Photoplethysmographic Prediction of the Ankle-Brachial Pressure Index through a Machine Learning Approach

 ,
,  ,
,  ,
,  , ,
, ,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
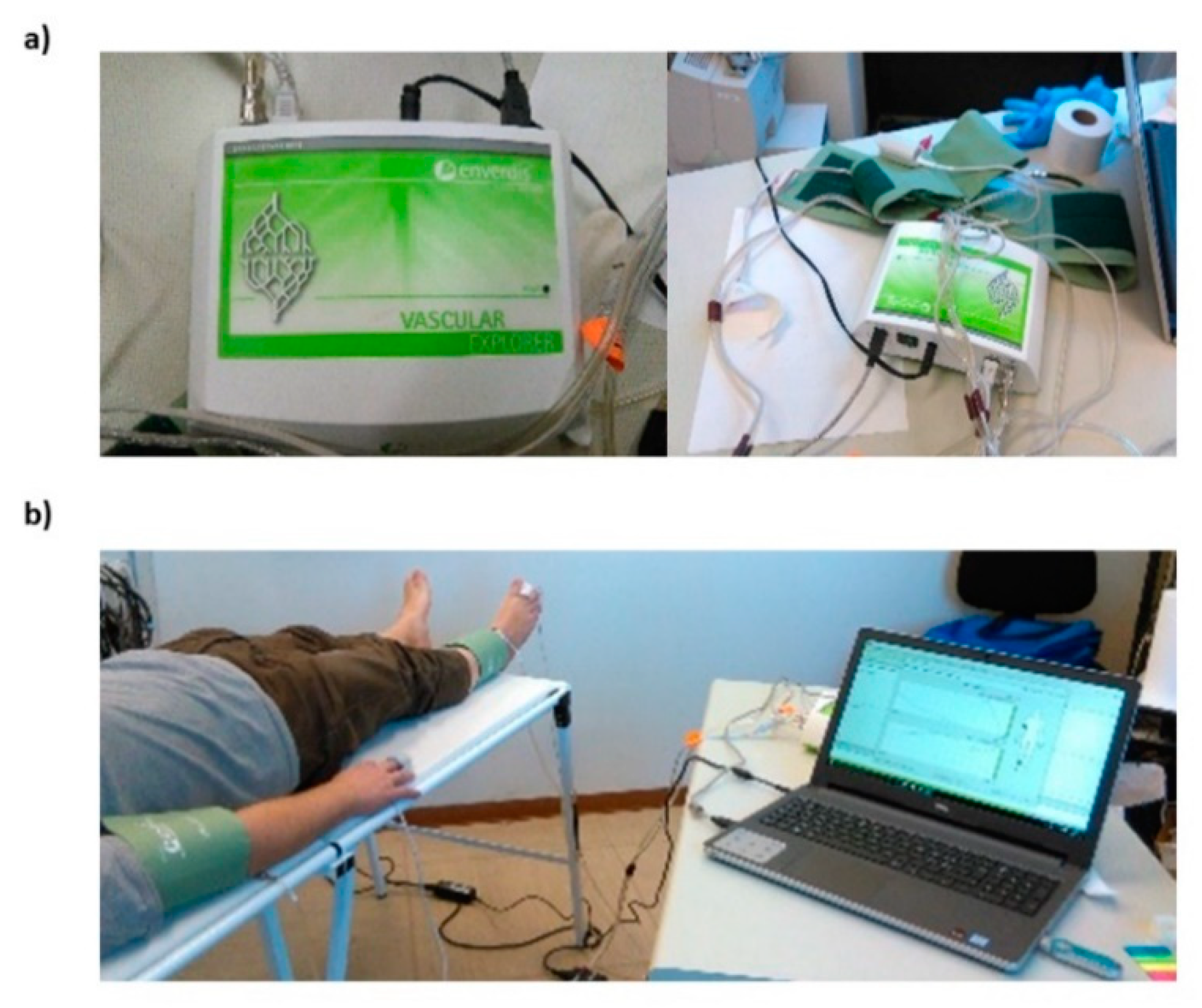
2.2. Vascular Explorer ABI Measurements
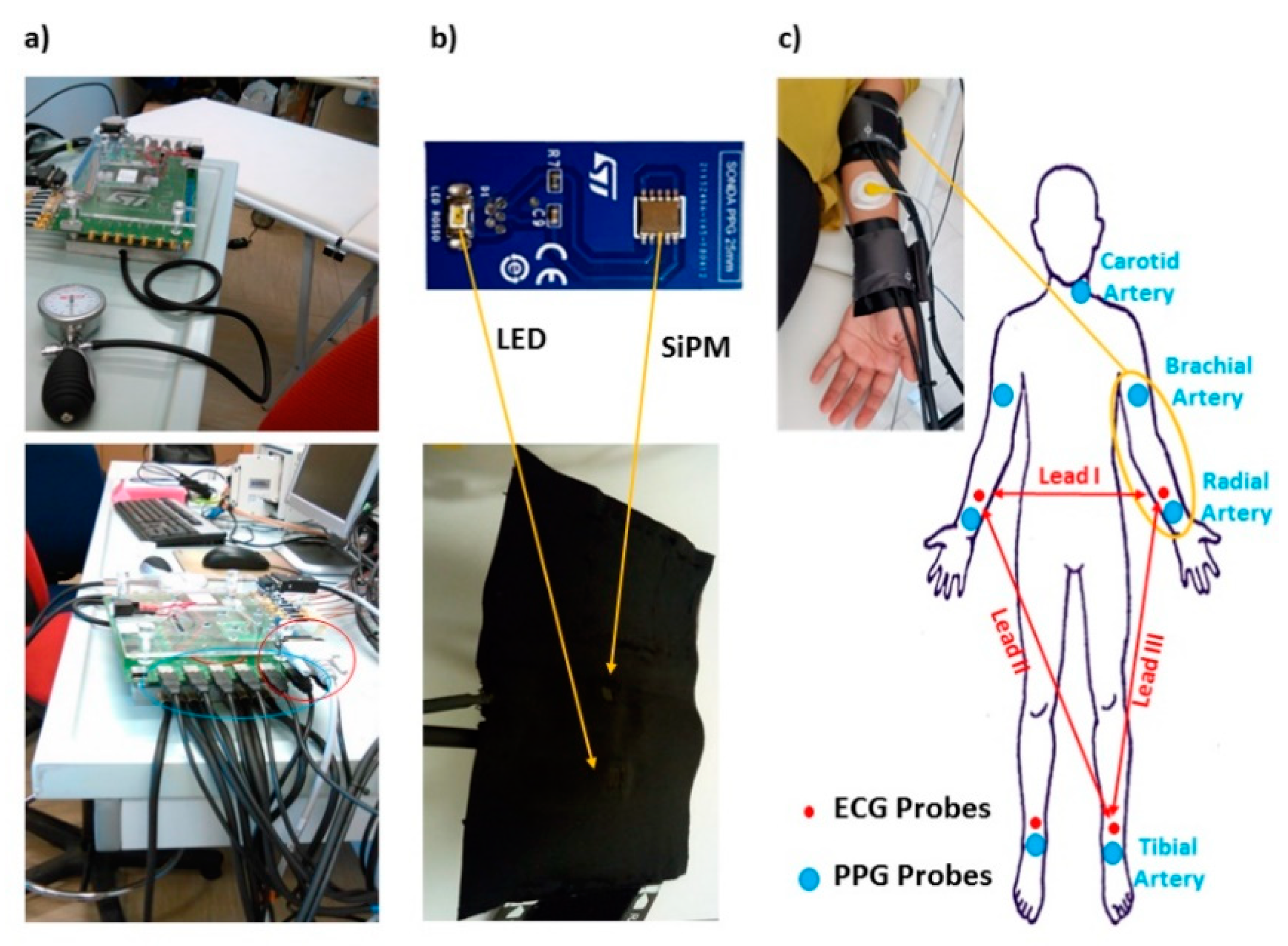
2.3. Photoplethysmographic (PPG) and Electrocardiographic (ECG) Recordings
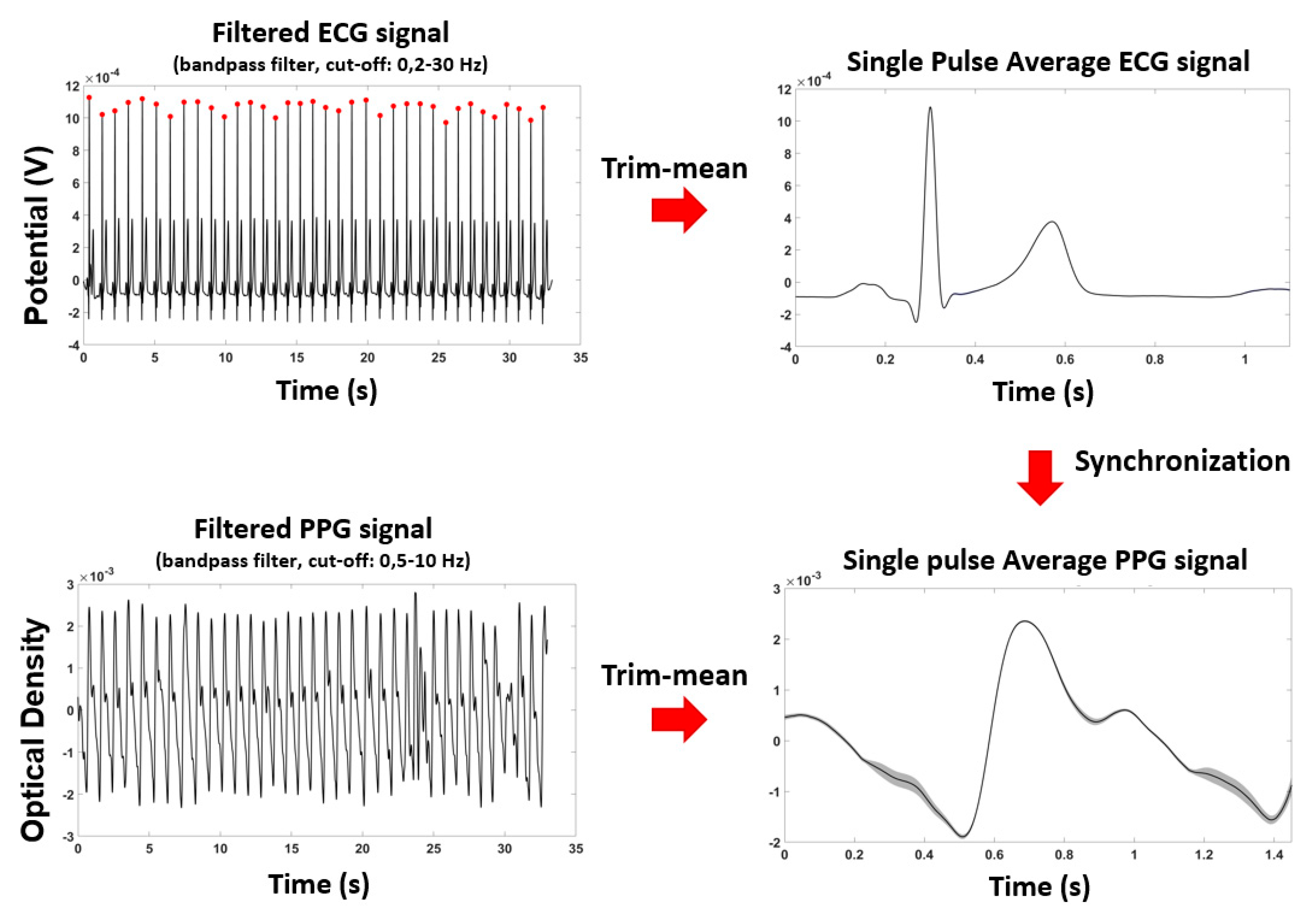
2.4. Photoplethysmographic (PPG) and Electrocardiographic (ECG) Signals Pre-Processing
2.5. Ankle-Brachial Index (ABI) Prediction by Means of Machine Learning (General Linear Model, GLM)
- Y = n × 1 column vector representing the dependent variable (e.g., VE-ABI)
- X = n × p design matrix where each column represents an independent variable of length n (e.g., PPG features);
- β = p × 1 column vector of weights of each predictor, indicating the strength of the association with Y;
- ε = n × 1 column vector of the residual error
- Maximum amplitude of the PPG ODs evaluated at brachial and tibial arteries (2 features, labelled MaxArm and MaxAnkle);
- Diastole to systole slope of the PPG signal at brachial and tibial arteries (2 features, labelled SlopeArm and SlopeAnkle) evaluated as:
- Time delay of the diastolic foot of PPG with respect to ECG R-peak at brachial and tibial arteries (2 features, labelled TDArm and TDAnkle);
- Ratio of an estimate of the systolic blood pressure at the ankle and at the brachial artery derived from PPG signals according to [42] (1 feature, labelled Ankle-Arm), evaluated as:
2.6. Statistical Analysis
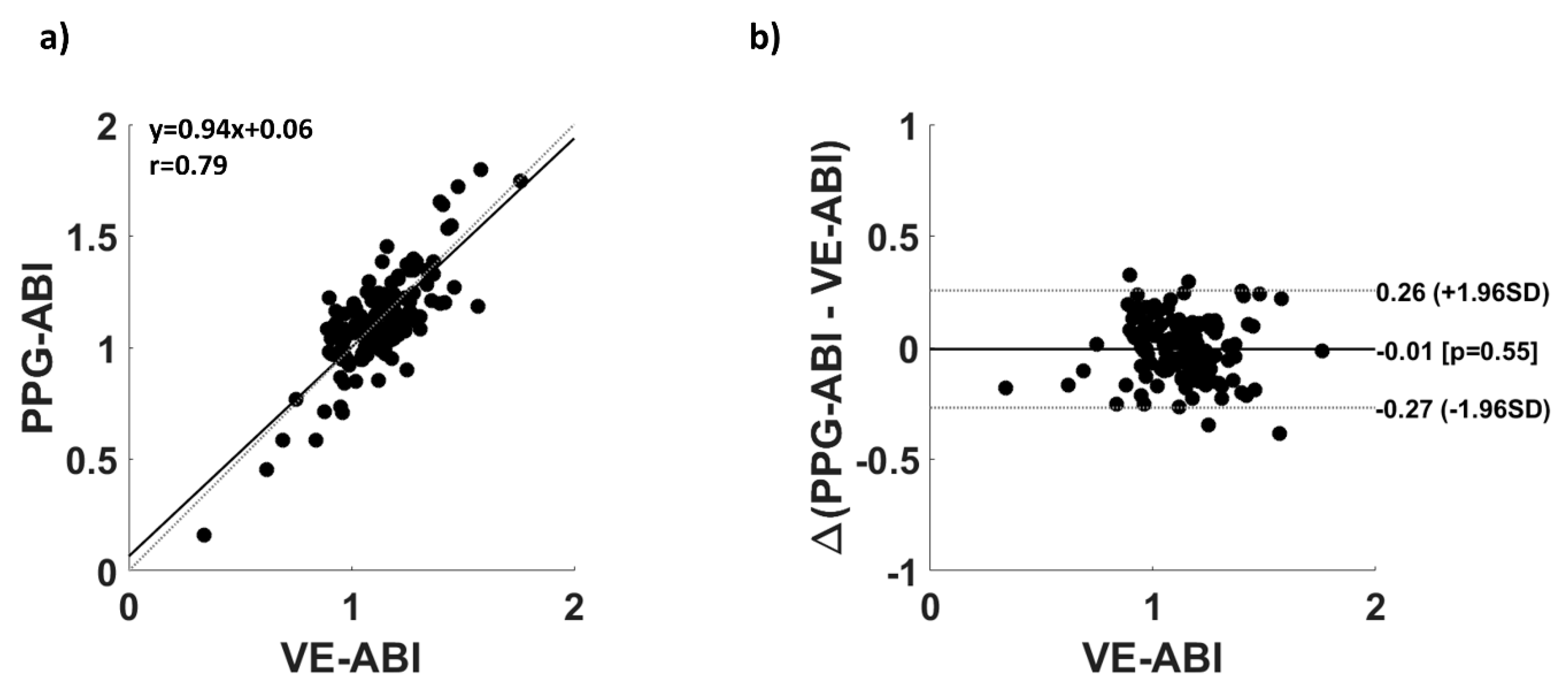
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Heald, C.L.; Fowkes, F.G.R.; Murray, G.D.; Price, J.F. Risk of mortality and cardiovascular disease associated with the ankle-brachial index: Systematic review. Atherosclerosis 2006, 189, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Breen, P.P.; Jayarathna, T.; Gargiulo, G.D. Live Demonstration: Morphic Sensor for Diagnosis of Peripheral Vascular Disease. In Proceedings of the 2019 IEEE Biomedical Circuits and Systems Conference (BioCAS), Nara, Japan, 17–19 October 2019. [Google Scholar]
