
Regenerative Endodontics as the Future Treatment of Immature Permanent Teeth



Abstract
:1. Introduction
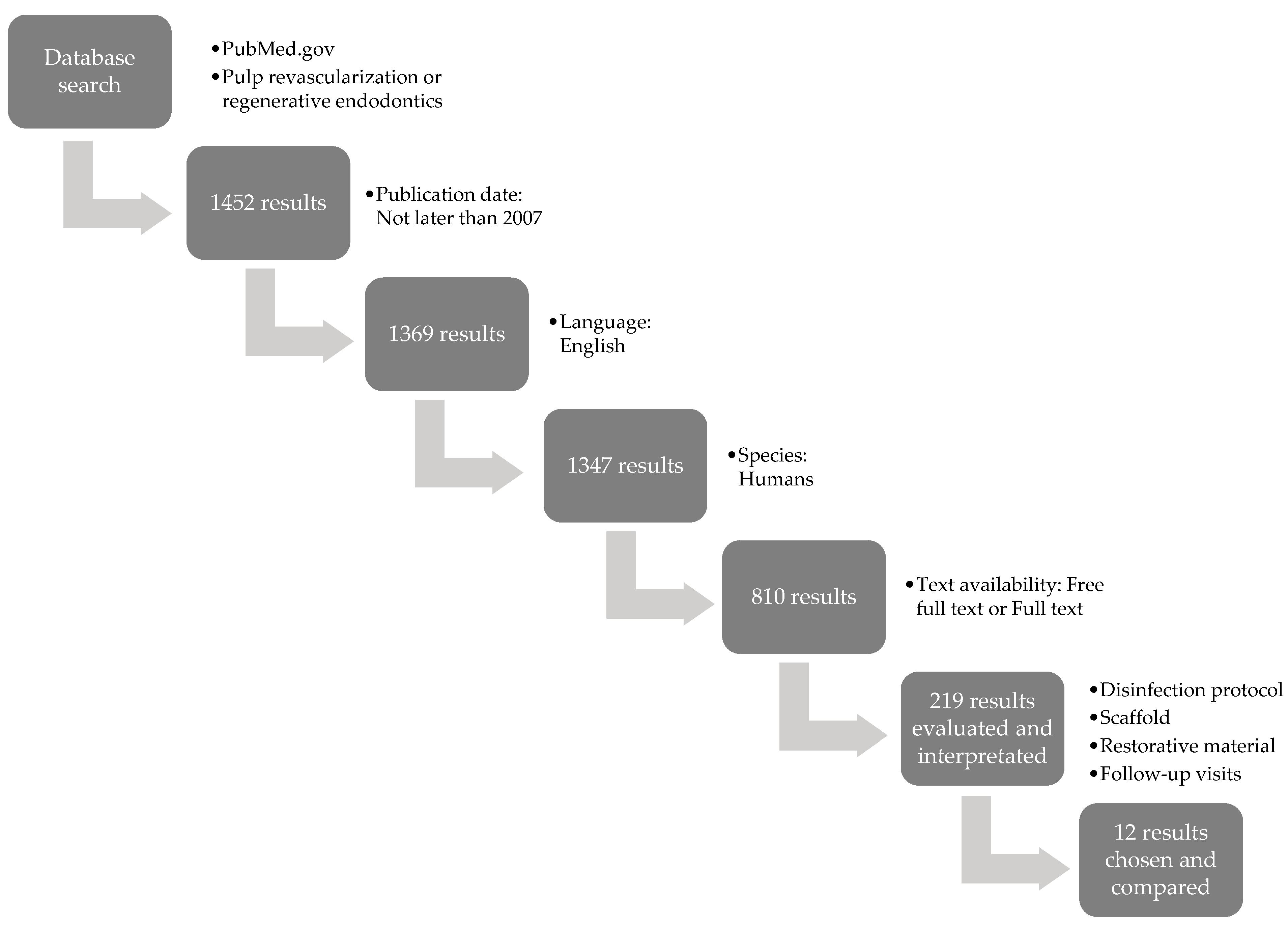
2. Materials and Methods
3. Results
3.1. Root Canal Disinfection
3.2. Components of the Pulp Regeneration Process
3.3. Root Canal Lumen Closure
3.4. Follow-Ups
3.5. Comparison of Methods and Effects of REP
3.6. Proposed Protocol of REP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Staffoli, S.; Plotino, G.; Torrijos, B.G.N.; Grande, N.M.; Bossù, M.; Gambarini, G.; Polimeni, A. Regenerative Endodontic Procedures Using Contemporary Endodontic Materials. Materials 2019, 12, 908. [Google Scholar] [CrossRef] [Green Version]
- Lee, L.-W.; Hsieh, S.-C.; Lin, Y.-H.; Huang, C.-F.; Hsiao, S.-H.; Hung, W.-C. Comparison of clinical outcomes for 40 necrotic immature permanent incisors treated with calcium hydroxide or mineral trioxide aggregate apexification/apexogenesis. J. Formos. Med. Assoc. 2015, 114, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Sheehy, E.C.; Roberts, G.J. Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: A review. Br. Dent. J. 1997, 183, 241–246. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Farik, B.; Munksgaard, E.C. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent. Traumatol. 2002, 18, 134–137. [Google Scholar] [CrossRef]
- Palma, P.J.; Martins, J.; Diogo, P.; Sequeira, D.; Ramos, J.C.; Diogenes, A.; Santos, J.M. Does Apical Papilla Survive and Develop in Apical Periodontitis Presence after Regenerative Endodontic Procedures? Appl. Sci. 2019, 9, 3942. [Google Scholar] [CrossRef] [Green Version]
- Palma, P.J.; Ramos, J.; Martins, J.B.; Diogenes, A.; Figueiredo, M.H.; Ferreira, P.; Viegas, C.; Santos, J.M. Histologic Evaluation of Regenerative Endodontic Procedures with the Use of Chitosan Scaffolds in Immature Dog Teeth with Apical Periodontitis. J. Endod. 2017, 43, 1279–1287. [Google Scholar] [CrossRef]
- Danwittayakorn, S.; Banomyong, D.; Ongchavalit, L.; Ngoenwiwatkul, Y.; Porkaew, P. Comparison of the Effects of Intraradicular Materials on the Incidence of Fatal Root Fracture in Immature Teeth Treated with Mineral Trioxide Aggregate Apexification: A Retrospective Study. J. Endod. 2019, 45, 977–984.e1. [Google Scholar] [CrossRef]
- Banchs, F.; Trope, M. Revascularization of Immature Permanent Teeth With Apical Periodontitis: New Treatment Protocol? J. Endod. 2004, 30, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.E.; Garcia-Godoy, F.; Hargreaves, K.M. Regenerative Endodontics: A Review of Current Status and a Call for Action. J. Endod. 2007, 33, 377–390. [Google Scholar] [CrossRef]
- Sedgley, C.M.; Cherkas, P.; Chogle, S.M.A.; Geisler, T.M.; Hargreaves, K.M.; Paranjpe, A.K.; Yamagishi, V.T.K. Endodontics Colleagues for Excellence. Regenerative Endodontics; AAE: Chicago, IL, USA, 2013. [Google Scholar]
- Hameed, M.H.; Gul, M.; Ghafoor, R.; Badar, S.B. Management of Immature Necrotic Permanent Teeth with Regenerative Endodontic Procedures—A Review Of Literature. J. Pak. Med. Assoc. 2019, 69, 1514–1520. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, E.; Jong, G.; Partridge, N.; Rosenberg, P.A.; Lin, L.M. Histologic Observation of a Human Immature Permanent Tooth with Irreversible Pulpitis after Revascularization/Regeneration Procedure. J. Endod. 2012, 38, 1293–1297. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.; Ricucci, D.; Gibbs, J.L.; Lin, L.M. Histological Findings of Revascularized/Revitalized Immature Permanent Molar with Apical Periodontitis Using Platelet-rich Plasma. J. Endod. 2013, 39, 138–144. [Google Scholar] [CrossRef]
- Becerra, P.; Ricucci, D.; Loghin, S.; Gibbs, J.L.; Lin, L.M. Histologic Study of a Human Immature Permanent Premolar with Chronic Apical Abscess after Revascularization/Revitalization. J. Endod. 2014, 40, 133–139. [Google Scholar] [CrossRef]
- Kim, S.G. Biological Molecules for the Regeneration of the Pulp-Dentin Complex. Dent. Clin. N. Am. 2017, 61, 127–141. [Google Scholar] [CrossRef]
- Zein, N.; Harmouch, E.; Lutz, J.-C.; De Grado, G.F.; Kuchler-Bopp, S.; Clauss, F.; Offner, D.; Hua, G.; Benkirane-Jessel, N.; Fioretti, F. Polymer-Based Instructive Scaffolds for Endodontic Regeneration. Materials 2019, 12, 2347. [Google Scholar] [CrossRef] [Green Version]
