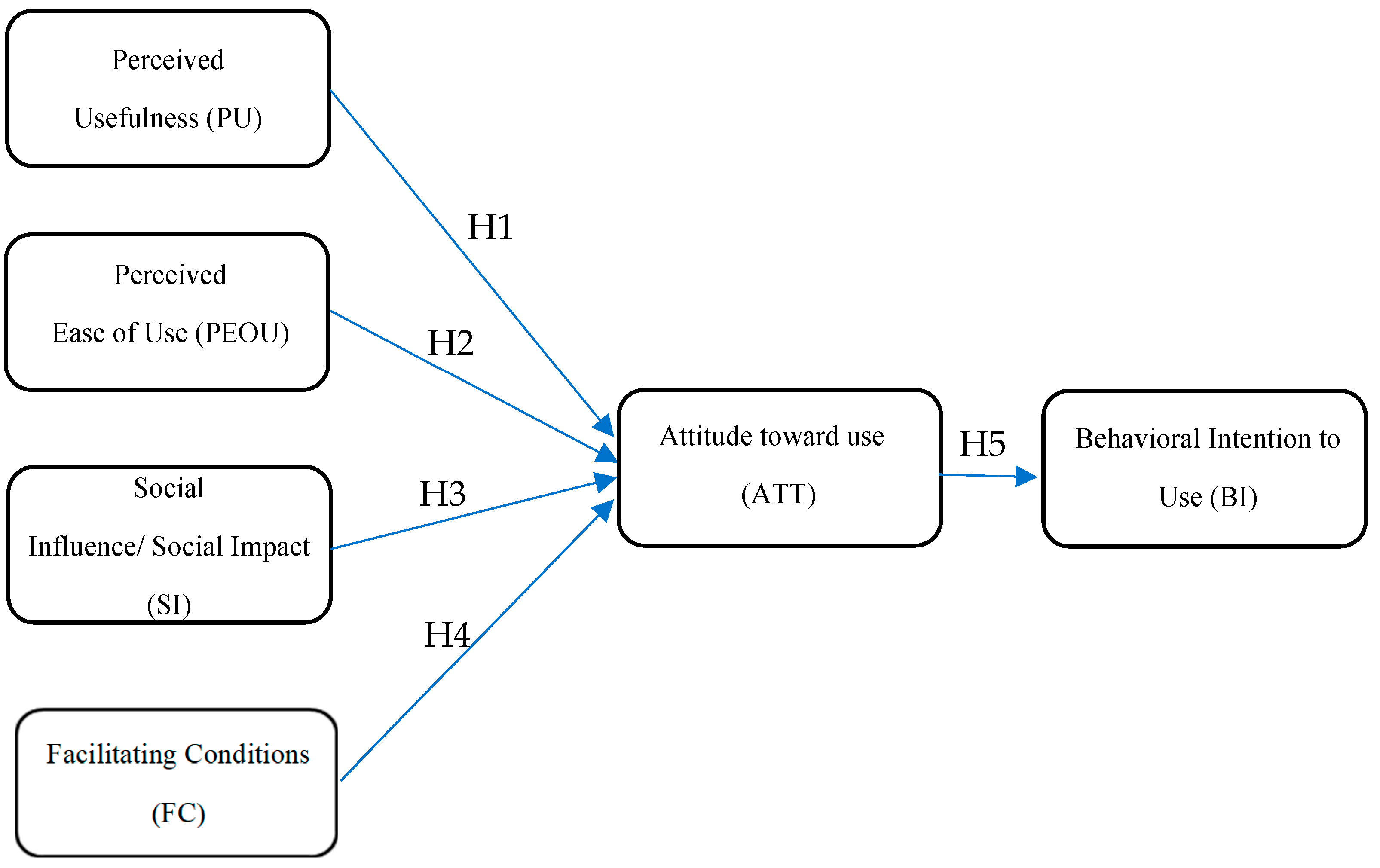
2.2. Theoretical Framework: Technology Acceptance Model
2.3. Hypothesis Development
2.3.1. Perceived Usefulness and Perceived Ease of Use
2.3.2. Social Influence/Social Impact
2.3.3. Facilitating Conditions
2.3.4. Attitude towards Using
2.3.5. Behavioral Intention to Use
3. Methodology
3.1. Data Collection
3.2. Measurement Instruments
3.3. Data Analysis Procedure
4. Results
4.1. Demographic Characteristics
4.2. Measurement Model
4.3. Hypothesis Testing
5. Discussion and Conclusions
5.1. Theoretical Implications
5.2. Practical Implications
6. Limitations and Directions for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdul Rahman, Mahera, Fatema Al-Tahri, Mouza Khalifa Al Mehairi, Frederick Robert Carrick, and Alia Mohammad Rafi Aldallal. 2022. Digital Health Technology for Remote Care in Primary Care During the COVID-19 Pandemic: Experience from Dubai. Telemedicine and E-Health 28: 1100–8. [Google Scholar] [CrossRef]
- Abrashkin, Karen A., Jenny Zhang, and Asantewaa Poku. 2021. Acute, Post-Acute, and Primary Care Utilization in a Home-Based Primary Care Program during COVID-19. Gerontologist 61: 78–85. [Google Scholar] [CrossRef] [PubMed]
- Ahlan, Abd Rahman, and Barroon Isma’eel Ahmad. 2015. An Overview of Patient Acceptance of Health Information Technology in Developing Countries: A Review and Conceptual Model. International Journal of Information Systems and Project Management 3: 29–48. [Google Scholar] [CrossRef]
- Ahmad, Ashfaq, Tareq Rasul, Anish Yousaf, and Umer Zaman. 2020. Understanding Factors Influencing Elderly Diabetic Patients’ Continuance Intention to Use Digital Health Wearables: Extending the Technology Acceptance Model (TAM). Journal of Open Innovation: Technology, Market, and Complexity 6: 81. [Google Scholar] [CrossRef]
- Ahmad, Nurul Asilah, Arimi Fitri Mat Ludin, Suzana Shahar, Shahrul Azman Mohd Noah, and Noorlaili Mohd Tohit. 2022. Willingness, Perceived Barriers and Motivators in Adopting Mobile Applications for Health-Related Interventions among Older Adults: A Scoping Review. BMJ Open 12: e054561. [Google Scholar] [CrossRef]
- Ajzen, Icek. 1991. The Theory of Planned Behavior. Organizational Behavior and Human Decision Processes 50: 179–211. [Google Scholar] [CrossRef]