- Zheng, Z.-J.; Sharrett, A.R.; Chambless, L.E.; Rosamond, W.D.; Nieto, F.J.; Sheps, D.S.; Dobs, A.; Evans, G.W.; Heiss, G. Associations of ankle-brachial index with clinical coronary heart disease, stroke and preclinical carotid and popliteal atherosclerosis:: The Atherosclerosis Risk in Communities (ARIC) Study. Atherosclerosis 1997, 131, 115–125. [Google Scholar] [CrossRef]
- Winsor, T. Influence of arterial disease on the systolic blood pressure gradients of the extremity. Am. J. Med. Sci. 1950, 220, 117–126. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Liu, K.; Greenland, P.; Guralnik, J.M.; Criqui, M.H.; Chan, C.; Pearce, W.H.; Schneider, J.R.; Ferrucci, L.; Celic, L. Functional decline in peripheral arterial disease: Associations with the ankle brachial index and leg symptoms. JAMA 2004, 292, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raman, P.G.; Thakur, B.S.; Mathew, V. Ankle brachial index as a predictor of generalized atherosclerosis. J. Assoc. Phys. India 2001, 49, 1074–1077. [Google Scholar]
- Resnick Helaine, E.; Lindsay Robert, S.; McDermott Mary, M.; Devereux Richard, B.; Jones Kristina, L.; Fabsitz Richard, R.; Howard Barbara, V. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality. Circulation 2004, 109, 733–739. [Google Scholar] [CrossRef] [Green Version]
- Victor, A.; Criqui Michael, H.; Pierre, A.; Allison Matthew, A.; Creager Mark, A.; Diehm, C.; Fowkes, F.; Gerry, R.; Hiatt William, R.; Björn, J.; et al. Measurement and interpretation of the ankle-brachial index. Circulation 2012, 126, 2890–2909. [Google Scholar]