- Jeeruphan, T.; Jantarat, J.; Yanpiset, K.; Suwannapan, L.; Khewsawai, P.; Hargreaves, K.M. Mahidol Study 1: Comparison of Radiographic and Survival Outcomes of Immature Teeth Treated with Either Regenerative Endodontic or Apexification Methods: A Retrospective Study. J. Endod. 2012, 38, 1330–1336. [Google Scholar] [CrossRef]
- Shivashankar, V.Y.; Johns, D.A.; Maroli, R.K.; Sekar, M.; Chandrasekaran, R.; Karthikeyan, S.; Renganathan, S.K. Comparison of the Effect of PRP, PRF and Induced Bleeding in the Revascularization of Teeth with Necrotic Pulp and Open Apex: A Triple Blind Randomized Clinical Trial. J. Clin. Diagn. Res. 2017, 11, ZC34–ZC39. [Google Scholar] [CrossRef]
- Kahler, B.; Rossi-Fedele, G.; Chugal, N.; Lin, L.M. An Evidence-based Review of the Efficacy of Treatment Approaches for Immature Permanent Teeth with Pulp Necrosis. J. Endod. 2017, 43, 1052–1057. [Google Scholar] [CrossRef]
- Cvek, M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Dent. Traumatol. 1992, 8, 45–55. [Google Scholar] [CrossRef]
- Fang, Y.; Wang, X.; Zhu, J.; Su, C.; Yang, Y.; Meng, L. Influence of Apical Diameter on the Outcome of Regenerative Endodontic Treatment in Teeth with Pulp Necrosis: A Review. J. Endod. 2018, 44, 414–431. [Google Scholar] [CrossRef]
- Estefan, B.S.; El Batouty, K.M.; Nagy, M.M.; Diogenes, A. Influence of Age and Apical Diameter on the Success of Endodontic Regeneration Procedures. J. Endod. 2016, 42, 1620–1625. [Google Scholar] [CrossRef]
- Kim, S.G.; Malek, M.; Sigurdsson, A.; Lin, L.M.; Kahler, B. Regenerative endodontics: A comprehensive review. Int. Endod. J. 2018, 51, 1367–1388. [Google Scholar] [CrossRef]
- Koç, S.; Del Fabbro, M. Does the Etiology of Pulp Necrosis Affect Regenerative Endodontic Treatment Outcomes? A Systematic Review and Meta-analyses. J. Évid. Based Dent. Pract. 2020, 20, 101400. [Google Scholar] [CrossRef]
- Conde, M.C.M.; Chisini, L.; Sarkis-Onofre, R.; Schuch, H.; Nör, J.E.; Demarco, F.F. A scoping review of root canal revascularization: Relevant aspects for clinical success and tissue formation. Int. Endod. J. 2016, 50, 860–874. [Google Scholar] [CrossRef] [Green Version]
- Yadav, P.; Pruthi, P.J.; Nawal, R.R.; Talwar, S.; Verma, M. Novel use of platelet-rich fibrin matrix and MTA as an apical barrier in the management of a failed revascularization case. Dent. Traumatol. 2015, 31, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Nagata, J.; Zaia, A.; Souza-Filho, F.; Rocha-Lima, T.; Gomes, B.P.; Ferraz, C.; Jesus-Soares, A.D. Pulp revascularization for immature replanted teeth: A case report. Aust. Dent. J. 2015, 60, 416–420. [Google Scholar] [CrossRef]
- Fouad, A.F.; Verma, P. Healing after Regenerative Procedures with and without Pulpal Infection. J. Endod. 2014, 40, S58–S64. [Google Scholar] [CrossRef]
- Kahler, B.; Lin, L.M. A Review Of Regenerative Endodontics: Current Protocols And Future Directions. J. Istanb. Univ. Fac. Dent. 2017, 51, S41–S51. [Google Scholar] [CrossRef] [Green Version]
- Kontakiotis, E.G.; Filippatos, C.G.; Tzanetakis, G.N.; Agrafioti, A. Regenerative Endodontic Therapy: A Data Analysis of Clinical Protocols. J. Endod. 2015, 41, 146–154. [Google Scholar] [CrossRef]
- Martin, D.E.; de Almeida, J.F.A.; Henry, M.A.; Khaing, Z.Z.; Schmidt, C.E.; Teixeira, F.B.; Diogenes, A. Concentration-dependent Effect of Sodium Hypochlorite on Stem Cells of Apical Papilla Survival and Differentiation. J. Endod. 2014, 40, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Severing, A.-L.; Rembe, J.-D.; Koester, V.; Stuermer, E.K. Safety and efficacy profiles of different commercial sodium hypochlorite/hypochlorous acid solutions (NaClO/HClO): Antimicrobial efficacy, cytotoxic impact and physicochemical parametersin vitro. J. Antimicrob. Chemother. 2019, 74, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Aydin, Z.U.; Akpinar, K.E.; Hepokur, C.; Erdönmez, D. Assessment of toxicity and oxidative DNA damage of sodium hypochlorite, chitosan and propolis on fibroblast cells. Braz. Oral Res. 2018, 32, e119. [Google Scholar] [CrossRef]
- Navarro-Escobar, E.; Gonzalez-Rodriguez, M.; Ferrer-Luque, C. Cytotoxic effects of two acid solutions and 2.5% sodium hypochlorite used in endodontic therapy. Med. Oral Patol. Oral Cir. Bucal 2009, 15, e90–e94. [Google Scholar] [CrossRef] [Green Version]
