The Invasion of Bacterial Biofilms into the Dentinal Tubules of Extracted Teeth Retrofilled with Fluorescently Labeled Retrograde Filling Materials

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Teeth Collection, Preparation, and Distribution into Groups
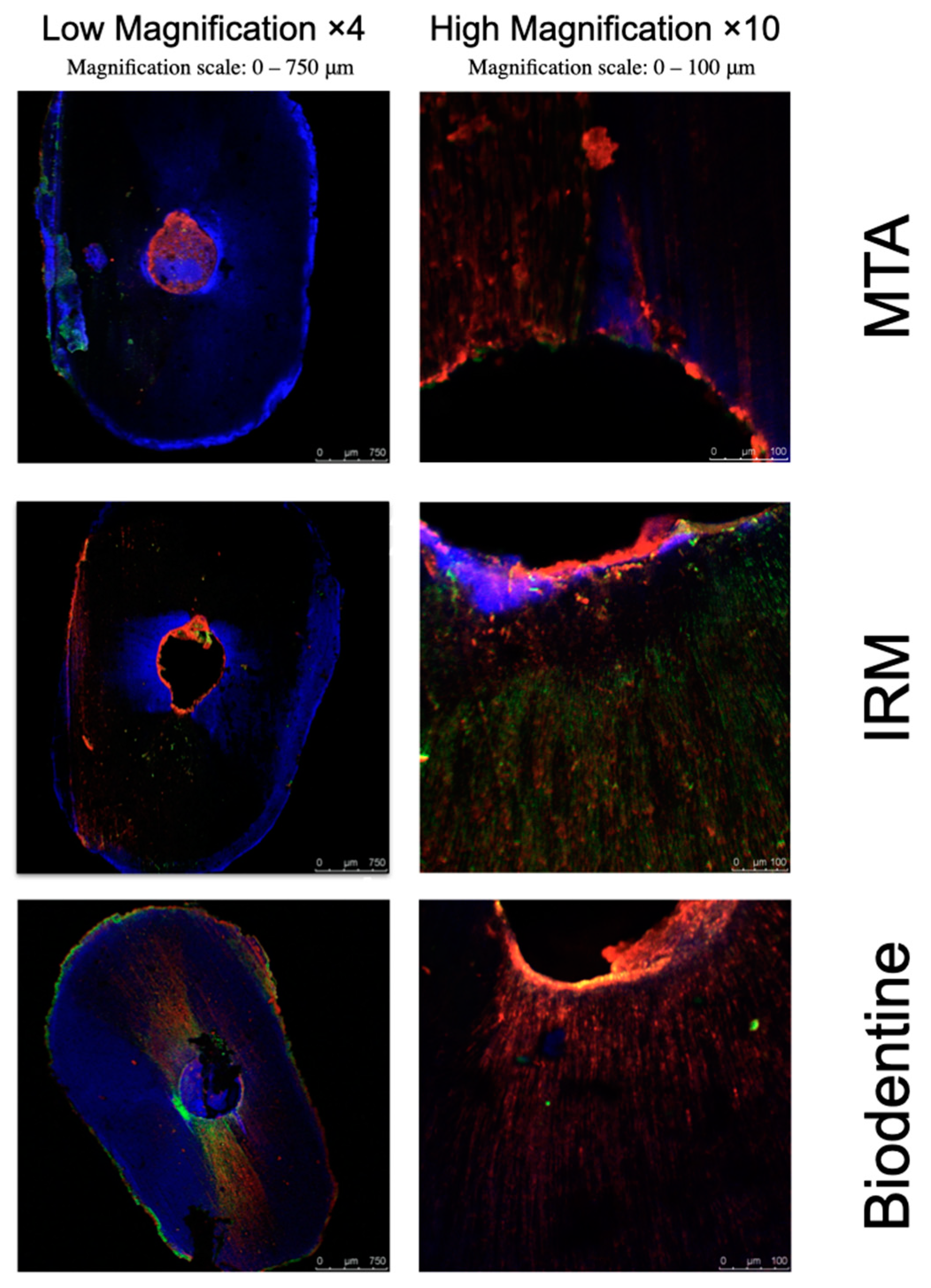
- (n = 15): Retrograde 3 mm preparations filled with fluorescently labeled MTA (ProRoot; Dentsply Tulsa Dental, Johnson City, TN, USA).
