
Bacterial Biofilm Growth on Various Dental Stabilization Systems for Avulsed and Luxated Teeth


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
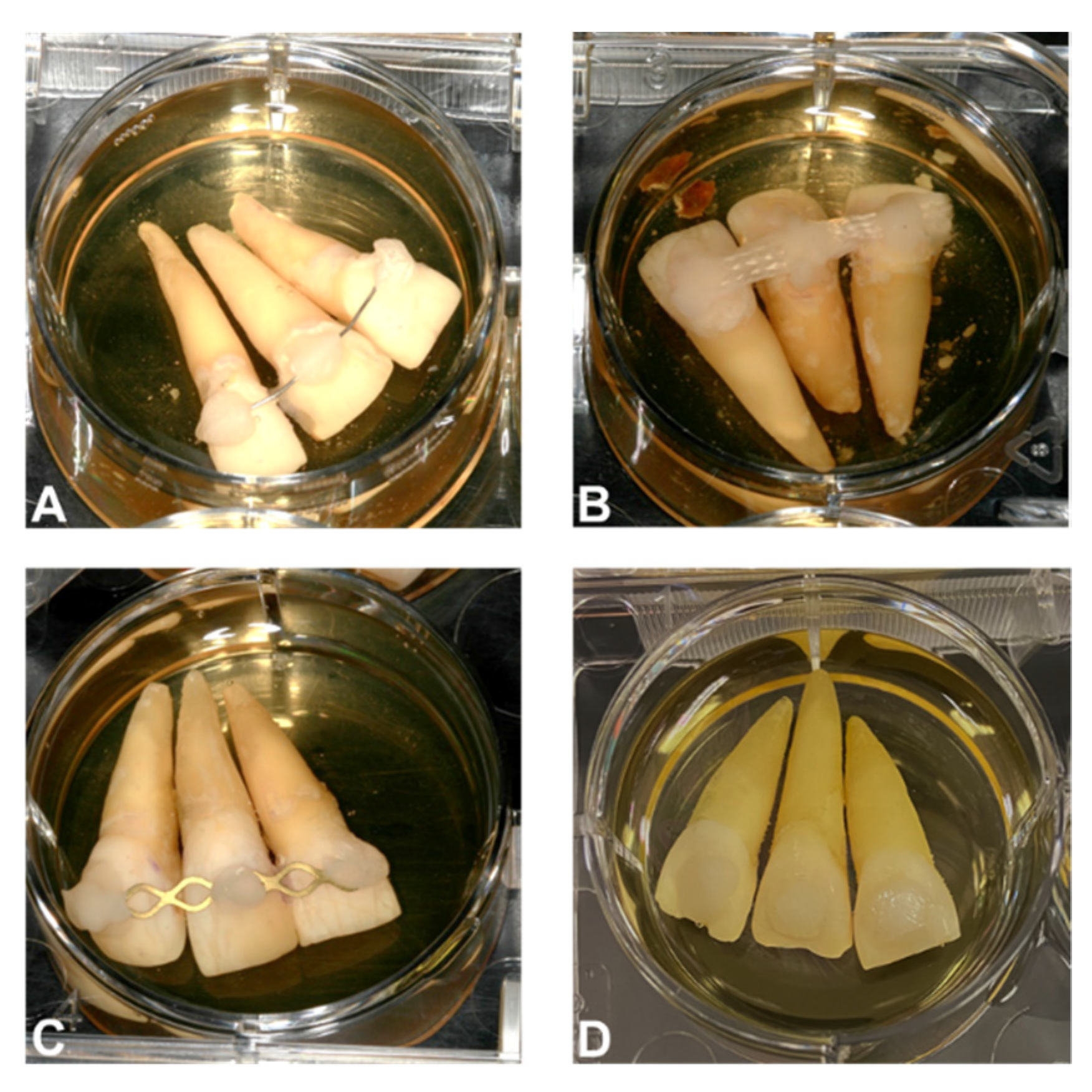
2.1. Teeth Selection and Bonding Process
2.2. Biofilm Preparation
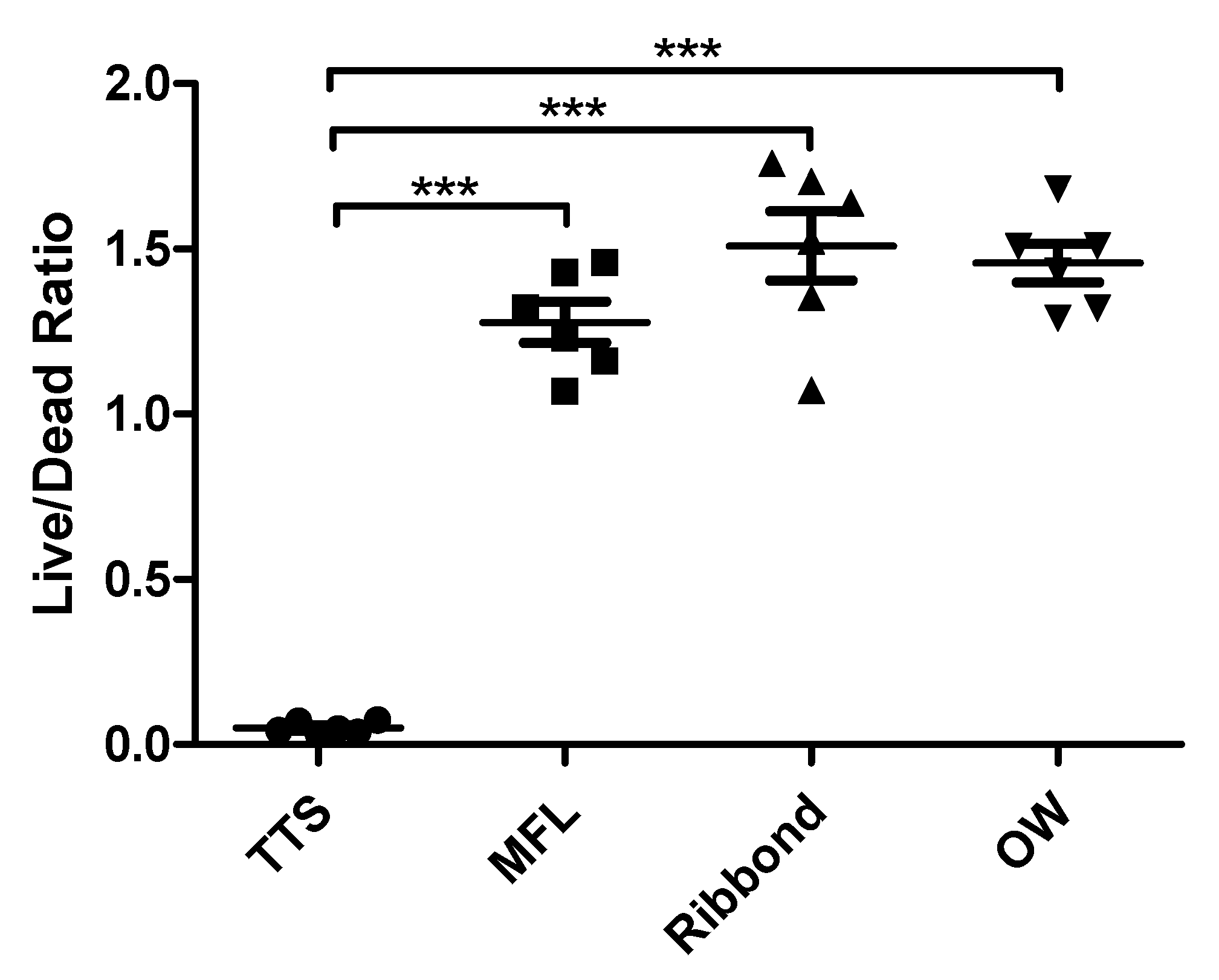
2.3. Cell Viability Assay
2.4. Statistical Analysis
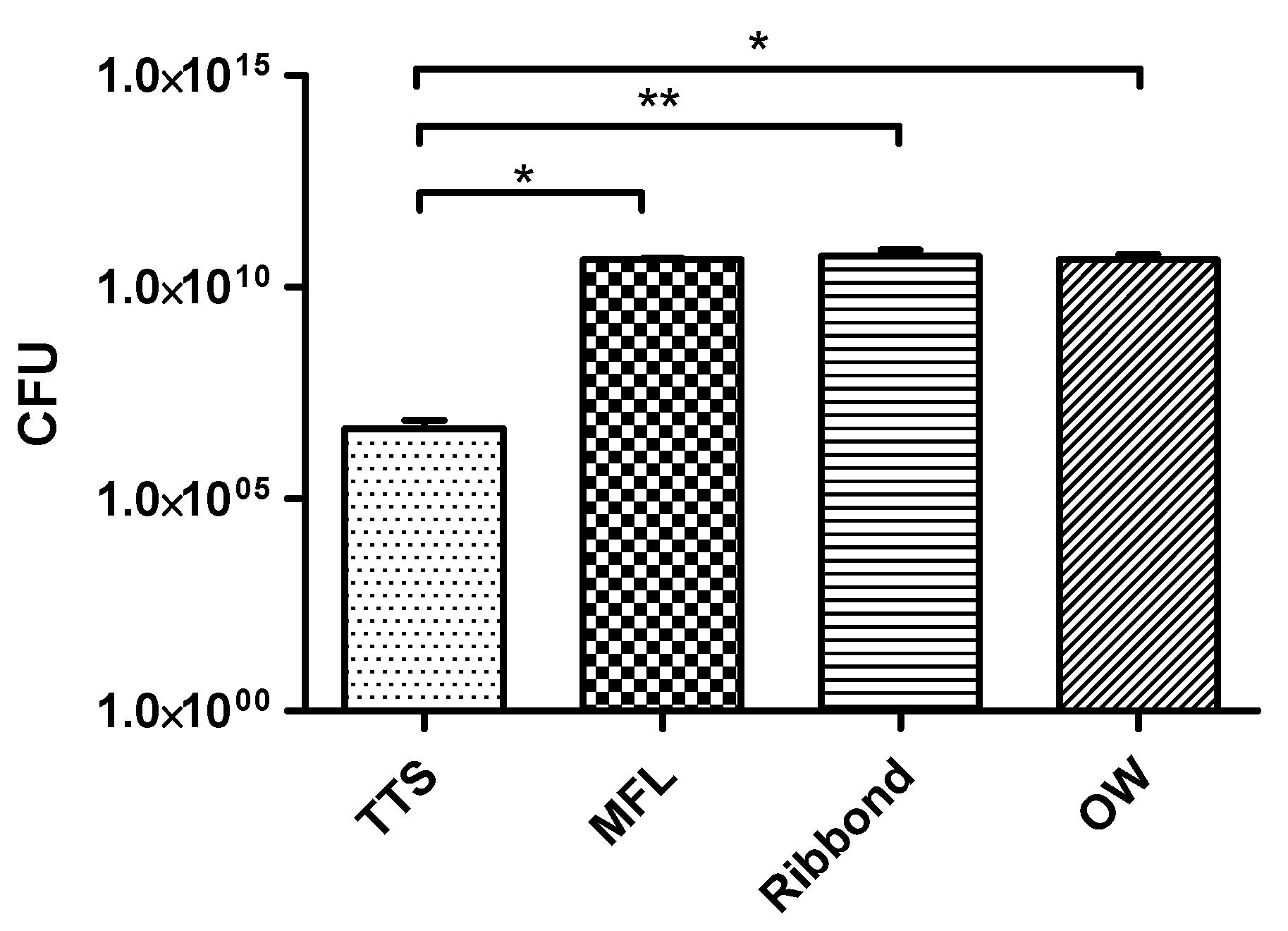
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Petti, S.; Glendor, U.; Andersson, L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dent. Traumatol. 2018, 34, 71–86. [Google Scholar] [CrossRef] [Green Version]
- Artun, J.; Behbehani, F.; Al-Jame, B.; Kerosuo, H. Incisor trauma in an adolescent Arab population: Prevalence, severity, and occlusal risk factors. Am. J. Orthod. Dentofacial. Orthop. 2005, 128, 347–352. [Google Scholar] [CrossRef]
- Skaare, A.B.; Jacobsen, I. Dental injuries in Norwegians aged 7–18 years. Dent. Traumatol. 2003, 19, 67–71. [Google Scholar] [CrossRef]
- Flores, M.T.; Malmgren, B.; Andersson, L.; Andreasen, J.O.; Bakland, L.K.; Barnett, F.; Bourguignon, C.; DiAngelis, A.; Hicks, L.; Sigurdsson, A.; et al. Guidelines for the management of traumatic dental injuries. III. Primary teeth. Dent. Traumatol. 2007, 23, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Flores, M.T.; Andersson, L.; Andreasen, J.O.; Bakland, L.K.; Malmgren, B.; Barnett, F.; Bourguignon, C.; DiAngelis, A.; Hicks, L.; Sigurdsson, A.; et al. Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth. Dent. Traumatol. 2007, 23, 130–136. [Google Scholar] [CrossRef]
- Flores, M.T.; Andersson, L.; Andreasen, J.O.; Bakland, L.K.; Malmgren, B.; Barnett, F.; Bourguignon, C.; DiAngelis, A.; Hicks, L.; Sigurdsson, A.; et al. Guidelines for the management of traumatic dental injuries. I. Fractures and luxations of permanent teeth. Dent. Traumatol. 2007, 23, 66–71. [Google Scholar] [CrossRef] [PubMed]