- American Association of Endodontists. AAE Clinical Considerations for a Regenerative Procedure; American Association of Endodontists: Chicago, IL, USA, 2018. [Google Scholar]
- Cunningham, W.T.; Joseph, S.W. Effect of temperature on the bactericidal action of sodium hypochlorite endodontic irrigant. Oral Surg. Oral Med. Oral Pathol. 1980, 50, 569–571. [Google Scholar] [CrossRef]
- Widbiller, M.; Althumairy, R.I.; Diogenes, A. Direct and Indirect Effect of Chlorhexidine on Survival of Stem Cells from the Apical Papilla and Its Neutralization. J. Endod. 2019, 45, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Namour, M.; Theys, S. Pulp Revascularization of Immature Permanent Teeth: A Review of the Literature and a Proposal of a New Clinical Protocol. Sci. World J. 2014, 2014, 737503. [Google Scholar] [CrossRef] [Green Version]
- Valsan, D.; Pulyodan, M.K.; Mohan, S.P.; Divakar, N.; Moyin, S.; Thayyil, S. Regenerative endodontics: A paradigm shift in clinical endodontics. J. Pharm. Bioallied Sci. 2020, 12, S20–S26. [Google Scholar] [CrossRef]
- Windley, W.; Teixeira, F.; Levin, L.; Sigurdsson, A.; Trope, M. Disinfection of Immature Teeth with a Triple Antibiotic Paste. J. Endod. 2005, 31, 439–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoshino, E.; Kurihara-Ando, N.; Sato, I.; Uematsu, H.; Sato, M.; Kota, K.; Iwaku, M. In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int. Endod. J. 1996, 29, 125–130. [Google Scholar] [CrossRef]
- Berkhoff, J.A.; Chen, P.B.; Teixeira, F.B.; Diogenes, A. Evaluation of Triple Antibiotic Paste Removal by Different Irrigation Procedures. J. Endod. 2014, 40, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Ruparel, N.B.; Teixeira, F.B.; Ferraz, C.C.; Diogenes, A. Direct Effect of Intracanal Medicaments on Survival of Stem Cells of the Apical Papilla. J. Endod. 2012, 38, 1372–1375. [Google Scholar] [CrossRef]
- Segura-Egea, J.J.; Gould, K.; Şen, B.H.; Jonasson, P.; Cotti, E.; Mazzoni, A.; Sunay, H.; Tjäderhane, L.; Dummer, P. European Society of Endodontology position statement: The use of antibiotics in endodontics. Int. Endod. J. 2018, 51, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Galler, K.M.; Krastl, G.; Simon, S.; Van Gorp, G.; Meschi, N.; Vahedi, B.; Lambrechts, P. European Society Of Endodontology Position Statement: Revitalization Procedures. Int. Endod. J. 2016, 49, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Brogni, J.K.; Vitali, F.C.; Cardoso, I.V.; Dos Santos, J.D.; Prado, M.; Alves, A.M.H.; Duque, T.M. A second attempt at pulp revascularisation on an immature traumatised anterior tooth: A case report with two-year follow-up. Aust. Endod. J. 2020, 47, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Estrela, C.; Pimenta, F.C.; Ito, I.Y.; Bammann, L.L. Antimicrobial evaluation of calcium hydroxide in infected dentinal tubules. J. Endod. 1999, 25, 416–418. [Google Scholar] [CrossRef]
- Bose, R.; Nummikoski, P.; Hargreaves, K. A Retrospective Evaluation of Radiographic Outcomes in Immature Teeth With Necrotic Root Canal Systems Treated With Regenerative Endodontic Procedures. J. Endod. 2009, 35, 1343–1349. [Google Scholar] [CrossRef] [Green Version]
- Gomes-Filho, J.E.; Duarte, P.C.T.; de Oliveira, C.B.; Watanabe, S.; Lodi, C.S.; Cintra, L.T. Ângelo; Bernabé, P.F.E. Tissue Reaction to a Triantibiotic Paste Used for Endodontic Tissue Self-regeneration of Nonvital Immature Permanent Teeth. J. Endod. 2012, 38, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraghavan, R.; Mathian, V.M.; Sundaram, A.M.; Karunakaran, R.; Vinodh, S. Triple antibiotic paste in root canal therapy. J. Pharm. Bioallied Sci. 2012, 4, S230–S233. [Google Scholar] [CrossRef]
- Reynolds, K.; Johnson, J.D.; Cohenca, N. Pulp revascularization of necrotic bilateral bicuspids using a modified novel technique to eliminate potential coronal discolouration: A case report. Int. Endod. J. 2009, 42, 84–92. [Google Scholar] [CrossRef]
- Park, H.-B.; Lee, B.-N.; Hwang, Y.-C.; Hwang, I.-N.; Oh, W.-M.; Chang, H.-S. Treatment of non-vital immature teeth with amoxicillin-containing triple antibiotic paste resulting in apexification. Restor. Dent. Endod. 2015, 40, 322–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thibodeau, B.; Trope, M. Pulp Revascularization Of A Necrotic Infected Immature Permanent Tooth: Case Report And Review Of The Literature. Pediatr. Dent. 2007, 29, 47–50. [Google Scholar]
