Immediate Implant Placement and Provisionalization in the Esthetic Zone Revisited: The Marginal Migration Concept (MMC)

Abstract
:1. Introduction
2. Case 1
2.1. “Report and Protocol”
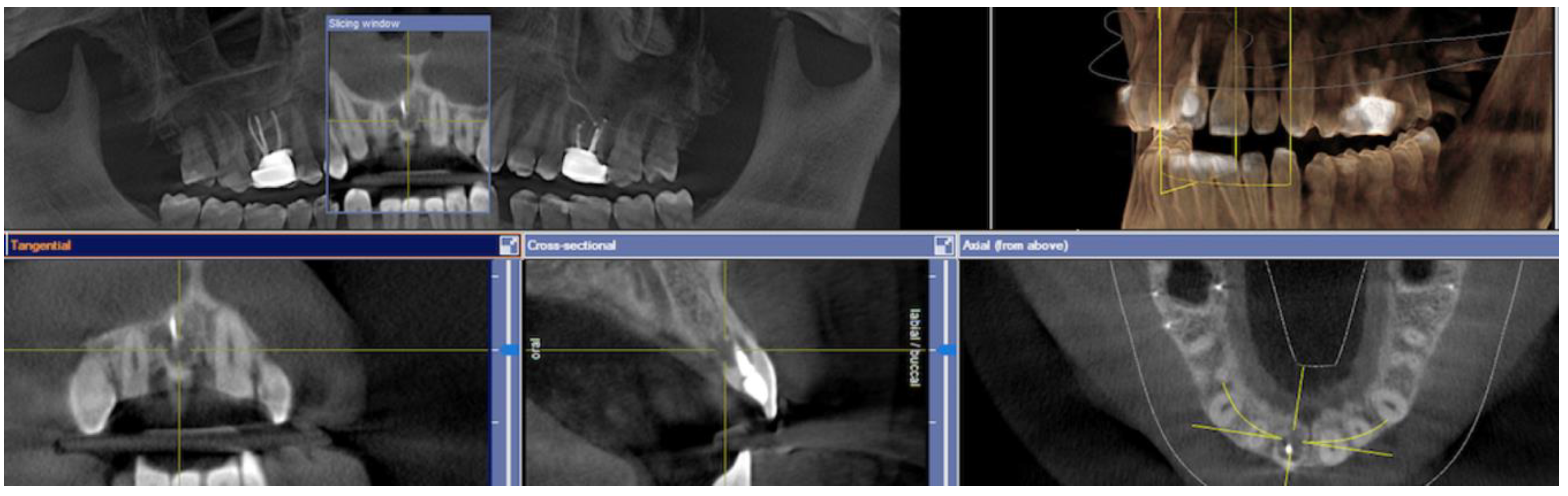
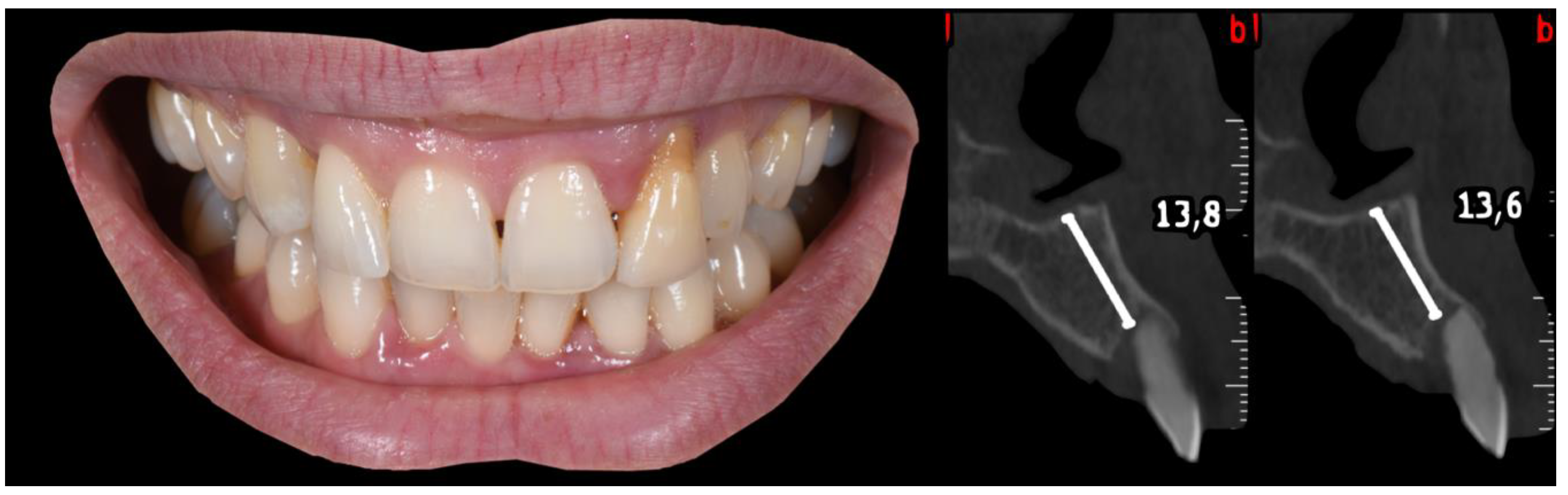
2.2. Pre-Surgical Stage
2.3. Surgical Stage
- (A)
- Extraction socket presentation, where the red line represents the supra-periosteal pouch flap.
