Macrophage Accumulation and Angiogenesis in Epicardial Adipose Tissue in Cardiac Patients with or without Chronic Heart Failure


 , ,
, , 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Procedures
2.3. Risk Factor Analysis
2.4. EAT Histopathological, Immunohistochemical and Morphometrical Analysis
2.5. EAT Inflammation and Angiogenesis
2.6. Statistical Analysis
3. Results
3.1. CV Risk Factor Analysis
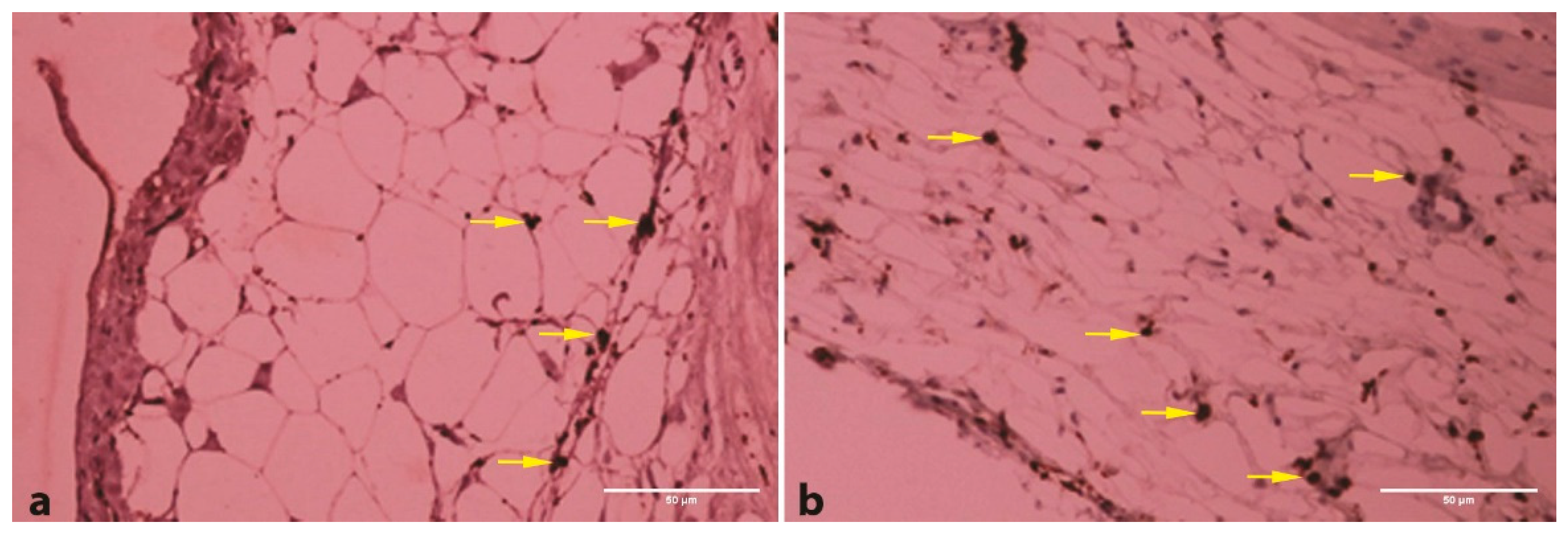
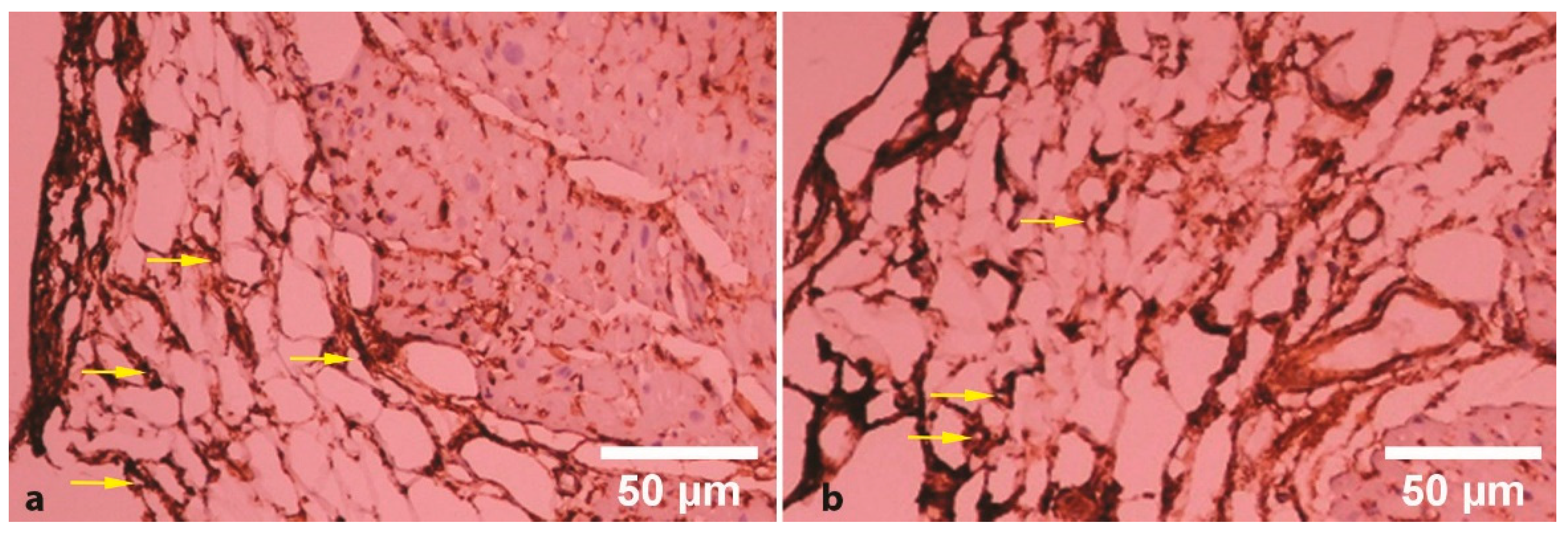
3.2. EAT Histopathological, Immunohistochemical and Morphometrical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Matloch, Z.; Kotulak, T.; Haluzik, M. The role of epicardial adipose tissue in heart disease. Physiol. Res. 2016, 65, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Barbaro, G. Epicardial adipose tissue feeding and overfeeding the heart. Nutrition 2019, 59, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Butcovan, D.; Oboroceanu, T.; Cimpeanu, C.; Mironescu, A.; Haliga, R.; Pinzariu, A.; Lupusoru, R.; Popescu, E.; Mocanu, V. The involvement of Epicardial adiposity and inflammation in Postoperatory atrial Fibrilation-Immunohistochemical qualitative and quantitative assessment. Rev. Chim. (Bucharest) 2017, 68, 8–13. [Google Scholar] [CrossRef]
- Ansaldo, A.M.; Montecucco, F.; Sahebkar, A.; Dallegri, F.; Carbone, F. Epicardial adipose tissue and cardiovascular diseases. Int. J. Cardiol. 2019, 278, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Bachar, G.N.; Dicker, D.; Kornowski, R.; Atar, E. Epicardial adipose tissue as a predictor of coronary artery disease in asymptomatic subjects. Am. J. Cardiol. 2012, 110, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Tinica, G.; Mocanu, V.; Zugun-Eloae, F.; Butcovan, D. Clinical and histological predictive risk factors of atrial fibrillation in patients undergoing open-heart surgery. Exp Ther Med 2015, 10, 2299–2304. [Google Scholar] [CrossRef] [Green Version]
- Iacobellis, G.; Ribaudo, M.C.; Zappaterreno, A.; Iannucci, C.V.; Leonetti, F. Relation between epicardial adipose tissue and left ventricular mass. Am J Cardiol 2004, 94, 1084–1087. [Google Scholar] [CrossRef]
