Contact Lenses as Drug Delivery System for Glaucoma: A Review


 , , ,
, , , 
Abstract
:1. Introduction
1.1. Physiology and Pathophysiology of Glaucoma
1.2. Primary Open-Angle Glaucoma
1.3. Primary Angle-Closure Glaucoma
1.4. Diagnosis
1.5. Pharmacological Treatment
2. Drug Delivery Systems with Contact Lenses
2.1. Soaking
2.2. Functional Monomers
2.3. Molecular Imprinting
2.4. Colloidal Nanoparticles
2.5. Drug-Polymer Film Embedded
2.6. Supercritical Fluid
3. Contact Lens Drug Delivery in Glaucoma
3.1. Soaking
3.2. Functional Monomers
3.3. Molecular Imprinting
3.4. Colloidal Nanoparticles
3.5. Drug-Polymer Film Embedded
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cherecheanu, A.P.; Garhofer, G.; Schmidl, D.; Werkmeister, R.; Schmetterer, L. Ocular perfusion pressure and ocular blood flow in glaucoma. Curr. Opin. Pharmacol. 2013, 13, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinreb, R.N.; Khaw, P.T. Primary open-angle glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef]
- Coleman, A.L.; Miglior, S. Risk factors for glaucoma onset and progression. Surv. Ophthalmol. 2008, 53 (Suppl. 1), S3–S10. [Google Scholar] [CrossRef] [PubMed]
- Nickells, R.W.; Howell, G.R.; Soto, I.; John, S.W. Under pressure: Cellular and molecular responses during glaucoma, a common neurodegeneration with axonopathy. Annu. Rev. Neurosci. 2012, 35, 153–179. [Google Scholar] [CrossRef] [Green Version]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K., 2nd; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: A randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch. Ophthalmol. 2002, 120, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Heijl, A.; Leske, M.C.; Bengtsson, B.; Hyman, L.; Bengtsson, B.; Hussein, M. Reduction of intraocular pressure and glaucoma progression: Results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002, 120, 1268–1279. [Google Scholar] [CrossRef]
- Investigators, A. The Advanced Glaucoma Intervention Study (AGIS): 9. Comparison of glaucoma outcomes in black and white patients within treatment groups. Am. J. Ophthalmol. 2001, 132, 311–320. [Google Scholar] [CrossRef]
- Vass, C.; Hirn, C.; Sycha, T.; Findl, O.; Bauer, P.; Schmetterer, L. Medical interventions for primary open angle glaucoma and ocular hypertension. Cochrane Database Syst. Rev. 2007, 2007. [Google Scholar] [CrossRef]
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Leite, M.T.; Sakata, L.M.; Medeiros, F.A. Managing glaucoma in developing countries. Arq. Bras. Oftalmol. 2011, 74, 83–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotchford, A.P.; Kirwan, J.F.; Muller, M.A.; Johnson, G.J.; Roux, P. Temba glaucoma study: A population-based cross-sectional survey in urban South Africa. Ophthalmology 2003, 110, 376–382. [Google Scholar] [CrossRef]
- Chowdhury, U.R.; Madden, B.J.; Charlesworth, M.C.; Fautsch, M.P. Proteome analysis of human aqueous humor. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4921–4931. [Google Scholar] [CrossRef]
- Niesel, P. Pathophysiology of hydrodynamics in glaucoma. Fortschr. Ophthalmol. 1988, 85, 33–37. [Google Scholar]
- Goel, M.; Picciani, R.G.; Lee, R.K.; Bhattacharya, S.K. Aqueous humor dynamics: A review. Open Ophthalmol. J. 2010, 4, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heys, J.J.; Barocas, V.H. A boussinesq model of natural convection in the human eye and the formation of Krukenberg’s spindle. Ann. Biomed. Eng. 2002, 30, 392–401. [Google Scholar] [CrossRef]
- Tamm, E.R. The trabecular meshwork outflow pathways: Structural and functional aspects. Exp. Eye Res. 2009, 88, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Alm, A.; Nilsson, S.F. Uveoscleral outflow—A review. Exp. Eye Res. 2009, 88, 760–768. [Google Scholar] [CrossRef]
- Yucel, Y.H.; Johnston, M.G.; Ly, T.; Patel, M.; Drake, B.; Gumus, E.; Fraenkl, S.A.; Moore, S.; Tobbia, D.; Armstrong, D.; et al. Identification of lymphatics in the ciliary body of the human eye: A novel “uveolymphatic” outflow pathway. Exp. Eye Res. 2009, 89, 810–819. [Google Scholar] [CrossRef]
- Sigal, I.A.; Ethier, C.R. Biomechanics of the optic nerve head. Exp. Eye Res. 2009, 88, 799–807. [Google Scholar] [CrossRef]
- Alasil, T.; Wang, K.; Yu, F.; Field, M.G.; Lee, H.; Baniasadi, N.; de Boer, J.F.; Coleman, A.L.; Chen, T.C. Correlation of retinal nerve fiber layer thickness and visual fields in glaucoma: A broken stick model. Am. J. Ophthalmol. 2014, 157, 953–959. [Google Scholar] [CrossRef] [Green Version]
- Vitale, S.; Smith, T.D.; Quigley, T.; Kerrigan-Baumrind, T.A.; Pease, T.E.; Varma, R.; Friedman, T.S.; Katz, J.; Tielsch, J.M. Screening performance of functional and structural measurements of neural damage in open-angle glaucoma: A case-control study from the Baltimore Eye Survey. J. Glaucoma 2000, 9, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Varma, R.; Ying-Lai, M.; Francis, B.A.; Nguyen, B.B.; Deneen, J.; Wilson, M.R.; Azen, S.P.; Los Angeles Latino Eye Study Group. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: The Los Angeles Latino Eye Study. Ophthalmology 2004, 111, 1439–1448. [Google Scholar] [CrossRef] [PubMed]
