
Debris Removal by Activation of Endodontic Irrigants in Complex Root Canal Systems: A Standardized In-Vitro-Study

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Preparation and Volumetric Measurement
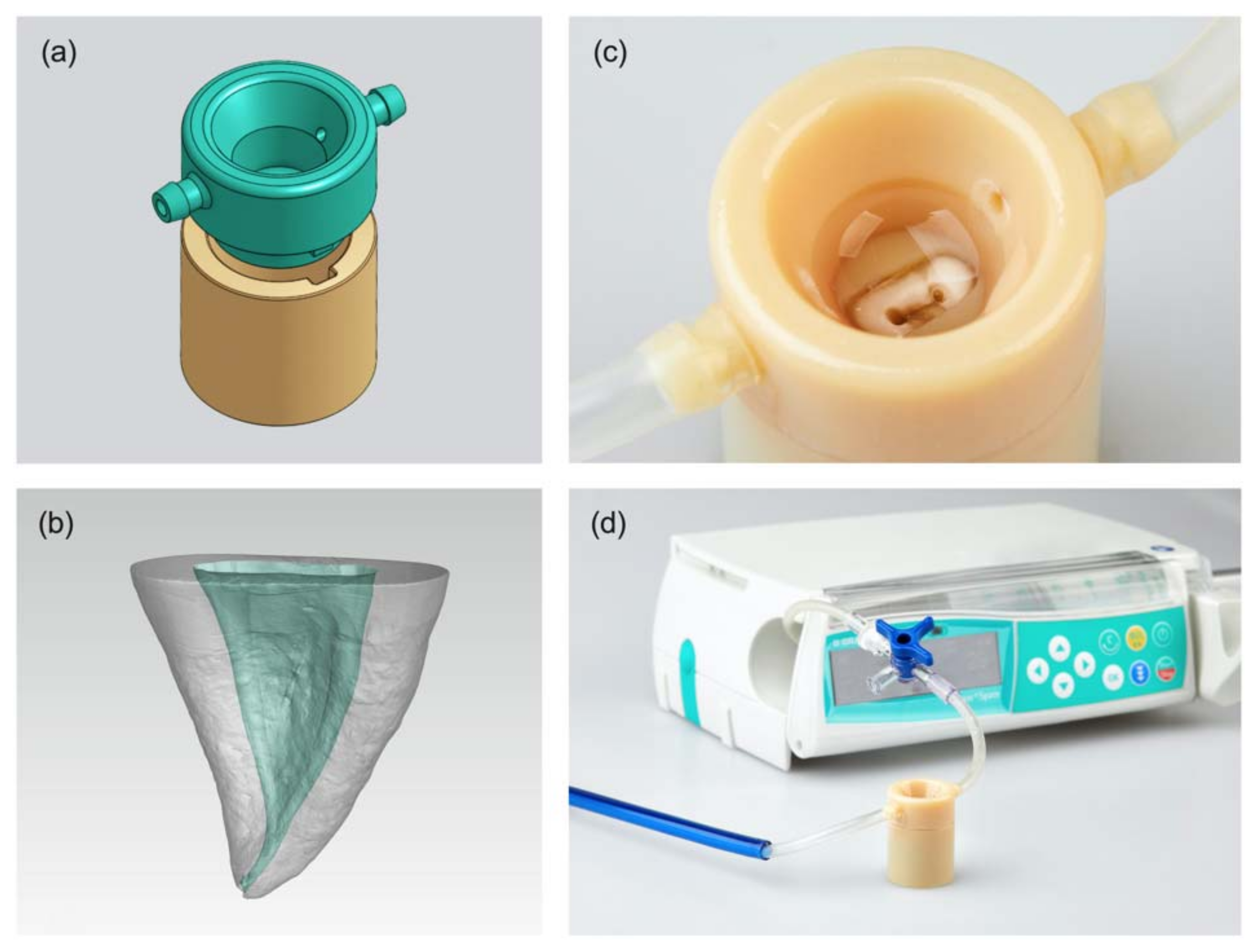
2.2. Production of 3D-Printed Irrigation Models
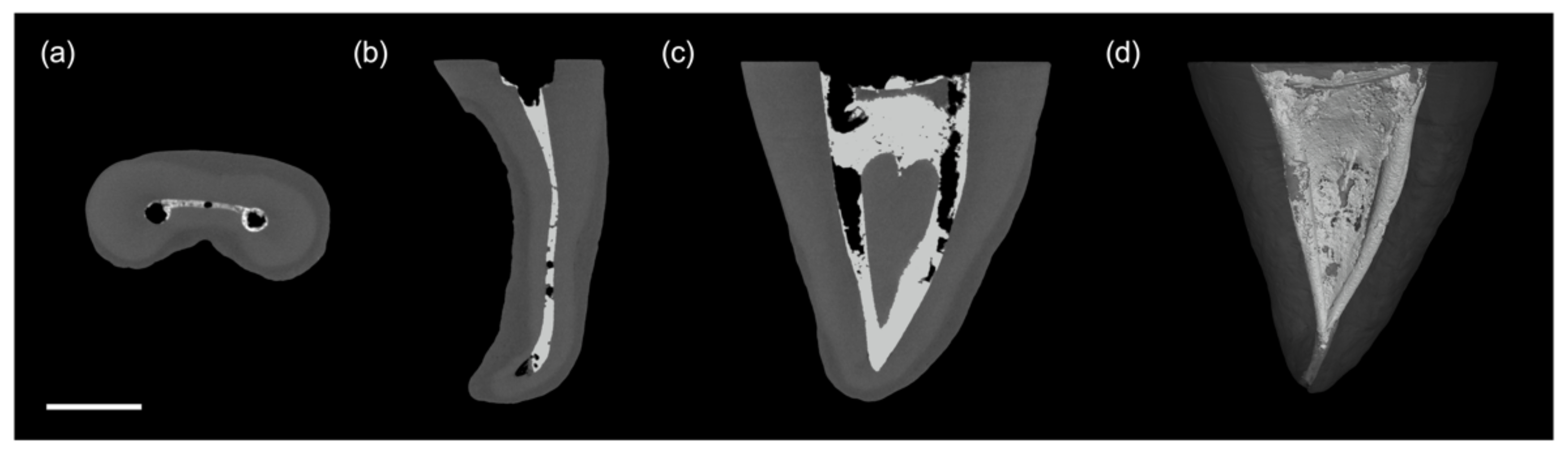
2.3. Root Canal Preparation and Introduction of Artificial Debris
2.4. Final Irrigation and Activation
- 5 mL NaOCl for 1 min
- 5 mL ultrapure water for 1min
- 5 mL of EDTA for 1 min
- 5 mL ultrapure water for 1min
- 5 mL NaOCl for 1.5 min (30 s activation, 30 s resting phase, followed by 30 s activation).
2.5. Data Treatment and Statistical Analysis
3. Results
3.1. Formation of AHTD
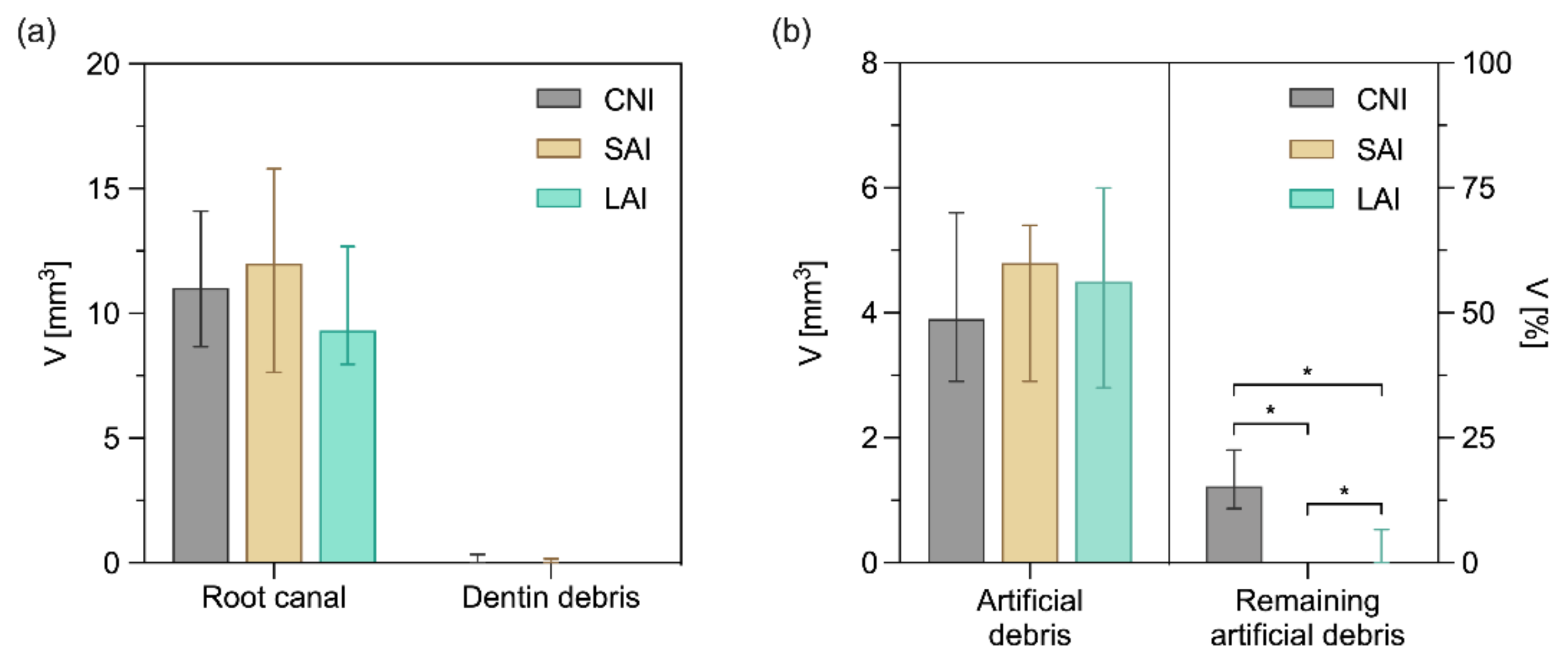
3.2. Insertion and Removal of Artificial Debris
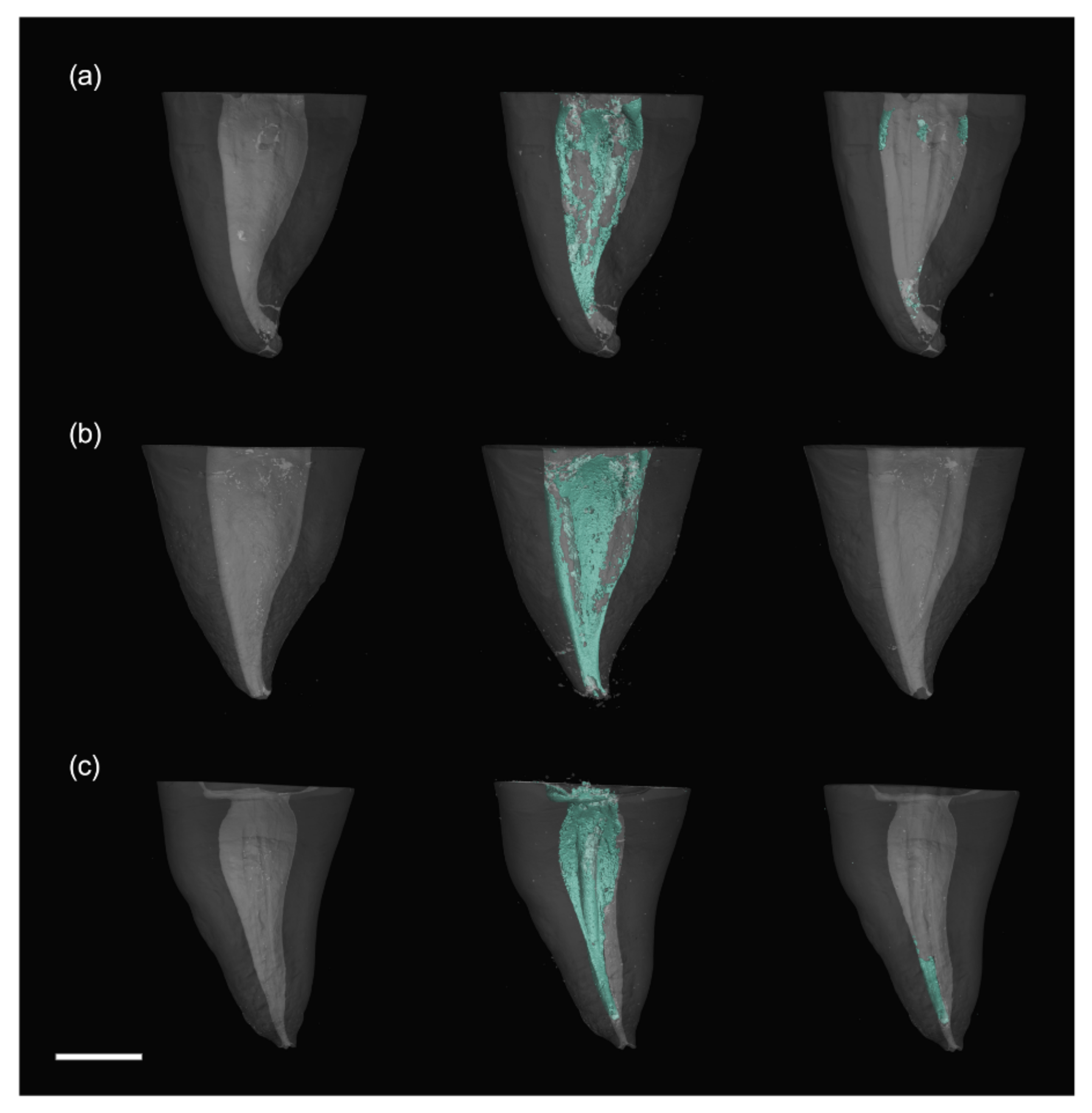
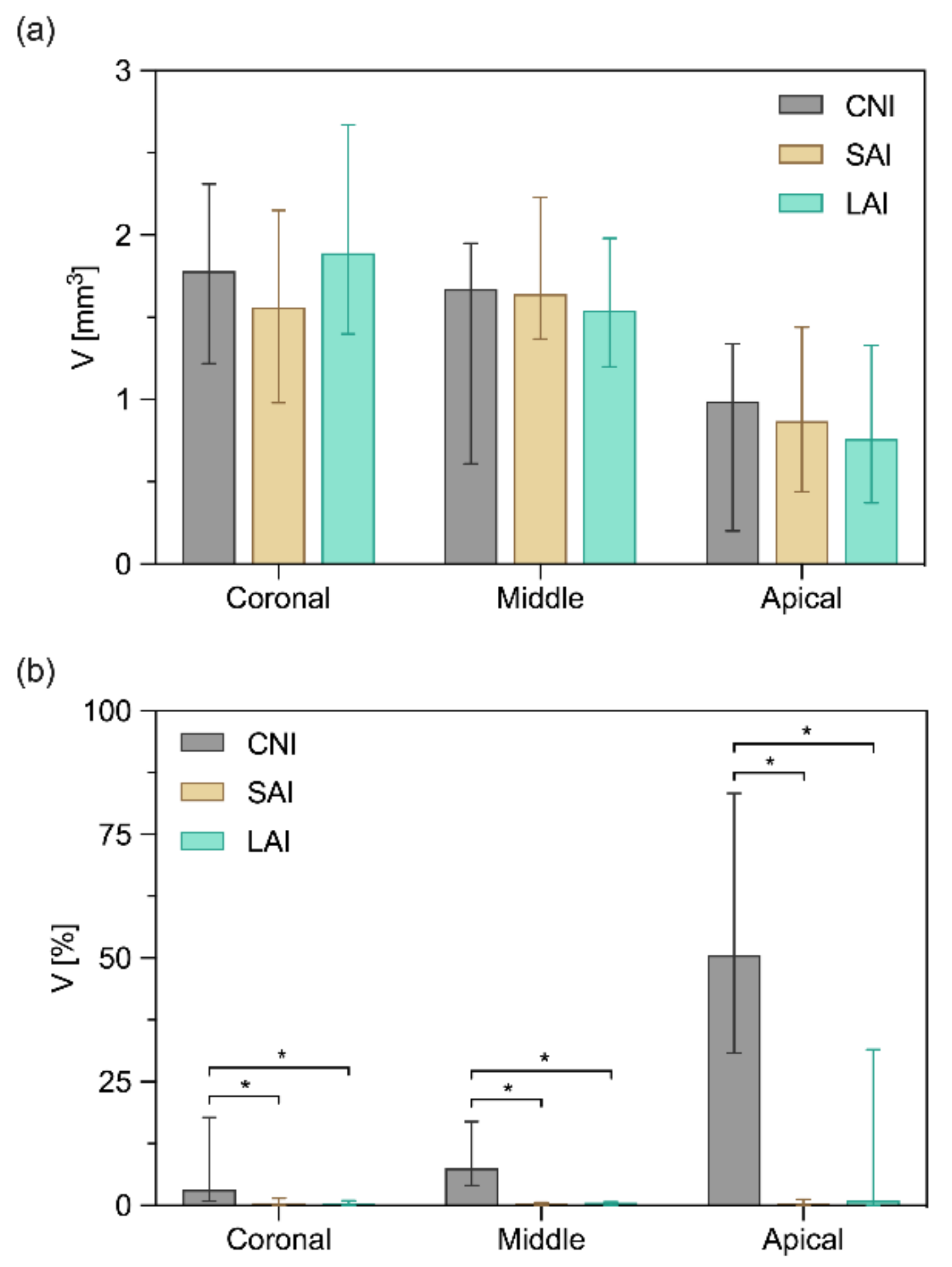
3.3. Removal of Artificial Debris in the Individual Root Thirds
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paqué, F.; Laib, A.; Gautschi, H.; Zehnder, M. Hard-Tissue Debris Accumulation Analysis by High-Resolution Computed Tomography Scans. J. Endod. 2009, 35, 1044–1047. [Google Scholar] [CrossRef] [Green Version]
- Haapasalo, M.; Shen, Y.; Wang, Z.; Gao, Y. Irrigation in endodontics. Br. Dent. J. 2014, 216, 299–303. [Google Scholar] [CrossRef]
- Meto, A.; Droboniku, E.; Blasi, E.; Colombari, B.; Tragaj, E.; Cervino, G.; Fiorillo, L.; Meto, A. Copper–Calcium Hydroxide and Permanent Electrophoretic Current for Treatment of Apical Periodontitis. Materials 2021, 14, 678. [Google Scholar] [CrossRef] [PubMed]
- Peters, O.A.; Schönenberger, K.; Laib, A. Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int. Endod. J. 2001, 34, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Shen, Y.; Peng, B.; Haapasalo, M. Root canal preparation of mandibular molars with 3 nickel-titanium rotary instruments: A micro-computed tomographic study. J. Endod. 2014, 40, 1860–1864. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Pérez, A.R.; Marceliano-Alves, M.F.; Provenzano, J.C.; Silva, S.G.; Pires, F.R.; Vieira, G.C.S.; Rôças, I.N.; Alves, F.R.F. What happens to unprepared root canal walls: A correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int. Endod. J. 2018, 51, 501–508. [Google Scholar] [CrossRef]
- Zehnder, M. Root Canal Irrigants. J. Endod. 2006, 32, 389–398. [Google Scholar] [CrossRef]