- MacDougall, A.M.; Tandon, V.; Rn, M.P.W.; Wilson, T.W. Oscillometric measurement of the ankle-brachial index. Can. J. Cardiol. 2008, 24, 49–51. [Google Scholar] [CrossRef] [Green Version]
- Beckman, J.A.; Higgins, C.O.; Gerhard-Herman, M. Automated oscillometric determination of the ankle–brachial index provides accuracy necessary for office practice. Hypertension 2006, 47, 35–38. [Google Scholar] [CrossRef]
- Ramanathan, A.; Conaghan, P.J.; Jenkinson, A.D.; Bishop, C.R. Comparison of ankle-brachial pressure index measurements using an automated oscillometric device with the standard doppler ultrasound technique. ANZ J. Surg. 2003, 73, 105–108. [Google Scholar] [CrossRef]
- Herráiz-Adillo, Á.; Martínez-Vizcaíno, V.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Garrido-Miguel, M.; Notario-Pacheco, B. Diagnostic accuracy study of an oscillometric ankle-brachial index in peripheral arterial disease: The influence of oscillometric errors and calcified legs. PLoS ONE 2016, 11, e0167408. [Google Scholar] [CrossRef]
- Kario, K.; Thijs, L.; Staessen, J.A. Blood pressure measurement and treatment decisions: Masked and white-coat hypertension. Circul. Res. 2019, 124, 990–1008. [Google Scholar] [CrossRef]
- Challoner, A.V.J. Photoelectric plethysmography for estimating cutaneous blood flow. Non Invasive Physiol. Meas. 1979, 1, 125–151. [Google Scholar]
- Georgieva-Tsaneva, G.; Gospodinova, E.; Gospodinov, M.; Cheshmedzhiev, K. Portable sensor system for registration, processing and mathematical analysis of ppg signals. Appl. Sci. 2020, 10, 1051. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.-H.; Wang, J.-J.; Chen, W.; Pan, K.-L.; Su, C.-H. Classification of photoplethysmographic signal quality with fuzzy neural network for improvement of stroke volume measurement. Appl. Sci. 2020, 10, 1476. [Google Scholar] [CrossRef] [Green Version]