- Ding, J.; Hsu, F.C.; Harris, T.B.; Liu, Y.; Kritchevsky, S.B.; Szklo, M.; Ouyang, P.; Espeland, M.A.; Lohman, K.K.; Criqui, M.H.; et al. The association of pericardial fat with incident coronary heart disease: the Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2009, 90, 499–504. [Google Scholar] [CrossRef]
- Mahabadi, A.A.; Massaro, J.M.; Rosito, G.A.; Levy, D.; Murabito, J.M.; Wolf, P.A.; O’Donnell, C.J.; Fox, C.S.; Hoffmann, U. Association of pericardial fat, intrathoracic fat, and visceral abdominal fat with cardiovascular disease burden: the Framingham Heart Study. Eur. Heart J. 2009, 30, 850–856. [Google Scholar] [CrossRef] [Green Version]
- Bala, C.; Craciun, A.E.; Hancu, N. Updating the Concept of Metabolically Healthy Obesity. Acta Endocrinol. (Bucharest) 2016, 12, 197–205. [Google Scholar] [CrossRef]
- Khawaja, T.; Greer, C.; Chokshi, A.; Chavarria, N.; Thadani, S.; Jones, M.; Schaefle, K.; Bhatia, K.; Collado, J.E.; Shimbo, D.; et al. Epicardial fat volume in patients with left ventricular systolic dysfunction. Am. J. Cardiol. 2011, 108, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Doesch, C.; Haghi, D.; Fluchter, S.; Suselbeck, T.; Schoenberg, S.O.; Michaely, H.; Borggrefe, M.; Papavassiliu, T. Epicardial adipose tissue in patients with heart failure. J. Cardiovasc. Magn. Reson. 2010, 12, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosito, G.A.; Massaro, J.M.; Hoffmann, U.; Ruberg, F.L.; Mahabadi, A.A.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample: the Framingham Heart Study. Circulation 2008, 117, 605–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matloch, Z.; Cinkajzlova, A.; Mraz, M.; Haluzik, M. The Role of Inflammation in Epicardial Adipose Tissue in Heart Diseases. Curr. Pharm. Des. 2018, 24, 297–309. [Google Scholar] [CrossRef]
- Parisi, V.; Paolillo, S.; Rengo, G.; Formisano, R.; Petraglia, L.; Grieco, F.; D’Amore, C.; Dellegrottaglie, S.; Marciano, C.; Ferrara, N.; et al. Sleep-disordered breathing and epicardial adipose tissue in patients with heart failure. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 126–132. [Google Scholar] [CrossRef]
- Timofte, D.; Mocanu, V.; Zugun Eloae, F.; Hristov, I.; Silivestru Cretu, I.; Aursulesei, V.; Balan, G.G.; Ciuntu, B.M.; Oboroceanu, T.; Tiron, A.; et al. Immunohistochemical Expression of Growth Hormone Secretagogue Receptor (GSH-R) of Adipose Tissue Macrophagesin Obese Bariatric Patients. Rev. Chim. (Bucharest) 2019, 70, 3428–3430. [Google Scholar] [CrossRef]