- Ram, Z. Effectiveness of root canal irrigation. Oral Surgery Oral Med. Oral Pathol. 1977, 44, 306–312. [Google Scholar] [CrossRef]
- Jiang, L.M.; Lak, B.; Eijsvogels, L.M.; Wesselink, P.; Van Der Sluis, L.W.M. Comparison of the cleaning efficacy of different final irrigation techniques. J. Endod. 2012, 38, 838–841. [Google Scholar] [CrossRef]
- Blank-Gonalves, L.M.; Nabeshima, C.K.; Martins, G.H.R.; MacHado, M.E.D.L. Qualitative analysis of the removal of the smear layer in the apical third of curved roots: Conventional irrigation versus activation systems. J. Endod. 2011, 37, 1268–1271. [Google Scholar] [CrossRef]
- Haupt, F.; Meinel, M.; Gunawardana, A.; Hülsmann, M. Effectiveness of different activated irrigation techniques on debris and smear layer removal from curved root canals: A SEM evaluation. Aust. Endod. J. 2020, 46, 40–46. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Lambrianidis, T.; Kastrinakis, E. Irrigant flow within a prepared root canal using various flow rates: A Computational Fluid Dynamics study. Int. Endod. J. 2009, 42, 144–155. [Google Scholar] [CrossRef]
- Dioguardi, M.; Crincoli, V.; Sovereto, D.; Caloro, G.A.; Aiuto, R.; Illuzzi, G.; Caponio, V.C.A.; Troiano, G.; De Lillo, A.; Ciavarella, D.; et al. Effectiveness of Vapor Lock Effect Removal in Endo Training Blocks: Manual Dynamic Agitation versus Passive Ultrasonic Irrigation. Appl. Sci. 2019, 9, 5411. [Google Scholar] [CrossRef] [Green Version]
- Gu, L.S.; Kim, J.R.; Ling, J.; Choi, K.K.; Pashley, D.H.; Tay, F.R. Review of Contemporary Irrigant Agitation Techniques and Devices. J. Endod. 2009, 35, 791–804. [Google Scholar] [CrossRef]
- Jiang, L.M.; Verhaagen, B.; Versluis, M.; van der Sluis, L.W.M. Evaluation of a Sonic Device Designed to Activate Irrigant in the Root Canal. J. Endod. 2010, 36, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Van Der Sluis, L.W.M.; Versluis, M.; Wu, M.K.; Wesselink, P.R. Passive ultrasonic irrigation of the root canal: A review of the literature. Int. Endod. J. 2007, 40, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, K.W.; Liebi, M.; Stauffacher, S.; Eick, S.; Lussi, A. Antibacterial Efficacy of a New Sonic Irrigation Device for Root Canal Disinfection. J. Endod. 2016, 42, 1799–1803. [Google Scholar] [CrossRef]
