
The Impact of Calcitriol on Orthodontic Tooth Movement: A Cumulative Systematic Review and Meta-Analysis

 ,
,  ,
,  and
and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
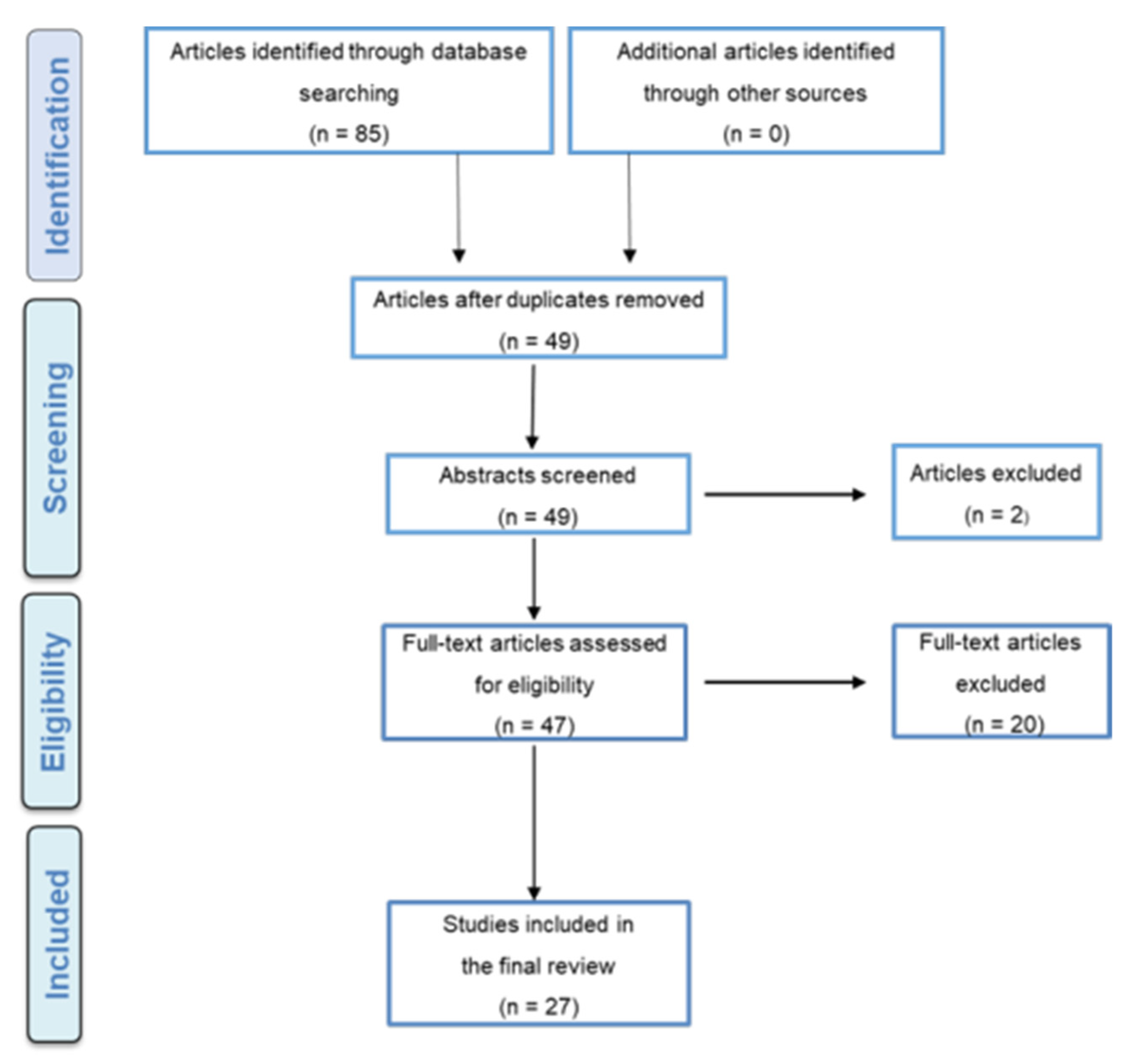
2.3. Studies Selection
2.4. Data extraction Process and Quality Assessment
2.5. Meta-Analysis and Quantitative Data Synthesis
3. Results
3.1. Level of Quality and Recommendation
3.2. Structured Assessment Review
3.3. Animal Studies
3.4. Human In Vitro Studies and Clinical Trials
3.5. Quantitative Data Synthesis and Meta-Analysis Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fisher, M.A.; Wenger, R.M.; Hans, M.G. Pretreatment characteristics associated with orthodontic treatment duration. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Mavreas, D.; Athanasiou, A.E. Factors affecting the duration of orthodontic treatment: A systematic review. Eur. J. Orthod. 2008, 30, 386–395. [Google Scholar] [CrossRef] [Green Version]
- Geiger, A.M.; Gorelick, L.; Gwinnett, A.J.; Benson, B.J. Reducing white spot lesions in orthodontic populations with fluoride rinsing. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 403–407. [Google Scholar] [CrossRef]
- Pandis, N.; Nasika, M.; Polychronopoulou, A.; Eliades, T. External apical root resorption in patients treated with conventional and self-ligating brackets. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 646–651. [Google Scholar] [CrossRef]
- Long, H.; Pyakurel, U.; Wang, Y.; Liao, L.; Zhou, Y.; Lai, W. Interventions for accelerating orthodontic tooth movement: A systematic review. Angle Orthod. 2013, 83, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Angbawi, A.; Mcintyre, G.T.; Fleming, P.S.; Bearn, D.R. Non-surgical adjunctive interventions for accelerating tooth movement in patients undergoing fixed orthodontic treatment. Cochrane Database Syst. Rev. 2015, 11, CD010887. [Google Scholar] [CrossRef] [PubMed]
- Sivarajan, S.; Doss, J.G.; Papageorgiou, S.N.; Cobourne, M.T.; Wey, M.C. Mini-implant supported canine retraction with micro-osteoperforation: A split-mouth randomized clinical trial. Angle Orthod. 2019, 89, 183–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalemaj, Z.; Debernardl, C.L.; Buti, J. Efficacy of surgical and non-surgical interventions on accelerating orthodontic tooth movement: A systematic review. Eur. J. Oral Implantol. 2015, 8, 9–24. [Google Scholar]
- Hoogeveen, E.J.; Jansma, J.; Ren, Y. Surgically facilitated orthodontic treatment: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 51–64. [Google Scholar] [CrossRef]
