Evaluation of a Balloon-Type Vaginal Endoscope Based on Three-Dimensional Printing Technology for Self-Assessment of Pelvic Organ Prolapse




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Insertion of Endoscope
2.2. Recognition of Location And Symptoms
2.2.1. Location of Symptom
2.2.2. Conditions of Symptoms
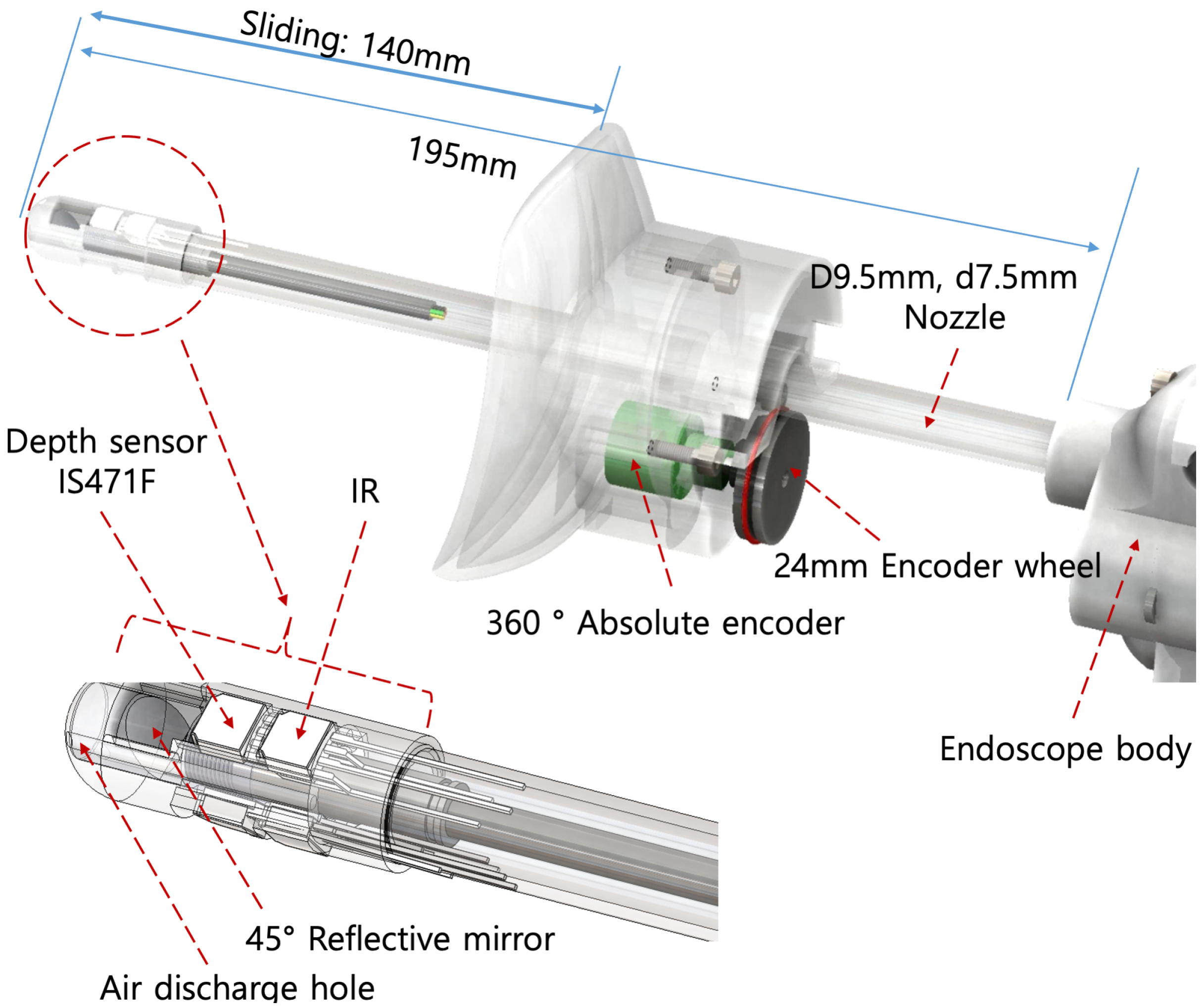
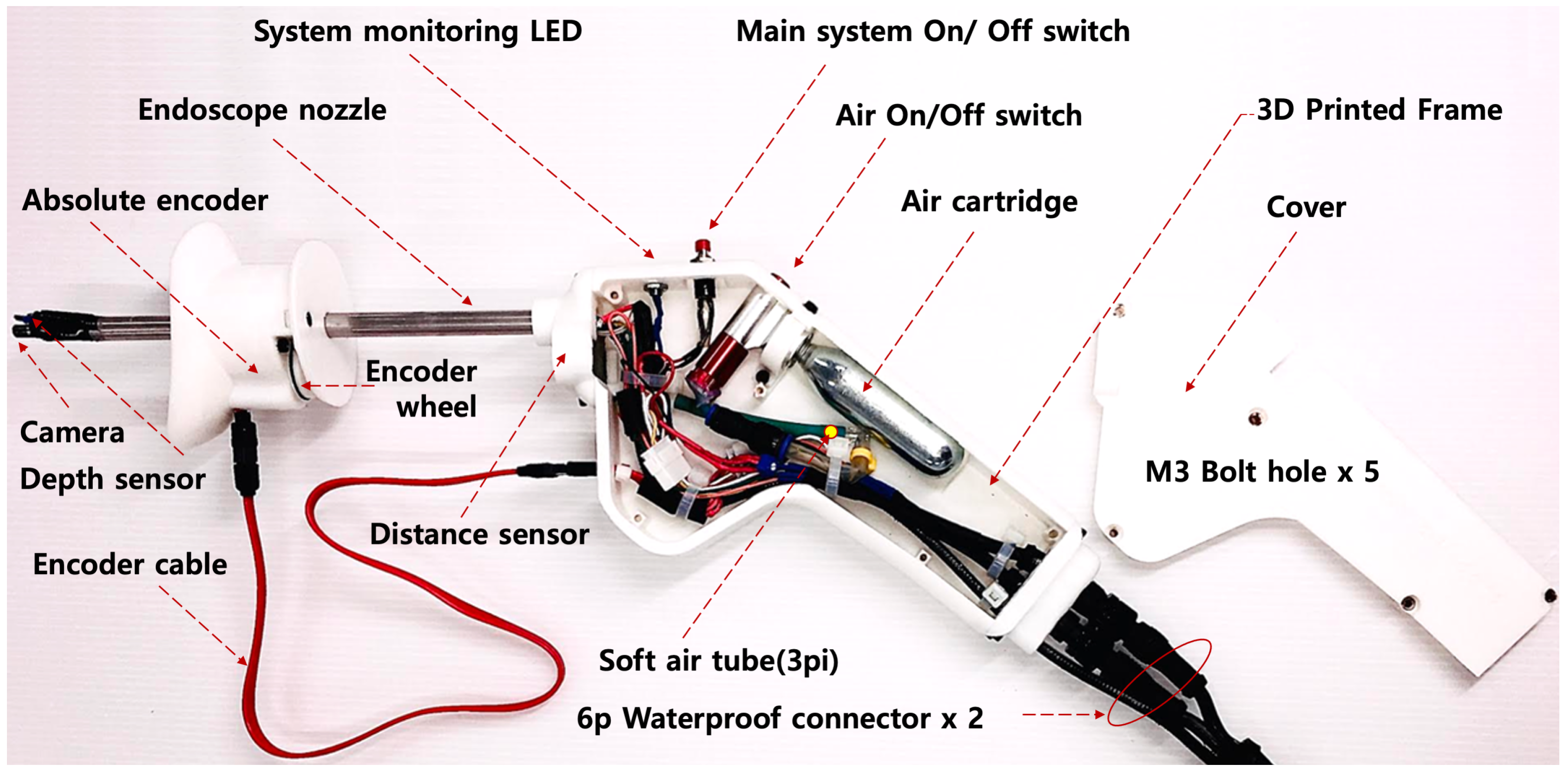
3. Design of Experimental System
3.1. System Architecture Outside the Endoscope
3.2. Electrical Schematic of the Inner Parts of the Endoscope
3.3. Regulation of the Airflow
4. Results
4.1. Results of Design for Testbed
4.2. Measurement Outcomes for Arbitrary Prolapse through the Testbed
5. Discussion
5.1. Standardization of Description of Pelvic Organ Prolapse and Specification of System
5.2. Ultrasound Assessment of Pelvic Organ Prolapse
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dietz, H.P. Pelvic organ prolapse—A review. Aust. Fam. Physician 2015, 44, 446. [Google Scholar]
- U.S. Census Bureau. U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Available online: https://www2.census.gov/programs-surveys/popproj/technical-documentation/methodology/idbsummeth.pdf (accessed on 5 June 2020).