- (B)
- Three-dimensional implant positioning, where different locations of the implant axis can achieve the desired location of the platform and neck of the implant.
- (C)
- Fits abutment selection, where the shoulder is located 0.5 mm apically to the cervical gingival margin.
- (D)
- Membrane adaptation, being in contact with the internal wall of the socket.
- (E)
- Bone replacement graft BRG introduction into the available space present within the socket, occupying both the soft and hard tissue zones present below the abutment’s shoulder.
- (F)
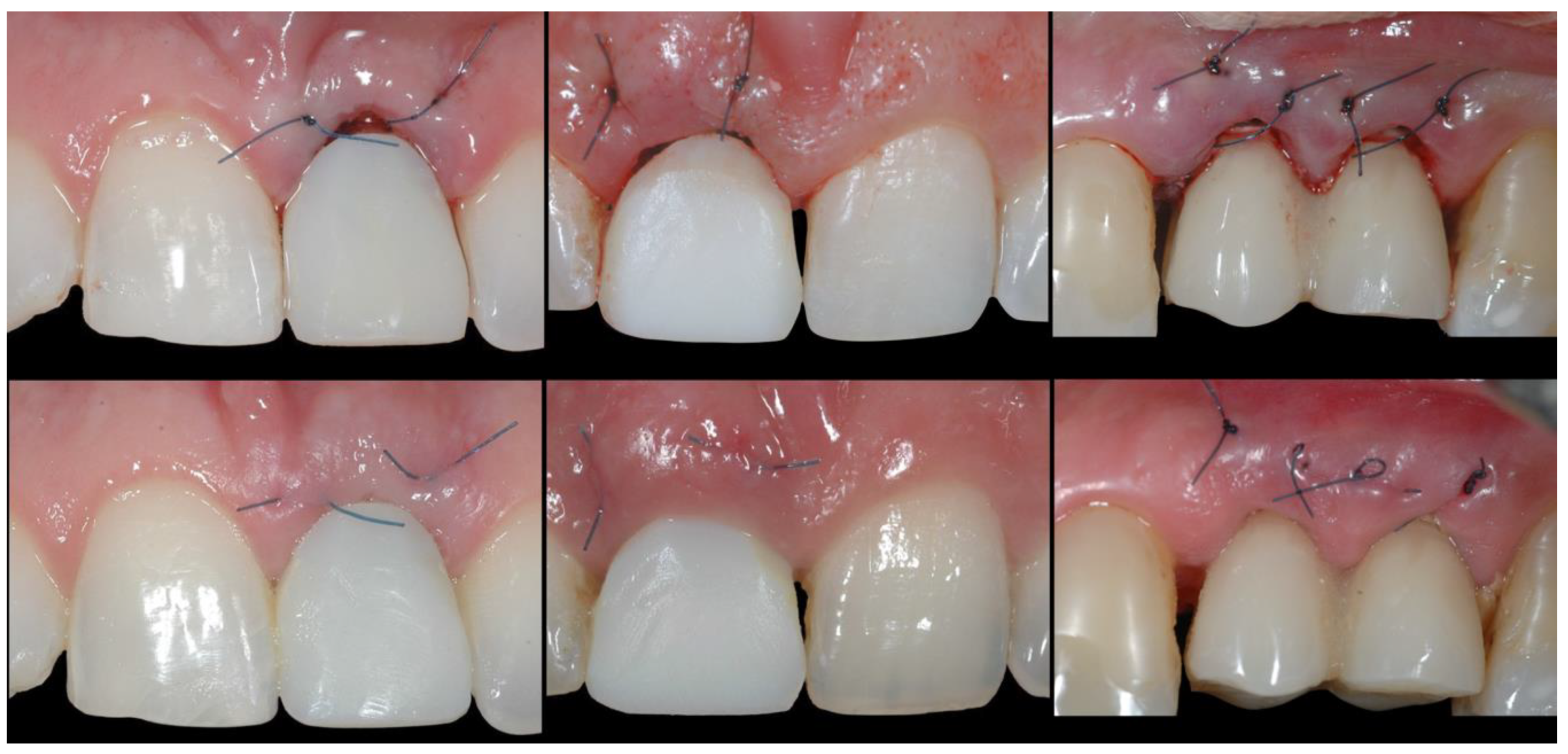
- Membrane adaptation and suturing with vertical mattress sutures.