- (n = 15): Retrograde 3 mm preparations filled with fluorescently labeled IRM (IRM; Dentsply, Mannheim, Germany).
- (n = 15): Retrograde 3 mm preparations filled with fluorescently labeled Biodentine (Biodentine; Septodont, Saint-Maur-des-Fossés, France).
- (n = 5): Retrograde 3 mm preparations, not filled (Positive control).
- (n = 5): Like Group 1 but without ensuing bacterial contamination (MTA negative control).
- (n = 5): Like Group 2 but without ensuing bacterial contamination (IRM negative control).
- (n = 5): Like Group 3 but without ensuing bacterial contamination (Biodentine negative control).
2.2. The Experimental Model
2.3. Simulation of Enterococcus Faecalis Bacterial Infection
2.4. Preparing the Roots for the Assessments
2.5. Confocal Laser Microscopy Assessment
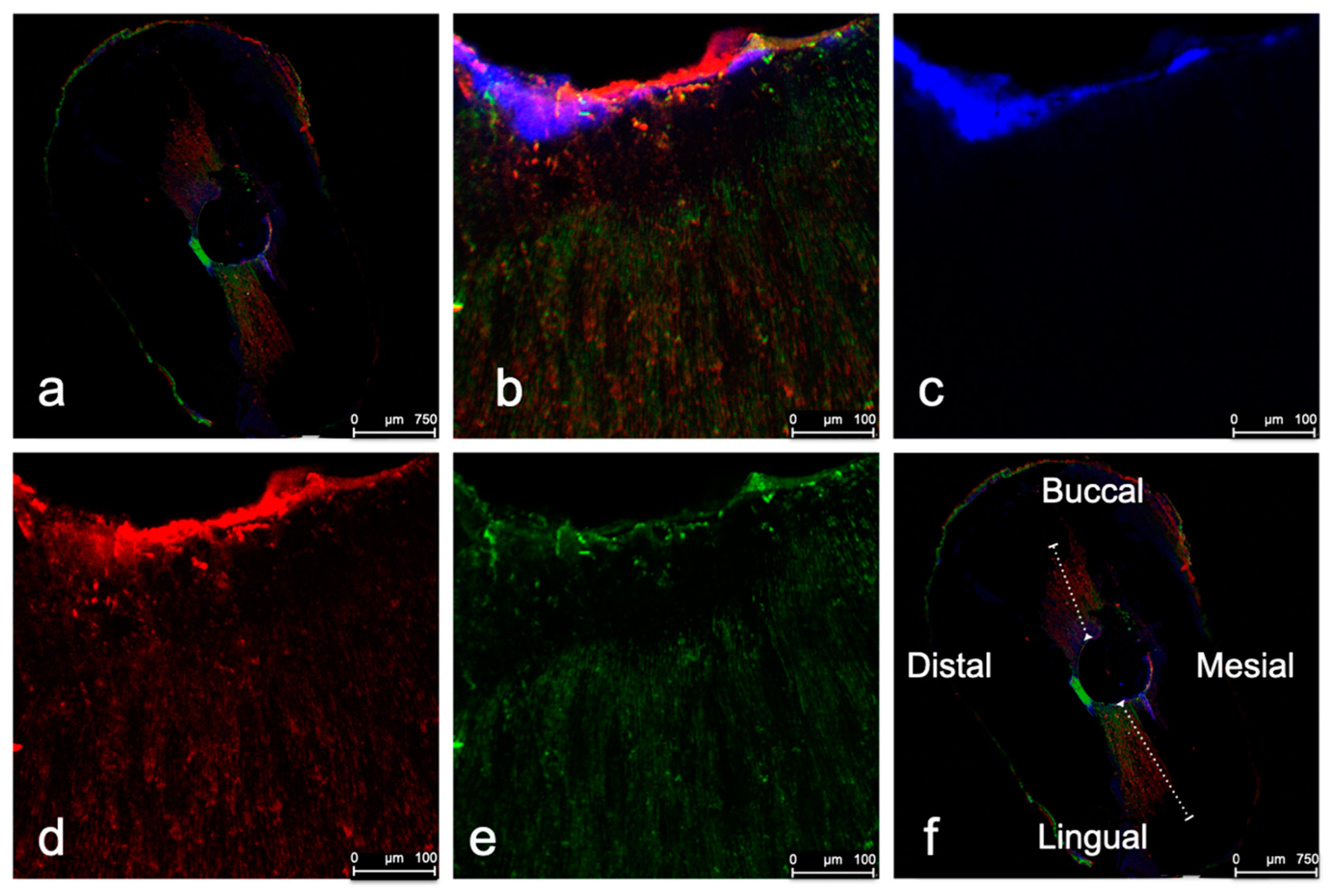
- The depths of bacterial invasion and filling penetrations within the tubuli were measured at the buccal, lingual, mesial, and distal areas of the root dentin axial slices, defining the root canal wall as the beginning point (Figure 2f).