- Ajzen, Icek. 2015. Belief, Attitude, Intention and Behaviour: An Introduction to Theory and Research. Boston: Addison-Wesley. [Google Scholar]
- An, Min Ho, Seng Chan You, Rae Woong Park, and Seongwon Lee. 2021. Using an Extended Technology Acceptance Model to Understand the Factors Influencing Telehealth Utilization after Flattening the COVID-19 Curve in South Korea: Cross-Sectional Survey Study. JMIR Medical Informatics 9: e25435. [Google Scholar] [CrossRef]
- An, Soontae, Hannah Kang, and Soondool Chung. 2018. Older Adults’ Adoption of Health-Related Mobile Application: The Role of Empowerment. Journal of Public Relations 22: 53–74. [Google Scholar] [CrossRef]
- Andersen, Ronald M. 1995. Revisiting the Behavioral Model and Access to Medical Care: Does It Matter? Journal of Health and Social Behavior 36: 1–10. [Google Scholar] [CrossRef]
- Bagozzi, Richard P., and Youjae Yi. 1991. Multitrait-Multimethod Matrices in Consumer Research. Journal of Consumer Research 17: 426–39. [Google Scholar] [CrossRef]
- Cardozo, Lavoisier, and Joel Steinberg. 2010. Telemedicine for Recently Discharged Older Patients. Telemedicine and E-Health 16: 49–55. [Google Scholar] [CrossRef] [PubMed]
- Chen, Ke, and Alan Hoi Shou Chan. 2011. A Review of Technology Acceptance by Older Adults. Gerontechnology 10: 1–12. [Google Scholar] [CrossRef]
- Chen, Ke, and Alan Hoi Shou Chan. 2014a. Predictors of Gerontechnology Acceptance by Older Hong Kong Chinese. Technovation 34: 126–35. [Google Scholar] [CrossRef]
- Chen, Ke, and Alan Hoi Shou Chan. 2014b. Gerontechnology Acceptance by Elderly Hong Kong Chinese: A Senior Technology Acceptance Model (STAM). Ergonomics 57: 635–52. [Google Scholar] [CrossRef]
- Chen, Ke, Vivian Wei Qun Lou, and Selina Siu Ching Lo. 2021. Exploring the Acceptance of Tablets Usage for Cognitive Training among Older People with Cognitive Impairments: A Mixed-Methods Study. Applied Ergonomics 93: 103381. [Google Scholar] [CrossRef]
- Choi, Ji-Yeon. 2018. A Study on Solitary Death Prevention Policies. Graduate school of Public Health Thesis Publication, Yonsei University. Available online: https://ir.ymlib.yonsei.ac.kr/handle/22282913/166342 (accessed on 4 November 2022).