- Tielsch, J.M.; Sommer, A.; Katz, J.; Royall, R.M.; Quigley, H.A.; Javitt, J. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA 1991, 266, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Wormald, R.P.; Basauri, E.; Wright, L.A.; Evans, J.R. The African Caribbean Eye Survey: Risk factors for glaucoma in a sample of African Caribbean people living in London. Eye 1994, 8 Pt 3, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Congdon, N.G.; Youlin, Q.; Quigley, H.; Hung, P.T.; Wang, T.H.; Ho, T.C.; Tielsch, J.M. Biometry and primary angle-closure glaucoma among Chinese, white, and black populations. Ophthalmology 1997, 104, 1489–1495. [Google Scholar] [CrossRef]
- Medeiros, F.A.; Alencar, L.M.; Zangwill, L.M.; Bowd, C.; Sample, P.A.; Weinreb, R.N. Prediction of functional loss in glaucoma from progressive optic disc damage. Arch. Ophthalmol. 2009, 127, 1250–1256. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, F.A.; Vizzeri, G.; Zangwill, L.M.; Alencar, L.M.; Sample, P.A.; Weinreb, R.N. Comparison of retinal nerve fiber layer and optic disc imaging for diagnosing glaucoma in patients suspected of having the disease. Ophthalmology 2008, 115, 1340–1346. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, F.A.; Zangwill, L.M.; Bowd, C.; Weinreb, R.N. Comparison of the GDx VCC scanning laser polarimeter, HRT II confocal scanning laser ophthalmoscope, and stratus OCT optical coherence tomograph for the detection of glaucoma. Arch. Ophthalmol. 2004, 122, 827–837. [Google Scholar] [CrossRef] [Green Version]
- Chauhan, B.C.; O’Leary, N.; AlMobarak, F.A.; Reis, A.S.C.; Yang, H.; Sharpe, G.P.; Hutchison, D.M.; Nicolela, M.T.; Burgoyne, C.F. Enhanced detection of open-angle glaucoma with an anatomically accurate optical coherence tomography-derived neuroretinal rim parameter. Ophthalmology 2013, 120, 535–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medeiros, F.A.; Zangwill, L.M.; Anderson, D.R.; Liebmann, J.M.; Girkin, C.A.; Harwerth, R.S.; Fredette, M.J.; Weinreb, R.N. Estimating the rate of retinal ganglion cell loss in glaucoma. Am. J. Ophthalmol. 2012, 154, 814–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higginbotham, E.J.; Diestelhorst, M.; Pfeiffer, N.; Rouland, J.F.; Alm, A. The efficacy and safety of unfixed and fixed combinations of latanoprost and other antiglaucoma medications. Surv. Ophthalmol. 2002, 47 (Suppl. 1), S133–S140. [Google Scholar] [CrossRef]
- Kaiserman, I.; Fendyur, A.; Vinker, S. Topical beta blockers in asthmatic patients-is it safe? Curr. Eye Res. 2009, 34, 517–522. [Google Scholar] [CrossRef]
- Alkozi, H.A.; Navarro, G.; Aguinaga, D.; Reyes-Resina, I.; Sanchez-Naves, J.; Perez de Lara, M.J.; Franco, R.; Pintor, J. Adreno-melatonin receptor complexes control ion homeostasis and intraocular pressure—Their disruption contributes to hypertensive glaucoma. Br. J. Pharmacol. 2020, 177, 2090–2105. [Google Scholar] [CrossRef]
- Martinez-Aguila, A.; Fonseca, B.; Perez de Lara, M.J.; Pintor, J. Effect of Melatonin and 5-Methoxycarbonylamino-N-Acetyltryptamine on the Intraocular Pressure of Normal and Glaucomatous Mice. J. Pharmacol. Exp. Ther. 2016, 357, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Alarma-Estrany, P.; Guzman-Aranguez, A.; Huete, F.; Peral, A.; Plourde, R., Jr.; Pelaez, T.; Yerxa, B.; Pintor, J. Design of novel melatonin analogs for the reduction of intraocular pressure in normotensive rabbits. J. Pharmacol. Exp. Ther. 2011, 337, 703–709. [Google Scholar] [CrossRef] [Green Version]
- Andres-Guerrero, V.; Molina-Martinez, I.T.; Peral, A.; de las Heras, B.; Pintor, J.; Herrero-Vanrell, R. The use of mucoadhesive polymers to enhance the hypotensive effect of a melatonin analogue, 5-MCA-NAT, in rabbit eyes. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1507–1515. [Google Scholar] [CrossRef] [Green Version]
- Rowland, J.M.; Potter, D.E.; Reiter, R.J. Circadian rhythm in intraocular pressure: A rabbit model. Curr. Eye Res. 1981, 1, 169–173. [Google Scholar] [CrossRef]
- Agorastos, A.; Huber, C.G. The role of melatonin in glaucoma: Implications concerning pathophysiological relevance and therapeutic potential. J. Pineal Res. 2011, 50, 1–7. [Google Scholar] [CrossRef]
- Alarma-Estrany, P.; Crooke, A.; Peral, A.; Pintor, J. Requirement of intact sympathetic transmission for the ocular hypotensive effects of melatonin and 5-MCA-NAT. Auton. Neurosci. 2007, 137, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Aguila, A.; Fonseca, B.; Bergua, A.; Pintor, J. Melatonin analogue agomelatine reduces rabbit’s intraocular pressure in normotensive and hypertensive conditions. Eur. J. Pharmacol. 2013, 701, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Pescosolido, N.; Gatto, V.; Stefanucci, A.; Rusciano, D. Oral treatment with the melatonin agonist agomelatine lowers the intraocular pressure of glaucoma patients. Ophthalmic Physiol. Opt. 2015, 35, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Mediero, A.; Alarma-Estrany, P.; Pintor, J. New treatments for ocular hypertension. Auton. Neurosci. 2009, 147, 14–19. [Google Scholar] [CrossRef]
- Pintor, J.; Peral, A.; Pelaez, T.; Martin, S.; Hoyle, C.H. Presence of diadenosine polyphosphates in the aqueous humor: Their effect on intraocular pressure. J. Pharmacol. Exp. Ther. 2003, 304, 342–348. [Google Scholar] [CrossRef]
- Fonseca, B.; Martinez-Aguila, A.; de Lara, M.J.P.; Pintor, J. Diadenosine tetraphosphate as a potential therapeutic nucleotide to treat glaucoma. Purinergic Signal. 2017, 13, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Baudouin, C.; Labbe, A.; Liang, H.; Pauly, A.; Brignole-Baudouin, F. Preservatives in eyedrops: The good, the bad and the ugly. Prog. Retin. Eye Res. 2010, 29, 312–334. [Google Scholar] [CrossRef]
