
Scanning of a Dental Implant with a High-Frequency Ultrasound Scanner: A Pilot Study




Abstract
:1. Introduction
2. Materials and Methods
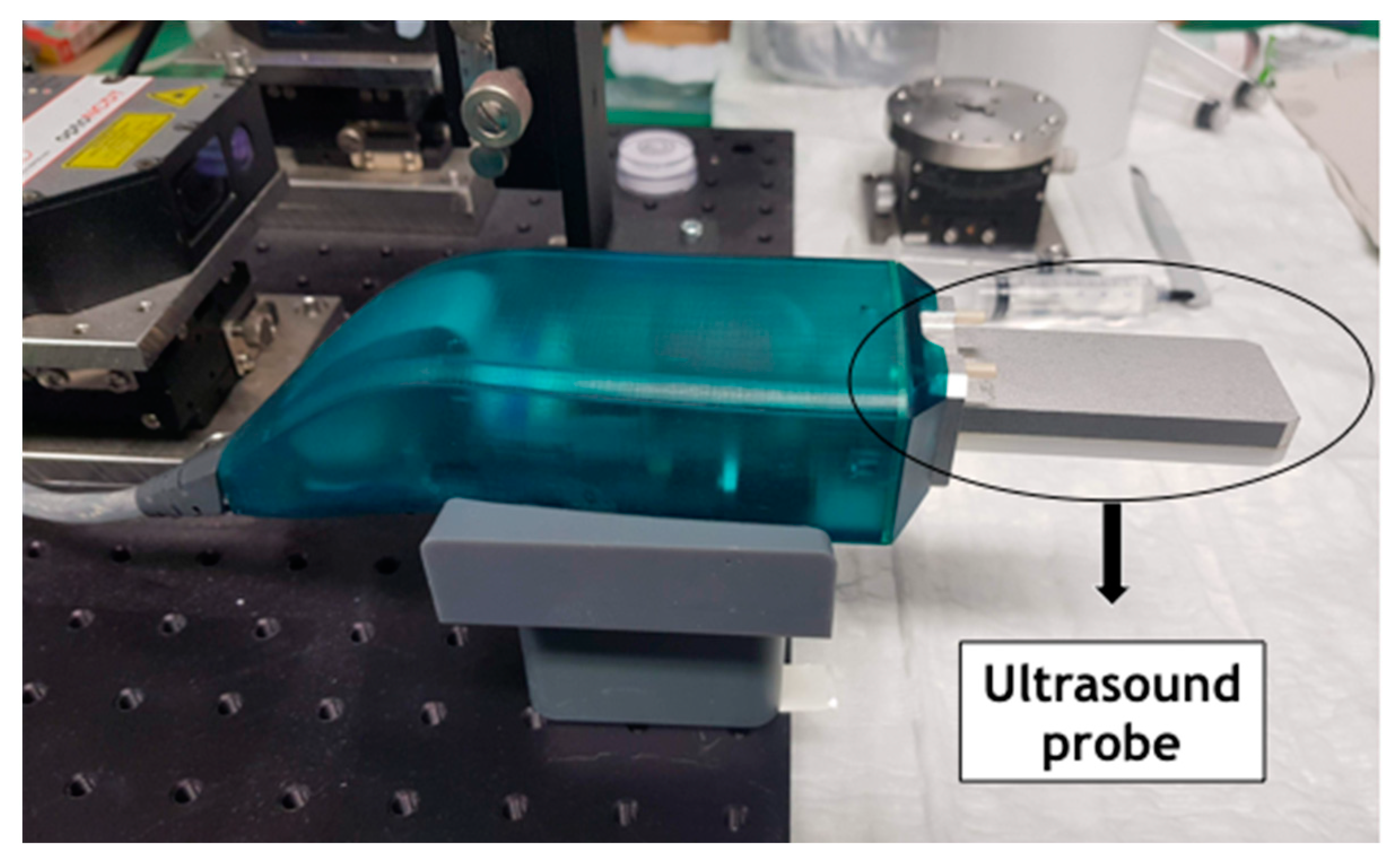
2.1. Ultrasound
2.2. Laboratory Scanner
2.3. Intraoral Scanner
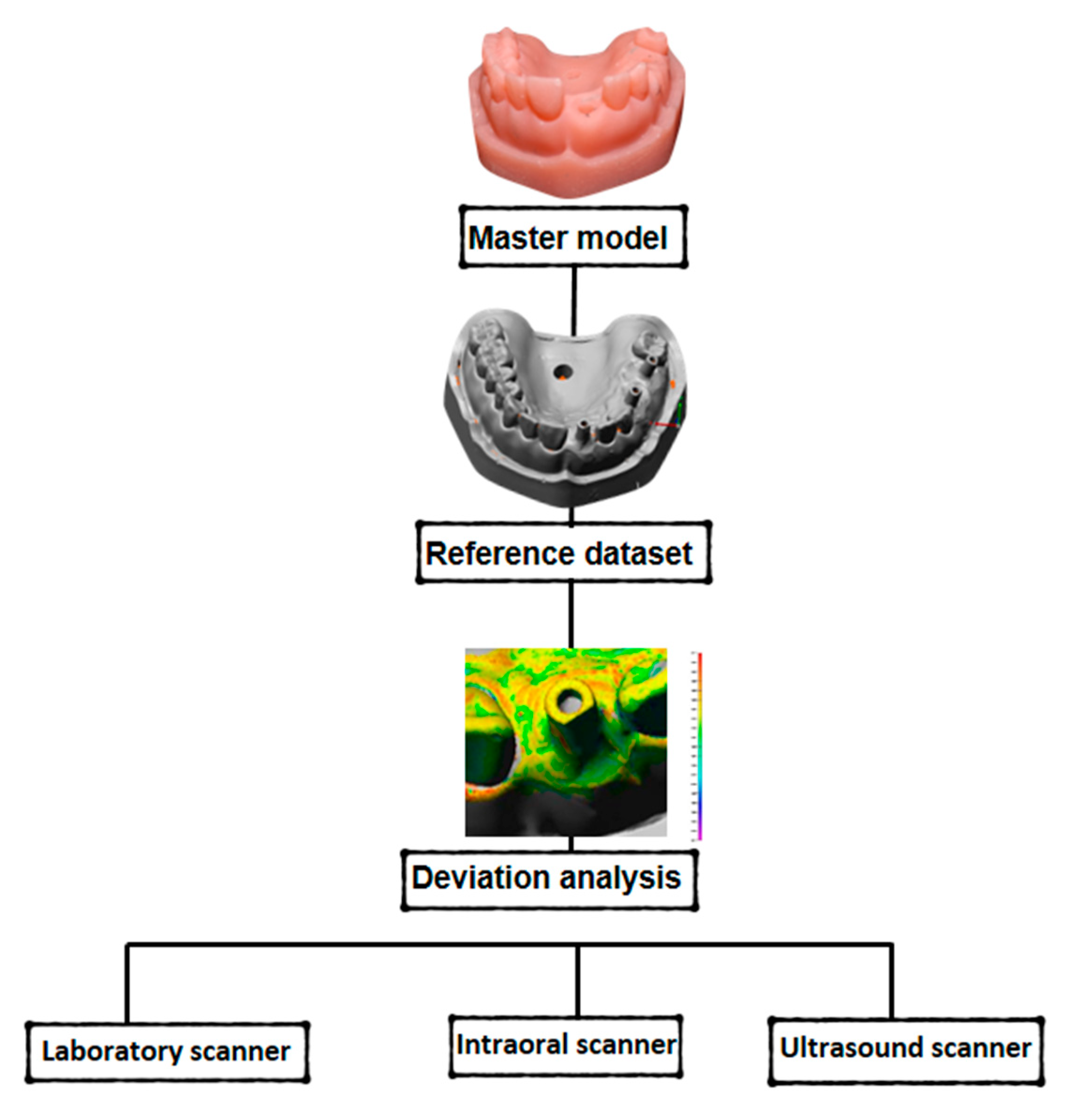
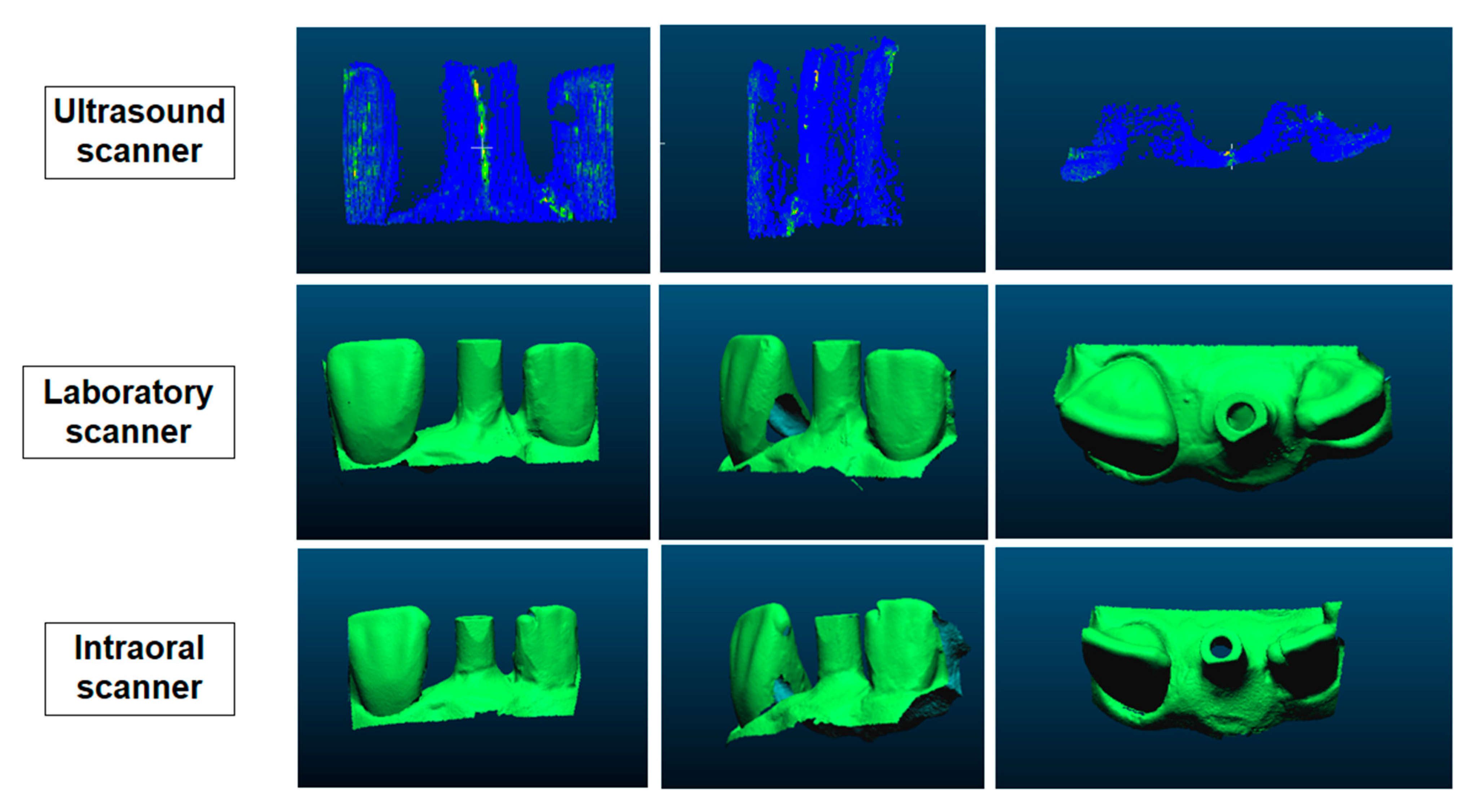
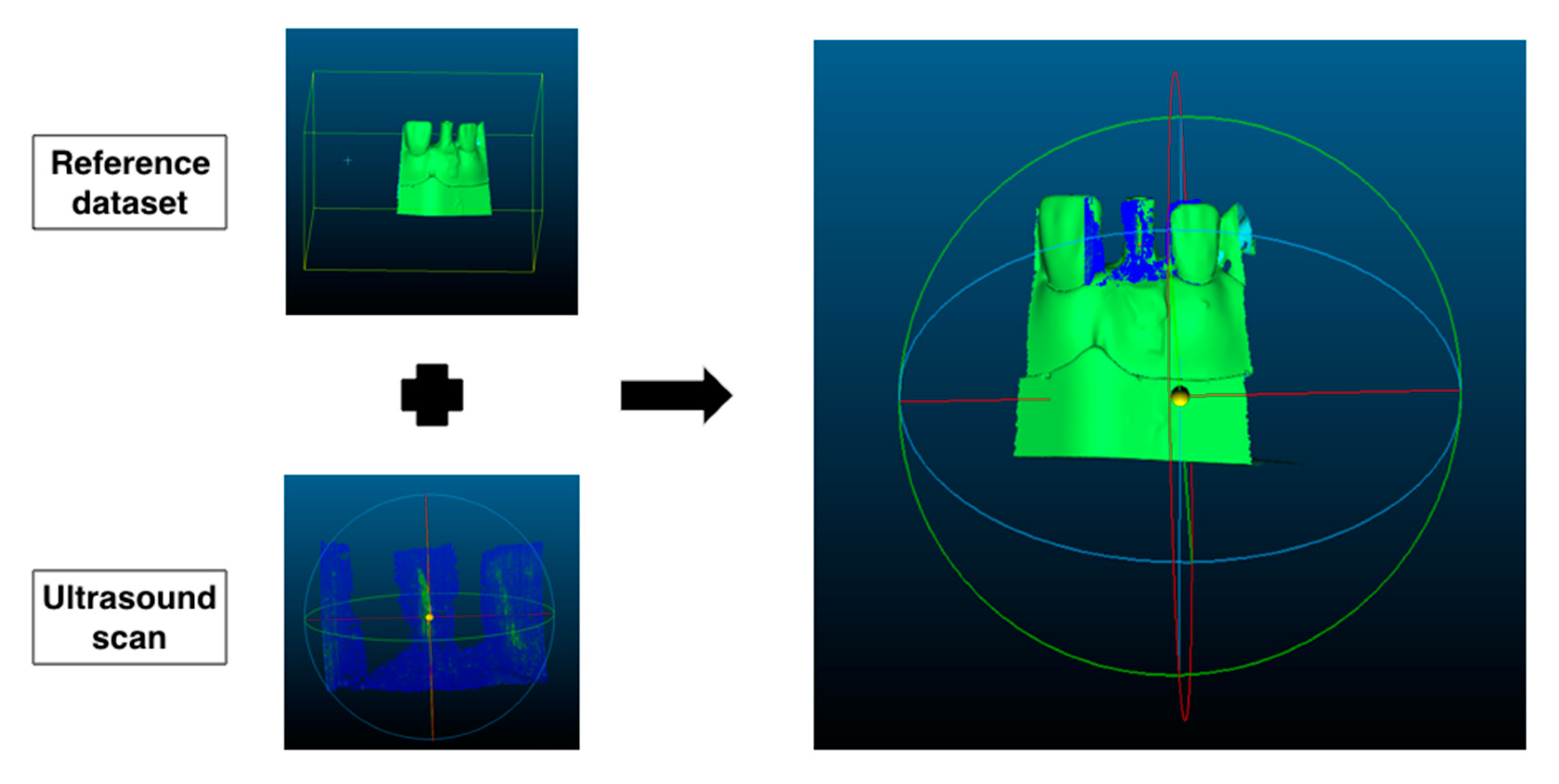
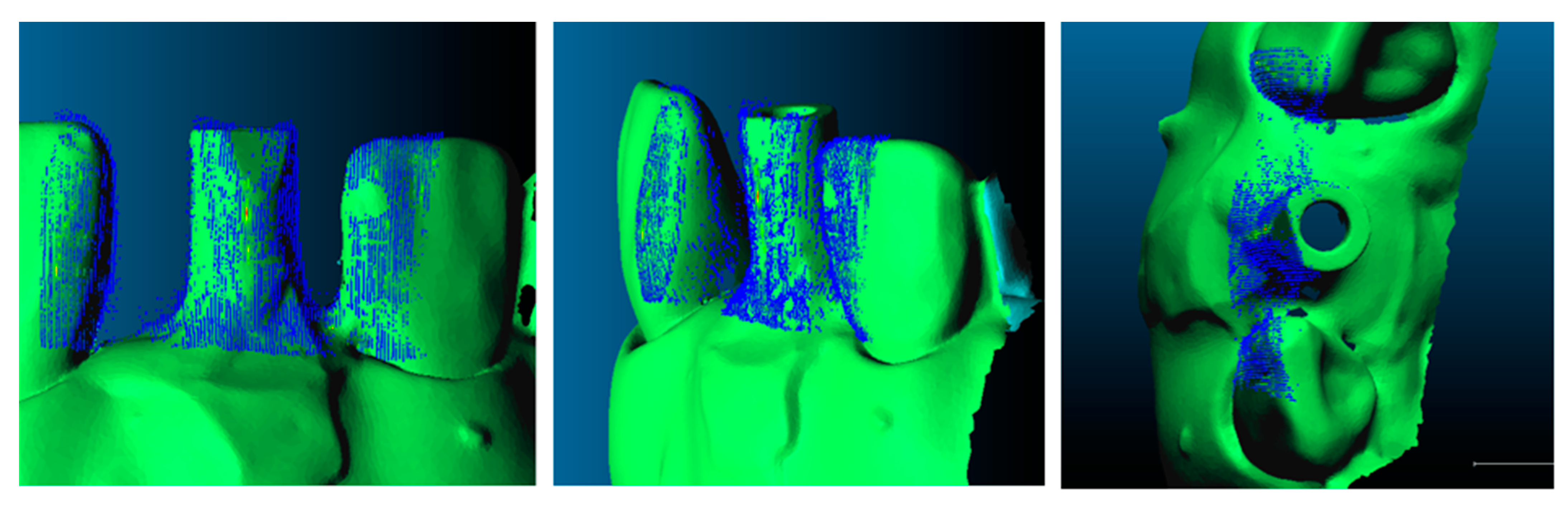
2.4. Measurement Analysis
2.5. Statistical Analysis
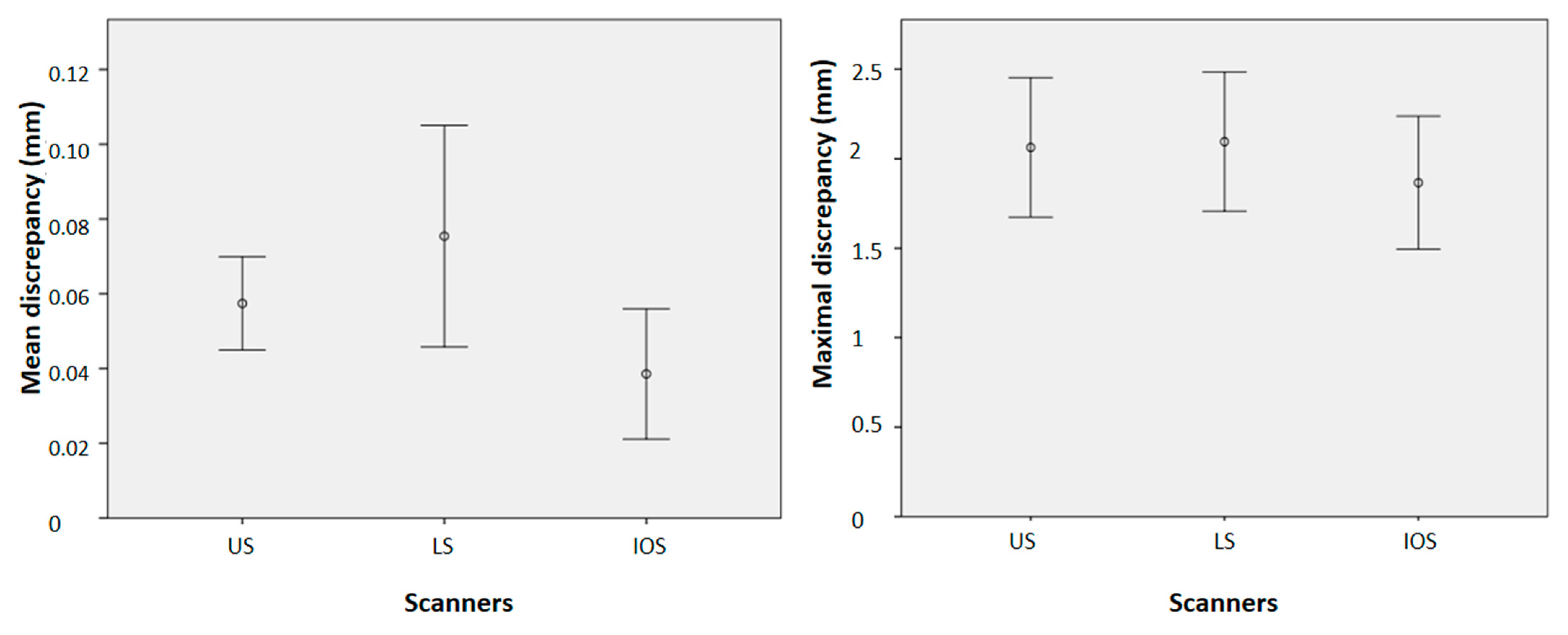
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamamoto, E.; Marotti, J.; de Campos, T.T.; Tortamano Neto, P. Accuracy of four transfer impression techniques for dental implants: A scanning electron microscopic analysis. Int. J. Oral Maxillofac. Implant. 2010, 25, 1115–1124. [Google Scholar]
- Marotti, J.; Tortamano, P.; Castilho, T.R.R.N.; Steagall, W., Jr.; Wolfart, S.; Haselhuhn, K. Accuracy of a self-perforating impression tray for dental implants. J. Prosthet. Dent. 2014, 112, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.J.; Gallucci, G.O.; Doukoudakis, A.; Weber, H.P.; Chronopoulos, V. Accuracy of implant impressions for partially and completely edentulous patients: A systematic review. Int J. Oral Maxillofac. Implant. 