Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes



Abstract
:1. Introduction
- Environmental factors: air temperature, mean radiant temperature, relative air humidity, air movement (air velocity);
- Factors related to the state of the human body: thermoregulation mechanism, central nervous system, cardiovascular system, respiratory system, skeletal-muscular system, digestive system;
- Factors related to clothing/textiles as a barrier between the body and the environment: insulating ability (resistance to heat transfer), air permeability, water vapour permeability, water repellency, drying rate.
2. Methodology: Computational Data
2.1. Environmental Factors
2.2. Factors Related to Human Body Status
2.3. Factors Related to Clothing
- 0.96 clo: surgical polyester ensemble with coal fibrеs and multiple-use barrier surgical polyester gown with carbon fibres and liquid proof fabric of higher resistance on sleeves and front;
- 1.01 clo: surgical polyester ensemble with coal fibres and multiple-use polyester surgical gown with polytetrafluorethylene protective sleeves and front and carbon fibres on the back;
- 1.05 clo: surgical polyester ensemble with coal fibres and single-use cotton surgical gown.
3. Results and Discussion
3.1. Thermophysiological Comfort of the Patient
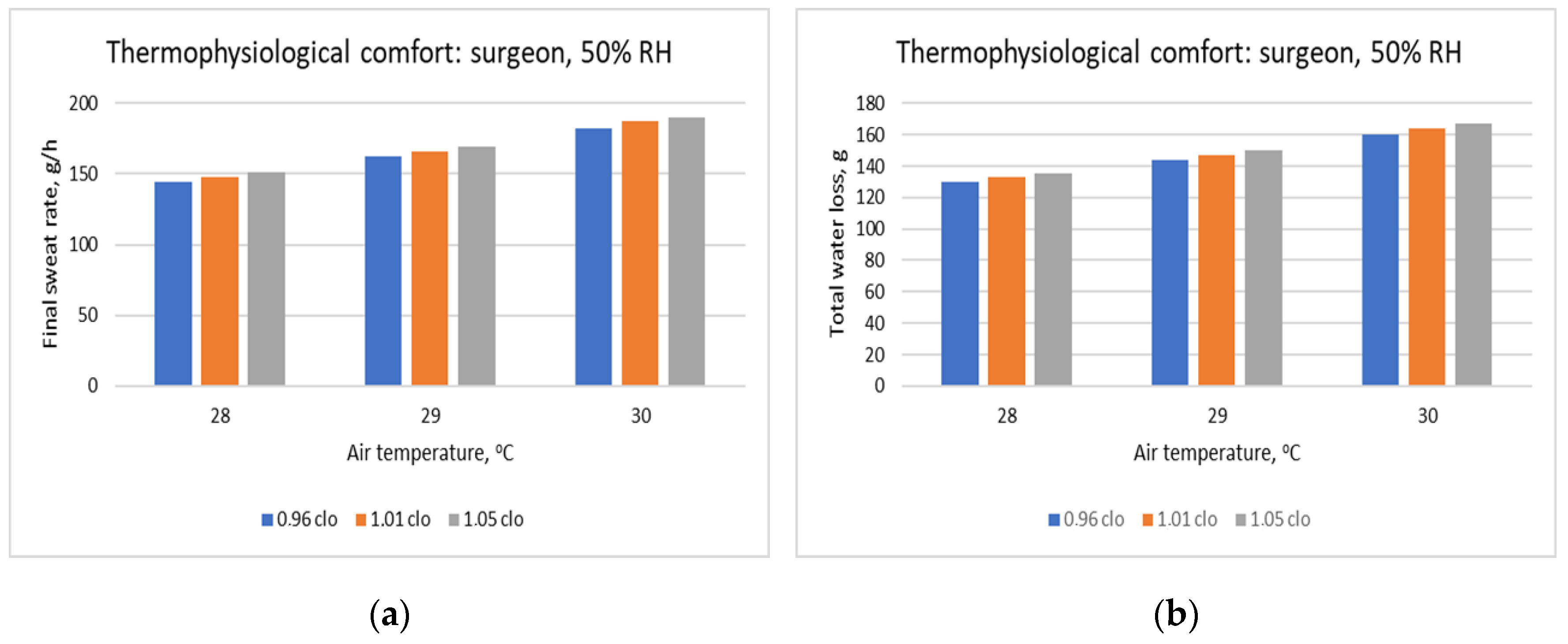
3.2. Thermophysiological Comfort of the Surgeon
- For clothing ensemble with 0.96 clo: from 18 °C, 30% RH (PMV = −0.48) to 23 °C, 40% RH (PMV = +0.48).