- Chung, Jane, Hilaire J. Thompson, Jonathan Joe, Amanda Hall, and George Demiris. 2017. Examining Korean and Korean American Older Adults’ Perceived Acceptability of Home-Based Monitoring Technologies in the Context of Culture. Informatics for Health and Social Care 42: 61–76. [Google Scholar] [CrossRef]
- Cohen, Jason F., Jean-Marie Bancilhon, and Michael Jones. 2013. South African Physicians’ Acceptance of e-Prescribing Technology: An Empirical Test of a Modified UTAUT Model. South African Computer Journal 50: 43–54. Available online: https://journals.co.za/doi/abs/10.10520/EJC139543 (accessed on 6 December 2022). [CrossRef]
- Czaja, Sara J., Neil Charness, Arthur D. Fisk, Christopher Hertzog, Sankaran N. Nair, Wendy A. Rogers, and Joseph Sharit. 2006. Factors Predicting the Use of Technology: Findings from the Center for Research and Education on Aging and Technology Enhancement (Create). In Psychology and Aging. Arlington: American Psychological Association. [Google Scholar] [CrossRef]
- Davis, Fred D. 1989. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Quarterly: Management Information Systems 13: 319–39. [Google Scholar] [CrossRef]
- Davis, Fred D., Richard P. Bagozzi, and Paul R. Warshaw. 1989. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Management Science 35: 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Demiris, George, Brian K. Hensel, Marjorie Skubic, and Marilyn Rantz. 2008. Senior Residents’ Perceived Need of and Preferences for ‘Smart Home’ Sensor Technologies. International Journal of Technology Assessment in Health Care 24: 120–24. [Google Scholar] [CrossRef] [PubMed]
- Deng, Zhaohua, Xiuting Mo, and Shan Liu. 2014. Comparison of the Middle-Aged and Older Users’ Adoption of Mobile Health Services in China. International Journal of Medical Informatics 83: 210–24. [Google Scholar] [CrossRef] [PubMed]
- Eun, Ki Soo. 2008. Population Aging and Social Strategies for Aging Problems in Korea. Korea Journal 48: 5–34. [Google Scholar] [CrossRef]
- Farivar, Samira, Mohamed Abouzahra, and Maryam Ghasemaghaei. 2020. Wearable Device Adoption among Older Adults: A Mixed-Methods Study. International Journal of Information Management 55: 102209. [Google Scholar] [CrossRef]
- Gagnon, Marie-Pierre, Marie Desmartis, Michel Labrecque, Josip Car, Claudia Pagliari, Pierre Pluye, Pierre Frémont, Johanne Gagnon, Nadine Tremblay, and France Légaré. 2012. Systematic review of factors influencing the adoption of information and communication technologies by healthcare professionals. Journal of Medical Systems 36: 241–77. [Google Scholar] [CrossRef]
- Garavand, Ali, Mohammah Mohseni, Heshmatollah Asadi, Manal Etemadi, Mohammad Moradi-Joo, and Ahmad Moosavi. 2016. Factors Influencing the Adoption of Health Information Technologies: A Systematic Review. Electronic Physician 8: 2713. [Google Scholar] [CrossRef] [PubMed]
- Gordon, Lachlan A. N. 2018. Assessment of Smart Watches for Management of Non-Communicable Diseases in the Ageing Population: A Systematic Review. Geriatrics 3: 56. [Google Scholar] [CrossRef]
- Guner, Hacer, and Cengiz Acarturk. 2020. The Use and Acceptance of ICT by Senior Citizens: A Comparison of Technology Acceptance Model (TAM) for Elderly and Young Adults. Universal Access in the Information Society 19: 311–30. [Google Scholar] [CrossRef]
- Ha, Jiyeon, and Hyeyoung K. Park. 2020. Factors Affecting the Acceptability of Technology in Health Care among Older Korean Adults with Multiple Chronic Conditions: A Cross-Sectional Study Adopting the Senior Technology Acceptance Model. Clinical Interventions in Aging 15: 1873–81. [Google Scholar] [CrossRef]
- Hanafi, Hafizul Fahri, Mohd Helmy Wahab, Kung Teck Wong, Abu Zarrin Selamat, Muhamad Hariz Muhamad Adnan, and Fatin Hana Naning. 2020. Mobile Augmented Reality Hand Wash (MARHw): Mobile Application to Guide Community to Ameliorate Handwashing Effectiveness to Oppose COVID-19 Disease. International Journal of Integrated Engineering 12: 217–23. [Google Scholar] [CrossRef]