2014, 29, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Sabouhi, M.; Bajoghli, F.; Abolhasani, M. Evaluation of the three-dimensional accuracy of implant impression techniques in two simulated clinical conditions by optical scanning. Int J. Oral Maxillofac. Implant. 2015, 30, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Marotti, J.; Tortamano, P.; Wolfart, S. Moldagem em Implantodontia. RPG Rev. Pós Grad. 2012, 19, 113–121. [Google Scholar]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital versus conventional impressions in fixed prosthodontics: A review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Alsharbaty, M.H.M.; Alikhasi, M.; Zarrati, S.; Shamshiri, A.R. A clinical comparative study of 3-dimensional accuracy between digital and conventional implant impression techniques. J. Prosthodont. 2019, 28, 902–908. [Google Scholar] [CrossRef]
- Ting-Shu, S.; Jian, S. Intraoral digital impression technique: A review. J. Prosthodont. 2015, 24, 313–321. [Google Scholar] [CrossRef]
- Wulfman, C.; Naveau, A.; Rignon-Bret, C. Digital scanning for complete-arch implant supported restorations: A systematic review. J. Prosthet. Dent. 2020, 124, 161–167. [Google Scholar] [CrossRef]
- Wearne, S.L.; Rodriguez, A.; Ehlenberger, D.B.; Rocher, A.B.; Henderson, S.C.; Hof, P.R. New techniques for imaging, digitization and analysis of three-dimensional neural morphology on multiple scales. Neuroscience 2005, 136, 661–680. [Google Scholar] [CrossRef]