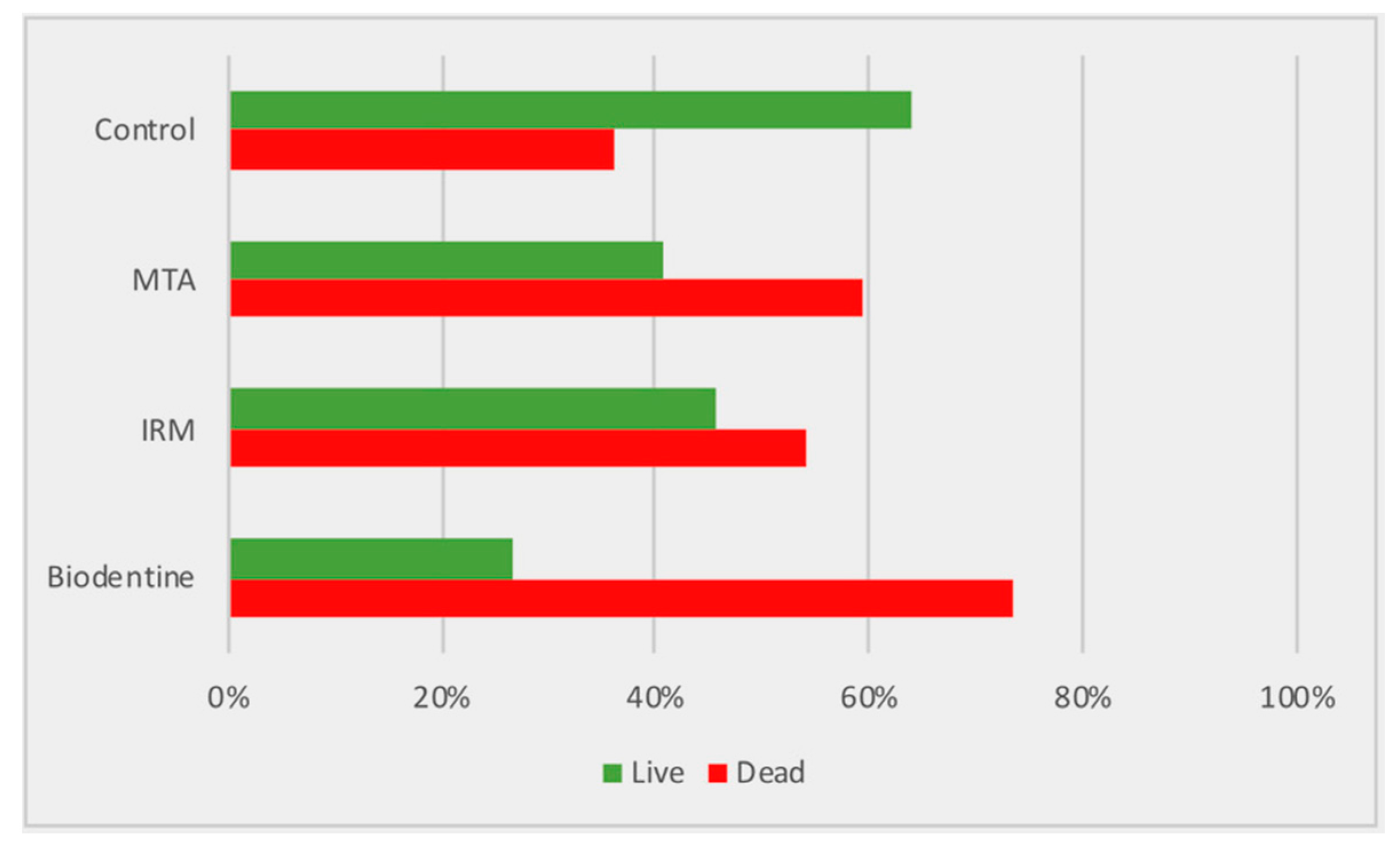
- The bacterial viability was calculated as the proportions of live and dead bacteria.