- Rusch, T.L.; Sankar, R.; Scharf, J.E. Signal processing methods for pulse oximetry. Comput. Biol. Med. 1996, 26, 143–159. [Google Scholar] [CrossRef]
- Gratton, E.; Fantini, S.; Franceschini, M.A.; Gratton, G.; Fabiani, M. Measurements of scattering and absorption changes in muscle and brain. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 1997, 352, 727–735. [Google Scholar] [CrossRef]
- Croce, P.; Zappasodi, F.; Merla, A.; Chiarelli, A.M. Exploiting neurovascular coupling: A Bayesian sequential Monte Carlo approach applied to simulated EEG fNIRS data. J. Neural Eng. 2017, 14, 046029. [Google Scholar] [CrossRef]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Song, Z.; Yimin, Y. Study of pulse wave velocity noninvasive detecting instrument based on radial artery and finger photoplethysmography pulse wave. In Proceedings of the 2008 International Symposium on Intelligent Information Technology Application Workshops, Shanghai, China, 21–22 December 2008; pp. 705–708. [Google Scholar]
- Huotari, M.; Vehkaoja, A.; Määttä, K.; Kostamovaara, J. Photoplethysmography and its detailed pulse waveform analysis for arterial stiffness. J. Struct. Mech. 2011, 44, 345–362. [Google Scholar]
- Otsuka, T.; Kawada, T.; Katsumata, M.; Ibuki, C.; Kusama, Y. Independent determinants of second derivative of the finger photoplethysmogram among various cardiovascular risk factors in middle-aged men. Hypertens. Res. 2007, 30, 1211. [Google Scholar] [CrossRef] [Green Version]
- Pilt, K.; Meigas, K.; Ferenets, R.; Temitski, K.; Viigimaa, M. Photoplethysmographic signal waveform index for detection of increased arterial stiffness. Physiol. Meas. 2014, 35, 2027. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, R.; Manzo, A.; Delgado, J.; Padilla, J.M.; Trénor, B.; Saiz, J. A computer based photoplethysmographic vascular analyzer through derivatives. In Proceedings of the 2008 Computers in Cardiology, Bologna, Italy, 14–17 September 2008; pp. 177–180. [Google Scholar]