- Giménez, B.; Özcan, M.; Martínez-Rus, F.; Pradíes, G. Accuracy of a digital impression system based on parallel confocal laser technology for implants with consideration of operator experience and implant angulation and depth. Int. J. Oral Maxillofac. Implant. 2014, 29, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Giménez, B.; Özcan, M.; Martínez-Rus, F.; Pradés, G. Accuracy of a digital impression system based on active wavefront sampling technology for implants considering operator experience, implant angulation, and depth. Clin. Implant. Dent. Relat. Res. 2015, 17, e54–e64. [Google Scholar] [CrossRef] [PubMed]
- Wisjmeier, D.; Joda, T.; Flügge, T.; Fokas, G.; Tahmaseb, A.; Bechelli, D. Group 5 ITI Consensus Report: Digital technologies. Clin. Oral Implant. Res. 2018, 29, 436–442. [Google Scholar]
- Vollborn, T.; Habor, D.; Chuembou Pekam, F.; Heger, S.; Marotti, J.; Reich, S.; Wolfart, S.; Tinschert, J.; Radermacher, K. Soft tissue-preserving computer-aided impression: A novel concept using ultrasonic 3D-scanning. Int. J. Comput. Dent. 2014, 17, 277–296. [Google Scholar]
- Bohner, L.; Habor, D.; Gremse, F.; Tortamano, P.; Wolfart, S.; Marotti, J. Accuracy of high-frequency ultrasound scanner in detecting peri-implant bone defects. Ultrasound Med. Biol. 2019, 45, 650–659. [Google Scholar] [CrossRef]