- The correlation between the filling material type and penetration depth, and that between the bacterial invasion depth and viability, was determined.
2.6. Statistical Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gartner, A.H.; Dorn, S.O. Advances in endodontic surgery. Dent. Clin. N. Am. 1992, 36, 357–378. [Google Scholar] [PubMed]
- Tsesis, I.; Elbahary, S.; Venezia, N.B.; Rosen, E. Bacterial colonization in the apical part of extracted human teeth following root-end resection and filling: A confocal laser scanning microscopy study. Clin. Oral Investig. 2018, 22, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Gundam, S.; Patil, J.; Venigalla, B.S.; Yadanaparti, S.; Maddu, R.; Gurram, S.R. Comparison of marginal adaptation of mineral trioxide aggregate, glass ionomer cement and intermediate restorative material as root-end filling materials, using scanning electron microscope: An in vitro study. J. Conserv. Dent. 2014, 17, 566–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nepal, M.; Shubham, S.; Tripathi, R.; Khadka, J.; Kunwar, D.; Gautam, V.; Gautam, N. Spectrophotometric analysis evaluating apical microleakage in retrograde filling using GIC, MTA and biodentine: An in-vitro study. BMC Oral Health 2020, 20, 37. [Google Scholar] [CrossRef]
- Heinrich, K.; Leslie, D.J.; Jonas, K. Modulation of bacterial proliferation as a survival strategy. Adv. Appl. Microbiol. 2015, 92, 127–171. [Google Scholar] [CrossRef]
- Kuci, A.; Alacam, T.; Yavas, O.; Ergul-Ulger, Z.; Kayaoglu, G. Sealer penetration into dentinal tubules in the presence or absence of smear layer: A confocal laser scanning microscopic study. J. Endod. 2014, 40, 1627–1631. [Google Scholar] [CrossRef]
- Aziz, A.; Parmar, D.; McNaughton, A.; Tompkins, G.R. Bacterial viability determination in a dentinal tubule infection model by confocal laser scanning microscopy. Methods Mol. Biol. 2010, 666, 141–150. [Google Scholar] [CrossRef]
- Zapata, R.O.; Bramante, C.M.; de Moraes, I.G.; Bernardineli, N.; Gasparoto, T.H.; Graeff, M.S.; Campanelli, A.P.; Garcia, R.B. Confocal laser scanning microscopy is appropriate to detect viability of Enterococcus faecalis in infected dentin. J. Endod. 2008, 34, 1198–1201. [Google Scholar] [CrossRef]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Wu, M.K.; R’Oris, A.; Barkis, D.; Wesselink, P.R. Prevalence and extent of long oval canals in the apical third. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 739–743. [Google Scholar] [CrossRef] [Green Version]
- Roane, J.B.; Sabala, C.L.; Duncanson, M.G., Jr. The “balanced force” concept for instrumentation of curved canals. J. Endod. 1985, 11, 203–211. [Google Scholar] [CrossRef]