- Jung, C.; Kim, S.; Sun, T.; Cho, Y.-B.; Song, M. Pulp-dentin regeneration: Current approaches and challenges. J. Tissue Eng. 2019, 10, 2041731418819263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Althumairy, R.I.; Teixeira, F.B.; Diogenes, A. Effect of Dentin Conditioning with Intracanal Medicaments on Survival of Stem Cells of Apical Papilla. J. Endod. 2014, 40, 521–525. [Google Scholar] [CrossRef]
- Graham, L.; Cooper, P.R.; Cassidy, N.; Nor, J.E.; Sloan, A.J.; Smith, A.J. The effect of calcium hydroxide on solubilisation of bio-active dentine matrix components. Biomaterials 2006, 27, 2865–2873. [Google Scholar] [CrossRef] [PubMed]
- Galler, K.M.; Buchalla, W.; Hiller, K.-A.; Federlin, M.; Eidt, A.; Schiefersteiner, M.; Schmalz, G. Influence of Root Canal Disinfectants on Growth Factor Release from Dentin. J. Endod. 2015, 41, 363–368. [Google Scholar] [CrossRef] [PubMed]
- El-Tayeb, M.M.; Abu-Seida, A.M.; El Ashry, S.; El-Hady, S.A. Evaluation of antibacterial activity of propolis on regenerative potential of necrotic immature permanent teeth in dogs. BMC Oral Health 2019, 19, 174. [Google Scholar] [CrossRef] [Green Version]
- Mohan, D.; Maruthingal, S.; Indira, R.; Divakar, D.D.; Al Kheraif, A.A.; Ramakrishnaiah, R.; Durgesh, B.; Basavarajappa, S.; John, J. Photoactivated disinfection (PAD) of dental root canal system—An ex-vivo study. Saudi J. Biol. Sci. 2016, 23, 122–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poggio, C.; Arciola, C.R.; Dagna, A.; Florindi, F.; Chiesa, M.; Saino, E.; Imbriani, M.; Visai, L. Photoactivated Disinfection (PAD) in Endodontics: An in vitro Microbiological Evaluation. Int. J. Artif. Organs 2011, 34, 889–897. [Google Scholar] [CrossRef]
- Katalinić, I.; Budimir, A.; Bošnjak, Z.; Jakovljević, S.; Anić, I. The photo-activated and photo-thermal effect of the 445/970 nm diode laser on the mixed biofilm inside root canals of human teeth in vitro: A pilot study. Photodiagnosis Photodyn. Ther. 2019, 26, 277–283. [Google Scholar] [CrossRef]
- Johns, D.A.; Shivashankar, V.Y.; Krishnamma, S.; Johns, M. Use of photoactivated disinfection and platelet-rich fibrin in regenerative Endodontics. J. Conserv. Dent. 2014, 17, 487–490. [Google Scholar] [CrossRef]
- Abdel Hafiz Abdel Rahim, A.S.; Abdelgawad, F.; Abd Alsamed, A.M.; Moheb, D.M.; Wahab El-Dokky, N.A. Case Report: Single Visit Photo-activated Disinfection In Regenerative Endodontics. F1000Research 2020, 8, 1519. [Google Scholar] [CrossRef] [PubMed]
- López, F.U.; Kopper, P.M.P.; Della Bona, A.; Steier, L.; De Figueiredo, J.A.P.; Vier-Pelisser, F.V. Effect of Different Irrigating Solutions and Photo-Activated Therapy for In Vivo Root Canal Treatment. Braz. Dent. J. 2015, 26, 228–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topçuoğlu, G.; Topçuoğlu, H.S. Regenerative Endodontic Therapy in a Single Visit Using Platelet-rich Plasma and Biodentine in Necrotic and Asymptomatic Immature Molar Teeth: A Report of 3 Cases. J. Endod. 2016, 42, 1344–1346. [Google Scholar] [CrossRef] [PubMed]
- McCabe, P. Revascularization of an immature tooth with apical periodontitis using a single visit protocol: A case report. Int. Endod. J. 2014, 48, 484–497. [Google Scholar] [CrossRef]
- Meschi, N.; Hilkens, P.; Lambrichts, I.; Eynde, K.V.D.; Mavridou, A.; Strijbos, O.; De Ketelaere, M.; Van Gorp, G.; Lambrechts, P. Regenerative endodontic procedure of an infected immature permanent human tooth: An immunohistological study. Clin. Oral Investig. 2015, 20, 807–814. [Google Scholar] [CrossRef]
- Araújo, P.R.D.S.; Silva, L.B.; Neto, A.P.D.S.; De Arruda, J.A.A.; Álvares, P.R.; Sobral, A.P.V.; Júnior, S.A.; Leão, J.C.; Da Silva, R.B.; Sampaio, G.C. Pulp Revascularization: A Literature Review. Open Dent. J. 2017, 10, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Lambrichts, I.; Driesen, R.B.; Dillen, Y.; Gervois, P.; Ratajczak, J.; Vangansewinkel, T.; Wolfs, E.; Bronckaers, A.; Hilkens, P. Dental Pulp Stem Cells: Their Potential in Reinnervation and Angiogenesis by Using Scaffolds. J. Endod. 2017, 43, S12–S16. [Google Scholar] [CrossRef]