- De Gregorio, C.; Estevez, R.; Cisneros, R.; Heilborn, C.; Cohenca, N. Effect of EDTA, Sonic, and Ultrasonic Activation on the Penetration of Sodium Hypochlorite into Simulated Lateral Canals: An In Vitro Study. J. Endod. 2009, 35, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.A.; Walker, T.L.; Hutter, J.W.; Nicoll, B.K. Comparison of the cleaning efficacy of passive sonic activation and passive ultrasonic activation after hand instrumentation in molar root canals. J. Endod. 1999, 25, 735–738. [Google Scholar] [CrossRef] [Green Version]
- Rödig, T.; Bozkurt, M.; Konietschke, F.; Hülsmann, M. Comparison of the vibringe system with syringe and passive ultrasonic irrigation in removing debris from simulated root canal irregularities. J. Endod. 2010, 36, 1410–1413. [Google Scholar] [CrossRef]
- Urban, K.; Donnermeyer, D.; Schäfer, E.; Bürklein, S. Canal cleanliness using different irrigation activation systems: A SEM evaluation. Clin. Oral Investig. 2017, 21, 2681–2687. [Google Scholar] [CrossRef] [PubMed]
- Verstraeten, J.; Jacquet, W.; De Moor, R.J.G.; Meire, M.A. Hard tissue debris removal from the mesial root canal system of mandibular molars with ultrasonically and laser-activated irrigation: A micro-computed tomography study. Lasers Med. Sci. 2017, 32, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, A.D.; Williams, A.R. Effects of constraint on the oscillatory pattern of endosonic files. J. Endod. 1989, 15, 189–194. [Google Scholar] [CrossRef]
- Roy, R.A.; Ahmad, M.; Crum, L.A. Physical mechanisms governing the hydrodynamic response of an oscillating ultrasonic file. Int. Endod. J. 1994, 27, 197–207. [Google Scholar] [CrossRef]
- Retsas, A.; Koursoumis, A.; Tzimpoulas, N.; Boutsioukis, C. Uncontrolled Removal of Dentin during In Vitro Ultrasonic Irrigant Activation in Curved Root Canals. J. Endod. 2016, 42, 1545–1549. [Google Scholar] [CrossRef]
- Lea, S.C.; Felver, B.; Landini, G.; Walmsley, A.D. Ultrasonic scaler oscillations and tooth-surface defects. J. Dent. Res. 2009, 88, 229–234. [Google Scholar] [CrossRef]
- Peters, O.A.; Bardsley, S.; Fong, J.; Pandher, G.; Divito, E. Disinfection of root canals with photon-initiated photoacoustic streaming. J. Endod. 2011, 37, 1008–1012. [Google Scholar] [CrossRef]
- DiVito, E.; Peters, O.A.; Olivi, G. Effectiveness of the erbium: YAG laser and new design radial and stripped tips in removing the smear layer after root canal instrumentation. Lasers Med. Sci. 2012, 27, 273–280. [Google Scholar] [CrossRef]