- Kytridou, V.; Gutmann, J.L.; Nunn, M.H. Adaptation and sealability of two contemporary obturation techniques in the absence of the dentinal smear layer. Int. Endod. J. 1999, 32, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Adamo, H.L.; Buruiana, R.; Schertzer, L.; Boylan, R.J. A comparison of MTA, Super-EBA, composite and amalgam as root-end filling materials using a bacterial microleakage model. Int. Endod. J. 1999, 32, 197–203. [Google Scholar] [CrossRef]
- Brosco, V.H.; Bernardineli, N.; Torres, S.A.; Consolaro, A.; Bramante, C.M.; de Moraes, I.G.; Ordinola-Zapata, R.; Garcia, R.B. Bacterial leakage in obturated root canals-part 2: A comparative histologic and microbiologic analyses. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Fuss, Z.; Weiss, E.I.; Shalhav, M. Antibacterial activity of calcium hydroxide-containing endodontic sealers on Enterococcus faecalis in vitro. Int. Endod. J. 1997, 30, 397–402. [Google Scholar] [CrossRef]
- Panchuk-Voloshina, N.; Haugland, R.P.; Bishop-Stewart, J.; Bhalgat, M.K.; Millard, P.J.; Mao, F.; Leung, W.Y.; Haugland, R.P. Alexa dyes, a series of new fluorescent dyes that yield exceptionally bright, photostable conjugates. J. Histochem. Cytochem. 1999, 47, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Ørstavik, D. Endodontic filling materials. Endod. Top. 2014, 31, 53–67. [Google Scholar] [CrossRef]
- Kim, S.G. Variations in Outcome of Endodontic Surgery; Tsesis, I., Ed.; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar] [CrossRef]
- Rosen, E.; Kolodkin-Gal, I.; Tsesis, I. Challenges in the Eradication of Enterococcus faecalis and its Implications on Health. Curr. Oral Health Rep. 2018. [Google Scholar] [CrossRef]
- Love, R.M.; Jenkinson, H.F. Invasion of dentinal tubules by oral bacteria. Crit. Rev. Oral Biol. Med. 2002, 13, 171–183. [Google Scholar] [CrossRef] [Green Version]
- Langeland, K. Tissue response to dental caries. Endod. Dent. Traumatol. 1987, 3, 149–171. [Google Scholar] [CrossRef]
- De-Deus, G. Research that matters—Root canal filling and leakage studies. Int. Endod. J. 2012, 45, 1063–1064. [Google Scholar] [CrossRef] [PubMed]
- Rechenberg, D.K.; De-Deus, G.; Zehnder, M. Potential systematic error in laboratory experiments on microbial leakage through filled root canals: Review of published articles. Int. Endod. J. 2011, 44, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Rechenberg, D.K.; Thurnheer, T.; Zehnder, M. Potential systematic error in laboratory experiments on microbial leakage through filled root canals: An experimental study. Int. Endod. J. 2011, 44, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Vertucci, F.J.; Beatty, R.G. Apical leakage associated with retrofilling techniques: A dye study. J. Endod. 1986, 12, 331–336. [Google Scholar] [CrossRef]