- Heinz, Melinda, Peter Martin, Jennifer A. Margrett, Mary Yearns, Warren Franke, Hen I. Yang, Johnny Wong, and Carl K. Chang. 2013. Perceptions of Technology among Older Adults. Journal of Gerontological Nursing 39: 42–51. [Google Scholar] [CrossRef]
- Holden, Richard J., and Ben Tzion Karsh. 2010. The Technology Acceptance Model: Its Past and Its Future in Health Care. Journal of Biomedical Informatics 43: 159–72. [Google Scholar] [CrossRef]
- Holtz, Bree, and Sarah Krein. 2011. Understanding Nurse Perceptions of a Newly Implemented Electronic Medical Record System. Journal of Technology in Human Services 29: 247–62. [Google Scholar] [CrossRef]
- Hong, Sung Jung, Sung-Hyun Lee, and Kyung Mi Kim. 2020. A Study on the Influence of Usage Intention of IoT Healthcare Service for Elderly. Journal of the Korea Convergence Society 11: 341–49. [Google Scholar] [CrossRef]
- Hoque, Rakibul, and Golam Sorwar. 2017. Understanding Factors Influencing the Adoption of MHealth by the Elderly: An Extension of the UTAUT Model. International Journal of Medical Informatics 101: 75–84. [Google Scholar] [CrossRef] [PubMed]
- Hu, Paul J., Patrick Y.K. Chau, Olivia R. Liu Sheng, and Kar Yan Tam. 1999. Examining the Technology Acceptance Model Using Physician Acceptance of Telemedicine Technology. Undefined 16: 91–112. [Google Scholar] [CrossRef]
- Hur, Hwa-La, and Myeong-Chul Park. 2020. Design of Monitoring System Based on IoT Sensor for Health Management of an Elderly Alone. Journal of The Korea Society of Computer and Information 25: 81–87. [Google Scholar] [CrossRef]
- Jo, Heui Sug, Yu Seong Hwang, and Yuliya Dronina. 2021a. Mediating Effects of Smartphone Utilization between Attitude and Willingness to Use Home-Based Healthcare Ict among Older Adults. Healthcare Informatics Research 27: 137–45. [Google Scholar] [CrossRef]
- Jo, Tae Hee, Jae Hoon Ma, and Seung Hyun Cha. 2021b. Elderly Perception on the Internet of Things-Based Integrated Smart-Home System. Sensors 21: 1284. [Google Scholar] [CrossRef]
- Kapadia, Vasvi, Arni Ariani, Junhua Li, and Pradeep K. Ray. 2015. Emerging ICT Implementation Issues in Aged Care. International Journal of Medical Informatics 84: 892–900. [Google Scholar] [CrossRef]
- Kijsanayotin, Boonchai, Supasit Pannarunothai, and Stuart M. Speedie. 2009. Factors Influencing Health Information Technology Adoption in Thailand’s Community Health Centers: Applying the UTAUT Model. International Journal of Medical Informatics 78: 404–16. [Google Scholar] [CrossRef] [PubMed]
- Kim, Tae-Ho, and Hak-Seon Kim. 2016. Delivery app understanding and acceptance among food tech customers using the modified technology acceptance model. Journal of Tourism Sciences 40: 127–44. [Google Scholar] [CrossRef]
- Kim, Tae Kyung, and Moon Choi. 2019. Older Adults’ Willingness to Share Their Personal and Health Information When Adopting Healthcare Technology and Services. International Journal of Medical Informatics 126: 86–94. [Google Scholar] [CrossRef]
- Lazaro, May Jorella S., Jaeseo Lim, Sung Ho Kim, and Myung Hwan Yun. 2020. Wearable Technologies: Acceptance Model for Smartwatch Adoption among Older Adults. Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). Vol. 12207 LNCS. Belin: Springer International Publishing. [Google Scholar] [CrossRef]
- Lee, Chaiwoo, and Joseph F. Coughlin. 2015. PERSPECTIVE: Older Adults’ Adoption of Technology: An Integrated Approach to Identifying Determinants and Barriers. Journal of Product Innovation Management 32: 747–59. [Google Scholar] [CrossRef]
- Li, Junde, Qi Ma, Alan H. S. Chan, and Siushing Man. 2019. Health Monitoring through Wearable Technologies for Older Adults: Smart Wearables Acceptance Model. Applied Ergonomics 75: 162–69. [Google Scholar] [CrossRef] [PubMed]