- Lloyd, A.; Uhles, J.P.; Clement, D.J.; Garcia-Godoy, F. Elimination of intracanal tissue and debris through a novel laser-activated system assessed using high-resolution micro-computed tomography: A pilot study. J. Endod. 2014, 40, 584–587. [Google Scholar] [CrossRef] [PubMed]
- Lukač, N.; Muc, B.T.; Jezeršek, M.; Lukač, M. Photoacoustic Endodontics Using the Novel SWEEPS Er:YAG Laser modality. J. Laser Health Acad 2017, 1, 1–7. [Google Scholar]
- Galler, K.M.; Grubmüller, V.; Schlichting, R.; Widbiller, M.; Eidt, A.; Schuller, C.; Wölflick, M.; Hiller, K.A.; Buchalla, W. Penetration depth of irrigants into root dentine after sonic, ultrasonic and photoacoustic activation. Int. Endod. J. 2019, 52, 1210–1217. [Google Scholar] [CrossRef]
- Yang, Q.; Liu, M.W.; Zhu, L.X.; Peng, B. Micro-CT study on the removal of accumulated hard-tissue debris from the root canal system of mandibular molars when using a novel laser-activated irrigation approach. Int. Endod. J. 2020, 53, 529–538. [Google Scholar] [CrossRef]
- Wang, X.N.; Shi, J. Shock wave-enhanced emission photoacoustic streaming versus photon-induced photoacoustic streaming modes for clearing root canal bacteria using erbium-doped yttrium aluminum garnet lasers: An in vitro study. BMC Oral Health 2019. preprint. [Google Scholar] [CrossRef]
- Căpută, P.E.; Retsas, A.; Kuijk, L.; de Paz, L.E.C.; Boutsioukis, C. Ultrasonic Irrigant Activation during Root Canal Treatment: A Systematic Review. J. Endod. 2019, 45, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Rengo, C.; Spagnuolo, G.; Ametrano, G.; Juloski, J.; Rengo, S.; Ferrari, M. Micro-computerized tomographic analysis of premolars restored with oval and circular posts. Clin. Oral Investig. 2014, 18, 571–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riccitiello, F.; Amato, M.; Leone, R.; Spagnuolo, G.; Sorrentino, R. In vitro Evaluation of the Marginal Fit and Internal Adaptation of Zirconia and Lithium Disilicate Single Crowns: Micro-CT Comparison Between Different Manufacturing Procedures. Open Dent. J. 2018, 12, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Vertucci, F.J. Root canal anatomy of the human permanent teeth. Oral Surg. Oral Med. Oral Pathol. 1984, 58, 589–599. [Google Scholar] [CrossRef]
- Widbiller, M.; Eidt, A.; Hiller, K.-A.; Buchalla, W.; Schmalz, G.; Galler, K.M. Ultrasonic activation of irrigants increases growth factor release from human dentine. Clin. Oral Investig. 2017, 21, 879–888. [Google Scholar] [CrossRef]