- Kielbassa, A.M.; Uchtmann, H.; Wrbas, K.T.; Bitter, K. In vitro study assessing apical leakage of sealer-only backfills in root canals of primary teeth. J. Dent. 2007, 35, 607–613. [Google Scholar] [CrossRef]
- Rosen, E.; Tsesis, I.; Elbahary, S.; Storzi, N.; Kolodkin-Gal, I. Eradication of Enterococcus faecalis Biofilms on Human Dentin. Front. Microbiol. 2016, 7, 2055. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, B.S.; Kim, Y.M.; Lee, D.; Kim, S.Y. The Penetration Ability of Calcium Silicate Root Canal Sealers into Dentinal Tubules Compared to Conventional Resin-Based Sealer: A Confocal Laser Scanning Microscopy Study. Materials (Basel) 2019, 12, 531. [Google Scholar] [CrossRef] [Green Version]
- Dorn, S.O.; Gartner, A.H. Retrograde filling materials: A retrospective success-failure study of amalgam, EBA, and IRM. J. Endod. 1990, 16, 391–393. [Google Scholar] [CrossRef]
- Peters, L.B.; Wesselink, P.R.; Moorer, W.R. The fate and the role of bacteria left in root dentinal tubules. Int. Endod. J. 1995, 28, 95–99. [Google Scholar] [CrossRef]
- Weis, M.V.; Parashos, P.; Messer, H.H. Effect of obturation technique on sealer cement thickness and dentinal tubule penetration. Int. Endod. J. 2004, 37, 653–663. [Google Scholar] [CrossRef] [Green Version]
- Vasiliadis, L.; Darling, A.I.; Levers, B.G. The amount and distribution of sclerotic human root dentine. Arch. Oral Biol. 1983, 28, 645–649. [Google Scholar] [CrossRef]
- Russell, A.A.; Chandler, N.P.; Hauman, C.; Siddiqui, A.Y.; Tompkins, G.R. The butterfly effect: An investigation of sectioned roots. J. Endod. 2013, 39, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.B.; Wesselink, P.R.; Buijs, J.F.; van Winkelhoff, A.J. Viable bacteria in root dentinal tubules of teeth with apical periodontitis. J. Endod. 2001, 27, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Li, C.; Jia, L.; Wang, Y.; Liu, W.; Zhou, X.; Johnson, T.M.; Huang, D. Materials for retrograde filling in root canal therapy. Cochrane Database Syst. Rev. 2016, 12, CD005517. [Google Scholar] [CrossRef]
- Torabinejad, M.; Parirokh, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part II: Other clinical applications and complications. Int. Endod. J. 2018, 51, 284–317. [Google Scholar] [CrossRef]
- Camilleri, J.; Sorrentino, F.; Damidot, D. Investigation of the hydration and bioactivity of radiopacified tricalcium silicate cement, Biodentine and MTA Angelus. Dent. Mater. 2013, 29, 580–593. [Google Scholar] [CrossRef]