- Knight, O.J.; Lawrence, S.D. Sustained drug delivery in glaucoma. Curr. Opin. Ophthalmol. 2014, 25, 112–117. [Google Scholar] [CrossRef]
- Peng, C.C.; Burke, M.T.; Carbia, B.E.; Plummer, C.; Chauhan, A. Extended drug delivery by contact lenses for glaucoma therapy. J. Control. Release 2012, 162, 152–158. [Google Scholar] [CrossRef]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular drug delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef]
- Hughes, P.M.; Olejnik, O.; Chang-Lin, J.E.; Wilson, C.G. Topical and systemic drug delivery to the posterior segments. Adv. Drug Deliv. Rev. 2005, 57, 2010–2032. [Google Scholar] [CrossRef] [PubMed]
- Velpandian, T. Intraocular penetration of antimicrobial agents in ophthalmic infections and drug delivery strategies. Expert Opin. Drug Deliv. 2009, 6, 255–270. [Google Scholar] [CrossRef]
- Kompella, U.B.; Kadam, R.S.; Lee, V.H. Recent advances in ophthalmic drug delivery. Ther. Deliv. 2010, 1, 435–456. [Google Scholar] [CrossRef] [Green Version]
- Kosoko, O.; Quigley, H.A.; Vitale, S.; Enger, C.; Kerrigan, L.; Tielsch, J.M. Risk factors for noncompliance with glaucoma follow-up visits in a residents’ eye clinic. Ophthalmology 1998, 105, 2105–2111. [Google Scholar] [CrossRef]
- Okeke, C.O.; Quigley, H.A.; Jampel, H.D.; Ying, G.S.; Plyler, R.J.; Jiang, Y.; Friedman, D.S. Adherence with topical glaucoma medication monitored electronically the Travatan Dosing Aid study. Ophthalmology 2009, 116, 191–199. [Google Scholar] [CrossRef]
- Hollo, G.; Topouzis, F.; Fechtner, R.D. Fixed-combination intraocular pressure-lowering therapy for glaucoma and ocular hypertension: Advantages in clinical practice. Expert Opin. Pharmacother. 2014, 15, 1737–1747. [Google Scholar] [CrossRef] [PubMed]
- Skalicky, S.E.; Goldberg, I.; McCluskey, P. Ocular surface disease and quality of life in patients with glaucoma. Am. J. Ophthalmol. 2012, 153, 1–9. [Google Scholar] [CrossRef]
- Guzman-Aranguez, A.; Fonseca, B.; Carracedo, G.; Martin-Gil, A.; Martinez-Aguila, A.; Pintor, J. Dry Eye Treatment Based on Contact Lens Drug Delivery: A Review. Eye Contact Lens 2016, 42, 280–288. [Google Scholar] [CrossRef]
- Singh, R.B.; Ichhpujani, P.; Thakur, S.; Jindal, S. Promising therapeutic drug delivery systems for glaucoma: A comprehensive review. Ther. Adv. Ophthalmol. 2020, 12, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Ciolino, J.B.; Stefanescu, C.F.; Ross, A.E.; Salvador-Culla, B.; Cortez, P.; Ford, E.M.; Wymbs, K.A.; Sprague, S.L.; Mascoop, D.R.; Rudina, S.S.; et al. In vivo performance of a drug-eluting contact lens to treat glaucoma for a month. Biomaterials 2014, 35, 432–439. [Google Scholar] [CrossRef] [Green Version]
- Berdy, G.J.; Abelson, M.B.; Smith, L.M.; George, M.A. Preservative-free artificial tear preparations. Assessment of corneal epithelial toxic effects. Arch. Ophthalmol. 1992, 110, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Gasset, A.R.; Ishii, Y.; Kaufman, H.E.; Miller, T. Cytotoxicity of ophthalmic preservatives. Am. J. Ophthalmol. 1974, 78, 98–105. [Google Scholar] [CrossRef]
- Musgrave, C.S.A.; Fang, F. Contact Lens Materials: A Materials Science Perspective. Materials 2019, 12, 261. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Xue, Y.; Hu, G.; Lin, T.; Gou, J.; Yin, T.; He, H.; Zhang, Y.; Tang, X. A comprehensive review on contact lens for ophthalmic drug delivery. J. Control. Release 2018, 281, 97–118. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.B.; Efron, N.; Woods, C.A.; International Contact Lens Prescribing Survey Consortium. Determinants of the frequency of contact lens wear. Eye Contact Lens 2013, 39, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Efron, N.; Morgan, P.B.; Woods, C.A.; International Contact Lens Prescribing Survey Consortium. International survey of rigid contact lens fitting. Optom. Vis. Sci. 2013, 90, 113–118. [Google Scholar] [CrossRef]
- Kim, E.; Saha, M.; Ehrmann, K. Mechanical Properties of Contact Lens Materials. Eye Contact Lens 2018, 44 (Suppl. 2), S148–S156. [Google Scholar] [CrossRef]
- Sedlácek, J. Possibility of the application of ophthalmic drugs with the use of gel contact lenses. Ceskoslovenska Oftalmol. 1965, 21, 509–512. [Google Scholar]
- North, D.P. Treatment of acute glaucoma. Can. Med. Assoc. J. 1971, 105, 561. [Google Scholar]
- Podos, S.M.; Becker, B.; Asseff, C.; Hartstein, J. Pilocarpine therapy with soft contact lenses. Am. J. Ophthalmol. 1972, 73, 336–341. [Google Scholar] [CrossRef]
- Hillman, J.S. Management of acute glaucoma with pilocarpine-soaked hydrophilic lens. Br. J. Ophthalmol. 1974, 58, 674–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruben, M.; Watkins, R. Pilocarpine dispensation for the soft hydrophilic contact lens. Br. J. Ophthalmol. 1975, 59, 455–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNamara, N.A.; Polse, K.A.; Bonanno, J.A. Fluorophotometry in contact lens research: The next step. Optom. Vis. Sci. 1998, 75, 316–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pahuja, P.; Arora, S.; Pawar, P. Ocular drug delivery system: A reference to natural polymers. Expert Opin. Drug Deliv. 2012, 9, 837–861. [Google Scholar] [CrossRef]