- Liang, Huigang, Yajiong Xue, and Terry Anthony Byrd. 2003. PDA Usage in Healthcare Professionals: Testing an Extended Technology Acceptance Model. International Journal of Mobile Communications 1: 372–89. [Google Scholar] [CrossRef]
- Liu, Dewen, Qi Li, and Shenghao Han. 2022. Using Extended Technology Acceptance Model to Assess the Adopt Intention of a Proposed IoT-Based Health Management Tool. Sensors 22: 6092. [Google Scholar] [CrossRef] [PubMed]
- Liu, Liping, and Qingxiong Ma. 2006. Perceived System Performance:A Test of an Extended Technology Acceptance Model. Data Base for Advances in Information Systems 37: 51–59. [Google Scholar] [CrossRef]
- Lorenzen-Huber, Lesa, Mary Boutain, L. Jean Camp, Kalpana Shankar, and Kay H. Connelly. 2011. Privacy, Technology, and Aging: A Proposed Framework. Ageing International 36: 232–52. [Google Scholar] [CrossRef] [Green Version]
- Macedo, Isabel Maria. 2017. Predicting the Acceptance and Use of Information and Communication Technology by Older Adults: An Empirical Examination of the Revised UTAUT2. Computers in Human Behavior 75: 935–48. [Google Scholar] [CrossRef]
- Mitzner, Tracy L., Julie B. Boron, Cara Bailey Fausset, Anne E. Adams, Neil Charness, Sara J. Czaja, Katinka Dijkstra, Arthur D. Fisk, Wendy A. Rogers, and Joseph Sharit. 2010. Older Adults Talk Technology: Technology Usage and Attitudes. Computers in Human Behavior 26: 1710–21. [Google Scholar] [CrossRef] [PubMed]
- Mostaghel, Rana, and Pejvak Oghazi. 2017. Elderly and Technology Tools: A Fuzzyset Qualitative Comparative Analysis. Quality and Quantity 51: 1969–82. [Google Scholar] [CrossRef] [PubMed]
- Or, Calvin K.L., Ben Tzion Karsh, Dolores J. Severtson, Laura J. Burke, Roger L. Brown, and Patricia Flatley Brennan. 2011. Factors Affecting Home Care Patients’ Acceptance of a Web-Based Interactive Self-Management Technology. Journal of the American Medical Informatics Association 18: 51–59. [Google Scholar] [CrossRef]
- Palmiero, Massimiliano, Raffaella Nori, and Laura Piccardi. 2016. Verbal and Visual Divergent Thinking in Aging. Experimental Brain Research 235: 1021–29. [Google Scholar] [CrossRef]
- Pan, Shuya, and Maryalice Jordan-Marsh. 2010. Internet Use Intention and Adoption among Chinese Older Adults: From the Expanded Technology Acceptance Model Perspective. Computers in Human Behavior 26: 1111–19. [Google Scholar] [CrossRef]
- Peek, Sebastiaan T. M., Katrien G. Luijkx, Maurice D. Rijnaard, Marianne E. Nieboer, Claire S. Van Der Voort, Sil Aarts, Joost Van Hoof, Hubertus J.M. Vrijhoef, and Eveline J.M. Wouters. 2016. Older Adults’ Reasons for Using Technology While Aging in Place. Gerontology 62: 226–37. [Google Scholar] [CrossRef] [PubMed]
- Porter, Eileen J., and Lawrence H. Ganong. 2002. Considering the Use of a Personal Emergency Response System: An Experience of Frail, Older Women. Care Management Journals 3: 192–98. [Google Scholar] [CrossRef]
- Rahimi, Bahlol, Hamed Nadri, Hadi Lotfnezhad Afshar, and Toomas Timpka. 2018. A Systematic Review of the Technology Acceptance Model in Health Informatics. Applied Clinical Informatics 9: 604–34. [Google Scholar] [CrossRef]
- Rawstorne, Patrick, Rohan Jayasuriya, and Peter Caputi. 2000. Issues in Predicting and Explaining Usage Behaviors with the Technology Acceptance Model and the Theory of Planned Behavior When Usage Is Mandatory. Paper presented at ICIS 2000 Proceedings, Brisbane, Australia, December 10–13; Available online: https://aisel.aisnet.org/icis2000/5 (accessed on 7 September 2022).
- Shin, Hye-Ri, Hee-Jeong Yoon, Su-Kyoung Kim, and Young-Sun Kim. 2020. Comprehensive Senior Technology Acceptance Model for Digital Health Devices. Journal of Digital Convergence 18: 201–15. [Google Scholar] [CrossRef]
- Statistics Korea. 2021. “2021 Statistics on the Aged”. Available online: http://kostat.go.kr/portal/eng/pressReleases/11/3/index.board (accessed on 8 August 2022).