- Chiarelli, A.M.; Bianco, F.; Perpetuini, D.; Bucciarelli, V.; Filippini, C.; Cardone, D.; Zappasodi, F.; Gallina, S.; Merla, A. Data-driven assessment of cardiovascular ageing through multisite photoplethysmography and electrocardiography. Med. Eng. Phys. 2019, 73, 39–50. [Google Scholar] [CrossRef]
- Mcauliffe, J.D.; Blei, D.M. Supervised topic models. In Proceedings of the Advances in Neural Information Processing Systems, Montreal, Canada, 3–8 December 2008; pp. 121–128. [Google Scholar]
- Monti, M.M. Statistical analysis of fMRI time-series: A critical review of the GLM approach. Front. Hum. Neurosci. 2011, 5, 28. [Google Scholar] [CrossRef] [Green Version]
- Perpetuini, D.; Cardone, D.; Filippini, C.; Chiarelli, A.M.; Merla, A. Modelling impulse response function of functional infrared imaging for general linear model analysis of autonomic activity. Sensors 2019, 19, 849. [Google Scholar] [CrossRef] [Green Version]
- Chiarelli, A.M.; Romani, G.L.; Merla, A. Fast optical signals in the sensorimotor cortex: General Linear Convolution Model applied to multiple source–detector distance-based data. NeuroImage 2014, 85, 245–254. [Google Scholar] [CrossRef]
- Betge, S.; Kretzschmar, D.; Figulla, H.-R.; Lichtenauer, M.; Jung, C. Predictive value of the augmentation index derived vascular age in patients with newly diagnosed atherosclerosis. Heart Vessel. 2017, 32, 252–259. [Google Scholar] [CrossRef] [Green Version]
- McEniery, C.M.; Hall, I.R.; Qasem, A.; Wilkinson, I.B.; Cockcroft, J.R.; Investigators, A. Normal vascular aging: Differential effects on wave reflection and aortic pulse wave velocity: The Anglo-Cardiff Collaborative Trial (ACCT). J. Am. Coll. Cardiol. 2005, 46, 1753–1760. [Google Scholar] [CrossRef] [Green Version]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef]