- Torabinejad, M.; Hong, C.U.; Pitt Ford, T.R.; Kettering, J.D. Antibacterial effects of some root end filling materials. J. Endod. 1995, 21, 403–406. [Google Scholar] [CrossRef]
- Slutzky, H.; Slutzky-Goldberg, I.; Weiss, E.I.; Matalon, S. Antibacterial properties of temporary filling materials. J. Endod. 2006, 32, 214–217. [Google Scholar] [CrossRef]
- Chong, B.S.; Owadally, I.D.; Pitt Ford, T.R.; Wilson, R.F. Antibacterial activity of potential retrograde root filling materials. Endod. Dent. Traumatol. 1994, 10, 66–70. [Google Scholar] [CrossRef]
- Bani, M.; Sungurtekin-Ekci, E.; Odabas, M.E. Efficacy of Biodentine as an Apical Plug in Nonvital Permanent Teeth with Open Apices: An In Vitro Study. BioMed Res. Int. 2015, 2015, 359275. [Google Scholar] [CrossRef] [Green Version]
- Roberts, A.E.; Kragh, K.N.; Bjarnsholt, T.; Diggle, S.P. The Limitations of In Vitro Experimentation in Understanding Biofilms and Chronic Infection. J. Mol. Biol. 2015, 427, 3646–3661. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Filling Material Penetration | Bacterial Penetration | Group | ||||||
|---|---|---|---|---|---|---|---|---|
| SD | Median | Max | Min | SD | Median | Max | Min | |
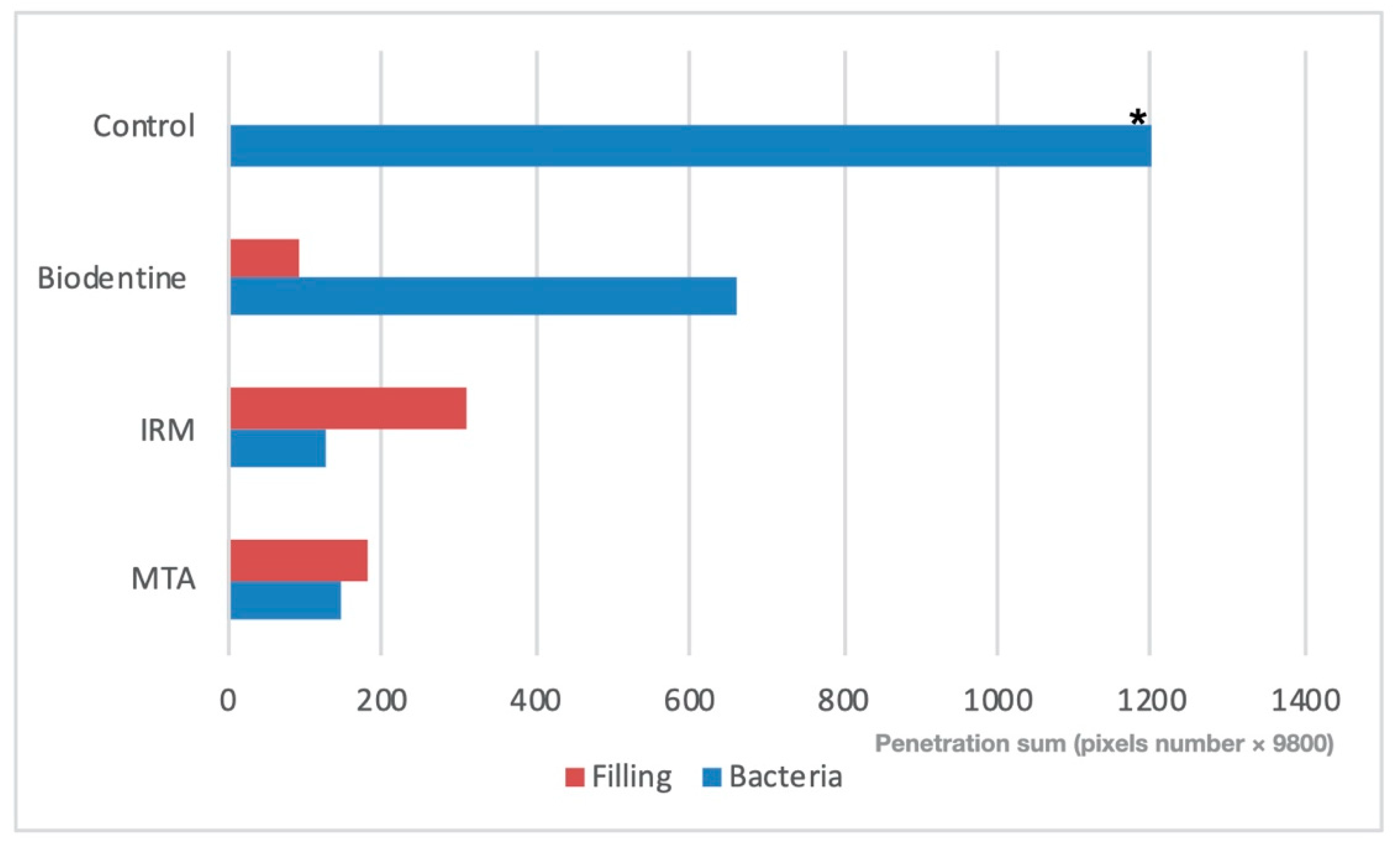
| 198 | 183 | 644 | 58 | 158 | 146 | 500 | 33 | MTA |
| 158 | 311 | 957 | 11 | 342 | 129 | 996 | 9 | IRM |
| 155 | 93 a | 535 a | 32 | 451 | 663 b | 1480 | 160 | Biodentine |
| - | - | - | - | 189 | 1200 c | 1610 | 890 c | Control |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosen, E.; Elbahary, S.; Haj-Yahya, S.; Jammal, L.; Shemesh, H.; Tsesis, I. The Invasion of Bacterial Biofilms into the Dentinal Tubules of Extracted Teeth Retrofilled with Fluorescently Labeled Retrograde Filling Materials. Appl. Sci. 2020, 10, 6996. https://doi.org/10.3390/app10196996
Rosen E, Elbahary S, Haj-Yahya S, Jammal L, Shemesh H, Tsesis I. The Invasion of Bacterial Biofilms into the Dentinal Tubules of Extracted Teeth Retrofilled with Fluorescently Labeled Retrograde Filling Materials. Applied Sciences. 2020; 10(19):6996. https://doi.org/10.3390/app10196996
Chicago/Turabian StyleRosen, Eyal, Shlomo Elbahary, Sohad Haj-Yahya, Lotof Jammal, Hagay Shemesh, and Igor Tsesis. 2020. "The Invasion of Bacterial Biofilms into the Dentinal Tubules of Extracted Teeth Retrofilled with Fluorescently Labeled Retrograde Filling Materials" Applied Sciences 10, no. 19: 6996. https://doi.org/10.3390/app10196996
APA StyleRosen, E., Elbahary, S., Haj-Yahya, S., Jammal, L., Shemesh, H., & Tsesis, I. (2020). The Invasion of Bacterial Biofilms into the Dentinal Tubules of Extracted Teeth Retrofilled with Fluorescently Labeled Retrograde Filling Materials. Applied Sciences, 10(19), 6996. https://doi.org/10.3390/app10196996