- Steele, Robert, Amanda Lo, Chris Secombe, and Yuk Kuen Wong. 2009. Elderly Persons’ Perception and Acceptance of Using Wireless Sensor Networks to Assist Healthcare. International Journal of Medical Informatics 78: 788–801. [Google Scholar] [CrossRef]
- Tural, Elif, Danni Lu, and D. Austin Cole. 2020. Factors Predicting Older Adults’ Attitudes toward and Intentions to Use Stair Mobility Assistive Designs at Home. Preventive Medicine Reports 18: 101082. [Google Scholar] [CrossRef] [PubMed]
- Vassli, Lars Tore, and Babak A. Farshchian. 2018. Acceptance of Health-Related ICT among Elderly People Living in the Community: A Systematic Review of Qualitative Evidence. International Journal of Human-Computer Interaction 34: 99–116. [Google Scholar] [CrossRef]
- Venkatesh, Viswanath, and Fred D. Davis. 2000. A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. Management Science 46: 186–204. [Google Scholar] [CrossRef]
- Venkatesh, Viswanath, James Y. L. Thong, and Xin Xu. 2012. Consumer Acceptance and Use of Information Technology: Extending the Unified Theory of Acceptance and Use of Technology. MIS Quarterly: Management Information Systems 36: 157–78. [Google Scholar] [CrossRef]
- Venkatesh, Viswanath, James Y. L. Thong, Frank K. Y. Chan, Paul Jen Hwa Hu, and Susan A. Brown. 2011. Extending the Two-Stage Information Systems Continuance Model: Incorporating UTAUT Predictors and the Role of Context. Information Systems Journal 21: 527–55. [Google Scholar] [CrossRef]
- Venkatesh, Viswanath, Michael G. Morris, Gordon B. Davis, and Fred D. Davis. 2003. User Acceptance of Information Technology: Toward a Unified View. MIS Quarterly: Management Information Systems 27: 425–78. [Google Scholar] [CrossRef]
- Vidal-Alaball, Josep, Ruthy Acosta-Roja, Nuria PastorHernández, Unai SanchezLuque, Danielle Morrison, Silvia NarejosPérez, Jesús Perez-Llano, Angels Salvador Vèrges, and Francesc López Seguí. 2020. Telemedicine in the Face of the COVID-19 Pandemic. Atencion Primaria 52: 418–22. [Google Scholar] [CrossRef]
- Wildenbos, Gaby Anne, Linda Peute, and Monique Jaspers. 2018. Aging Barriers Influencing Mobile Health Usability for Older Adults: A Literature Based Framework (MOLD-US). International Journal of Medical Informatics 114: 66–75. [Google Scholar] [CrossRef]
- Wills, Matthew J., Omar F. El-gayar, and Dorine Bennett. 2008. Examining Healthcare Professionals’ Acceptance of Electronic Medical Records Using Utaut. Issues In Information Systems 9: 396–401. [Google Scholar] [CrossRef]
- Wilson, Jessica, Milena Heinsch, David Betts, Debbie Booth, and Frances Kay-Lambkin. 2021. Barriers and Facilitators to the Use of E-Health by Older Adults: A Scoping Review. BMC Public Health 21: 1–12. [Google Scholar] [CrossRef]
- Wu, Juanjuan, and Sanga Song. 2021. Older Adults’ Online Shopping Continuance Intentions: Applying the Technology Acceptance Model and the Theory of Planned Behavior. International Journal of Human-Computer Interaction 37: 938–48. [Google Scholar] [CrossRef]
- Yang, Heetae, Jieun Yu, Hangjung Zo, and Munkee Choi. 2016. User Acceptance of Wearable Devices: An Extended Perspective of Perceived Value. Telematics and Informatics 33: 256–69. [Google Scholar] [CrossRef]
- Yap, Yee Yann, Siow Hooi Tan, and Shay Wei Choon. 2022. Elderly’s Intention to Use Technologies: A Systematic Literature Review. Heliyon 8: e08765. [Google Scholar] [CrossRef] [PubMed]
- Yein, Nilakshi, and Swati Pal. 2021. Analysis of the User Acceptance of Exergaming (Fall- Preventive Measure)—Tailored for Indian Elderly Using Unified Theory of Acceptance and Use of Technology (UTAUT2) Model. Entertainment Computing 38: 100419. [Google Scholar] [CrossRef]