- Bohner, L.; Habor, D.; Tortamano, P.; Radermacher, K.; Wolfart, S.; Marotti, J. Assessment of buccal bone surrounding dental implants using a high-frequency ultrasound scanner. Ultrasound Med. Biol. 2019, 45, 1427–1434. [Google Scholar] [CrossRef]
- Culjat, M.O.; Choi, M.; Singh, R.S.; White, S.N. Ultrasound imaging of dental implants. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; Volume 2012, pp. 456–459. [Google Scholar]
- Degen, K.; Habor, D.; Radermacher, K.; Heger, S.; Kern, J.S.; Wolfart, S.; Marotti, J. Assessment of cortical bone thickness using ultrasound. Clin. Oral Implant. Res. 2017, 28, 520–528. [Google Scholar] [CrossRef]
- Chuembou Pekam, F.; Marotti, J.; Wolfart, S.; Tinschert, J.; Radermacher, K.; Heger, S. High-frequency ultrasound as an option for scanning of prepared teeth: An in vitro study. Ultrasound Med. Biol. 2015, 41, 309–316. [Google Scholar] [CrossRef]
- Marotti, J.; Broeckmann, J.; Pekam, F.C.; Praça, L.; Radermacher, K.; Wolfart, S. Impression of subgingival dental preparation can be taken with ultrasound. Ultrasound Med. Biol. 2019, 45, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Praça, L.; Pekam, F.C.; Rego, R.O.; Radermacher, K.; Wolfart, S.; Marotti, J. Accuracy of single crowns fabricated from ultrasound digital impressions. Dent. Mater. 2018, 34, 280–288. [Google Scholar] [CrossRef]