- von Arx, T.; Filippi, A.; Lussi, A. Comparison of a new dental trauma splint device (TTS) with three commonly used splinting techniques. Dent. Traumatol. 2001, 17, 266–274. [Google Scholar] [CrossRef] [Green Version]
- von Arx, T.; Filippi, A.; Buser, D. Splinting of traumatized teeth with a new device: TTS (Titanium Trauma Splint). Dent. Traumatol. 2001, 17, 180–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristerson, L.; Andreasen, J.O. The effect of splinting upon periodontal and pulpal healing after autotransplantation of mature and immature permanent incisors in monkeys. Int. J. Oral Surg. 1983, 12, 239–249. [Google Scholar] [CrossRef]
- Andreasen, J.O. Treatment of fractured and avulsed teeth. ASDC J. Dent. Child 1971, 38, 29–31. [Google Scholar]
- Nasjleti, C.E.; Castelli, W.A.; Caffesse, R.G. The effects of different splinting times on replantation of teeth in monkeys. Oral Surg. Oral Med. Oral Pathol. 1982, 53, 557–566. [Google Scholar] [CrossRef]
- Abbott, P.V. Prevention and management of external inflammatory resorption following trauma to teeth. Aust. Dent. J. 2016, 61 (Suppl. 1), 82–94. [Google Scholar] [CrossRef] [PubMed]
- Fuss, Z.; Tsesis, I.; Lin, S. Root resorption–diagnosis, classification and treatment choices based on stimulation factors. Dent. Traumatol. 2003, 19, 175–182. [Google Scholar] [CrossRef]
- Trope, M. Luxation injuries and external root resorption-etiology, treatment, and prognosis. J. Calif. Dent. Assoc. 2000, 28, 860–866. [Google Scholar]
- Paula-Silva, F.W.G.; Ribeiro-Santos, F.R.; Petean, I.B.F.; Manfrin Arnez, M.F.; Almeida-Junior, L.A.; Carvalho, F.K.; Silva, L.A.B.D.; Faccioli, L.H. Root canal contamination or exposure to lipopolysaccharide differentially modulate prostaglandin E 2 and leukotriene B 4 signaling in apical periodontitis. J. Appl. Oral Sci. 2020, 28, e20190699. [Google Scholar] [CrossRef]