- Widbiller, M.; Eidt, A.; Lindner, S.R.; Hiller, K.-A.; Schweikl, H.; Buchalla, W.; Galler, K.M. Dentine matrix proteins: Isolation and effects on human pulp cells. Int. Endod. J. 2018, 51, 278–290. [Google Scholar] [CrossRef] [Green Version]
- Zorzin, J.; Wießner, J.; Wießner, T.; Lohbauer, U.; Petschelt, A.; Ebert, J. Removal of radioactively marked calcium hydroxide from the root canal: Influence of volume of irrigation and activation. J. Endod. 2016, 42, 637–640. [Google Scholar] [CrossRef]
- Cruz, A.; Vera, J.; Gascón, G.; Palafox-Sánchez, C.A.; Amezcua, O.; Mercado, G. Debris remaining in the apical third of root canals after chemomechanical preparation by using sodium hypochlorite and glyde: An in vivo study. J. Endod. 2014, 40, 1419–1423. [Google Scholar] [CrossRef]
- Robinson, J.P.; Lumley, P.J.; Cooper, P.R.; Grover, L.M.; Walmsley, A.D. Reciprocating root canal technique induces greater debris accumulation than a continuous rotary technique as assessed by 3-dimensional micro-computed tomography. J. Endod. 2013, 39, 1067–1070. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Wu, M.K.; Wesselink, P.R. The efficacy of ultrasonic irrigation to remove artificially placed dentine debris from different-sized simulated plastic root canals. Int. Endod. J. 2004, 37, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Van Der Sluis, L.W.M.; Wu, M.K.; Wesselink, P.R. The efficacy of ultrasonic irrigation to remove artificially placed dentine debris from human root canals prepared using instruments of varying taper. Int. Endod. J. 2005, 38, 764–768. [Google Scholar] [CrossRef]
- Kurzmann, C.; Meire, M.A.; Lettner, S.; Farmakis, E.T.R.; Moritz, A.; De Moor, R.J.G. The efficacy of ultrasonic and PIPS (photon-induced acoustic streaming) irrigation to remove artificially placed dentine debris plugs out of an artificial and natural root model. Lasers Med. Sci. 2020, 35, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, A.; Cox, T.C.; Paranjpe, A.; Flake, N.M.; Cohenca, N.; Johnson, J.D. Efficacy of sonic and ultrasonic activation for removal of calcium hydroxide from mesial canals of mandibular molars: A microtomographic study. J. Endod. 2011, 37, 235–238. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, R.L.; Guerisoli, D.M.Z.; Duque, J.A.; Alcalde, M.P.; Onoda, H.K.; Domingues, F.H.F.; Vivan, R.R.; Duarte, M.A.H. Computed microtomography evaluation of calcium hydroxide-based root canal dressing removal from oval root canals by different methods of irrigation. Microsc. Res. Tech. 2019, 82, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.J.N.L.; Carvalho, C.R.; Belladonna, F.G.; Prado, M.C.; Lopes, R.T.; De-Deus, G.; Moreira, E.J.L. Micro-CT evaluation of different final irrigation protocols on the removal of hard-tissue debris from isthmus-containing mesial root of mandibular molars. Clin. Oral Investig. 2019, 23, 681–687. [Google Scholar] [CrossRef]
- Leoni, G.B.; Versiani, M.A.; Silva-Sousa, Y.T.; Bruniera, J.F.B.; Pécora, J.D.; Sousa-Neto, M.D. Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int. Endod. J. 2017, 50, 398–406. [Google Scholar] [CrossRef]
- Cesario, F.; Duarte, M.A.H.; Duque, J.A.; Alcalde, M.P.; De Andrade, F.B.; So, M.V.R.; De Vasconcelos, B.C.; Vivan, R.R. Comparisons by microcomputed tomography of the efficiency of different irrigation techniques for removing dentinal debris from artificial grooves. J. Conserv. Dent. 2018, 21, 383–387. [Google Scholar] [CrossRef]
- Huang, T.Y.; Gulabivala, K.; Ng, Y.L. A bio-molecular film ex-vivo model to evaluate the influence of canal dimensions and irrigation variables on the efficacy of irrigation. Int. Endod. J. 2008, 41, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Gulabivala, K.; Ng, Y.-L.; Gilbertson, M.; Eames, I. The fluid mechanics of root canal irrigation. Physiol. Meas. 2010, 31, 49–84. [Google Scholar] [CrossRef] [Green Version]
- Donnermeyer, D.; Wyrsch, H.; Bürklein, S.; Schäfer, E. Removal of Calcium Hydroxide from Artificial Grooves in Straight Root Canals: Sonic Activation Using EDDY Versus Passive Ultrasonic Irrigation and XPendo Finisher. J. Endod. 2019, 45, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Swimberghe, R.C.D.; De Clercq, A.; De Moor, R.J.G.; Meire, M.A. Efficacy of sonically, ultrasonically and laser-activated irrigation in removing a biofilm-mimicking hydrogel from an isthmus model. Int. Endod. J. 2019, 52, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Hage, W.; De Moor, R.J.G.; Hajj, D.; Sfeir, G.; Sarkis, D.K.; Zogheib, C. Impact of Different Irrigant Agitation Methods on Bacterial Elimination from Infected Root Canals. Dent. J. 2019, 7, 64. [Google Scholar] [CrossRef] [Green Version]
- Boutsioukis, C.; Psimma, Z.; Kastrinakis, E. The effect of flow rate and agitation technique on irrigant extrusion ex vivo. Int. Endod. J. 2014, 47, 487–496. [Google Scholar] [CrossRef]