- Luber, K.M.; Boero, S.; Choe, J.Y. The demographics of pelvic floor disorders: Current observations and future projections. Am. J. Obstet. Gynecol. 2001, 184, 1496–1503. [Google Scholar] [CrossRef] [PubMed]
- Subak, L.L.; Waetjen, L.E.; van den Eeden, S.; Thom, D.H.; Vittinghoff, E.; Brown, J.S. Cost of pelvic organ prolapse surgery in the United States. Obstet. Gynecol. 2001, 98, 646–651. [Google Scholar] [PubMed]
- Glazener, C.; MacArthur, C.; Bain, C.; Dean, N.; Toozs-Hobson, P.; Richardson, K.; Lancashire, R.; Herbison, P.; Hagen, S.; Grant, A.; et al. Epidemiology of pelvic organ prolapse in relation to delivery mode history at 12 years after childbirth: A longitudinal cohort study. Neurourol. Urodyn. 2010, 29, 819–820. [Google Scholar]
- Patel, D.; Xu, X.; Thomason, A.D.; Ransom, S.B.; Ivy, J.S.; DeLancey, J.O. Childbirth and pelvic floor dysfunction: An epidemiologic approach to the assessment of prevention opportunities at delivery. Am. J. Obstet. Gynecol. 2006, 195, 23–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, N.; Kamisan Atan, I.; Dietz, H. Obesity: How much does it matter for female pelvic organ prolapse? In RCOG World Congress; RCOG: Brisbane, Australia, 2015. [Google Scholar]
- Abdool, Z.; Dietz, H. A comparison of functional pelvic floor anatomy in white and black South African women with symptomatic pelvic organ prolapse. Neurourol. Urodyn. 2014, 33, 910–911. [Google Scholar]
- Laborda, E.; Gelman, W.; Anthony, F.; Monga, A. Is increased collagen metabolism the cause or effect of prolapse: A controlled study. Neurourol. Urodynam. 2003, 22, 505–506. [Google Scholar]
- Phillips, C.H.; Anthony, F.; Benyon, C.; Monga, A.K. Collagen metabolism in the uterosacral ligaments and vainal skin of women with uterine prolapse. BJOG 2006, 113, 39–46. [Google Scholar] [CrossRef]
- Ellerkmann, R.M.; Cundiff, G.W.; Melick, C.F.; Nihira, M.A.; Leffler, K.; Bent, A.E. Correlation of symptoms with location and severity of pelvic organ prolapse. Am. J. Obstet. Gynecol. 2001, 185, 1332–1338. [Google Scholar] [CrossRef]
- Heit, M.; Culligan, P.; Rosenquist, C.; Shott, S. Is pelvic organ prolapse a cause of pelvic or low back pain? Obstet. Gynecol. 2002, 99, 23–28. [Google Scholar]
- Handa, V.L.; Harvey, L.; Cundiff, G.W.; Siddique, S.A.; Kjerulff, K.H. Sexual function among women with urinary incontinence and pelvic organ prolapse. Am. J. Obstet. Gynecol. 2004, 191, 751–756. [Google Scholar] [CrossRef]
- Ulrich, D.; Guzman Rojas, R.; Dietz, H.P.; Mann, K.; Trutnovsky, G. Use of a visual analog scale for evaluation of bother from pelvic organ prolapse. Ultrasound Obstet. Gynecol. 2014, 43, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Barber, M.D. Symptoms and outcome measures of pelvic organ prolapse. Clin. Obstet. Gynecol. 2005, 48, 648–661. [Google Scholar] [CrossRef] [PubMed]
- Dietz, H.P.; Haylen, B.T.; Vancaillie, T.G. Female pelvic organ prolapse and voiding function. Int. Urogynecol. J. 2002, 13, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Bump, R.C.; Mattiasson, A.; Bo, K.; Brubaker, L.P.; DeLancey, J.O.; Klarskov, P.; Shull, B.L.; Smith, A.R. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am. J. Obstet. Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef]
- Weber, A.M.; Richter, H.E. Pelvic Organ Prolapse. Obstet. Gynecol. 2005, 106, 615–634. [Google Scholar] [CrossRef] [Green Version]
- Persu, C.; Chapple, C.R.; Cauni, V.; Gutue, S.; Geavlete, P. Pelvic Organ Prolapse Quantification System (POP-Q)—A new era in pelvic prolapse staging. J. Med. Life 2011, 4, 75–81. [Google Scholar]