- Piva, E.; Tarlé, S.A.; Nör, J.E.; Zou, D.; Hatfield, E.; Guinn, T.; Eubanks, E.J.; Kaigler, D. Dental Pulp Tissue Regeneration Using Dental Pulp Stem Cells Isolated and Expanded in Human Serum. J. Endod. 2017, 43, 568–574. [Google Scholar] [CrossRef] [Green Version]
- Dissanayaka, W.L.; Hargreaves, K.M.; Jin, L.; Samaranayake, L.P.; Zhang, C. The Interplay of Dental Pulp Stem Cells and Endothelial Cells in an Injectable Peptide Hydrogel on Angiogenesis and Pulp Regeneration In Vivo. Tissue Eng. Part A 2015, 21, 550–563. [Google Scholar] [CrossRef] [Green Version]
- Sakthivel, S.; Gayathri, V.; Anirudhan, S.; Roja, R.J.S. Platelet-rich Fibrin And Collagen Matrix For The Regeneration Of Infected Necrotic Immature Teeth. J. Clin. Transl. Res. 2020, 6, 1–5. [Google Scholar]
- Bakhtiar, H.; Mazidi, S.A.; Mohammadi Asl, S.; Ellini, M.R.; Moshiri, A.; Nekoofar, M.H.; Dummer, P.M.H. The role of stem cell therapy in regeneration of dentine-pulp complex: A systematic review. Prog. Biomater. 2018, 7, 249–268. [Google Scholar] [CrossRef] [Green Version]
- Jun, H.; Lei, D.; Qifang, Y.; Yuan, X.; Deqin, Y. Effects of concentrated growth factors on the angiogenic properties of dental pulp cells and endothelial cells: An in vitro study. Braz. Oral Res. 2018, 32, e48. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.-P.; Zhang, W.; Asrican, R.; Kim, H.-J.; Kaplan, D.L.; Yelick, P.C. Accurately Shaped Tooth Bud Cell–Derived Mineralized Tissue Formation on Silk Scaffolds. Tissue Eng. Part A 2008, 14, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Hou, J.; Wu, B.; Chen, T.; Luo, A. Effects of Platelet-rich Plasma and Cell Coculture on Angiogenesis in Human Dental Pulp Stem Cells and Endothelial Progenitor Cells. J. Endod. 2014, 40, 1810–1814. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.-M.; Kim, W.-J.; Lim, H.-S.; Choi, N.-K.; Kim, S.-H.; Kim, S.-M.; Jung, J.-Y. Combination of Mineral Trioxide Aggregate and Platelet-rich Fibrin Promotes the Odontoblastic Differentiation and Mineralization of Human Dental Pulp Cells via BMP/Smad Signaling Pathway. J. Endod. 2016, 42, 82–88. [Google Scholar] [CrossRef]
- Nosrat, A.; Kolahdouzan, A.; Khatibi, A.H.; Verma, P.; Jamshidi, D.; Nevins, A.J.; Torabinejad, M. Clinical, Radiographic, and Histologic Outcome of Regenerative Endodontic Treatment in Human Teeth Using a Novel Collagen-hydroxyapatite Scaffold. J. Endod. 2019, 45, 136–143. [Google Scholar] [CrossRef]
- Moussa, D.G.; Aparicio, C. Present and future of tissue engineering scaffolds for dentin-pulp complex regeneration. J. Tissue Eng. Regen. Med. 2018, 13, 58–75. [Google Scholar] [CrossRef] [Green Version]
- Cen, L.; Liu, W.; Cui, L.; Zhang, W.; Cao, Y. Collagen Tissue Engineering: Development of Novel Biomaterials and Applications. Pediatr. Res. 2008, 63, 492–496. [Google Scholar] [CrossRef]
- Chen, M.Y.-H.; Chen, K.-L.; Chen, C.-A.; Tayebaty, F.; Rosenberg, P.A.; Lin, L.M. Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int. Endod. J. 2011, 45, 294–305. [Google Scholar] [CrossRef]
- Wang, H.H.; Sarmast, N.D.; Shadmehr, E.; Angelov, N.; Shabahang, S.; Torabinejad, M. Application of Enamel Matrix Derivative (Emdogain) in Endodontic Therapy: A Comprehensive Literature Review. J. Endod. 2018, 44, 1066–1079. [Google Scholar] [CrossRef]
- Mittal, N.; Parashar, V. Regenerative Evaluation Of Immature Roots Using PRF And Artificial Scaffolds In Necrotic Permanent Teeth: A Clinical Study. Contemp. Dent. Pract. 2019, 20, 720–726. [Google Scholar] [CrossRef]
- Bottino, M.C.; Pankajakshan, D.; Nör, J.E. Advanced Scaffolds for Dental Pulp and Periodontal Regeneration. Dent. Clin. N. Am. 2017, 61, 689–711. [Google Scholar] [CrossRef]
- Jiang, X.; Liu, H.; Peng, C. Clinical and Radiographic Assessment of the Efficacy of a Collagen Membrane in Regenerative Endodontics: A Randomized, Controlled Clinical Trial. J. Endod. 2017, 43, 1465–1471. [Google Scholar] [CrossRef]
- Diogenes, A.; Ruparel, N.B. Regenerative Endodontic Procedures. Dent. Clin. N. Am. 2017, 61, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Cehreli, Z.C.; Isbitiren, B.; Sara, S.; Erbas, G. Regenerative Endodontic Treatment (Revascularization) of Immature Necrotic Molars Medicated with Calcium Hydroxide: A Case Series. J. Endod. 2011, 37, 1327–1330. [Google Scholar] [CrossRef]