- Vinciguerra, V.; Ambra, E.; Maddiona, L.; Romeo, M.; Mazzillo, M.; Rundo, F.; Fallica, G.; di Pompeo, F.; Chiarelli, A.M.; Zappasodi, F. PPG/ECG Multisite Combo System Based on SiPM Technology. In Convegno Nazionale Sensori; Springer: Catania, Italy, 2018; pp. 353–360. [Google Scholar]
- Perpetuini, D.; Chiarelli, A.M.; Maddiona, L.; Rinella, S.; Bianco, F.; Bucciarelli, V.; Gallina, S.; Perciavalle, V.; Vinciguerra, V.; Merla, A. Multi-Site Photoplethysmographic and Electrocardiographic System for Arterial Stiffness and Cardiovascular Status Assessment. Sensors 2019, 19, 5570. [Google Scholar] [CrossRef] [Green Version]
- Perpetuini, D.; Chiarelli, A.M.; Vinciguerra, V.; Vitulli, P.; Rinella, S.; Cardone, D.; Bianco, F.; Perciavalle, V.; Gallina, S.; Fallica, G. Integrated multi-channel PPG and ECG system for cardiovascular risk assessment. Proceedings 2019, 27, 8. [Google Scholar] [CrossRef] [Green Version]
- Chiarelli, A.M.; Libertino, S.; Zappasodi, F.; Mazzillo, M.C.; Di Pompeo, F.; Merla, A.; Lombardo, S.A.; Fallica, G.P. Characterization of a fiber-less, multichannel optical probe for continuous wave functional near-infrared spectroscopy based on silicon photomultipliers detectors: In-vivo assessment of primary sensorimotor response. Neurophotonics 2017, 4, 035002. [Google Scholar] [CrossRef] [Green Version]
- Vinciguerra, V.; Ambra, E.; Maddiona, L.; Oliveri, S.; Romeo, M.F.; Mazzillo, M.; Rundo, F.; Fallica, G. Progresses towards a processing pipeline in photoplethysmogram (PPG) based on SiPMs. In Proceedings of the 2017 European Conference on Circuit Theory and Design (ECCTD), Catania, Italy, 4–6 September 2017; pp. 1–5. [Google Scholar]
- Moeinzadeh, H.; Assad, J.; Bifulco, P.; Cesarelli, M.; O’Loughlin, A.; Shugman, I.M.; Gargiulo, G.D. Einthoven Unipolar Leads: Towards a better understanding of Wilson Central Terminal. In Proceedings of the 2019 International Conference on Electrical Engineering Research & Practice (ICEERP), Sydney, Australia, 24–28 November 2019; pp. 1–4. [Google Scholar]