- Nayak, K.; Galil, W.; Wiltshire, P. Molecular Biology of Orthodontic Tooth Movement. J. Dent. Oral Health 2013, 1, 1–6. [Google Scholar]
- Roodman, G.D. Role of cytokines in the regulation of bone resorption. Calcif. Tissue Int. 1993, 53, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Younis, L.T.; Masood, M.; Ismail, F.; Bahnasi, E. The Role of Components and Molecules of Periodontal Ligament in Orthodontic Tooth Movement. Asian J. Dent. Res. 2019, 2, 1–12. [Google Scholar]
- Kouskoura, T.; Katsaros, C.; von Gunten, S. The potential use of pharmacological agents to modulate orthodontic tooth movement (OTM). Front. Physiol. 2017, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogawa, M.; Findlay, D.; Anderson, P.H.; Ormsby, R.; Vincent, C.; Morris, H.A.; Atkins, G.J. Osteoclastic Metabolism of 25(OH)-Vitamin D3: A Potential Mechanism for Optimization of Bone Resorption. Endocrinology 2010, 10, 4613–4625. [Google Scholar] [CrossRef] [Green Version]
- Reichel, H.; Koeffl, H.; Norman, A. The role of the vitamin D3 endocrine system in health and disease. N. Engl. J. Med. 1989, 320, 980–991. [Google Scholar] [CrossRef] [PubMed]
- Posa, F.; Di Benedetto, A.; Colaianni, G.; Cavalcanti-Adam, E.; Brunetti, G.; Porro, C.; Trotta, T.; Grano, M.; Mori, G. Vitamin D3 effects on osteoblastic differentiation of mesenchymal stem cells from dental tissues. Stem Cells Int. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kale, S.; Kocadereli, I.; Atilla, P.; Asan, E. Comparison of the effects of 1,25 dihydroxycholecalciferol and prostaglandin E2 on orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 607–614. [Google Scholar] [CrossRef]
- Kawakami, M.; Takano-Yamamoto, T. Local injection of 1,25-dihydroxyvitamin D3 enhanced bone formation for tooth stabilization after experimental tooth movement in rats. J. Bone Miner. Metab. 2004, 22, 541–546. [Google Scholar] [CrossRef]
- Blanco, J.; Diaz, R.; Gross, H. Efecto de laadministración sistémica del1,25Dihidrxicolecalciferol sobrelavelocidad del movimiento ortodóncico en humanos. Estudio Clínico Revista Odontos 2001, 8, 13–24. [Google Scholar]
- Guyatt, G.; Oxman, A.; Vist, G.; Kunz, R.; Falck-Ytter, Y.; Alnoso-Coelle, P.; Schünemann, H.J. An emerging consensus on rating quality of evidence and strength of recommendations. Br. Med. J. 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- OCEBM Levels of Evidence Working Group. The Oxford 2011 Levels of Evidence. Oxford Centre for Evidence-Based Medicine. 2016. Available online: http://www.cebm.net/index.aspx?o=5653 (accessed on 23 June 2020).