- (G)
- Temporary prosthesis delivery, where the cervical margin is located supra-gingivally and comprises a 90′ emergence angle in relation to the abutment.
- (A)
- Supra-periosteal pouch design, demonstrating proper lateral and vertical extensions. The red lines demonstrate the pouch, while the yellow line demonstrates the mucogingival junction.
- (B)
- First abutment in place and membrane adaptation prior to BRG introduction.
- (C)
- Final relationship between first temporary prosthesis, abutment, and cervical gingival tissue.
2.4. Transitional Restoration Stage
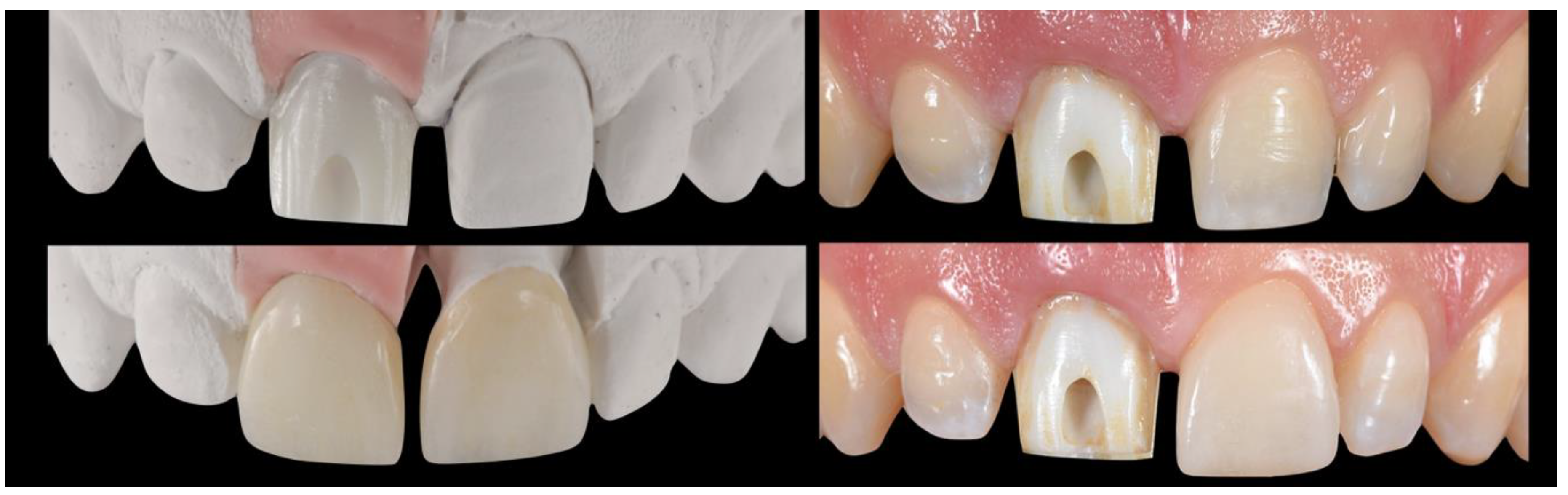
2.5. Impression Stage
2.6. Lab Stage
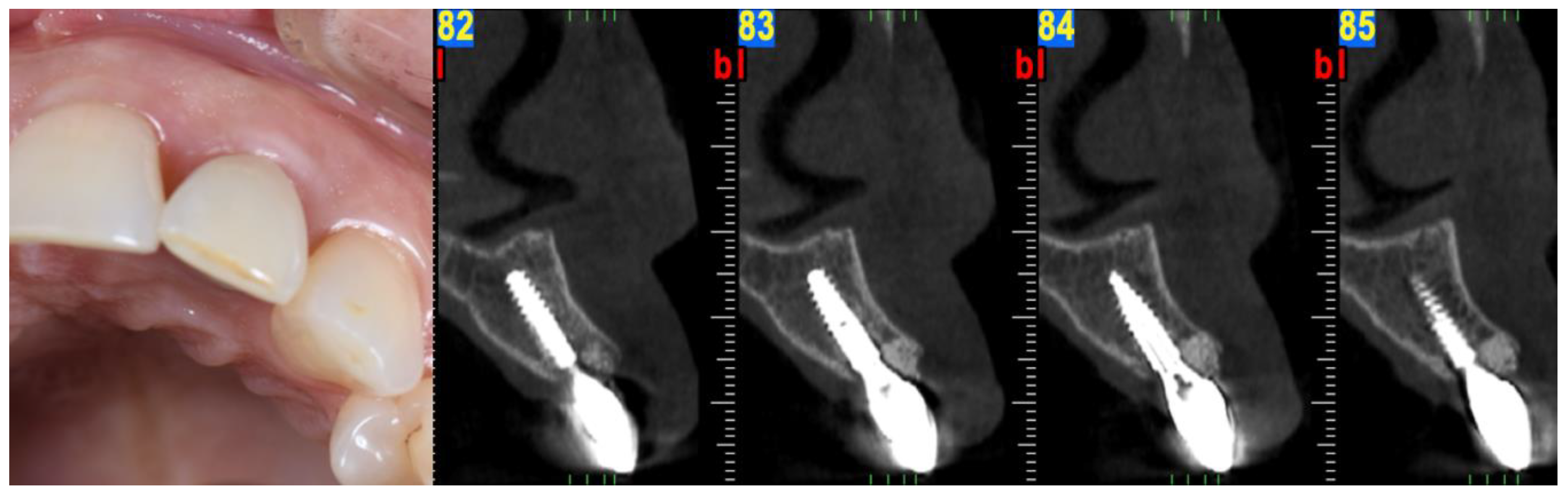
2.7. Prosthesis Delivery
3. Case 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Avila, G.; Galindo, P.; Rios, H.; Wang, H.L. Immediate implant loading: Current status from available literature. Implant Dent. 2007, 16, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Amler, M.H. The time sequence of tissue regeneration in human extraction wounds. Oral Surg. Oral Med. Oral Pathol. 1969, 27, 309–318. [Google Scholar] [CrossRef]
- Cardaropoli, G.; Araújo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Ridge alterations following implant placement in fresh extraction sockets; an experimental study in the dog. J. Clin. Periodontol. 2005, 32, 645–665. [Google Scholar] [CrossRef]
- Araujo, M.G.; Sukekava, F.; Wennstrom, J.L.; Lindhe, J. Tissue modeling following implant placement in fresh extraction sockets. Clin. Oral Implant. Res. 2006, 17, 615–624. [Google Scholar] [CrossRef]
- Araujo, M.G.; Wennstrom, J.L.; Lindhe, J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation. Clin. Oral Implant. Res. 2006, 17, 606–614. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Landsberg, C.J.; Bichacho, N. A modified surgical/prosthetic approach for optimal single implant supported crown. Part I--The socket seal surgery. Pract. Periodontics Aesthet Dent. 1994, 6, 11–17. [Google Scholar]
- Hurzeler, M.B.; Zuhr, O.; Schupbach, P.; Rebele, S.F.; Emmanouilidis, N.; Fickl, S. The socket-shield technique: A proof-of-principle report. J. Clin. Periodontol. 2010, 37, 855–862. [Google Scholar] [CrossRef]
- Chu, S.J.; Hochman, M.N.; Tan-Chu, J.H.; Mieleszko, A.J.; Tarnow, D.P. A Novel Prosthetic Device and Method for Guided Tissue Preservation of Immediate Postextraction Socket Implants. Int. J. Periodontics Restor. Dent. 2014, 34, S9–S17. [Google Scholar]
- Waki, T.; Kan, J.Y. Immediate placement and provisionalization of maxillary anterior single implant with guided bone regeneration, connective tissue graft, and coronally positioned flap procedures. Int. J. Esthet Dent. 2016, 11, 174–185. [Google Scholar]
- Chen, S.T.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla--a systematic review. Int. J. Oral Maxillofac Implant. 2014, 29, 186–215. [Google Scholar] [CrossRef] [Green Version]