- Jones, L.; Brennan, N.A.; Gonzalez-Meijome, J.; Lally, J.; Maldonado-Codina, C.; Schmidt, T.A.; Subbaraman, L.; Young, G.; Nichols, J.J.; members of the TFOS International Workshop on Contact Lens Discomfort. The TFOS International Workshop on Contact Lens Discomfort: Report of the contact lens materials, design, and care subcommittee. Investig. Ophthalmol. Vis. Sci. 2013, 54. [Google Scholar] [CrossRef]
- ElShaer, A.; Mustafa, S.; Kasar, M.; Thapa, S.; Ghatora, B.; Alany, R.G. Nanoparticle-Laden Contact Lens for Controlled Ocular Delivery of Prednisolone: Formulation Optimization Using Statistical Experimental Design. Pharmaceutics 2016, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Pucker, A.D.; Jones-Jordan, L.A.; Marx, S.; Powell, D.R.; Kwan, J.T.; Srinivasan, S.; Sickenberger, W.; Jones, L.; Contact Lens Assessment of Symptomatic Subjects (CLASS) Study Group. Clinical factors associated with contact lens dropout. Cont. Lens Anterior Eye 2019, 42, 318–324. [Google Scholar] [CrossRef]
- Zaki, M.; Pardo, J.; Carracedo, G. A review of international medical device regulations: Contact lenses and lens care solutions. Cont. Lens Anterior Eye 2019, 42, 136–146. [Google Scholar] [CrossRef]
- Efron, N.; Jones, L.; Bron, A.J.; Knop, E.; Arita, R.; Barabino, S.; McDermott, A.M.; Villani, E.; Willcox, M.D.; Markoulli, M.; et al. The TFOS International Workshop on Contact Lens Discomfort: Report of the contact lens interactions with the ocular surface and adnexa subcommittee. Investig. Ophthalmol. Vis. Sci. 2013, 54, TFOS98–TFOS122. [Google Scholar] [CrossRef]
- Alipour, F.; Khaheshi, S.; Soleimanzadeh, M.; Heidarzadeh, S.; Heydarzadeh, S. Contact Lens-related Complications: A Review. J. Ophthalmic Vis. Res. 2017, 12, 193–204. [Google Scholar] [CrossRef]
- Kuc, C.J.; Lebow, K.A. Contact Lens Solutions and Contact Lens Discomfort: Examining the Correlations Between Solution Components, Keratitis, and Contact Lens Discomfort. Eye Contact Lens 2018, 44, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, C.A.; Kaufman, P.L.; Kiland, J.A. Benzalkonium chloride and glaucoma. J. Ocul. Pharmacol. Ther. 2014, 30, 163–169. [Google Scholar] [CrossRef]
- Dominguez-Godinez, C.; Carracedo, G.; Pintor, J. Diquafosol delivery from silicone hydrogel contact lenses: Improved effect on tear secretion. J. Ocul. Pharmacol. Ther. 2018, 34, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Godínez, C.; Martín Gil, A.; Carracedo Rodríguez, G.; Guzmán Aránguez, A.I.; González-Méijome, J.M.; Pintor, J. In vitro and in vivo delivery of the secretagogue diadenosine tetraphosphate from conventional and silicone hydrogel soft contact lenses. J. Optom. 2013, 6, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, M.G.; Morrison, P.W.J.; Boostrom, H.M.; Morgan, S.R.; Fallon, M.; Lewis, P.N.; Whitaker, D.; Brancale, A.; Varricchio, C.; Quantock, A.J.; et al. In Vitro Topical Delivery of Chlorhexidine to the Cornea: Enhancement Using Drug-Loaded Contact Lenses and β-Cyclodextrin Complexation, and the Importance of Simulating Tear Irrigation. Mol. Pharmaceut. 2020, 17, 1428–1441. [Google Scholar] [CrossRef] [PubMed]
- Minami, T.; Ishida, W.; Kishimoto, T.; Nakajima, I.; Hino, S.; Arai, R.; Matsunaga, T.; Fukushima, A.; Yamagami, S. In vitro and in vivo performance of epinastine hydrochloride-releasing contact lenses. PLoS ONE 2019, 14, e0210362. [Google Scholar] [CrossRef]
- Schultz, C.; Breaux, J.; Schentag, J.; Morck, D. Drug delivery to the posterior segment of the eye through hydrogel contact lenses. Clin. Exp. Optom. 2011, 94, 212–218. [Google Scholar] [CrossRef]
- Sekar, P.; Chauhan, A. Effect of vitamin-E integration on delivery of prostaglandin analogs from therapeutic lenses. J. Colloid Interface Sci. 2019, 539, 457–467. [Google Scholar] [CrossRef]
- Xu, J.; Li, X.; Sun, F. In vitro and in vivo evaluation of ketotifen fumarate-loaded silicone hydrogel contact lenses for ocular drug delivery. Drug Deliv. 2011, 18, 150–158. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Yang, Y.; Lei, M.; Ye, C.; Zhao, C.; Xu, J.; Wu, K.; Yu, M. Experimental studies on soft contact lenses for controlled ocular delivery of pirfinedone: In vitro and in vivo. Drug Deliv. 2016, 23, 3538–3543. [Google Scholar] [CrossRef] [Green Version]
- Hsu, K.H.; Carbia, B.E.; Plummer, C.; Chauhan, A. Dual drug delivery from vitamin e loaded contact lenses for glaucoma therapy. Eur. J. Pharmaceut. Biopharm. 2015, 94, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Andrade-Vivero, P.; Fernandez-Gabriel, E.; Alvarez-Lorenzo, C.; Concheiro, A. Improving the loading and release of NSAIDs from pHEMA hydrogels by copolymerization with functionalized monomers. J. Pharmaceut. Sci. 2007, 96, 802–813. [Google Scholar] [CrossRef] [PubMed]
- Uchida, R.; Sato, T.; Tanigawa, H.; Uno, K. Azulene incorporation and release by hydrogel containing methacrylamide propyltrimenthylammonium chloride, and its application to soft contact lens. J. Control. Release 2003, 92, 259–264. [Google Scholar] [CrossRef]
- Sato, T.; Uchida, R.; Tanigawa, H.; Uno, K.; Murakami, A. Application of polymer gels containing side-chain phosphate groups to drug-delivery contact lenses. J. Appl. Polym. Sci. 2005, 98, 731–735. [Google Scholar] [CrossRef]