- Ratri Nareswari, R.; Narmada, I.; Djaharu’ddin, I.; Putrani, N.; Nugrada, A. Effect of vitamin D3 administration on vascular endothelial growth factor expression and angiogenesis number in orthodontic tooth movement of pregnant Wistar rat. J. Postgrad. Med. Inst. 2019, 33, 182–188. [Google Scholar]
- Cui, J.; Li, J.; Wang, W.; Han, X.; Sun, J.; Feng, W.; Liu, B.; Liu, H.; Amizuka, N.; Li, M. The effect of calcitriol on high mobility group box 1 expression in periodontal ligament cells during orthodontic tooth movement in rats. J. Mol. Histol. 2016, 47, 221–228. [Google Scholar] [CrossRef]
- Kawakami, M. Effects of local application of 1,25 (OH)2D3 on experimental tooth movement in rats. J. Osaka 1990, 35, 128–146. [Google Scholar]
- Bielaczyc, A.; Golebiewska, M. Ultrastructural changes of a tooth root in young rats fed a low calcium and vitamin D3-deficient diet. Roczniki Akademii Medycznej w Bialymstoku 1990, 42, 153–158. [Google Scholar]
- Baran, S.; Hamamci, O.; Akalar, M. An investigation of the effects of the local use of 1:25 dihydroxycholecalciferol (1:25 D) on tension sites during experimental tooth movement in rats. J. Marmara Uni. Dent. Fac. 1996, 2, 557–561. [Google Scholar]
- Takano-Yamamoto, T.; Kawakami, M.; Kobayshiro, Y.; Sakuda, M. The Effect of Local Application of 1,25-Dihydroxycholecalciferol on Osteoclast Numbers in Orthodontically Treated Rats. J. Dent. Res. 1992, 71, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.K.; Sinclair, P.M. The local use of vitamin D3 to increase the rate of orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 278–284. [Google Scholar] [CrossRef]
- Yamasaki, K. Effects of vitamin D3 on orthodontic tooth movement in rats. Kokubyo Gakkai Zasshi 1976, 43, 41–63. [Google Scholar] [CrossRef]
- Imazu, H. Histo-biochemical changes during tooth movement under controlled fed rat. Gifu Shika Gakkai Zasshi 1984, 11, 401–423. [Google Scholar]
- Kawal, H. Tooth movement in rats during a calcium and vitamin D3 deficient regimen. Gifu Shika Gakkai Zasshi 1984, 11, 380–400. [Google Scholar]
- Zhang, D.; Lorenzo, J. 1,25(OH)2 vitamin D33 induces IL-1 alpha mRNA expression from osteoblastic-like and bone marrow co-culture cells. Chin. J. Stomatol. 1998, 33, 375–377. [Google Scholar]
- Basdra, E.K.; Komposch, G. Osteoblast-like properties of human periodontal ligament cells: An in vitro analysis. Eur. J. Orthod. 1997, 19, 615–621. [Google Scholar] [CrossRef]
- Tehranchi, A.; Sadighnia, A.; Younessian, F.; Abdi, A.; Shirvani, A. Correlation of Vitamin D3 status and orthodontic-induced external apical root resorption. Dent. Res. J. 2017, 14, 403–411. [Google Scholar]
- Fontana, M.L.S.S.N.; De Souza, C.M.H.; Bernardino, J.F.; Hoette, F.; Hoette, M.L.; Thum, L.; Terumi, O.O.; Capelozza Filho, L.; Olandoski, M.; Trevilatto, P.C. Association analysis of clinical aspects and vitamin D3 receptor gene polymorphism with external apical root resorption in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Kaklamanos, E.G.; Makrygiannakis, M.A.; Athanasiou, A.E. Does medication administration affect the rate of orthodontic tooth movement and root resorption development in humans? A systematic review. Eur. J. Orthod. 2019, 42, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, K.; Mando, M. Effect of Drugs on Orthodontic Tooth Movement in Human Beings: A Systematic Review of Randomized Clinical Trials. Open Dent. J. 2019, 13, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Kacprzak, A.; Strzecki, A. Methods of accelerating orthodontic tooth movement: A review of contemporary literature. Dent. Med. Probl. 2018, 55, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Batmaraj, U. The effects of commonly used drugs on orthodontic tooth movement: A systematic review. Asian J. Pharm. Clin. Res. 2014, 7, 10–14. [Google Scholar]