- Diez, H.P.; Shek, K.L. Levator defects can be diagnosed by 2D translabial ultrasound. Int. Urogynecol. J. 2009, 20, 807–811. [Google Scholar]
- Paraiso, M.F.; Walters, M.D.; Rackley, R.R.; Melek, S.; Hugney, C. Laparoscopic and abdominal sacral colpopexies: A comparative cohort study. Am. J. Obstet. Gynecol. 2005, 192, 1752–1758. [Google Scholar] [CrossRef]
- Visco, A.G.; Weidner, A.C.; Barber, M.D.; Myers, E.R.; Cundiff, G.W.; Bump, R.C.; Addison, W.A. Vaginal mesh erosion after abdominal sacral colpopexy. Am. J. Obstet. Gynecol. 2001, 184, 297–302. [Google Scholar] [CrossRef]
- Olsen, A.L.; Smith, V.J.; Bergestrom, J.O.; Colling, J.C.; Clark, A.L. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet. Gynecol. 1997, 89, 501–506. [Google Scholar] [CrossRef]
- Bent, A.E.; Cundiff, G.W.; Swift, S.E. Ostergard’s urogynecology and pelvic floor dysfunction. In Chapter 26 Surgical Management of Pelvic Organ Prolapse; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Thakar, R.; Stanton, S. Management of genital prolapse. BMJ 2004, 324, 1258–1262. [Google Scholar] [CrossRef] [PubMed]
- Harvey, M.A. Pelvic floor exercises during and after pregnancy: A systematic review of their role in preventing pelvic floor dysfunction. J. Obstet. Gynaecol. Can. 2003, 25, 487–498. [Google Scholar] [CrossRef]
- Cundiff, G.W.; Weidner, A.; Visco, A.G.; Bump, R.C.; Addison, W.A. A survey of pessary use by the membership of the American Urogynecology Society. Obstet. Gynecol. 2000, 95, 931–935. [Google Scholar] [PubMed]
- Pott-Grinstein, E.; Newcomer, J.R. Gynecologists’ patterns of prescribing pessaries. J. Reprod. Med. 2001, 46, 205–208. [Google Scholar] [PubMed]
- Clemons, J.L.; Aguilar, V.C.; Tillinghast, T.A.; Jackson, N.D.; Myers, D.L. Risk factors associated with an unsuccessful pessary fitting trial in women with pelvic organ prolapse. Am. J. Obstet. Gynecol. 2004, 190, 345–350. [Google Scholar] [CrossRef]
- Clemons, J.L.; Aguilar, V.C.; Tillinghast, T.A.; Jackson, N.D.; Myers, D.L. Patient satisfaction and changes in prolapse and urinary symptoms in women who were fitted successfully with a pessary for pelvic organ prolapse. Am. J. Obstet. Gynecol. 2004, 190, 1025–1029. [Google Scholar] [CrossRef]
- Dietz, H.P.; Lekskulchai, O. Ultrasound assessment of pelvic organ prolapse: The relationship between prolapse severity and symptoms. Ultrasound Obstet. Gynecol. 2007, 29, 688–691. [Google Scholar] [CrossRef]
- Kobashi, K.C.; Leach, G.E. Pelvic prolapse. J. Urol. 2000, 164, 1879–1890. [Google Scholar] [CrossRef]










© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jun, M.; Jeong, H.; Endo, M.; Kodama, M.; Ohno, Y. Evaluation of a Balloon-Type Vaginal Endoscope Based on Three-Dimensional Printing Technology for Self-Assessment of Pelvic Organ Prolapse. Appl. Sci. 2020, 10, 5108. https://doi.org/10.3390/app10155108
Jun M, Jeong H, Endo M, Kodama M, Ohno Y. Evaluation of a Balloon-Type Vaginal Endoscope Based on Three-Dimensional Printing Technology for Self-Assessment of Pelvic Organ Prolapse. Applied Sciences. 2020; 10(15):5108. https://doi.org/10.3390/app10155108
Chicago/Turabian StyleJun, Myoungjae, Hieyong Jeong, Masayuki Endo, Michiko Kodama, and Yuko Ohno. 2020. "Evaluation of a Balloon-Type Vaginal Endoscope Based on Three-Dimensional Printing Technology for Self-Assessment of Pelvic Organ Prolapse" Applied Sciences 10, no. 15: 5108. https://doi.org/10.3390/app10155108
APA StyleJun, M., Jeong, H., Endo, M., Kodama, M., & Ohno, Y. (2020). Evaluation of a Balloon-Type Vaginal Endoscope Based on Three-Dimensional Printing Technology for Self-Assessment of Pelvic Organ Prolapse. Applied Sciences, 10(15), 5108. https://doi.org/10.3390/app10155108