- Kakisu, K.; Matsunaga, T.; Kobayakawa, S.; Sato, T.; Tochikubo, T. Development and efficacy of a drug-releasing soft contact lens. Investig. Ophthalmol. Vis. Sci. 2013, 54, 2551–2561. [Google Scholar] [CrossRef] [Green Version]
- Brahim, S.; Narinesingh, D.; Guiseppi-Elie, A. Release characteristics of novel pH-sensitive p(HEMA-DMAEMA) hydrogels containing 3-(trimethoxy-silyl) propyl methacrylate. Biomacromolecules 2003, 4, 1224–1231. [Google Scholar] [CrossRef]
- Glisoni, R.J.; García-Fernández, M.J.; Pino, M.; Gutkind, G.; Moglioni, A.G.; Alvarez-Lorenzo, C.; Concheiro, A.; Sosnik, A. β-Cyclodextrin hydrogels for the ocular release of antibacterial thiosemicarbazones. Carbohydr. Polym. 2013, 93, 449–457. [Google Scholar] [CrossRef]
- Kaczmarek, J.C.; Tieppo, A.; White, C.J.; Byrne, M.E. Adjusting biomaterial composition to achieve controlled multiple-day release of dexamethasone from an extended-wear silicone hydrogel contact lens. J. Biomater. Sci. Polym. Ed. 2014, 25, 88–100. [Google Scholar] [CrossRef]
- García-Millán, E.; Koprivnik, S.; Otero-Espinar, F.J. Drug loading optimization and extended drug delivery of corticoids from pHEMA based soft contact lenses hydrogels via chemical and microstructural modifications. Int. J. Pharmaceut. 2015, 487, 260–269. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Soni, T.G.; Shah, D.O. A review on therapeutic contact lenses for ocular drug delivery. Drug Deliv. 2016, 23, 3017–3026. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Desai, A.R.; Choksi, H.H.; Patil, R.J.; Ranch, K.M.; Vyas, B.A.; Shah, D.O. Effect of surfactant chain length on drug release kinetics from microemulsion-laden contact lenses. Int. J. Pharm. 2017, 524, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Aouak, T.; Saeed, W.S.; Al-Hafi, N.M.; Al-Odayni, A.B.; Alghamdi, A.A.; Bedja, I. Poly (2-hydroxyethylmethacrylate -co-methylmethacrylate)/Lignocaine Contact Lens Preparation, Characterization, and in vitro Release Dynamic. Polymers 2019, 11, 917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Q.; Mao, S. Enhanced drug loading efficiency of contact lenses via salt-induced modulation Qiang. Asian J. Pharm. Sci. 2019, 14, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, X.; Sun, F. Cyclodextrin-containing hydrogels for contact lenses as a platform for drug incorporation and release. Acta Biomater. 2010, 6, 486–493. [Google Scholar] [CrossRef]
- Hu, X.; Gong, X. A new route to fabricate biocompatible hydrogels with controlled drug delivery behavior. J. Colloid Interface Sci. 2016, 470, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Phan, C.M.; Subbaraman, L.N.; Jones, L. In vitro drug release of natamycin from beta-cyclodextrin and 2-hydroxypropyl-beta-cyclodextrin-functionalized contact lens materials. J. Biomater. Sci. Polym. Ed. 2014, 25, 1907–1919. [Google Scholar] [CrossRef]
- Li, R.; Guan, X.; Lin, X.; Guan, P.; Zhang, X.; Rao, Z.; Du, L.; Zhao, J.; Rong, J.; Zhao, J. Poly(2-hydroxyethyl methacrylate)/beta-cyclodextrin-hyaluronan contact lens with tear protein adsorption resistance and sustained drug delivery for ophthalmic diseases. Acta Biomater. 2020, 110, 105–118. [Google Scholar] [CrossRef]
- White, C.J.; Byrne, M.E. Molecularly imprinted therapeutic contact lenses. Expert Opin. Drug Deliv. 2010, 7, 765–780. [Google Scholar] [CrossRef]
- Hiratani, H.; Mizutani, Y.; Alvarez-Lorenzo, C. Controlling drug release from imprinted hydrogels by modifying the characteristics of the imprinted cavities. Macromol. Biosci. 2005, 5, 728–733. [Google Scholar] [CrossRef]
- Alvarez-Lorenzo, C.; Concheiro, A. Molecularly imprinted polymers for drug delivery. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2004, 804, 231–245. [Google Scholar] [CrossRef]
- Hiratani, H.; Alvarez-Lorenzo, C. Timolol uptake and release by imprinted soft contact lenses made of N,N-diethylacrylamide and methacrylic acid. J. Controll. Release 2002, 83, 223–230. [Google Scholar] [CrossRef]
- Alvarez-Lorenzo, C.; Hiratani, H.; Gomez-Amoza, J.L.; Martinez-Pacheco, R.; Souto, C.; Concheiro, A. Soft contact lenses capable of sustained delivery of timolol. J. Pharm. Sci. 2002, 91, 2182–2192. [Google Scholar] [CrossRef] [PubMed]
- Malakooti, N.; Alexander, C.; Alvarez-Lorenzo, C. Imprinted Contact Lenses for Sustained Release of Polymyxin B and Related Antimicrobial Peptides. J. Pharm. Sci. 2015, 104, 3386–3394. [Google Scholar] [CrossRef] [PubMed]
- Tieppo, A.; White, C.J.; Paine, A.C.; Voyles, M.L.; McBride, M.K.; Byrne, M.E. Sustained in vivo release from imprinted therapeutic contact lenses. J. Control. Release 2012, 157, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Tieppo, A.; Pate, K.M.; Byrne, M.E. In vitro controlled release of an anti-inflammatory from daily disposable therapeutic contact lenses under physiological ocular tear flow. Eur. J. Pharm. Biopharm. 2012, 81, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Rivera, F.; Serro, A.P.; Silva, D.; Concheiro, A.; Alvarez-Lorenzo, C. Hydrogels for diabetic eyes: Naltrexone loading, release profiles and cornea penetration. Mater. Sci. Eng. C 2019, 105. [Google Scholar] [CrossRef]