- Camacho, A.D. Dental movement acceleration: Literature review by an alternative scientific evidence method. World J. Methodol. 2014, 4, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Nimeri, G.; Kau, C.; Abou-Kheir, N.; Corona, R. Acceleration of tooth movement during orthodontic treatment-A frontier in orthodontics. Prog. Orthod. 2013, 14, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Tyrovola, J.; Spyropoulos, M. Effects of drugs and systemic factors on orthodontic treatment. Quintessence Int. 2001, 32, 365–371. [Google Scholar] [PubMed]
- Al-Hasani, N.R.; Al-Bustani, A.I.; Ghareeb, M.M.; Hussain, S.A. Clinical efficacy of locally injected calcitriol in orthodontic tooth movement. Int. J. Pharm. Pharm. Sci. 2011, 3, 139–143. [Google Scholar]
- Iosub Ciur, M.D.; Zetu, I.N.; Haba, D.; Viennot, S.; Bourgeois, D.; Andrian, S. Evaluation of the Influence of Local Administration of Vitamin D3 on the Rate of Orthodontic Tooth Movement. Rev. Med. Chir. Soc. Med. Nat. Iasi. 2016, 120, 694–699. [Google Scholar] [PubMed]
- Bartzela, T.; Türp, J.C.; Motschall, E.; Maltha, J.C. Medication effects on the rate of orthodontic tooth movement: A systematic literature review. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 16–26. [Google Scholar] [CrossRef]
- Makrygiannakis, M.A.; Kaklamanos, E.G.; Athanasiou, A.E. Does common prescription medication affect the rate of orthodontic tooth movement? A systematic review. Eur. J. Orthod. 2018, 40, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Leethanakul, C.; Kanokkulchai, S.; Pongpanich, S.; Leepong, N.; Charoemratrote, C. Interseptal bone reduction on the rate of maxillary canine retraction. Angle Orthod. 2014, 84, 839–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takano-Yamamoto, T.; Kawakami, M.; Yamashiro, T. Effect of Age on the Rate of Tooth Movement in Combination with Local Use of 1,25(OH) 2D3 and Mechanical Force in the Rat. J. Dent. Res. 1992, 71, 1487–1492. [Google Scholar] [CrossRef]
- Aboul-Ela, S.M.B.E.D.; El-Beialy, A.R.; El-Sayed, K.M.F.; Selim, E.M.N.; El-Mangoury, N.H.; Mostafa, Y.A. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 252–259. [Google Scholar] [CrossRef]
- Da Silva Sousa, M.V.; Scanavini, M.A.; Sannomiya, E.K.; Velasco, L.G.; Angelieri, F. Influence of low-level laser on the speed of orthodontic movement. Photomed. Laser Surg. 2011, 29, 191–196. [Google Scholar] [CrossRef]
- Eltimamy, A.; El-Sharaby, F.A.; Eid, F.H.; El-Dakrory, A.E. The effect of local pharmacological agents in acceleration of orthodontic tooth movement: A systematic review. Open Access Maced. J. Med. Sci. 2019, 7, 882–886. [Google Scholar] [CrossRef] [Green Version]
- Frost, H.M. The regional acceleratory phenomenon. Orthop. Clin. N. Am. 1981, 12, 725–726. [Google Scholar]