- Tarnow, D.; Chu, S.; Salama, M.; Stappert, C.; Salama, H.; Garber, D.; Sarnachiaro, G.; Sarnachiaro, E.; Gotta, S.; Saito, H. Flapless postextraction socket implant placement in the esthetic zone: Part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int. J. Periodontics Restor. Dent. 2014, 34, 323–331. [Google Scholar] [CrossRef]
- Chu, S.; Salama, M.; Garber, D.; Salama, H.; Sarnachiaro, G.; Sarnachiaro, E.; Gotta, S.; Reynolds, M.; Saito, H.; Tarnow, D. Flapless Postextraction Socket Implant Placement, Part 2: The Effects of Bone Grafting and Provisional Restoration on Peri-implant Soft Tissue Height and Thickness—A Retrospective Study. Int. J. Periodontics Restor. Dent. 2015, 35, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Amato, F.; Polara, G.; Spedicato, G.A. Tissue Dimensional Changes in Single-Tooth Immediate Extraction Implant Placement in the Esthetic Zone: A Retrospective Clinical Study. Int. J. Oral Maxillofac Implant. 2018, 33, 439–447. [Google Scholar] [CrossRef] [Green Version]
- Mitsias, M.M.; Bratos, M.; Siormpas, K.; Pikos, M.A.; Kotsakis, G.A.; Root Membrane Group. Longitudinal Soft Tissue Changes during Periodontal Ligament-Mediated Immediate Implant Placement with the Root-Membrane Technique. Int. J. Oral Maxillofac Implant. 2020, 35, 379–385. [Google Scholar] [CrossRef]
- Gluckman, H.; Salama, M.; Du Toit, J. A retrospective evaluation of 128 socket-shield cases in the esthetic zone and posterior sites: Partial extraction therapy with up to 4 years follow-up. Clin. Implant Dent Relat. Res. 2018, 20, 122–129. [Google Scholar] [CrossRef]
- Salama, H.; Salama, M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: A systematic approach to the management of extraction site defects. Int. J. Periodontics Restor. Dent. 1993, 13, 312–333. [Google Scholar]
- Elian, N.; Cho, S.C.; Froum, S.; Smith, R.B.; Tarnow, D.P. A simplified socket classification and repair technique. Pract. Proced Aesthet Dent. 2007, 19, 99–104. [Google Scholar]
- De Jong, K.J.; Abraham-Inpijn, L. A risk-related patient-administered medical questionnaire for dental practice. Int. Dent. J. 1994, 44, 471–479. [Google Scholar]
- Blanco, J.; Carral, C.; Argibay, O.; Liñares, A. Implant placement in fresh extraction sockets. Periodontology 2000 2019, 79, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L.; Cicciù, M.; D’Amico, C.; Mauceri, R.; Oteri, G.; Cervino, G. Finite Element Method and Von Mises Investigation on Bone Response to Dynamic Stress with a Novel Conical Dental Implant Connection. BioMed Res. Int. 2020, 2020, 2976067. [Google Scholar] [CrossRef] [PubMed]
- Covani, U.; Cornelini, R.; Calvo-Guirado, J.L.; Tonelli, P.; Barone, A. Bone remodeling around implants placed in fresh extraction sockets. Int. J. Periodonticsrestorative Dent. 2010, 30, 601–607. [Google Scholar]