- Rizk, H.M.; Al-Deen, M.S.S.; Emam, A.A. Pulp Revascularization/Revitalization of Bilateral Upper Necrotic Immature Permanent Central Incisors with Blood Clot vs Platelet-rich Fibrin Scaffolds—A Split-mouth Double-blind Randomized Controlled Trial. Int. J. Clin. Pediatr. Dent. 2020, 13, 337–343. [Google Scholar] [CrossRef]
- Torabinejad, M.; Turman, M. Revitalization of Tooth with Necrotic Pulp and Open Apex by Using Platelet-rich Plasma: A Case Report. J. Endod. 2011, 37, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, e37–e44. [Google Scholar] [CrossRef] [PubMed]
- Nagaveni, N.B.; Poornima, P.; Mathew, M.G.; Soni, A.J.; Khan, M. A Comparative Evaluation of Revascularization Done in Traumatized Immature, Necrotic Anterior Teeth with and without Platelet-rich Fibrin: A Case Report. Int. J. Clin. Pediatr. Dent. 2020, 13, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Narang, I.; Mittal, N.; Mishra, N. A comparative evaluation of the blood clot, platelet-rich plasma, and platelet-rich fibrin in regeneration of necrotic immature permanent teeth: A clinical study. Contemp. Clin. Dent. 2015, 6, 63–68. [Google Scholar] [CrossRef]
- Joshi, S.R.; Palekar, A.U.; Pendyala, G.S.; Mopagar, V.; Padmawar, N.; Shah, P. Clinical success of platelet-rich fibrin and mineral trioxide aggregate (MTA) or MTA-like agents in healing of periapical lesion in nonsurgically treated pulpless immature permanent teeth: A systematic review. J. Int. Soc. Prev. Community Dent. 2020, 10, 379–383. [Google Scholar] [CrossRef]
- Kathuria, A.; Chaudhry, S.; Talwar, S.; Verma, M. Endodontic management of single rooted immature mandibular second molar with single canal using MTA and platelet-rich fibrin membrane barrier: A case report. J. Clin. Exp. Dent. 2011, 3, e487–e490. [Google Scholar] [CrossRef]
- Sarkar, N.; Caicedo, R.; Ritwik, P.; Moiseyeva, R.; Kawashima, I. Physicochemical Basis of the Biologic Properties of Mineral Trioxide Aggregate. J. Endod. 2005, 31, 97–100. [Google Scholar] [CrossRef]
- Peng, C.; Yang, Y.; Zhao, Y.; Liu, H.; Xu, Z.; Zhao, D.; Qin, M. Long-term treatment outcomes in immature permanent teeth by revascularisation using MTA and GIC as canal-sealing materials: A retrospective study. Int. J. Paediatr. Dent. 2017, 27, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Madani, Z.; Alvandifar, S.; Bizhani, A. Evaluation Of Tooth Discoloration After Treatment with Mineral Trioxide Aggregate, Calcium-enriched Mixture, And Biodentine® in the Presence And Absence of Blood. Dent. Res. J. 2019, 16, 377–383. [Google Scholar]
- Akbulut, M.B.; Terlemez, A.; Akman, M.; Buyukerkmen, B.; Guneser, M.B.; Eldeniz, A.U. Tooth discoloration effects of calcium silicate based barrier materials used in revascularization and treatment with internal bleaching. J. Dent. Sci. 2017, 12, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Rudagi, K.B.; Rudagi, B. One-step apexification in immature tooth using grey mineral trioxide aggregate as an apical barrier and autologus platelet rich fibrin membrane as an internal matrix. J. Conserv. Dent. 2012, 15, 196–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wongwatanasanti, N.; Jantarat, J.; Sritanaudomchai, H.; Hargreaves, K.M. Effect of Bioceramic Materials on Proliferation and Odontoblast Differentiation of Human Stem Cells from the Apical Papilla. J. Endod. 2018, 44, 1270–1275. [Google Scholar] [CrossRef]
- Aggarwal, V.; Miglani, S.; Singla, M. Conventional apexification and revascularization induced maturogenesis of two non-vital, immature teeth in same patient: 24 months follow up of a case. J. Conserv. Dent. 2012, 15, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.; Logani, A.; Jadhav, G. Comparative outcome of revascularization in bilateral, non-vital, immature maxillary anterior teeth supplemented with or without platelet rich plasma: A case series. J. Conserv. Dent. 2013, 16, 568–572. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Das Adhikari, H. Report of a case of platelet-rich fibrin-mediated revascularization of immature 12 with histopathological evaluation. J. Conserv. Dent. 2018, 21, 691–695. [Google Scholar] [CrossRef]
- Maniglia-Ferreira, C.; Filho, E.D.G.; Gomes, F.D.A.; Reis, S.A.; Pappen, F.G. 12-Year Follow-Up of Regenerative Endodontic Treatment of Immature Permanent Upper Incisors with Acute Abscess. Braz. Dent. J. 2020, 31, 680–684. [Google Scholar] [CrossRef]