- Roodman, G.D.; Ibbotson, K.J.; MacDonald, B.R.; Kuehl, T.J.; Mundy, G.R. 1, 25-Dihydroxyvitamin D3 causes formation of multinucleated cells with several osteoclast characteristics in cultures of primate marrow. Proc. Natl. Acad. Sci. USA 1985, 82, 8213–8217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, K.; Chambers, T.J. Generation of osteoclasts in cultures of rabbit bone marrow and spleen cells. J. Cell. Physiol. 1987, 132, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Yamana, H.; Yoshiki, S.; Roodman, G.D.; Mundy, G.R.; Jnoes, S.J.; Boyde, A.; Suda, T. Osteoclast-like cell formation and its regulation by osteotropic hormones in mouse bone marrow cultures. Endocrinology 1988, 122, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, M.L.; Saravana Pandian, K. Acceleration of tooth movement during orthodontic treatment-A frontier in orthodontics. J. Pharm. Sci. Res. 2017, 9, 741–744. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Design and Method | Sample Size | Aims | Study Duration | Intervention | Orthodontic Intervention | Findings | Level of Evidence † | Level of Recommendation †† |
|---|---|---|---|---|---|---|---|---|---|
| Ratri Nareswari et al. (2019) [22] | In vivo experimental study, histological and immuohistochemistry. | 28 female Wistar rats | To investigate the effect of vitamin D3 on vascular endothelial growth factor expression during orthodontic tooth movement. | 14 days | Vitamin D3 (0.2 mg/kg) was given every 3 days. | Coil spring (Ni-Ti) was inserted between maxillary central incisor and 1st left maxillary molar. | Vitamin D3 administration did not significantly increase VEGF expression and angiogenesis number orthodontic tooth movement. | 5 | ⊕⊕⊕ |
| Cui et al. (2016) [23] | In vivo experimental study and immunohistochemistry. | 30 male Wistar rats | To investigate the effect of 1,25(OH)2D3 on HMGB1 expression by periodontal ligament cells in an orthodontic rat model. | 28 days | Administered with 1,25(OH)2D3 (100 ng/kg body weight) was adminstarted once every other day. | NiTi coil spring on the maxillary first molar | Indicates that administration of 1,25(OH)2D3 might create a favorable environment for orthodontic tooth movement. | 5 | ⊕⊕⊕⊕ |
| Kawakami and Takano-Yamamoto (1990) [24] | In vivo experimental study and histomorphometric analysis | 16 rats male Wistar rats | To investigate the effect local injection of vitamin D3 during tooth movement. | 14 days | 20 µL of 1,25(OH)2D3 | A piece of orthodontic elastic | Significant increase in mineral appositional rate associated with increased osteoblast surface value. | 5 | ⊕⊕⊕ |
| Kale et al. (2004) [17] | In vivo experimental study and histological examination. | 37 Wistar rats | To investigate the effect of local administrations of prostaglandin E2 and 1,25-dihydroxycholecalciferol (1,25-DHCC) on orthodontic tooth movement in rats. | 9 days | Prostaglandin E2 (PGE2) and 1,25-dihydroxycholecalciferol (1,25-DHCC) | A helical loop stainless steel spring | Both Prostaglandin E2 and 1,25-DHCC enhanced the amount of tooth movement significantly. | 5 | ⊕⊕ |
| Bielaczyc and Golebiewska (1997) [25] | In vivo experimental study with scanning microscopy observation. | 20 young Wistar rats | To investigate the structural changes on the roots in rats fed by deficient diet with low calcium and vitamin D3. | Inaccessible | Feeding a low calcium and vitamin D3. | Inaccessible | Increased cementolysis and decreased mineralization of cementum and dentin. | 5 | ⊕⊕ |
| Baran et al. (1996) [26] | In vivo experimental study and histological examination. | 32 Wistar albino rats | To assess the effects of 1:25 dihydroxychole-calciferol, one of the most potent osteoclastic activity stimulants. | Inaccessible | Administration of 1:25 dihydroxychole-calciferol. | Inaccessible | Higher area of unilateral apposition was observed in the experimental group. | 5 | ⊕⊕ |