- Rojas-Vizcaya, F. Biological aspects as a rule for single implant placement. The 3A-2B rule: A clinical report. J. Prosthodont. 2013, 22, 575–580. [Google Scholar] [CrossRef]
- Canullo, L.; Fedele, G.R.; Iannello, G.; Jepsen, S. Platform switching and marginal bone-level alterations: The results of a randomized-controlled trial. Clin. Oral Implant. Res. 2010, 21, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Pesce, P.; Patini, R.; Antonacci, D.; Tommasato, G. What Are the Effect of Different Abutment Morphologies on Peri-implant Hard and Soft Tissue Behavior? A Systematic Review and Meta-Analysis. Int. J. Prosthodont. 2020, 33, 297–306. [Google Scholar] [CrossRef]
- Iasella, J.M.; Greenwell, H.; Miller, R.L.; Hill, M.; Drisko, C.; Bohra, A.A.; Scheetz, J.P. Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: A clinical and histologic study in humans. J. Periodontol. 2003, 74, 990–999. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, R.; Holtzclaw, D.; Rosen, P.S. A review on alveolar ridge preservation following tooth extraction. J. Evid. Based Dent. Pract. 2012, 12 (Suppl. 3), 149–160. [Google Scholar] [CrossRef]
- Castellon, P.; Casadaban, M.; Block, M.S. Techniques to facilitate provisionalization of implant restorations. J. Oral Maxillofac Surg. 2005, 63, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.K.; Rungcharassaeng, K.; Deflorian, M.; Weinstein, T.; Wang, H.L.; Testori, T. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontology 2000 2018, 77, 197–212. [Google Scholar] [CrossRef]
- Chung, S.; McCullagh, A.; Irinakis, T. Immediate loading in the maxillary arch: Evidence-based guidelines to improve success rates: A review. J. Oral Implant. 2011, 37, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Wittneben, J.G.; Buser, D.; Belser, U.C.; Brägger, U. Peri-implant soft tissue conditioning with provisional restorations in the esthetic zone: The dynamic compression technique. Int. J. Periodontics Restor. Dent. 2013, 33, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Furze, D.; Byrne, A.; Alam, S.; Wittneben, J.G. Esthetic Outcome of Implant Supported Crowns with and Without Peri-Implant Conditioning Using Provisional Fixed Prosthesis: A Random-ized Controlled Clinical Trial. Clin. Implant. Dent Relat. Res. 2016, 18, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Lyons, K.; Tawse-Smith, A.; Ma, S. Resonance Frequency Analysis in Assessing Implant Stability: A Retrospective Analysis. Int. J. Prosthodont. 2019, 32, 317–326. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implant. Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Donovan, T.E.; Chee, W.W. A review of contemporary impression materials and techniques. Dent. Clin. N. Am. 2004, 48, 445–470. [Google Scholar] [CrossRef]
- Terry, D.A.; Snow, S.R.; McLaren, E.A. Contemporary dental photography: Selection and application. Compend. Contin. Educ. Dent. 2008, 29, 440. [Google Scholar]