- Heger, S.; Vollborn, T.; Tinschert, J.; Wolfart, S.; Radermacher, K. Accuracy assessment of high frequency 3D ultrasound for digital impression-taking of prepared teeth. In Proceedings of the SPIE Medical Imaging, Lake Buena Vista, FL, USA, 9–14 February 2013; Volume 8675. [Google Scholar]
- Jain, A.K.; Taylor, R.H. Understanding bone responses in B-mode ultrasound images and automatic bone surface extraction using a bayesian probabilistic framework. In Proceedings of the Medical imaging 2004: Ultrasonic imaging and signal processing, San Diego, CA, USA, 14–19 February 2004; pp. 131–142. [Google Scholar]
- Chuembou, F.; Harbor, D.; Radermacher, K.; Heger, S. TPS-RPM based segmentation of three-dimensional high frequency ultrasound SAFT images for CAD/CAM based tooth digitization. In Proceedings of the IEEE International Ultrasonics Symposium, Chicago, IL, USA, 3–6 September 2014; Volume 2014, pp. 2347–2350. [Google Scholar]
- Habor, D.; Neuhaus, S.; Vollborn, T.; Wolfart, S.; Radermacher, K.; Heger, S. Model based assessment of vestibular jaw bone thickness using high frequency 3D ultrasound micro-scanning. In Proceedings of the SPIE Medical Imaging, Lake Buena Vista, FL, USA, 9–14 February 2013; Volume 8675, p. 86750Z. [Google Scholar]