- Chiarelli, A.M.; Maclin, E.L.; Low, K.A.; Mathewson, K.E.; Fabiani, M.; Gratton, G. Combining energy and Laplacian regularization to accurately retrieve the depth of brain activity of diffuse optical tomographic data. J. Biomed. Opt. 2016, 21, 36008. [Google Scholar] [CrossRef] [Green Version]
- Schultz-Ehrenburg, U.; Blazek, V. Value of quantitative photoplethysmography for functional vascular diagnostics. Skin Pharmacol. Physiol. 2001, 14, 316–323. [Google Scholar] [CrossRef]
- Lazazzera, R.; Belhaj, Y.; Carrault, G. A new wearable device for blood pressure estimation using photoplethysmogram. Sensors 2019, 19, 2557. [Google Scholar] [CrossRef] [Green Version]
- Vehtari, A.; Gelman, A.; Gabry, J. Practical Bayesian model evaluation using leave-one-out cross-validation and WAIC. Stat. Comput. 2017, 27, 1413–1432. [Google Scholar] [CrossRef] [Green Version]
- Hsu, H.; Lachenbruch, P.A. Paired t test. In Wiley Encyclopedia of Clinical Trials; Wiley: Hobeken, NJ, USA, 2007; pp. 1–3. [Google Scholar]
- Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Psychology Press: East Sussex, UK, 2014; ISBN 1-135-46825-7. [Google Scholar]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Dewitte, K.; Fierens, C.; Stöckl, D.; Thienpont, L.M. Application of the Bland–Altman plot for interpretation of method-comparison studies: A critical investigation of its practice. Clin. Chem. 2002, 48, 799–801. [Google Scholar] [CrossRef]
- Krouwer, J.S. Why Bland–Altman plots should use X, not (Y + X)/2 when X is a reference method. Stat. Med. 2008, 27, 778–780. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normalized (z-scored) Regressor | β-Value | t-Stat | p-Value |
|---|---|---|---|
| MaxArm | 0.03 | 0.438 | 0.662 |