- Pettini, F.; Pettini, P. Root resorption of replanted teeth: An SEM study. Endod. Dent. Traumatol. 1998, 14, 144–149. [Google Scholar] [CrossRef]
- Balto, K.; White, R.; Mueller, R.; Stashenko, P. A mouse model of inflammatory root resorption induced by pulpal infection. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 461–468. [Google Scholar] [CrossRef]
- Fouad, A.F. Microbiological Aspects of Traumatic Injuries. J. Endod. 2019, 45, S39–S48. [Google Scholar] [CrossRef]
- Al-Nazhan, S.A.; Spangberg, L.W. Light and SEM observation of internal root resorption of a traumatized permanent central incisor. Int. Endod. J. 1995, 28, 133–136. [Google Scholar] [CrossRef]
- Galler, K.M.; Gratz, E.M.; Widbiller, M.; Buchalla, W.; Knuttel, H. Pathophysiological mechanisms of root resorption after dental trauma: A systematic scoping review. BMC Oral Health 2021, 21, 163. [Google Scholar] [CrossRef]
- Grossman, L.I. Origin of microorganisms in traumatized, pulpless, sound teeth. J. Dent. Res. 1967, 46, 551–553. [Google Scholar] [CrossRef]
- Love, R.M. The effect of tissue molecules on bacterial invasion of dentine. Oral Microbiol. Immunol. 2002, 17, 32–37. [Google Scholar] [CrossRef]
- Love, R.M.; Jenkinson, H.F. Invasion of dentinal tubules by oral bacteria. Crit. Rev. Oral Biol. Med. 2002, 13, 171–183. [Google Scholar] [CrossRef] [Green Version]
- Gomes, B.P.; Berber, V.B.; Kokaras, A.S.; Chen, T.; Paster, B.J. Microbiomes of Endodontic-Periodontal Lesions before and after Chemomechanical Preparation. J. Endod. 2015, 41, 1975–1984. [Google Scholar] [CrossRef]