- Elfrink, M.E.C.; Heijdra, J.S.C.; Krikken, J.B.; Kouwenberg-Bruring, W.H.; Kouwenberg, H.; Weerheijm, K.L.; Veerkamp, J.S.J. Regenerative endodontic therapy: A follow-up of 47 anterior traumatised teeth. Eur. Arch. Paediatr. Dent. 2021, 22, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Silujjai, J.; Linsuwanont, P. Treatment Outcomes of Apexification or Revascularization in Nonvital Immature Permanent Teeth: A Retrospective Study. J. Endod. 2017, 43, 238–245. [Google Scholar] [CrossRef]
- Palma, P.J.; Marques, J.A.; Santos, J.; Falacho, R.I.; Sequeira, D.; Diogo, P.; Caramelo, F.; Ramos, J.C.; Santos, J.M. Tooth Discoloration after Regenerative Endodontic Procedures with Calcium Silicate-Based Cements—An Ex Vivo Study. Appl. Sci. 2020, 10, 5793. [Google Scholar] [CrossRef]
- Możyńska, J.; Metlerski, M.; Lipski, M.; Nowicka, A. Tooth Discoloration Induced by Different Calcium Silicate–based Cements: A Systematic Review of In Vitro Studies. J. Endod. 2017, 43, 1593–1601. [Google Scholar] [CrossRef]
- Camilleri, J.; Borg, J.; Damidot, D.; Salvadori, E.; Pilecki, P.; Zaslansky, P.; Darvell, B.W. Colour and chemical stability of bismuth oxide in dental materials with solutions used in routine clinical practice. PLoS ONE 2020, 15, e0240634. [Google Scholar] [CrossRef] [PubMed]
- Palma, P.J.; Marques, J.A.; Antunes, M.; Falacho, R.I.; Sequeira, D.; Roseiro, L.; Santos, J.M.; Ramos, J.C. Effect of restorative timing on shear bond strength of composite resin/calcium silicate–based cements adhesive interfaces. Clin. Oral Investig. 2021, 25, 3131–3139. [Google Scholar] [CrossRef]
- Alobaid, A.S.; Cortes, L.M.; Lo, J.; Nguyen, T.T.; Albert, J.; Abu-Melha, A.S.; Lin, L.M.; Gibbs, J.L. Radiographic and Clinical Outcomes of the Treatment of Immature Permanent Teeth by Revascularization or Apexification: A Pilot Retrospective Cohort Study. J. Endod. 2014, 40, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Nicoloso, G.F.; Goldenfum, G.M.; Pizzol, T.D.S.D.; Scarparo, R.K.; Montagner, F.; Rodrigues, J.D.A.; Casagrande, L. Pulp Revascularization or Apexification for the Treatment of Immature Necrotic Permanent Teeth: Systematic Review and Meta-Analysis. J. Clin. Pediatr. Dent. 2019, 43, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Neelamurthy, P.S.; Kumar, R.A.; Balakrishnan, V.; Venkatesan, S.M.; Narayan, G.S.; Karthikeyan, I. Revascularization in Immature and Mature Teeth with Necrotic Pulp: A Clinical Study. J. Contemp. Dent. Pract. 2018, 19, 1393–1399. [Google Scholar] [CrossRef]
- Saoud, T.M.; Martin, G.; Chen, Y.-H.M.; Chen, K.-L.; Chen, C.-A.; Songtrakul, K.; Malek, M.; Sigurdsson, A.; Lin, L.M. Treatment of Mature Permanent Teeth with Necrotic Pulps and Apical Periodontitis Using Regenerative Endodontic Procedures: A Case Series. J. Endod. 2016, 42, 57–65. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Type | Function |
|---|---|
| Human Dental Pulp Derived Stem Cells (HDPSCs) | Differentiation toward odontoblasts, osteoblasts, adipocytes, neurons, initiation of angiogenesis |
| Stem Cells from Human Exfoliated Deciduous Teeth (SHEDs) | Differentiation toward odontoblasts, osteoblasts, adipocytes, neurons |
| Periodontal Ligament Stem Cells (PDLSCs) | Osteogenesis |
| Dental Follicle Stem Cells (DFSCs) | Differentiation toward odontoblasts, fibroblasts, osteoblasts, cementoblasts |
| Human Umbilical Vein Endothelial Cells (HUVECs) | Angiogenesis |
| Stem Cells from the Apical Papilla (SCAPs) | Differentiation toward odontoblasts |
| Type | Function |
|---|---|
| Bone Morphogenetic Protein (BMP) | Dentinogenesis |
| Vascular Endothelial Growth Factor (VEGF) | Proliferation, angiogenesis |
| IGF Insulin-like Growth Factor (IGF) | Proliferation |
| TGF-β Transforming Growth Factor-β (TGF-β) | Migration, proliferation |
| FGF Fibroblast Growth Factor (FGF) | Migration, proliferation, dentinogenesis |
| Platelet-Derived Growth Factor (PDGF) | Migration, angiogenesis |
| Scaffold | Origin | Chemical Structure | Characteristics |
|---|---|---|---|
| Fibrin | Natural | Protein | Low-cost, biocompatible, derived from blood plasma, does not induce an immune response |
| Silk | Natural | Protein | Biodegradable, biocompatible, does not induce an immune response |