- Macedo, R.G.; Verhaagen, B.; Rivas, D.F.; Versluis, M.; Wesselink, P.; Van Der Sluis, L. Cavitation measurement during sonic and ultrasonic activated irrigation. J. Endod. 2014, 40, 580–583. [Google Scholar] [CrossRef]
- Eggmann, F.; Vokac, Y.; Eick, S.; Neuhaus, K.W. Sonic irrigant activation for root canal disinfection: Power modes matter! BMC Oral Health 2020, 20, 102. [Google Scholar] [CrossRef] [Green Version]
- Kirsch, J.; Sina Reinauer, K.; Meissner, H.; Dannemann, M.; Kucher, M.; Modler, N.; Hannig, C.; Weber, M.-T. Ultrasonic and sonic irrigant activation in endodontics: A fractographic examination. Dtsch. Zahnärztl Z. Int. 2019, 1, 209–221. [Google Scholar] [CrossRef]
- Pashley, E.L.; Birdsong, N.L.; Bowman, K.; Pashley, D.H. Cytotoxic effects of NaOCl on vital tissue. J. Endod. 1985, 11, 525–528. [Google Scholar] [CrossRef]
- Gernhardt, C.R.; Eppendorf, K.; Kozlowski, A.; Brandt, M. Toxicity of concentrated sodium hypochlorite used as an endodontic irrigant. Int. Endod. J. 2004, 37, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Hülsmann, M.; Hahn, W. Complications during root canal irrigation—Literature review and case reports. Int. Endod. J. 2000, 33, 186–193. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Tzimpoulas, N. Uncontrolled Removal of Dentin during in Vitro Ultrasonic Irrigant Activation. J. Endod. 2016, 42, 289–293. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Verhaagen, B.; Walmsley, A.D.; Versluis, M.; Van Der Sluis, L.W.M. Measurement and visualization of file-to-wall contact during ultrasonically activated irrigation in simulated canals. Int. Endod. J. 2013, 46, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Plotino, G.; Grande, N.M.; Mercade, M.; Cortese, T.; Staffoli, S.; Gambarini, G.; Testarelli, L. Efficacy of sonic and ultrasonic irrigation devices in the removal of debris from canal irregularities in artificial root canals. J. Appl. Oral Sci. 2019, 27, e20180045. [Google Scholar] [CrossRef]
- Lukač, N.; Jezeršek, M. Amplification of pressure waves in laser-assisted endodontics with synchronized delivery of Er:YAG laser pulses. Lasers Med. Sci. 2018, 33, 823–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohl, C.-D.; Arora, M.; Dijkink, R.; Janve, V.; Lohse, D. Surface cleaning from laser-induced cavitation bubbles. Appl. Phys. Lett. 2006, 89, 074102. [Google Scholar] [CrossRef]