- Nagy, E.; Jermendy, A.L.; Merkely, B.; Maurovich-Horvat, P. Clinical importance of epicardial adipose tissue. Arch. Med. Sci. 2017, 13, 864–874. [Google Scholar] [CrossRef]
- Kitagawa, T.; Yamamoto, H.; Sentani, K.; Takahashi, S.; Tsushima, H.; Senoo, A.; Yasui, W.; Sueda, T.; Kihara, Y. Data set for volumetric and pathological findings of epicardial adipose tissue. Data Brief 2015, 5, 337–341. [Google Scholar] [CrossRef] [Green Version]
- Eroglu, S.; Sade, L.E.; Yildirir, A.; Bal, U.; Ozbicer, S.; Ozgul, A.S.; Bozbas, H.; Aydinalp, A.; Muderrisoglu, H. Epicardial adipose tissue thickness by echocardiography is a marker for the presence and severity of coronary artery disease. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 211–217. [Google Scholar] [CrossRef]
- Mahabadi, A.A.; Berg, M.H.; Lehmann, N.; Kalsch, H.; Bauer, M.; Kara, K.; Dragano, N.; Moebus, S.; Jockel, K.H.; Erbel, R.; et al. Association of epicardial fat with cardiovascular risk factors and incident myocardial infarction in the general population: the Heinz Nixdorf Recall Study. J. Am. Coll. Cardiol. 2013, 61, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Mookadam, F.; Goel, R.; Alharthi, M.S.; Jiamsripong, P.; Cha, S. Epicardial fat and its association with cardiovascular risk: a cross-sectional observational study. Heart Views 2010, 11, 103–108. [Google Scholar]
- Ahn, S.G.; Lim, H.S.; Joe, D.Y.; Kang, S.J.; Choi, B.J.; Choi, S.Y.; Yoon, M.H.; Hwang, G.S.; Tahk, S.J.; Shin, J.H. Relationship of epicardial adipose tissue by echocardiography to coronary artery disease. Heart 2008, 94, e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salazar, J.; Luzardo, E.; Mejias, J.C.; Rojas, J.; Ferreira, A.; Rivas-Rios, J.R.; Bermudez, V. Epicardial Fat: Physiological, Pathological, and Therapeutic Implications. Cardiol. Res. Pract. 2016, 2016, 1291537. [Google Scholar] [CrossRef] [Green Version]