- Marotti, J.; Neuhaus, S.; Habor, D.; Bohner, L.; Heger, S.; Radermacher, K.; Wolfart, S. High-frequency ultrasound for assessment of peri-implant bone thickness. J. Clin. Med. 2019, 8, 1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhaskar, V.; Chan, H.L.; Mac Eachern, M.; Kripfgans, O.D. Updates on ultrasound research in implant dentistry: A systematic review of potential clinical indications. Dentomaxillofac. Radiol. 2018, 47, 20180076. [Google Scholar] [CrossRef]
- Choi, M.; Culjat, M.O.; Singh, R.S.; White, S.N. Ultrasound imagery for dental implant diagnosis and treatment planning in a porcine model. J. Prosthet. Dent. 2012, 108, 344–353. [Google Scholar] [CrossRef]
- Demirtuk Kocasarac, H.; Angelopoulos, C. Ultrasound in Dentistry: Toward a future of radiation-free imaging. Dent. Clin. 2018, 62, 481–489. [Google Scholar]
- Marotti, J.; Heger, S.; Tinschert, J.; Tortamano, P.; Chuembou, F.; Radermacher, K.; Wolfart, S. Recent advances of ultrasound imaging in dentistry—A review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 819–832. [Google Scholar] [CrossRef]
- Flügge, T.; Van der Meer, W.J.; Gonzales, B.G.; Vach, K.; Wisjmeijer, D.; Wang, P. The accuracy of different dental impression techniques for implant-supported dental prostheses: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 374–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habor, D. Ultraschallbasierte Struktur-und Geometrieanalyse für die Planung und Verlaufskontrolle von dentalen Implantationen. In Aachener Beiträge zur Medizintechnik, 63th ed.; Leonhardt, S., Radermacher, K., Schmitz-Rode, T., Eds.; Shaker: Aachen, Germany, 2021; p. 212. [Google Scholar]