| Chitosan | Natural | Polysaccharide | Biocompatible, biodegradable, may cause allergic reactions |
| Hyaluronic acid | Natural | Polysaccharide | Biocompatible, low immunogenic potential, hydrogel-forming extracellular matrix |
| Collagen | Natural/synthetic | Protein | Biocompatible, low immunogenic potential, hydrogel-forming extracellular matrix |
| Self-assembling peptides | Synthetic | Peptides | Biocompatible, forming hydrogels |
| Polylactic acid (PLA), Polyglycolic acid (PGA), Poly(lactide-co-glycolide) (PLGA) | Synthetic | Polyesters | Biocompatible, biodegradable, may cause slight inflammatory reactions |
| Bioactive ceramics | Synthetic | Calcium phosphates, Bioactive glasses (mixture of sodium silicon oxides, calcium, magnesium, iron, etc.) | Biocompatible, low immunogenic potential, osteoinductivity |
| Year | Author | Irrigation/Disinfection | Scaffold | Restoration |
|---|---|---|---|---|
| 2007 | Thibodeau and Trope | 1.25% NaOCl, TAP | BC, MTA | Composite |
| 2012 | Aggarwal et al. | 5.25% NaOCl, distilled water, 2% CHX, TAP, Ca(OH)2 | BC, MTA | GI, composite |
| 2013 | Jadhav et al. | 2.5% NaOCl, TAP | BC, PRP, collagen | RMGI |
| 2014 | Johns et al. | 5.25% NaOCl, 0.9% NaCl, PAD | PRF, MTA | Composite |
| 2015 | McCabe | 5% NaOCl, 17% EDTA | BC, MTA | GI |
| 2016 | Topçuoglu et al. | 2.5% NaOCl, 0.9% NaCl, 17% EDTA | PRP, Biodentine | Composite |
| 2017 | Shivashankar et al. | 5.25% NaOCl, TAP | BC/PRP/PRF, MTA | IRM |
| 2018 | Adhikari and Gupta | 3% NaOCl, 17% EDTA, Ca(OH)2 | PRF, MTA | Composite |
| 2019 | Rahim et al. | 1.5% NaOCl, 0.9% NaCl, PAD, 17% EDTA | BC, MTA | GI, composite |
| 2020 | Maniglia-Ferreira et al. | 2.5% NaOCl, 17% EDTA, 2% CHX, DAP, Ca(OH)2, zinc oxide | BC, MTA | RMGI |
| 2020 | Elfrink et al. | 2% NaOCl, DAP/TAP | BC, MTA | Composite |
| 2020 | Sakthivel et al. | 0.5% NaOCl, 17% EDTA, Ca(OH)2 | PRF, BC, Collagen, MTA | GI, composite |
| First Appointment | Second Appointment (Only in the Absence of Signs of Inflammation) | Follow-Up (Clinical and Radiological Examination) |
|---|---|---|
| 1. Local anesthesia (may be done with vasoconstrictor) | 1. Local anesthesia (3% mepivacaine without vasoconstrictors) | 1. After three months |
| 2. Isolating the operating field with a rubber dam, disinfecting with iodine solution (Povidone/Betadine) | 2. Isolating the operating field with a rubber dam, disinfecting with iodine solution (Povidone/Betadine) | 2. After six months |
| 3. Endodontic access (sterile drills) | 3. Reopening of the tooth (sterile drills) | 3. After nine months |
| 4. Intra-chamber application of a bonding system or Biodentine * * If TAP is used | 4. Irrigation with 20 mL of 0.9% NaCl (5 min), 20 mL of 17% EDTA (5 min) | 4. After 12 months |
| 5. Irrigation with 20 mL of 2% NaOCl (5 min, ultrasound activation), 20 mL of 17% EDTA (5 min), 20 mL of 0.9% NaCl (5 min) | 5. Draining the canal with sterile paper points | 5. Every six months |
| 6. Draining the canal with sterile paper points | 6. Inducing bleeding of the apical area * (e.g., sterile, #25 K-file, 2 mm beyond the apex), clot formation (15 min), collagen membrane application * Or PRP/PRF application | |
| 7. Calcium hydroxide application (or TAP/DAP—not recommended) | 7. Application of 3–4 mm MTA/Biodentine to the clot | |
| 8. Tight temporary filling, e.g., RMGI | 8. Tight permanent filling (RMGI, composite) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zbańska, J.; Herman, K.; Kuropka, P.; Dobrzyński, M. Regenerative Endodontics as the Future Treatment of Immature Permanent Teeth. Appl. Sci. 2021, 11, 6211. https://doi.org/10.3390/app11136211
Zbańska J, Herman K, Kuropka P, Dobrzyński M. Regenerative Endodontics as the Future Treatment of Immature Permanent Teeth. Applied Sciences. 2021; 11(13):6211. https://doi.org/10.3390/app11136211
Chicago/Turabian StyleZbańska, Justyna, Katarzyna Herman, Piotr Kuropka, and Maciej Dobrzyński. 2021. "Regenerative Endodontics as the Future Treatment of Immature Permanent Teeth" Applied Sciences 11, no. 13: 6211. https://doi.org/10.3390/app11136211
APA StyleZbańska, J., Herman, K., Kuropka, P., & Dobrzyński, M. (2021). Regenerative Endodontics as the Future Treatment of Immature Permanent Teeth. Applied Sciences, 11(13), 6211. https://doi.org/10.3390/app11136211