- Rösing, C.K.; Fiorini, T.; Haas, A.N.; Muniz, F.W.M.G.; Oppermann, R.V.; Susin, C. The impact of maintenance on peri-implant health. Braz. Oral Res. 2019, 33, e074. [Google Scholar] [CrossRef] [Green Version]
- Sheridan, R.A.; Decker, A.M.; Plonka, A.B.; Wang, H.L. The Role of Occlusion in Implant Therapy: A Comprehensive Updated Review. Implant Dent. 2016, 25, 829–838. [Google Scholar] [CrossRef]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Ballini, A.; Scacco, S.; Coletti, D.; Pluchino, S.; Tatullo, M. Mesenchymal Stem Cells as Promoters, Enhancers, and Playmakers of the Translational Regenerative Medicine. Stem Cells Int. 2017, 2017, 3292810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porcaro, G.; Busa, A.; Bianco, E.; Caccianiga, G.; Maddalone, M. Use of aPartial-thickness Flap for Guided Bone Regeneration in the Upper Jaw. J. Contemp. Dent. Pract. 2017, 18, 1117–1121. [Google Scholar] [PubMed]
- Lin, Z.; Fateh, A.; Salem, D.M.; Intini, G. Periosteum: Biology and applications in craniofacial bone regeneration. J. Dent. Res. 2014, 93, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lassere, B. The vertical mattress suture in periodontal flap surgery. Inf. Dent. 1983, 65, 3825–3830. [Google Scholar] [PubMed]
- Kumar, K.; Sharma, R.K.; Tewari, S.; Narula, S.C. Use of modified vertical internal mattress suture versus simple loop interrupted suture in modified Widman flap surgery: A randomized clinical study. Quintessence Int. 2019, 50, 732–740. [Google Scholar]
- Chu, S.J.; Salama, M.A.; Salama, H.; Garber, D.A.; Saito, H.; Sarnachiaro, G.O.; Tarnow, D.P. The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compend. Contin. Educ. Dent. 2012, 33, 524–534. [Google Scholar]
- Tan-Chu, J.H.; Tuminelli, F.J.; Kurtz, K.S.; Tarnow, D.P. Analysis of buccolingual dimensional changes of the extraction socket using the “ice cream cone” flapless grafting technique. Int. J. Periodontics Restor. Dent. 2014, 34, 399–403. [Google Scholar] [CrossRef]
- Atieh, M.A.; Alsabeeha, N.H.M. Soft tissue changes after connective tissue grafts around immediately placed and restored dental implants in the esthetic zone: A systematic review and meta-analysis. J. Esthet. Restor. Dent. 2020, 32, 280–290. [Google Scholar] [CrossRef]
- Grunder, U. Crestal ridge width changes when placing implants at the time of tooth extraction with and without soft tissue augmentation after a healing period of 6 months: Report of 24 consecutive cases. Int. J. Periodontics Restor. Dent. 2011, 31, 9–17. [Google Scholar]