- Gulsen, D.; Li, C.-C.; Chauhan, A. Dispersion of DMPC liposomes in contact lenses for ophthalmic drug delivery. Curr. Eye Res. 2005, 30, 1071–1080. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Parmar, R.J.; Desai, A.R.; Desai, D.M.; Shukla, M.R.; Ranch, K.M.; Shah, S.A.; Shah, D.O. Tailored gatifloxacin Pluronic(R) F-68-loaded contact lens: Addressing the issue of transmittance and swelling. Int. J. Pharm. 2020, 581, 119279. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Mangukiya, M.A.; Patel, P.A.; Vaidya, R.J.; Koli, A.R.; Ranch, K.M.; Shah, D.O. Extended release of ketotifen from silica shell nanoparticle-laden hydrogel contact lenses: In vitro and in vivo evaluation. J. Mater. Sci Mater. Med. 2016, 27, 113. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Choksi, H.H.; Desai, A.R.; Patel, A.S.; Ranch, K.M.; Vyas, B.A.; Shah, D.O. pH triggered controlled drug delivery from contact lenses: Addressing the challenges of drug leaching during sterilization and storage. Colloids Surf. B Biointerfaces 2017, 157, 72–82. [Google Scholar] [CrossRef]
- Xu, J.; Ge, Y.; Bu, R.; Zhang, A.; Feng, S.; Wang, J.; Gou, J.; Yin, T.; He, H.; Zhang, Y.; et al. Co-delivery of latanoprost and timolol from micelles-laden contact lenses for the treatment of glaucoma. J. Control. Release 2019, 305, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.F.; Zhong, J.; Chen, G.P.; Lin, Z.T.; Deng, Y.; Liu, Y.L.; Cao, P.Y.; Wang, B.; Wei, Y.; Wu, T.; et al. A Hydrogel-Based Hybrid Theranostic Contact Lens for Fungal Keratitis. ACS Nano 2016, 10, 6464–6473. [Google Scholar] [CrossRef] [PubMed]
- Carreira, A.S.; Ferreira, P.; Ribeiro, M.P.; Correia, T.R.; Coutinho, P.; Correia, I.J.; Gil, M.H. New drug-eluting lenses to be applied as bandages after keratoprosthesis implantation. Int. Pharm. 2014, 477, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Liu, C.; Sun, Z.; Zhang, X.; Liang, N.; Mao, S. Inner layer-embedded contact lenses for pH-triggered controlled ocular drug delivery. Eur. J. Pharm. Biopharm. 2018, 128, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Maulvi, F.A.; Singhania, S.S.; Desai, A.R.; Shukla, M.R.; Tannk, A.S.; Ranch, K.M.; Vyas, B.A.; Shah, D.O. Contact lenses with dual drug delivery for the treatment of bacterial conjunctivitis. Int. J. Pharm. 2018, 548, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Zhang, W.; Lei, Y.; Dang, M. Novel Polyvinyl Pyrrolidone–Loaded Olopatadine HCl–Laden Doughnut Contact Lens to Treat Allergic Conjunctivitis. J. Pharm. Sci. 2020, 109, 1714–1724. [Google Scholar] [CrossRef]
- Ross, A.E.; Bengani, L.C.; Tulsan, R.; Maidana, D.E.; Salvador-Culla, B.; Kobashi, H.; Kolovou, P.E.; Zhai, H.; Taghizadeh, K.; Kuang, L.; et al. Topical sustained drug delivery to the retina with a drug-eluting contact lens. Biomaterials 2019, 217. [Google Scholar] [CrossRef]
- Costa, V.P.; Braga, M.E.M.; Guerra, J.P.; Duarte, A.R.C.; Duarte, C.M.M.; Leite, E.O.B.; Gil, M.H.; de Sousa, H.C. Development of therapeutic contact lenses using a supercritical solvent impregnation method. J. Supercrit. Fluids 2010, 52, 306–316. [Google Scholar] [CrossRef]
- Yanez, F.; Martikainen, L.; Braga, M.E.; Alvarez-Lorenzo, C.; Concheiro, A.; Duarte, C.M.; Gil, M.H.; de Sousa, H.C. Supercritical fluid-assisted preparation of imprinted contact lenses for drug delivery. Acta Biomater. 2011, 7, 1019–1030. [Google Scholar] [CrossRef]
- Braga, M.E.M.; Costa, V.P.; Pereira, M.J.T.; Fiadeiro, P.T.; Gomes, A.P.A.R.; Duarte, C.M.M.; De Sousa, H.C. Effects of operational conditions on the supercritical solvent impregnation of acetazolamide in Balafilcon A commercial contact lenses. Int. J. Pharm. 2011, 420, 231–243. [Google Scholar] [CrossRef]
- Choi, J.H.; Li, Y.; Jin, R.; Shrestha, T.; Choi, J.S.; Lee, W.J.; Moon, M.J.; Ju, H.T.; Choi, W.; Yoon, K.C. The Efficiency of Cyclosporine A-Eluting Contact Lenses for the Treatment of Dry Eye. Curr. Eye Res. 2019, 44, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.C.; Spaeth, G.L. Compliance in patients prescribed eyedrops for glaucoma. Ophthalmic Surg. 1995, 26, 233–236. [Google Scholar] [PubMed]
- Stone, J.L.; Robin, A.L.; Novack, G.D.; Covert, D.W.; Cagle, G.D. An objective evaluation of eyedrop instillation in patients with glaucoma. Arch. Ophthalmol. 2009, 127, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Rotchford, A.P.; Murphy, K.M. Compliance with timolol treatment in glaucoma. Eye 1998, 12, 234–236. [Google Scholar] [CrossRef]
- Friedman, D.S.; Nordstrom, B.; Mozaffari, E.; Quigley, H.A. Glaucoma management among individuals enrolled in a single comprehensive insurance plan. Ophthalmology 2005, 112, 1500–1504. [Google Scholar] [CrossRef]
- Hermann, M.M.; Bron, A.M.; Creuzot-Garcher, C.P.; Diestelhorst, M. Measurement of adherence to brimonidine therapy for glaucoma using electronic monitoring. J. Glaucoma 2011, 20, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Morgan, L.B. A new drug delivery system for the eye. IMS Ind. Med. Surg. 1971, 40, 11–13. [Google Scholar]
- Maurice, D.M. Prolonged release systems and topically applied drugs. Sight Sav. Rev. 1972, 42, 42–50. [Google Scholar]
- Maddox, Y.T.; Bernstein, H.N. An evaluation of the Bionite hydrophilic contact lens for use in a drug delivery system. Ann. Ophthalmol. 1972, 4, 789–790. [Google Scholar]
- Hillman, J.S.; Marsters, J.B.; Broad, A. Pilocarpine delivery by hydrophilic lens in the management of acute glaucoma. Trans. Ophthalmol. Soc. UK 1975, 95, 79–84. [Google Scholar]