| MaxAnkle | 0.17 | 2.526 | 0.013 |
| SlopeArm | 0.02 | 0.329 | 0.743 |
| SlopeAnkle | 0.14 | 1.941 | 0.054 |
| TDArm | 0.09 | −1.270 | 0.206 |
| TDAnkle | −0.20 | −2.559 | 0.012 |
| Ankle-Arm | 0.51 | 7.782 | ~0 |
| Positive | Negative | TOT | ||
|---|---|---|---|---|
| Counts | Pathological ABI | 18 | 6 | 24 |
| Normal ABI | 11 | 111 | 122 | |
| % | Pathological ABI | 75 | 25 | 100 |
| Normal ABI | 9 | 91 | 100 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perpetuini, D.; Chiarelli, A.M.; Cardone, D.; Rinella, S.; Massimino, S.; Bianco, F.; Bucciarelli, V.; Vinciguerra, V.; Fallica, G.; Perciavalle, V.; et al. Photoplethysmographic Prediction of the Ankle-Brachial Pressure Index through a Machine Learning Approach. Appl. Sci. 2020, 10, 2137. https://doi.org/10.3390/app10062137
Perpetuini D, Chiarelli AM, Cardone D, Rinella S, Massimino S, Bianco F, Bucciarelli V, Vinciguerra V, Fallica G, Perciavalle V, et al. Photoplethysmographic Prediction of the Ankle-Brachial Pressure Index through a Machine Learning Approach. Applied Sciences. 2020; 10(6):2137. https://doi.org/10.3390/app10062137
Chicago/Turabian StylePerpetuini, David, Antonio Maria Chiarelli, Daniela Cardone, Sergio Rinella, Simona Massimino, Francesco Bianco, Valentina Bucciarelli, Vincenzo Vinciguerra, Giorgio Fallica, Vincenzo Perciavalle, and et al. 2020. "Photoplethysmographic Prediction of the Ankle-Brachial Pressure Index through a Machine Learning Approach" Applied Sciences 10, no. 6: 2137. https://doi.org/10.3390/app10062137
APA StylePerpetuini, D., Chiarelli, A. M., Cardone, D., Rinella, S., Massimino, S., Bianco, F., Bucciarelli, V., Vinciguerra, V., Fallica, G., Perciavalle, V., Gallina, S., & Merla, A. (2020). Photoplethysmographic Prediction of the Ankle-Brachial Pressure Index through a Machine Learning Approach. Applied Sciences, 10(6), 2137. https://doi.org/10.3390/app10062137