- Zucchelli, G.; Tavelli, L.; McGuire, M.K.; Rasperini, G.; Feinberg, S.E.; Wang, H.L.; Giannobile, W.V. Autogenous soft tissue grafting for periodontal and peri-implant plastic surgical reconstruction. J. Periodontol. 2020, 91, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, H.; Du Toit, J.; Pontes, C.C.; Hille, J. Hyperplastic Response Following Soft Tissue Augmentation in the Esthetic Zone. Clin. Adv. Periodontics 2019, 9, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Tettamanti, L.; Andrisani, C.; Bassi, M.A.; Vinci, R.; Silvestre-Rangil, J.; Tagliabue, A. Immediate loading implants: Review of the critical aspects. Oral Implant. 2017, 10, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Saadoun, A.P.; LeGall, M.; Touati, B. Selection and ideal tridimensional implant position for soft tissue aesthetics. Pract Periodontics Aesthet Dent. 1999, 11, 1063–1072. [Google Scholar] [PubMed]
- de Siqueira, R.A.C.; Cabral, B.L.; de Siqueira, G.R.; Mendonça, G.; Wang, H.L. Using Digital Technique to Obtain the Ideal Soft Tissue Contour in Immediate Implants with Provisionalization. Implant Dent. 2019, 28, 411–416. [Google Scholar] [CrossRef]
- Lee, C.T.; Sanz-Miralles, E.; Zhu, L.; Glick, J.; Heath, A.; Stoupel, J. Predicting bone and soft tissue alterations of immediate implant sites in the esthetic zone using clinical parameters. Clin. Implant Dent. Relat. Res. 2020, 22, 325–332. [Google Scholar] [CrossRef]
- Vela, X.; Rodríguez, X. The State of the Art of the Implant-Abutment Design to Maximize the Peri-Implant Tissue Potential. In Implants in the Aesthetic Zone; Schoenbaum, T., Ed.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- González-Martín, O.; Lee, E.; Weisgold, A.; Veltri, M.; Su, H. Contour Management of Implant Restorations for Optimal Emergence Profiles: Guidelines for Immediate andDelayed Provisional Restorations. Int. J. Periodontics Restor. Dent. 2020, 40, 61–70. [Google Scholar] [CrossRef]
- López-López, P.J.; Mareque-Bueno, J.; Boquete-Castro, A.; Raya, A.A.-S.; Martínez-González, J.M.; Calvo-Guirado, J.L. The effects of healing abutments of different size and anatomic shape placed immediately in extraction sockets on peri-implant hard and soft tissues. A pilot study in foxhound dogs. Clin. Oralimplants Res. 2016, 27, 90–96. [Google Scholar] [CrossRef]
- Vergoullis, I.; DDS, M.S.; Valavanis, K.D.D.S.; Badell, C.D.D.S.; Papadopoulos, G.C.D.T. The one functional position, implant level, indirect impression technique: Description of the technique and a case report. JIACD 2019, 11, 14–23. [Google Scholar]
- Wittneben, J.G.; Millen, C.; Brägger, U. Clinical performance of screw- versus cement-retained fixed implant-supported reconstructions--a systematic review. Int. J. Oral Maxillofac Implant. 2014, 29, 84–98. [Google Scholar] [CrossRef] [Green Version]
- Linkevicius, T.; Vindasiute, E.; Puisys, A.; Linkeviciene, L.; Maslova, N.; Puriene, A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin. Oral Implant. Res. 2013, 24, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Helvey, G.A. A Simple Technique for Fabricating a Screw-Retained/Cemented Implant-Supported Crown. Compend. Contin. Educ. Dent. 2017, 38, 153–159. [Google Scholar] [PubMed]