- Jezeršek, M.; Lukač, N.; Lukač, M. Measurement of Simulated Debris Removal Rates in an Artificial Root Canal to Optimize Laser-Activated Irrigation Parameters. Lasers Surg. Med. 2021, 53, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Parashos, P.; Messer, H.H. Rotary NiTi Instrument Fracture and its Consequences. J. Endod. 2006, 32, 1031–1043. [Google Scholar] [CrossRef]
- Mcguigan, M.B.; Louca, C.; Duncan, H.F. The impact of fractured endodontic instruments on treatment outcome. Br. Dent. J. 2013, 214, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Arslan, H.; Capar, I.D.; Saygili, G.; Gok, T.; Akcay, M. Effect of photon-initiated photoacoustic streaming on removal of apically placed dentinal debris. Int. Endod. J. 2014, 47, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Cerroni, L.; Palopoli, P.; Olivi, G.; Olivi, M.; Buoni, C.; Cianconi, L. FESEM evaluation of smear layer removal from conservatively shaped canals: Laser activated irrigation (PIPS and SWEEPS) compared to sonic and passive ultrasonic activation—an ex vivo study. BMC Oral Health 2021, 21, 81. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Widbiller, M.; Keim, L.; Schlichting, R.; Striegl, B.; Hiller, K.-A.; Jungbauer, R.; Buchalla, W.; Galler, K.M. Debris Removal by Activation of Endodontic Irrigants in Complex Root Canal Systems: A Standardized In-Vitro-Study. Appl. Sci. 2021, 11, 7331. https://doi.org/10.3390/app11167331
Widbiller M, Keim L, Schlichting R, Striegl B, Hiller K-A, Jungbauer R, Buchalla W, Galler KM. Debris Removal by Activation of Endodontic Irrigants in Complex Root Canal Systems: A Standardized In-Vitro-Study. Applied Sciences. 2021; 11(16):7331. https://doi.org/10.3390/app11167331
Chicago/Turabian StyleWidbiller, Matthias, Lukas Keim, Ralf Schlichting, Birgit Striegl, Karl-Anton Hiller, Rebecca Jungbauer, Wolfgang Buchalla, and Kerstin M. Galler. 2021. "Debris Removal by Activation of Endodontic Irrigants in Complex Root Canal Systems: A Standardized In-Vitro-Study" Applied Sciences 11, no. 16: 7331. https://doi.org/10.3390/app11167331
APA StyleWidbiller, M., Keim, L., Schlichting, R., Striegl, B., Hiller, K. -A., Jungbauer, R., Buchalla, W., & Galler, K. M. (2021). Debris Removal by Activation of Endodontic Irrigants in Complex Root Canal Systems: A Standardized In-Vitro-Study. Applied Sciences, 11(16), 7331. https://doi.org/10.3390/app11167331