- Kim, K.; Choi, H. High-frequency high-voltage class F amplifier for high-frequency wireless ultrasound systems. PLoS ONE 2021, 16, e0249034. [Google Scholar]
- Brezinski, M.E.; Tearney, G.J.; Weissman, N.J.; Boppart, S.A.; Bouma, B.E.; Hee, M.R.; Weyman, A.E.; Swanson, E.A.; Southern, J.F.; Fujimoto, J.G. Assessing atherosclerotic plaque morphology: Comparison of optical coherence tomography and high frequency intravascular ultrasound. Heart 1997, 77, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Vollborn, T.; Habor, D.; Junk, S.; Radermacher, K.; Heger, S. A voice-coil actuated ultrasound micro-scanner for intraoral high resolution impression taking. In Proceedings of the 2012 IEEE/RSJ International Conference in Intelligent Robots and Systems, Vilamoura-Algarve, Portugal, 7–12 October 2012; pp. 3571–3573. [Google Scholar]
- Dehurtevent, M.; Robberecht, L.; Behin, P. Influence of dentist experience with scan spray systems used in direct CAD/CAM impressions. J. Prosthet. Dent. 2015, 113, 17–21. [Google Scholar] [CrossRef]
- Maréchal, P.; Levassort, F.; Holc, J.; Tran-Huu-Hue, L.P.; Kosec, M.; Lethiecp, M. High-frequency transducers based on integrated piezoelectric thick films for medical imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2006, 53, 1524–1533. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Sum of Squares | Df | Mean Square | F | p-Value | |
|---|---|---|---|---|---|---|
| Sphericity assumed | Scanner | 6790.81 | 2 | 3395.40 | 3.17 | 0.06 |
| Error | 19,224.91 | 18 | 1068.051 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bohner, L.; Habor, D.; Radermacher, K.; Wolfart, S.; Marotti, J. Scanning of a Dental Implant with a High-Frequency Ultrasound Scanner: A Pilot Study. Appl. Sci. 2021, 11, 5494. https://doi.org/10.3390/app11125494
Bohner L, Habor D, Radermacher K, Wolfart S, Marotti J. Scanning of a Dental Implant with a High-Frequency Ultrasound Scanner: A Pilot Study. Applied Sciences. 2021; 11(12):5494. https://doi.org/10.3390/app11125494
Chicago/Turabian StyleBohner, Lauren, Daniel Habor, Klaus Radermacher, Stefan Wolfart, and Juliana Marotti. 2021. "Scanning of a Dental Implant with a High-Frequency Ultrasound Scanner: A Pilot Study" Applied Sciences 11, no. 12: 5494. https://doi.org/10.3390/app11125494
APA StyleBohner, L., Habor, D., Radermacher, K., Wolfart, S., & Marotti, J. (2021). Scanning of a Dental Implant with a High-Frequency Ultrasound Scanner: A Pilot Study. Applied Sciences, 11(12), 5494. https://doi.org/10.3390/app11125494