- For clothing ensemble with 1.01 clo: from 17 °C, 60% RH (PMV = −0.49) to 23 °C, 30% RH (PMV = +0.47).
- For clothing ensemble with 1.05 clo: from 17 °C, 40% RH (PMV = −0.49) to 22 °C, 60% RH (PMV = +0.49).
3.3. The Thermophysiological Comfort of the Patient vs. the Thermophysiological Comfort of the Surgeon
3.4. Research Strengths and Limitations
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Uścinowicz, P.; Chludzińska, M.; Bogdan, A. Thermal environment conditions in Polish operating rooms. Build. Environ. 2015, 94, 296–304. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 7730: Moderate Thermal Environments-Determination of the PMV and PPD Indices and Specification of the Conditions for Thermal Comfort; ISO: Geneva, Switzerland, 2005. [Google Scholar]
- Angelova, R.A. Textiles and Human Thermophysiological Comfort in the Indoor Environment; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Khodakarami, J.; Nasrollahi, N. Thermal comfort in hospitals–A literature review. Renew. Sustain. Energy Rev. 2012, 16, 4071–4077. [Google Scholar] [CrossRef]
- Van Gaever, R.; Jacobs, V.A.; Diltoer, M.; Peeters, L.; Vanlanduit, S. Thermal comfort of the surgical staff in the operating room. Build. Environ. 2014, 81, 37–41. [Google Scholar] [CrossRef]
- Chow, T.T.; Kwan, A.; Lin, Z.; Bai, W. Conversion of operating theatre from positive to negative pressure environment. J. Hosp. Infect. 2006, 64, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Patania, F.; Gagliano, A.; Nocera, F.; Galesi, A. Thermal comfort in operating rooms: A case study. WIT Trans. Biomed. Health 2011, 15, 105–114. [Google Scholar]
- Sadrizadeh, S.; Loomans, M.G.L.C. Thermal comfort in hospital and healthcare facilities: A literature review. In Proceedings of the 9th International Conference on Indoor Air Quality Ventilation & Energy Conservation in Buildings, Seoul, Korea, 23–26 October 2016; pp. 1–12. [Google Scholar]
- Zwolińska, M.; Bogdan, A. Thermal sensations of surgeons during work in surgical gowns. Int. J. Occup. Saf. Ergon. 2013, 19, 443–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balaras, C.A.; Dascalaki, E.; Gaglia, A. HVAC and indoor thermal conditions in hospital operating rooms. Energy Build. 2007, 39, 454–470. [Google Scholar] [CrossRef]
- Fanger, P.O. Thermal Comfort Analysis and Applications in Environmental Engineering; McGraw-Hill: New York, NY, USA, 1972. [Google Scholar]
- Moran, D.S.; Pandolf, K.B.; Shapiro, Y.; Heled, Y.; Shani, Y.; Mathew, W.T.; Gonzalez, R.R. An environmental stress index (ESI) as a substitute for the wet bulb globe temperature (WBGT). J. Therm. Biol. 2001, 26, 427–431. [Google Scholar] [CrossRef]
- D’Ambrosio Alfano, F.R.; Malchaire, J.; Palella, B.I.; Riccio, G. WBGT index revisited after 60 years of use. Ann. Occup. Hyg. 2014, 58, 955–970. [Google Scholar] [PubMed] [Green Version]
- Yaglou, C.P. Temperature, humidity, and air movement in industries: The effective temperature index. J. Ind. Hyg. 1927, 9, 297–309. [Google Scholar]
- Taleghani, M.; Tenpierik, M.; Kurvers, S.; Van Den Dobbelsteen, A. A review into thermal comfort in buildings. Renew. Sustain. Energy Rev. 2013, 26, 201–215. [Google Scholar] [CrossRef]
- Epstein, Y.; Moran, D.S. Thermal comfort and the heat stress indices. Ind. Health 2006, 44, 388–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atthajariyakul, S.; Leephakpreeda, T. Real-time determination of optimal indoor-air condition for thermal comfort, air quality and efficient energy usage. Energy Build. 2004, 36, 720–733. [Google Scholar] [CrossRef]
- Homod, R.Z.; Sahari, K.S.M.; Almurib, H.A.; Nagi, F.H. RLF and TS fuzzy model identification of indoor thermal comfort based on PMV/PPD. Build. Environ. 2012, 49, 141–153. [Google Scholar] [CrossRef]
- ISO. Ergonomics of the Thermal Environment-Analytical Determination and Interpretation of Heat Stress Using Calculation of the Predicted Heat Strain; International Standardisation Organisation: Geneva, Germany, 2004. [Google Scholar]
- Malchaire, J.B. Evaluation of natural wet bulb and wet globe thermometers. The Annals of occupational hygiene 1976, 19, 251–258. [Google Scholar]
- ASHRAE Standard 170-2013. Ventilation of Health Care Facilities; ASHRAE: Atlanta, GA, USA, 2013.