- Yi, Mun Y., Joyce D. Jackson, Jae S. Park, and Janice C. Probst. 2006. Understanding Information Technology Acceptance by Individual Professionals: Toward an Integrative View. Information & Management 43: 350–63. [Google Scholar] [CrossRef]
- Yoo, Hyun-Sil, Eung-Kyo Suh, and Tae-Hyung Kim. 2020. A Study on Technology Acceptance of Elderly Living Alone in Smart City Environment: Based on AI Speaker. Journal of Industrial Distribution & Business 11: 41–48. [Google Scholar] [CrossRef]


{kind=link}
| Construct | Item | Measurements | Reference |
|---|---|---|---|
| Perceived Usefulness | PU1 | Health Care Using a smart watch will help me manage my health. | (Venkatesh and Davis 2000) |
| PU2 | I believe that using a health care smart watch will make my daily life safer. | ||
| PU3 | Using a health care smart watch will improve my quality of life. | ||
| Perceived Ease of Use | PEOU1 | I think using a health care smart watch would be simple. | (Venkatesh and Davis 2000) |
| PEOU2 | Learning to use a health care smart watch will be easy. | ||
| PEOU3 | Health care smart watch will be convenient to use. | ||
| Social impact or Influence | SI1 | Family will approve of my use of a health care smart watch. | (Venkatesh et al. 2011, 2003; Ahmad et al. 2020) |
| SI2 | Acquaintances will recommend that I use a health care smart watch. | ||
| SI3 | Acquaintances will approve of me using a health care smart watch. | ||
| Facilitating conditions | FC1 | I will know how to use the health care smart watch. | (Venkatesh et al. 2011, 2003; Liu et al. 2022) |
| FC2 | If I encounter difficulties using your health care smart watch, I think someone will be able to help. | ||
| FC3 | I have sufficient financial resources to use a health care smart watch. | ||
| Attitude towards use | ATT1 | Using a health care smart watch will have a positive impact on my life | (Ajzen 2015; Venkatesh et al. 2003) |
| ATT2 | Using a health care smart watch will benefit my health. | ||
| ATT3 | I have positive thoughts about health care smart watches. | ||
| Behavioral Intention to Use | BI1 | I would use a health care smart watch if given the opportunity. | (Venkatesh and Davis 2000) |
| BI2 | I will use a health care smart watch for my health care. | ||
| BI3 | I will use a health care smart watch to change my life for the better. |
| Frequency (N = 170) | Percent | Mean | SD | ||
|---|---|---|---|---|---|
| Age | 56~65 | 55 | 32.4 | 1.84 | 0.685 |
| 66~75 | 89 | 52.4 | |||
| 76~85 | 25 | 14.7 | |||
| 86~95 | 1 | 0.6 | |||
| Gender | Male | 75 | 44.1 | 1.56 | 0.498 |
| Female | 95 | 55.9 | |||
| Occupation | Office worker | 18 | 10.6 | ||
| Professional | 18 | 10.6 | 3.90 | 1.454 | |
| Self-employed | 26 | 15.3 | |||
| Public official | 9 | 5.3 | |||
| Dependent | 99 | 58.2 | |||
| Number of people living together with | 1 | 12 | 7.1 | 2.84 | 0.965 |
| 2 | 59 | 34.7 | |||
| 3 | 44 | 25.9 | |||
| 4 and above | 55 | 32.4 | |||
| Income | <500,000 won | 13 | 7.6 | 3.33 | 1.249 |
| 500,000~ 1 million | 34 | 20 | |||
| 1–2 million | 47 | 27.6 | |||
| 2–3 million | 36 | 21.2 | |||
| >3 million | 40 | 23.5 | |||
| Expense | <500,000 won | 16 | 9.4 | ||
| 500,000~ 1 million | 46 | 27.1 | 3.02 | 1.174 | |
| 1–2 million | 48 | 28.2 | |||
| 2–3 million | 39 | 22.9 | |||
| >3 million | 21 | 12.4 | |||
| * Chronic diseases | No disease | 31 | 18.2 | ||
| Hypertension | 63 | 37.1 | |||
| Heart disease | 31 | 18.2 | |||
| Diabetes | 61 | 35.9 | |||
| Gastrointestinal | 28 | 16.5 | |||
| Arthritis | 44 | 25.9 | |||
| Dementia | 11 | 6.5 | |||
| Dyslipidemia | 6 | 3.5 |
| Constructs | Item | Loading | VIF | SMC | Composite Reliability | AVE | Cronbach’s α |
|---|---|---|---|---|---|---|---|
| Perceived Usefulness | PU1 | 0.896 | 2.367 | 0.803 | 0.926 | 0.808 | 0.881 |