| Takano-Yamamoto et al. (1992) | In vivo experimental study and histological examination on rats. | Experiment I: 112 rats divided into two groups. Experiment II: 80 rats. | To investigate the effect of local injection of 1,25-(OH)2D3 on osteoclast numbers during tooth movement. | In experiment 1: 3 days. In experiment 2: 15 days. | 20 µL of 1,25(OH)2D3 was injected locally with phosphate-buffered saline (PBS) on the control side. | Elastic band was placed between the first and the second upper molars. | Increased osteoclast number and bone resorption. | 5 | ⊕⊕⊕⊕ |
| Takano-Yamamoto et al. (1992) [27] | In vivo experimental study and blood chemistry | 30 seven week-old and 30 28 week-old male Wistar rats. | To investigate the effect of local injection of vitamin D3 in young and mature rats during tooth movement. | 21 days | 20 µL of 1,25(OH)2D3 was injected locally with phosphate-buffered saline (PBS) on the control side. | A coil spring was used with a force ranging between 5 g and 30 g. | No change was observed in serum calcium, phosphate, and alkaline phosphatase activity. | 5 | ⊕⊕⊕ |
| Kawakami (1990) [24] | In vivo experimental study, fluorescent labeling and quantitative histology on rats. | Wistar male rats (the number was not accessible) | To investigate the effect of locally injected vitamin D3, on the rate of tooth movement in rats. | 20 days | 20 µL was locally injected. | A piece of orthodontic helical spring was used to move the first molar. | The rate of tooth movement was increased. | 5 | ⊕⊕⊕ |
| Collins and Sinclair (1988) [28] | In vivo experimental study with histological examination and blood chemistry. | 10 cats, 5 cats pilot study | To investigate the effect of local administration of vitamin D3 on the rate of tooth movement. | 21 days | Injection of vitamin D3 metabolite into PDL. | Canine retraction with light wire retraction spring. | The rate of tooth movement and osteoclasts number was increased. | 5 | ⊕⊕⊕ |
| Authors Years | Type of Study | Active Substance | Model | Findings | Level of Evidence † | Level of Recommendation †† |
|---|---|---|---|---|---|---|
| Zhang and Lorenzo (1998) [32] | Histochemical and biochemical study | Vitamin 1,25(OH) 2D3 and Interleukin-1 (IL-1) | IL-1 alpha mRNA expression in bone marrow and osteoblastic cell co-cultures by semi-quantitative RT-PCR. | IL-1 involved in osteoclast formation induced by 1,25(OH)2D3 and IL-1 stimulate osteoclast progenitor proliferation. | 5 | ⊕⊕⊕⊕ |
| Basdra and Komposch (1997) [33] | Histochemical and biochemical study | 1α,25-dihydroxyvitamin D3 | PDL fibroblasts isolated from human periodontium (the roots of healthy extracted third molar) were cultured. | Human PDL fibroblast exhibit phenotypic characteristics similar to that of osteoblast-like cells and have the potential to differentiate into osteoblasts and/or cementoblast. | 5 | ⊕⊕⊕⊕ |
| Authors Years | Type of Study | Active Substance | Number of Participants | Gender | Age of Participants (Range) | Group Characteristics | Results | Level of Evidence † | Level of Recommendation †† | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 3 | |||||||||
| Tehranchi et al. (2017) [34] | Cross sectional study | Vitamin D3 | 34 | 23.5% males and 76.5% females | 12–23 years | Class I 13 (38.2%) | Class II 18 (53%) | Class III 3 (8%) | Vitamin D3 level is not among the clinical variables that are potential contributors for EARR. | 3 | ⊕⊕⊕ |