- Schultz, C.L.; Poling, T.R.; Mint, J.O. A medical device/drug delivery system for treatment of glaucoma. Clin. Exp. Optom. 2009, 92, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Uekama, K.; Otagiri, M. Cyclodextrins in drug carrier systems. Crit. Rev. Ther. Drug Carr. Syst. 1987, 3, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.C.; Kim, J.; Chauhan, A. Extended delivery of hydrophilic drugs from silicone-hydrogel contact lenses containing Vitamin E diffusion barriers. Biomaterials 2010, 31, 4032–4047. [Google Scholar] [CrossRef] [PubMed]
- García-Fernández, M.J.; Tabary, N.; Martel, B.; Cazaux, F.; Oliva, A.; Taboada, P.; Concheiro, A.; Alvarez-Lorenzo, C. Poly-(cyclo)dextrins as ethoxzolamide carriers in ophthalmic solutions and in contact lenses. Carbohydr. Polym. 2013, 98, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Hiratani, H.; Fujiwara, A.; Tamiya, Y.; Mizutani, Y.; Alvarez-Lorenzo, C. Ocular release of timolol from molecularly imprinted soft contact lenses. Biomaterials 2005, 26, 1293–1298. [Google Scholar] [CrossRef]
- Jung, H.J.; Chauhan, A. Temperature sensitive contact lenses for triggered ophthalmic drug delivery. Biomaterials 2012, 33, 2289–2300. [Google Scholar] [CrossRef]
- Jung, H.J.; Abou-Jaoude, M.; Carbia, B.E.; Plummer, C.; Chauhan, A. Glaucoma therapy by extended release of timolol from nanoparticle loaded silicone-hydrogel contact lenses. J. Control. Release 2013, 165, 82–89. [Google Scholar] [CrossRef]
- Carvalho, I.M.; Marques, C.S.; Oliveira, R.S.; Coelho, P.B.; Costa, P.C.; Ferreira, D.C. Sustained drug release by contact lenses for glaucoma treatment—A review. J. Control. Release 2015, 202, 76–82. [Google Scholar] [CrossRef]
- Asseff, C.F.; Weisman, R.L.; Podos, S.M.; Becker, B. Ocular penetration of pilocarpine in primates. Am. J. Ophthalmol. 1973, 75, 212–215. [Google Scholar] [CrossRef]
- Ramer, R.M.; Gasset, A.R. Ocular penetration of pilocarpine: The effect on concentration on the ocular penetration of pilocarpine. Ann. Ophthalmol. 1974, 6, 1160–1162. [Google Scholar]
- Marmion, V.J.; Yurdakul, S. Pilocarpine administration by contact lens. Trans. Ophthalmol. Soc. UK 1977, 97, 162–163. [Google Scholar]
- Peng, C.C.; Ben-Shlomo, A.; Mackay, E.O.; Plummer, C.E.; Chauhan, A. Drug delivery by contact lens in spontaneously glaucomatous dogs. Curr. Eye Res. 2012, 37, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Cho, S.; Park, H.S.; Kwon, I. Ocular drug delivery through pHEMA-Hydrogel contact lenses Co-loaded with lipophilic vitamins. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, H.; Fathalla, Z.; Moharram, H.; Ali, T.F.S.; Pierscionek, B. Cyclodextrin Enhances Corneal Tolerability and Reduces Ocular Toxicity Caused by Diclofenac. Oxid Med. Cell. Longev. 2018, 2018, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, N.J.; Bailey, L.A.O.; Becker, M.L.; Washburn, N.R.; Henderson, L.A. Macrophage response to methacrylate conversion using a gradient approach. Acta Biomater. 2007, 3, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Loftsson, T.; Másson, M.; Brewster, M.E. Self-Association of Cyclodextrins and Cyclodextrin Complexes. J. Pharm. Sci. 2004, 93, 1091–1099. [Google Scholar] [CrossRef]
- dos Santos, J.F.R.; Couceiro, R.; Concheiro, A.; Torres-Labandeira, J.J.; Alvarez-Lorenzo, C. Poly(hydroxyethyl methacrylate-co-methacrylated-β-cyclodextrin) hydrogels: Synthesis, cytocompatibility, mechanical properties and drug loading/release properties. Acta Biomater. 2008, 4, 745–755. [Google Scholar] [CrossRef]
- Ciolino, J.B.; Ross, A.E.; Tulsan, R.; Watts, A.C.; Wang, R.-F.; Zurakowski, D.; Serle, J.B.; Kohane, D.S. Latanoprost-Eluting Contact Lenses in Glaucomatous Monkeys. Ophthalmology 2016, 123, 2085–2092. [Google Scholar] [CrossRef]
- Carracedo, G.; Crooke, A.; Guzman-Aranguez, A.; Perez de Lara, M.J.; Martin-Gil, A.; Pintor, J. The role of dinucleoside polyphosphates on the ocular surface and other eye structures. Prog. Retin. Eye Res. 2016, 55, 182–205. [Google Scholar] [CrossRef]
- Loma, P.; Guzman-Aranguez, A.; Perez de Lara, M.J.; Pintor, J. Diadenosine tetraphosphate improves adrenergic anti-glaucomatous drug delivery and efficiency. Exp. Eye Res. 2015, 134, 141–147. [Google Scholar] [CrossRef]
- Zhang, X.; Cao, X.; Qi, P. Therapeutic contact lenses for ophthalmic drug delivery: Major challenges. J. Biomater. Sci. Polym Ed. 2020, 31, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Dumbleton, K.; Caffery, B.; Dogru, M.; Hickson-Curran, S.; Kern, J.; Kojima, T.; Morgan, P.B.; Purslow, C.; Robertson, D.M.; Nelson, J.D.; et al. The TFOS International Workshop on Contact Lens Discomfort: Report of the subcommittee on epidemiology. Investig. Ophthalmol. Vis. Sci. 2013, 54. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, Y.; Yu, F.; Coleman, A.L. Burden of undetected and untreated glaucoma in the United States. Am. J. Ophthalmol. 2014, 158, 1121–1129. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Glaucoma Medication | Name | Local Adverse Effects | Systemic Adverse Effects |
|---|---|---|---|
| Prostaglandin analogues | Latanoprost, travoprost, brimatoprost | Conjunctival hyperemia, lengthening of eyelashes, change of iris color, uveitis, macular edema, keratitis | Systemic effects related to headaches |
| α-adrenergic agonist | Brimonidine, apraclonidine | Ocular irritation, Dry eyes, ocular allergy | Hypotension, irregular heart rate, bitter taste, dry mouth, renal or hepatic failure, respiratory arrest in young children |