- Rupf, S.; Kannengiesser, S.; Merte, K.; Pfister, W.; Sigusch, B.; Eschrich, K. Comparison of profiles of key periodontal pathogens in periodontium and endodontium. Endod. Dent. Traumatol. 2000, 16, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, F.M.; Kahler, B. Pulpal response after acute dental injury in the permanent dentition: Clinical implications—A review. J. Endod. 2015, 41, 299–308. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Lauridsen, E.; Andreasen, F.M. Contradictions in the treatment of traumatic dental injuries and ways to proceed in dental trauma research. Dent. Traumatol. 2010, 26, 16–22. [Google Scholar] [CrossRef]
- Andersson, L.; Andreasen, J.O.; Day, P.; Heithersay, G.; Trope, M.; Diangelis, A.J.; Kenny, D.J.; Sigurdsson, A.; Bourguignon, C.; Flores, M.T.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent. Traumatol. 2012, 28, 88–96. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Vinding, T.R.; Christensen, S.S.A. Predictors for healing complications in the permanent dentition after dental trauma. Endod. Top. 2006, 1, 20–27. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Jensen, S.S.; Sae-Lim, V. The role of antibiotics in preventing healing complications after traumatic dental injuries: A literature review. Endod. Top. 2006, 14, 80–92. [Google Scholar] [CrossRef]
- Yawata, Y.; Nguyen, J.; Stocker, R.; Rusconi, R. Microfluidic Studies of Biofilm Formation in Dynamic Environments. J. Bacteriol. 2016, 198, 2589–2595. [Google Scholar] [CrossRef] [Green Version]
- Fagerlind, M.G.; Webb, J.S.; Barraud, N.; McDougald, D.; Jansson, A.; Nilsson, P.; Harlén, M.; Kjelleberg, S.; Rice, S.A. Dynamic modelling of cell death during biofilm development. J. Theor. Biol. 2012, 295, 23–36. [Google Scholar] [CrossRef]