| Fontana et al. (2012) [35] | Cross sectional study | Vitamin D3 | 377 | 44.8% males and 55.2% females | 8–21 years | 160 (42%) with EARR ≤1.43 mm | 179(47%) with EARR>1.43 mm | 38(11%) untreated subjects | Vitamin D3 receptor polymorphism was associated with EARR in orthodontic patients | 2 | ⊕⊕⊕⊕ |
| Authors/Years | Findings |
|---|---|
| Kaklamanos et al. (2019) [36] | The rate of orthodontic tooth movement may be affected by consuming specific analgesics for a few days |
| Khalaf and Mando (2019) [37] | The rate of tooth movement was reduced by acetylsalicylic acid and ibuprofen whereas no impact on orthodontic tooth movement was observed when paracetamol, Rofecoxib, and tenoxicam were consumed. |
| Kacprzak and Strzecki (2018) [38] | In adults, corticotomy and its modifications might prove to be a useful in decreasing the duration of orthodontic treatment |
| Kouskoura et al. (2017) [13] | Many drugs can and will influence both bone metabolism and can influence cellular functions |
| Batmaraj (2014) [39] | Beneficial and harmful effects and clinical efficacy of new drugs must be tested and investigated. |
| Camacho (2014) [40] | Level of evidence was as follows: surgery first followed by low level laser beam application, corticotomy, and periodontal distraction |
| Nimeri et al. (2013) [41] | Piezocision technique is an effective approach to accelerate tooth movement |
| Tyrovola and Spyropoulos (2001) [42] | Hormones and drugs such as estrogen, androgen, bisphosphonates, vitamin D3, and calcitonin could delay orthodontic tooth movement, whereas thyroid hormones and corticosteroids might enhance orthodontic tooth movement. |
| Authors/Year | Study Design | Country | Aim (s) | Sample Size | Gender | Age (Range) | Level of Evidence † | Level of Recommendation †† |
|---|---|---|---|---|---|---|---|---|
| Al-Hasani et al. (2011) [43] | RCT (for dosage) Split mouth | Iraq | To investigate the effect of locally injected vitamin D3 (calcitriol) on the rate of orthodontic tooth movement. | 15 | Not reported | 17–28 years | 1 | ⊕⊕⊕⊕ |
| Iosub Ciur et al. (2016) [44] | RCT (for dosage) Split mouth | France | To investigate the effect of local administration of vitamin D3 on the dental roots and the rate of orthodontic tooth movement. | 4 | M:2(50%) F:2(50%) | 13–34 years | 1 | ⊕⊕⊕⊕ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Attar, A.; Abid, M.; Dziedzic, A.; Al-Khatieeb, M.M.; Seppala, M.; Cobourne, M.T.; Abed, H. The Impact of Calcitriol on Orthodontic Tooth Movement: A Cumulative Systematic Review and Meta-Analysis. Appl. Sci. 2021, 11, 8882. https://doi.org/10.3390/app11198882
Al-Attar A, Abid M, Dziedzic A, Al-Khatieeb MM, Seppala M, Cobourne MT, Abed H. The Impact of Calcitriol on Orthodontic Tooth Movement: A Cumulative Systematic Review and Meta-Analysis. Applied Sciences. 2021; 11(19):8882. https://doi.org/10.3390/app11198882
Chicago/Turabian StyleAl-Attar, Ali, Mushriq Abid, Arkadiusz Dziedzic, Mustafa M. Al-Khatieeb, Maisa Seppala, Martyn T. Cobourne, and Hassan Abed. 2021. "The Impact of Calcitriol on Orthodontic Tooth Movement: A Cumulative Systematic Review and Meta-Analysis" Applied Sciences 11, no. 19: 8882. https://doi.org/10.3390/app11198882
APA StyleAl-Attar, A., Abid, M., Dziedzic, A., Al-Khatieeb, M. M., Seppala, M., Cobourne, M. T., & Abed, H. (2021). The Impact of Calcitriol on Orthodontic Tooth Movement: A Cumulative Systematic Review and Meta-Analysis. Applied Sciences, 11(19), 8882. https://doi.org/10.3390/app11198882