- Konarska, M.; Soltynski, K.; Sudol-Szo-pinska, I.; Chojnacka, A. Comparative evaluation of clothing thermal insulation measured on a thermal manikin and on volunteers. Fibres Text. East. Eur. 2007, 15, 79–85. [Google Scholar]
- Bogdan, A.; Sudoł-Szopińska, I.; Szopiński, T. Assessment of textiles for use in operating theatres with respect to the thermal comfort of surgeons. Fibres Text. East. Eur. 2011, 19, 65–69. [Google Scholar]
- ISO. 15265:2004 Ergonomics of the Thermal Environment-Risk Assessment Strategy for the Prevention of Stress or Discomfort in Thermal Working Conditions; ISO: Geneva, Switzerland, 2004. [Google Scholar]
- Sessler, D.I. Mild perioperative hypothermia. New Engl. J. Med. 1997, 336, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Mascha, E.; Na, J.; Sessler, D.I. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiol. J. Am. Soc. Anesthesiol. 2008, 108, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, M.; Ford, J.; Harper, M. Peri-Operative warming devices: Performance and clinical application. Anaesthesia 2014, 69, 623–638. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clothing Insulation | Temperature | Humidity | Metabolism |
|---|---|---|---|
| 0.15 clo | 23–32 °C | 30–60% | 40 W/m2 |
| 0.96 clo | 16–30 °C | 30–60% | 145 W/m2 |
| 1.01 clo | 16–30 °C | 30–60% | 145 W/m2 |
| 1.05 clo | 16–30 °C | 30–60% | 145 W/m2 |
| Value | Thermal Sense |
|---|---|
| −3 | cold |
| −2 | cool |
| −1 | slightly cool |
| 0 | neutral |
| +1 | slightly warm |
| +2 | warm |
| +3 | hot |
| Category | Comfort Related to the Climatic Conditions |
|---|---|
| 3 | Severe discomfort without health risk |
| 4 | Slight cold discomfort without health risk |
| 5 | Comfort, no health risk |
| 6 | Slight warm discomfort without health risk |
| 7 | Severe warm discomfort without health risk |
| 8 | Long-term constraint: discomfort and dehydration after several hours of exposure |
| 9 | Short-term constraint: health risk after 30–120 min of exposure |
| 10 | Immediate constraint: health risk even for exposures of very short duration (less than 30 min) several hours of exposure |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelova, R.A.; Velichkova, R. Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes. Appl. Sci. 2020, 10, 1801. https://doi.org/10.3390/app10051801
Angelova RA, Velichkova R. Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes. Applied Sciences. 2020; 10(5):1801. https://doi.org/10.3390/app10051801
Chicago/Turabian StyleAngelova, Radostina A., and Rositsa Velichkova. 2020. "Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes" Applied Sciences 10, no. 5: 1801. https://doi.org/10.3390/app10051801
APA StyleAngelova, R. A., & Velichkova, R. (2020). Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes. Applied Sciences, 10(5), 1801. https://doi.org/10.3390/app10051801