- Fitzgibbons, T.P.; Czech, M.P. Epicardial and perivascular adipose tissues and their influence on cardiovascular disease: basic mechanisms and clinical associations. J. Am. Heart Assoc. 2014, 3, e000582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, D.S.; Zeng, H.L.; Li, R.; Huo, B.; Su, Y.S.; Fang, J.; Yang, Q.; Liu, L.G.; Hu, M.; Cheng, C.; et al. Aberrant Epicardial Adipose Tissue Extracellular Matrix Remodeling in Patients with Severe Ischemic Cardiomyopathy: Insight from Comparative Quantitative Proteomics. Sci. Rep. 2017, 7, 43787. [Google Scholar] [CrossRef]
- Aitken-Buck, H.M.; Babakr, A.A.; Coffey, S.; Jones, P.P.; Tse, R.D.; Lamberts, R.R. Epicardial adipocyte size does not correlate with body mass index. Cardiovasc. Pathol. 2019, 43, 107144. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Kurobe, H.; Akaike, M.; Chikugo, F.; Hori, T.; Bando, Y.; Nishio, C.; Higashida, M.; Nakaya, Y.; Kitagawa, T.; et al. Enhanced inflammation in epicardial fat in patients with coronary artery disease. Int. Heart J. 2011, 52, 139–142. [Google Scholar] [CrossRef] [Green Version]
- Schejbal, V. Epicardial fatty tissue of the right ventricle--morphology, morphometry and functional significance. Pneumologie 1989, 43, 490–499. [Google Scholar]
- Fosshaug, L.E.; Dahl, C.P.; Risnes, I.; Bohov, P.; Berge, R.K.; Nymo, S.; Geiran, O.; Yndestad, A.; Gullestad, L.; Aukrust, P.; et al. Altered Levels of Fatty Acids and Inflammatory and Metabolic Mediators in Epicardial Adipose Tissue in Patients With Systolic Heart Failure. J. Card. Fail. 2015, 21, 916–923. [Google Scholar] [CrossRef]
- Dozio, E.; Briganti, S.; Vianello, E.; Dogliotti, G.; Barassi, A.; Malavazos, A.E.; Ermetici, F.; Morricone, L.; Sigruener, A.; Schmitz, G.; et al. Epicardial adipose tissue inflammation is related to vitamin D deficiency in patients affected by coronary artery disease. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 267–273. [Google Scholar] [CrossRef]
- Iacobellis, G.; di Gioia, C.R.; Cotesta, D.; Petramala, L.; Travaglini, C.; De Santis, V.; Vitale, D.; Tritapepe, L.; Letizia, C. Epicardial adipose tissue adiponectin expression is related to intracoronary adiponectin levels. Horm. Metab. Res. 2009, 41, 227–231. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Patients without CHF (n = 9) | Patients with CHF (n = 6) |
|---|---|---|
| Age (y) | 58.3 ± 14.7 | 63.4 ± 11.2 |
| Male sex (%) | 33.3 | 100 * |
| Weight (kg) | 78.3 ± 14.5 | 88.0 ± 22.1 |
| BMI (kg/m2) | 27.6 ± 5.6 | 32.3 ± 7.1 * |