| PU2 | 0.904 | 2.617 | 0.817 | ||||
| PU3 | 0.896 | 2.400 | 0.803 | ||||
| Perceived Ease of Use | PEOU1 | 0.924 | 3.335 | 0.854 | 0.939 | 0.838 | 0.903 |
| PEOU2 | 0.934 | 3.764 | 0.872 | ||||
| PEOU3 | 0.887 | 2.351 | 0.787 | ||||
| Social Influence or Impact | S1 | 0.892 | 2.318 | 5.373 | 0.922 | 0.798 | 0.874 |
| S2 | 0.872 | 2.178 | 4.744 | ||||
| S3 | 0.916 | 2.746 | 7.541 | ||||
| Facilitating Condition | FC1 | 0.890 | 2.156 | 0.792 | 0.918 | 0.788 | 0.865 |
| FC2 | 0.899 | 2.454 | 0.808 | ||||
| FC3 | 0.874 | 2.175 | 0.764 | ||||
| Attitude towards use | ATT1 | 0.894 | 2.295 | 0.799 | 0.922 | 0.797 | 0.873 |
| ATT2 | 0.893 | 2.375 | 0.797 | ||||
| ATT3 | 0.891 | 2.328 | 0.794 | ||||
| Behavioral Intention to use | BI1 | 0.899 | 2.492 | 0.808 | 0.930 | 0.817 | 0.888 |
| BI2 | 0.922 | 3.005 | 0.850 | ||||
| BI3 | 0.890 | 2.403 | 0.792 |
| Items | PU | PEOU | SI | FC | ATT | BI |
|---|---|---|---|---|---|---|
| PU | 0.899 | |||||
| PEOU | 0.664 | 0.915 | ||||
| SI | 0.758 | 0.583 | 0.893 | |||
| FC | 0.663 | 0.784 | 0.617 | 0.888 | ||
| ATT | 0.768 | 0.701 | 0.644 | 0.704 | 0.893 | |
| BI | 0.692 | 0.682 | 0.644 | 0.647 | 0.716 | 0.904 |
| Items | PU | PEOU | SI | FC | ATT | BI |
|---|---|---|---|---|---|---|
| PU1 | 0.896 | 0.574 | 0.711 | 0.610 | 0.705 | 0.647 |
| PU2 | 0.904 | 0.629 | 0.675 | 0.606 | 0.670 | 0.618 |
| PU3 | 0.896 | 0.588 | 0.657 | 0.572 | 0.693 | 0.601 |
| PEOU1 | 0.641 | 0.924 | 0.572 | 0.757 | 0.666 | 0.638 |
| PEOU2 | 0.592 | 0.934 | 0.519 | 0.713 | 0.629 | 0.650 |
| PEOU3 | 0.588 | 0.887 | 0.508 | 0.681 | 0.629 | 0.562 |
| SI1 | 0.689 | 0.518 | 0.892 | 0.562 | 0.608 | 0.543 |
| SI2 | 0.647 | 0.489 | 0.872 | 0.520 | 0.555 | 0.619 |
| SI3 | 0.695 | 0.554 | 0.916 | 0.571 | 0.609 | 0.576 |
| FC1 | 0.621 | 0.724 | 0.533 | 0.890 | 0.667 | 0.629 |
| FC2 | 0.561 | 0.656 | 0.537 | 0.899 | 0.618 | 0.528 |
| FC3 | 0.582 | 0.706 | 0.576 | 0.874 | 0.586 | 0.562 |
| ATT1 | 0.717 | 0.628 | 0.621 | 0.620 | 0.894 | 0.666 |
| ATT2 | 0.654 | 0.604 | 0.585 | 0.650 | 0.893 | 0.624 |
| ATT3 | 0.684 | 0.646 | 0.566 | 0.617 | 0.891 | 0.627 |
| BI1 | 0.644 | 0.659 | 0.627 | 0.621 | 0.655 | 0.899 |
| BI2 | 0.642 | 0.612 | 0.588 | 0.586 | 0.657 | 0.922 |
| BI3 | 0.589 | 0.577 | 0.529 | 0.547 | 0.629 | 0.890 |
| Hypothesis | Path | β | t-Value | Comments |
|---|---|---|---|---|
| H1 | PU ➝ ATT | 0.425 | 4.296 *** | Supported |
| H2 | PEOU ➝ ATT | 0.204 | 2.136 * | Supported |
| H3 | SI ➝ ATT | 0.095 | 1.285 | Not supported |
| H4 | FC ➝ ATT | 0.204 | 2.276 * | Supported |
| H5 | ATT ➝ BI | 0.716 | 18.047 *** | Supported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zin, K.S.L.T.; Kim, S.; Kim, H.-S.; Feyissa, I.F. A Study on Technology Acceptance of Digital Healthcare among Older Korean Adults Using Extended Tam (Extended Technology Acceptance Model). Adm. Sci. 2023, 13, 42. https://doi.org/10.3390/admsci13020042
Zin KSLT, Kim S, Kim H-S, Feyissa IF. A Study on Technology Acceptance of Digital Healthcare among Older Korean Adults Using Extended Tam (Extended Technology Acceptance Model). Administrative Sciences. 2023; 13(2):42. https://doi.org/10.3390/admsci13020042
Chicago/Turabian StyleZin, Khin Shoon Lei Thant, Seieun Kim, Hak-Seon Kim, and Israel Fisseha Feyissa. 2023. "A Study on Technology Acceptance of Digital Healthcare among Older Korean Adults Using Extended Tam (Extended Technology Acceptance Model)" Administrative Sciences 13, no. 2: 42. https://doi.org/10.3390/admsci13020042
APA StyleZin, K. S. L. T., Kim, S., Kim, H. -S., & Feyissa, I. F. (2023). A Study on Technology Acceptance of Digital Healthcare among Older Korean Adults Using Extended Tam (Extended Technology Acceptance Model). Administrative Sciences, 13(2), 42. https://doi.org/10.3390/admsci13020042