- Alves, F.R.; Siqueira, J.F.; Carmo, F.L.; Santos, A.L.; Peixoto, R.S.; Rôças, I.N.; Rosado, A.S. Bacterial community profiling of cryogenically ground samples from the apical and coronal root segments of teeth with apical periodontitis. J. Endod. 2009, 35, 486–492. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N. Community as the unit of pathogenicity: An emerging concept as to the microbial pathogenesis of apical periodontitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 870–878. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F. Fate of the tissue in lateral canals and apical ramifications in response to pathologic conditions and treatment procedures. J. Endod. 2010, 36, 1–15. [Google Scholar] [CrossRef]
- Ricucci, D.; Loghin, S.; Siqueira, J.F. Exuberant Biofilm infection in a lateral canal as the cause of short-term endodontic treatment failure: Report of a case. J. Endod. 2013, 39, 712–718. [Google Scholar] [CrossRef]
- Bastos, J.V.; Côrtes, M.I.S. Pulp canal obliteration after traumatic injuries in permanent teeth-scientific fact or fiction? Braz. Oral Res. 2018, 32, e75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fouad, A.F.; Abbott, P.V.; Tsilingaridis, G.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; O’Connell, A.; Flores, M.T.; Day, P.F.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent. Traumatol. 2020, 36, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Antrim, D.D.; Ostrowski, J.S. A functional splint for traumatized teeth. J. Endod. 1982, 8, 328–331. [Google Scholar] [CrossRef]
- Bucci, M.; Borgonovo, A.; Bianchi, A.; Zanellato, A.; Re, D. Microbiological analysis of bacterial plaque on three different threads in oral surgery. Minerva. Stomatol. 2017, 66, 28–34. [Google Scholar] [CrossRef]
- Chaudhary, V.; Shrivastava, B.; Bhatia, H.P.; Aggarwal, A.; Singh, A.K.; Gupta, N. Multifunctional Ribbond--a versatile tool. J. Clin. Pediatr. Dent. 2012, 36, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Chowdhary, P.; Gurtu, A.; Mehrotra, N.; Kishore, A. Splinting of Longitudinal Fracture: An Innovative Approach. Case Rep. Dent. 2016, 2016, 5083874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikarinen, K. Tooth splinting: A review of the literature and consideration of the versatility of a wire-composite splint. Endod. Dent. Traumatol. 1990, 6, 237–250. [Google Scholar] [CrossRef]