| β-adrenergic blockers | Timolol, levubonol, betaxolol | Ocular irritation, Dry eyes | Bradycardia, bronchospasm, depression, fatigue, respiratory effects |
| Carbonic anhydrase inhibitors | Dorzolamide, brinzolamide, acetazolamide | Ocular irritation, Dry eyes, burning sensation with topical agents | Topical form: minimal systemic effects Oral form: paresthesia, nausea, diarrhea, loss of appetite and taste, lassitude, renal stones |
| Cholinergic agonists | Pilocarpine, carbachol | Ocular irritation, induced myopia, decreased vision due to ciliary spasm | Ciliary spams carry headaches in young patients |
| FDA Group | Water Content (Percentage) | Ionicity * |
|---|---|---|
| I | <50% | Nonionic |
| II | >50% | Nonionic |
| III | <50% | Ionic |
| IV | >50% | Ionic |
| V | - | - |
| Drug | Method Used | Loading Conditions | Results | Ref. |
|---|---|---|---|---|
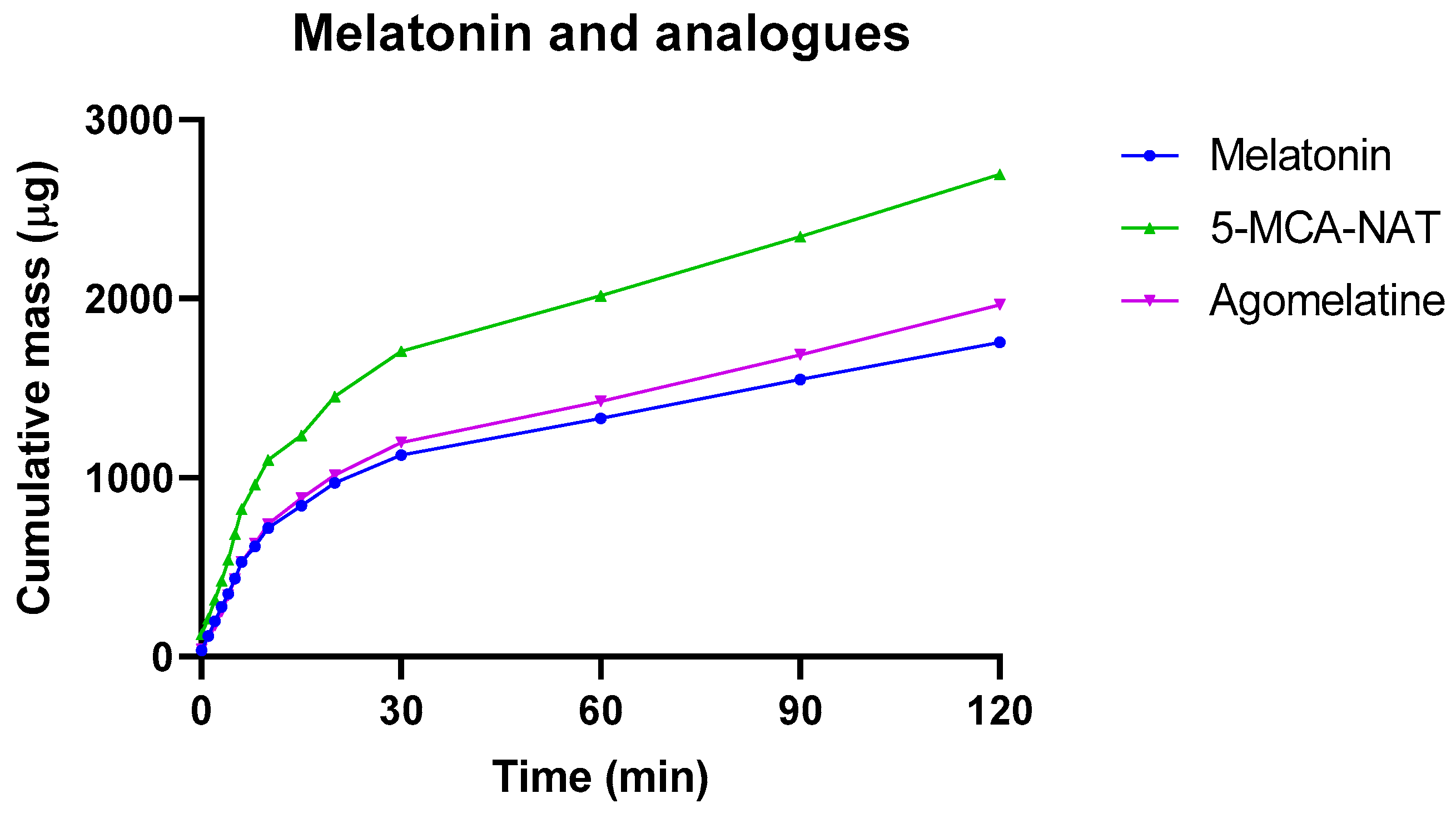
| Melatonin and analogues. | Soak and release. Balafilcon A | 1 mM concentration overnight (8 h) | In vitro: Increased time-release till 30 min | Figure 2 (original data) |
| Dinucleotides (Ap4A and Gp4G) | Soak and release. Balafilcon A | 1 mM concentration overnight (8 h) | In vitro: Increased time-release till 60 min, with 3 days of consecutive release | Figure 3 (original data) |
| Pilocarpine | Soak and release. Sauflon 85 (NVP and MMA) | 25 mL of 10 mg/mL pilocarpine for three days | 25 glaucomatous patients: Achieved same IOP control with 2 h worn than drop treatment, with a reduction of therapeutic dose (1% vs. 4%) | Hillman et al. [140] |
| Timolol or brimonidine | Soak and release. Varsufilcon A, etafilcon A and vifilcon CL | 0.65 mg/mL or 0.2 mg/mL for seven hours | 3 glaucomatous patients: Equivalent control of IOP than with eye drops with only using 30 min CLs per day for 14 days | Schultz 2009 [141] |
| Timolol | Soak and release. Lotrafilcon A | 2.67 mg/mL or 8 mg/mL solution for seven days | Glaucomatous dogs: Same efficacy with one-third drug loading for 4 days (5 mmHg). No IOP changes in untreated eye | Peng 2012 [142] |
| Timolol | Soak with vit-E. Narafilcon A | 3.5 mL of 1.5 mg/mL solution for seven days for control and 21 for vit E | Glaucomatous dogs: Same efficacy with 20% of dose on CL and eye drops. Increased time of hypotensive effects (4 days) | Peng 2012 [143] |
| Timolol and dorzolamide | Soak with vit-E. Senofilcon A | 3.5 mL of 12.75 mg/mL timolol and 20 mg/mL dorzolamide for four days | Glaucomatous dogs: Increased hypotensive effects for 8 days even after cessation of therapy. Less doses needed to obtain hypotensive effects (6-fold less) | Hsu 2015 [91] |
| Bimatoprost | Soak with vit-E. Senofilcon A and narafilcon A | 3 mL of 0.125 mg/mL bimatoprost for 2 days | In vitro: Increased time-release (>10 days) but reduces light transmission | Sekar 2019 [88] |
| Acetazolamide | Poly-CD. pHEMA CL | 5 mL acetazolamide 0.1 mg/mL for 4 days | In vitro: Increased time-release (24 days) | Dos Santos 2008 [144] |
| Ethoxzolamide | Poly-CD pHEMA CL | 1 mg/mL ethoxzolamide for 48 h | In vitro: Facilitated drug loading reaching 1 mg per lens. Increased time-release (>10 days). | García-Fernández 2013 [145] |
| Timolol | Molecular imprinted pHEMA CL | 10 mL of 1µM for three days | Rabbits: Increased time-release up to 180 min, twice as long as conventional CLs and three times as long as eye drops | Hiratani 2005 [146] |
| Timolol | Drug-PGT nanoparticles in Senofilcon A | 1 g timolol during CL polymerization | Glaucomatous dogs: Reduction of IOP during 2 days (4 mmHg) | Jung 2013 [147] |
| Timolol and latanoprost | mPEG-PLA micelles in Ocufilcon D | 50 µL of 100 µg timolol and 1 µg latanoprost | Rabbits with microspheres: Reduction of IOP during 7 days (7 mm Hg). Sustained drug release for up to 120 h for timolol and 96 h for latanoprost in tear film | Xu 2019 [121] |
| Latanoprost | PLGA between two layers of methafilcon | 80 µL of 50 mg/mL latanoprost | Rabbits: Higher IOP control, with higher concentration in aqueous humor compared to drops (1473 vs. 54 ng/mL) | Ciolino 2014 [60] |
| Latanoprost | PLGA between two layers of methafilcon | 30 and 40 µL of 10 mg/mL latanoprost | Glaucomatous monkeys: Increased time-release (>8 days). Higher IOP control than drop treatment (5.4 vs. 7.4 (low dose) and 9.3 (high dose)) | Ciolino 2015 [148] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peral, A.; Martinez-Aguila, A.; Pastrana, C.; Huete-Toral, F.; Carpena-Torres, C.; Carracedo, G. Contact Lenses as Drug Delivery System for Glaucoma: A Review. Appl. Sci. 2020, 10, 5151. https://doi.org/10.3390/app10155151
Peral A, Martinez-Aguila A, Pastrana C, Huete-Toral F, Carpena-Torres C, Carracedo G. Contact Lenses as Drug Delivery System for Glaucoma: A Review. Applied Sciences. 2020; 10(15):5151. https://doi.org/10.3390/app10155151
Chicago/Turabian StylePeral, Assumpta, Alejandro Martinez-Aguila, Cristina Pastrana, Fernando Huete-Toral, Carlos Carpena-Torres, and Gonzalo Carracedo. 2020. "Contact Lenses as Drug Delivery System for Glaucoma: A Review" Applied Sciences 10, no. 15: 5151. https://doi.org/10.3390/app10155151
APA StylePeral, A., Martinez-Aguila, A., Pastrana, C., Huete-Toral, F., Carpena-Torres, C., & Carracedo, G. (2020). Contact Lenses as Drug Delivery System for Glaucoma: A Review. Applied Sciences, 10(15), 5151. https://doi.org/10.3390/app10155151