| Obesity (%) | 0 | 100 * |
| History | ||
| Dyslipidemia (%) | 33.3 | 100 |
| Arterial hypertension (%) | 66.6 | 50 |
| DM type 2 (%) | 66.6 | 50 |
| Smoking (%) | 33.3 | 0 |
| Echocardiography | ||
| LVEDD (cm) | 5.0 ± 0.5 | 6.9 ± 1.2 * |
| LVESD (cm) | 3.3± 0.6 | 5.6 ± 1.3 * |
| LVEF (%) | 54.1 ± 3.3 | 28.5 ± 7.2 * |
| Biochemical values | ||
| Total cholesterol (mg/dL) | 212 ± 42 | 206 ± 38 ∗ |
| Triglycerides (mg/dL) | 161 ± 12 | 175 ±54 * |
| LDL cholesterol (mg/dL) | 124 ± 9 | 135 ± 11 * |
| HDL cholesterol (mg/dL) | 57 ± 4 | 45 ± 3 * |
| Patients | EAT thickness (μm) | CD68 (No/μm2) | CD34 (No/μm2) |
|---|---|---|---|
| Without CHF | 217.1 ± 21.3 | 244.9 ± 5.5 | 65.2 ± 1.7 |
| With CHF | 185.8 ± 27.9 | 325.7 ± 16.1 | 22.7 ± 3.8 |
| p-value | 0.07 | <0.001 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butcovan, D.; Mocanu, V.; Timofte, D.V.; Costan, V.V.; Danila, R.; Veselin, A.P.; Ciuntu, B.M.; Haliga, R.E.; Sascau, R.A.; Ghiga, G.; et al. Macrophage Accumulation and Angiogenesis in Epicardial Adipose Tissue in Cardiac Patients with or without Chronic Heart Failure. Appl. Sci. 2020, 10, 5871. https://doi.org/10.3390/app10175871
Butcovan D, Mocanu V, Timofte DV, Costan VV, Danila R, Veselin AP, Ciuntu BM, Haliga RE, Sascau RA, Ghiga G, et al. Macrophage Accumulation and Angiogenesis in Epicardial Adipose Tissue in Cardiac Patients with or without Chronic Heart Failure. Applied Sciences. 2020; 10(17):5871. https://doi.org/10.3390/app10175871
Chicago/Turabian StyleButcovan, Doina, Veronica Mocanu, Daniel V. Timofte, Victor V. Costan, Radu Danila, Adina Pricope Veselin, Bogdan M. Ciuntu, Raluca E. Haliga, Radu A. Sascau, Gabriela Ghiga, and et al. 2020. "Macrophage Accumulation and Angiogenesis in Epicardial Adipose Tissue in Cardiac Patients with or without Chronic Heart Failure" Applied Sciences 10, no. 17: 5871. https://doi.org/10.3390/app10175871
APA StyleButcovan, D., Mocanu, V., Timofte, D. V., Costan, V. V., Danila, R., Veselin, A. P., Ciuntu, B. M., Haliga, R. E., Sascau, R. A., Ghiga, G., & Statescu, C. (2020). Macrophage Accumulation and Angiogenesis in Epicardial Adipose Tissue in Cardiac Patients with or without Chronic Heart Failure. Applied Sciences, 10(17), 5871. https://doi.org/10.3390/app10175871