- Cantore, S.; Ballini, A.; Mori, G.; Dibello, V.; Marrelli, M.; Mirgaldi, R.; De Vito, D.; Tatullo, M. Anti-plaque and antimicrobial efficiency of different oral rinses in a 3-day plaque accumulation model. J. Biol. Regul. Homeost Agents. 2016, 30, 1173–1178. [Google Scholar] [PubMed]
- Sicilia-Felechosa, A.; Pereira-Fernández, A.; García-Lareu, J.; Bernardo-González, J.; Sicilia-Blanco, P.; Cuesta-Fernández, I. Flapless immediate implant placement and provisionalization in periodontal patients: A retrospective consecutive case-series study of single-tooth sites with dehiscence-type osseous defects. Clin. Oral Implant. Res. 2020, 31, 229–238. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontol 2000 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Salama, H.; Salama, M.A.; Garber, D.; Adar, P. The interproximal height of bone: A guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pract. Periodontics Aesthet Dent. 1998, 10, 1131–1141. [Google Scholar]
- Chu, S.J.; Sarnachiaro, G.O.; Hochman, M.N.; Tarnow, D.P. Subclassification and Clinical Management of Extraction Sockets with Labial Dentoalveolar Dehiscence Defects. Compend. Contin. Educ. Dent. 2015, 36, 518–520. [Google Scholar]
- El Chaar, E.; Oshman, S.; Fallah Abed, P. Single-Rooted Extraction Sockets: Classification and Treatment Protocol. Compend. Contin. Educ. Dent. 2016, 37, 537–541. [Google Scholar]

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Salama H, Salama M [18] | CLASS I | CLASS II | CLASS III |
|---|---|---|---|
| MMC | + | + | − |
| Chu SJ et al. [68] | TYPE A | TYPE B | TYPE C |
| MMC | + | + | + (If recession defect is class I Miller) |
| Ellian N et al. [19]. | TYPE I | TYPE II | TYPE III |
| MMC | + | + | + (If recession defect is class I Miller) |
| El Chaar E et al. [69] | GRADE I | GRADE II | GRADE III |
| MMC | + | + | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valavanis, K.; Vergoullis, I.; Papastamos, M.; Salama, H. Immediate Implant Placement and Provisionalization in the Esthetic Zone Revisited: The Marginal Migration Concept (MMC). Appl. Sci. 2020, 10, 8944. https://doi.org/10.3390/app10248944
Valavanis K, Vergoullis I, Papastamos M, Salama H. Immediate Implant Placement and Provisionalization in the Esthetic Zone Revisited: The Marginal Migration Concept (MMC). Applied Sciences. 2020; 10(24):8944. https://doi.org/10.3390/app10248944
Chicago/Turabian StyleValavanis, Konstantinos, Ioannis Vergoullis, Michalis Papastamos, and Henry Salama. 2020. "Immediate Implant Placement and Provisionalization in the Esthetic Zone Revisited: The Marginal Migration Concept (MMC)" Applied Sciences 10, no. 24: 8944. https://doi.org/10.3390/app10248944
APA StyleValavanis, K., Vergoullis, I., Papastamos, M., & Salama, H. (2020). Immediate Implant Placement and Provisionalization in the Esthetic Zone Revisited: The Marginal Migration Concept (MMC). Applied Sciences, 10(24), 8944. https://doi.org/10.3390/app10248944