- Taha, M.; El-Fallal, A.; Degla, H. In vitro and in vivo biofilm adhesion to esthetic coated arch wires and its correlation with surface roughness. Angle Orthod 2016, 86, 285–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshinari, M.; Oda, Y.; Kato, T.; Okuda, K. Influence of surface modifications to titanium on antibacterial activity in vitro. Biomaterials 2001, 22, 2043–2048. [Google Scholar] [CrossRef]
- Chouirfa, H.; Bouloussa, H.; Migonney, V.; Falentin-Daudré, C. Review of titanium surface modification techniques and coatings for antibacterial applications. Acta Biomater. 2019, 83, 37–54. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mona, M.; Walker, C.; Shaddox, L.M.; Pileggi, R. Bacterial Biofilm Growth on Various Dental Stabilization Systems for Avulsed and Luxated Teeth. Appl. Sci. 2021, 11, 8982. https://doi.org/10.3390/app11198982
Mona M, Walker C, Shaddox LM, Pileggi R. Bacterial Biofilm Growth on Various Dental Stabilization Systems for Avulsed and Luxated Teeth. Applied Sciences. 2021; 11(19):8982. https://doi.org/10.3390/app11198982
Chicago/Turabian StyleMona, Mahmoud, Clay Walker, Luciana M. Shaddox, and Roberta Pileggi. 2021. "Bacterial Biofilm Growth on Various Dental Stabilization Systems for Avulsed and Luxated Teeth" Applied Sciences 11, no. 19: 8982. https://doi.org/10.3390/app11198982
APA StyleMona, M., Walker, C., Shaddox, L. M., & Pileggi, R. (2021). Bacterial Biofilm Growth on Various Dental Stabilization Systems for Avulsed and Luxated Teeth. Applied Sciences, 11(19), 8982. https://doi.org/10.3390/app11198982