
Antibiotic Prophylaxis in the Prevention of Postoperative Infections in Mandibular Third Molar Extractions: Systematic Review and Meta-Analysis

 ,
,  , and
, and 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Evidence Quality Evaluation and Data Extraction
2.2. Meta-Analysis
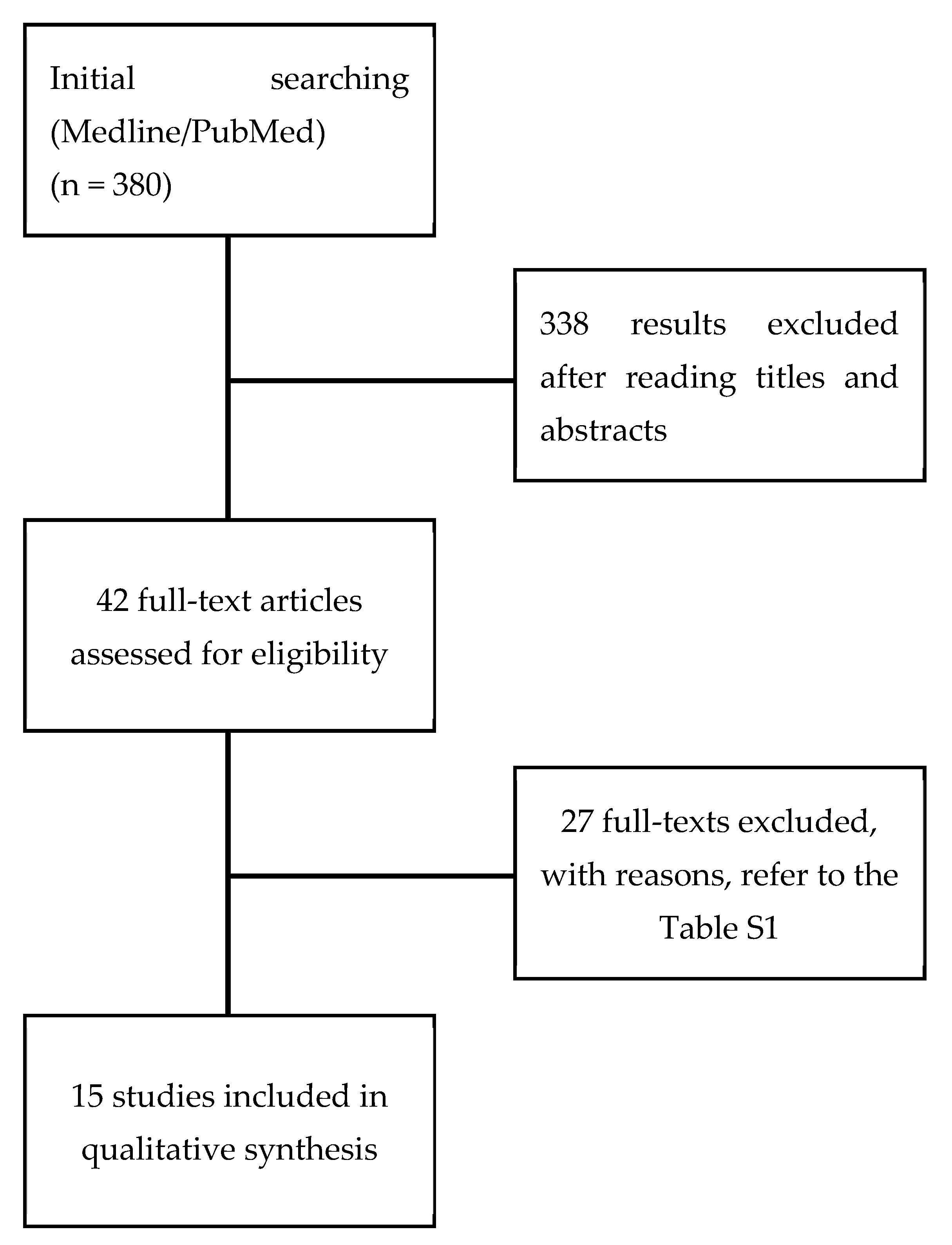
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ren, Y.F.; Malmstrom, H.S. Effectiveness of Antibiotic Prophylaxis in Third Molar Surgery: A Meta-Analysis of Randomized Controlled Clinical Trials. J. Oral Maxillofac. Surg. 2007, 65, 1909–1921. [Google Scholar] [CrossRef]
- Friedman, J.W. The prophylactic extraction of third molars: A public health hazard. Am. J. Public Health 2007, 97, 1554–1559. [Google Scholar] [CrossRef]
- Bloomer, C.R. Alveolar osteitis prevention by immediate placement of medicated packing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 90, 282–284. [Google Scholar] [CrossRef]
- Pell, G.; Gregory, G. Impacted mandibular third molars: Classification and modified technique for removel. Dent. Dig. 1933, 39, 330–338. [Google Scholar]
- Sancho-Puchades, M.; Herráez-Vilas, J.M.; Valmaseda-Castellón, E.; Berini-Aytés, L.; Gay-Escoda, C. Analysis of the antibiotic prophylaxis prescribed by Spanish Oral Surgeons. Med. Oral Patol. Oral Cir. Bucal 2009, 14, e533–e537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chugh, A.; Patnana, A.K.; Kumar, P.; Chugh, V.K.; Khera, D.; Singh, S. Critical analysis of methodological quality of systematic reviews and meta-analysis of antibiotics in third molar surgeries using AMSTAR 2. J. Oral Biol. Craniofacial Res. 2020, 10, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.K.; Gopinath, D.; Li, K.Y.; Leung, Y.Y.; Botelho, M.G. Does the use of amoxicillin/amoxicillin–clavulanic acid in third molar surgery reduce the risk of postoperative infection? A systematic review with meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Conaty, S.; Hoang, H.; Kirshen, D.; Kwong, C.; Schroeder, E.; Stromme, A. Pre and Post-Operative Antibiotic Prophylaxis in the Prevention of Complications Following Third Molar Surgery; University of Toronto: Toronto, ON, Canada, 2010. [Google Scholar]
- Marcussen, K.B.; Laulund, A.S.; Jorgensen, H.L.; Pinholt, E.M. A Systematic Review on Effect of Single-Dose Preoperative Antibiotics at Surgical Osteotomy Extraction of Lower Third Molars. J. Oral Maxillofac. Surg. 2016, 74, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Lang, M.S.; Gonzales, M.L.; Dodson, T.B. Do Antibiotics Decrease the Risk of Inflammatory Complications After Third Molar Removal in Community Practices? J. Oral Maxillofac. Surg. 2017, 75, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Isiordia-Espinoza, M.A.; Aragon-Martinez, O.H.; Martínez-Morales, J.F.; Zapata-Morales, J.R. Risk of wound infection and safety profile of amoxicillin in healthy patients which required third molar surgery: A systematic review and meta-analysis. Br. J. Oral Maxillofac. Surg. 2015, 53, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.V.; Kanatas, A.N.; Hardy, P. Antibiotic prophylaxis and third molar surgery. Br. Dent. J. 2005, 198, 327–330. [Google Scholar] [CrossRef] [Green Version]
- Jadad, A.R.; Moore, R.; Carroll, D.; Jenkinson, C.; Reynolds, D.M.; Gavaghan, D.; McQuay, H.J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Petitti, D.B. Approaches to heterogeneity in meta-analysis. Stat. Med. 2001, 20, 3625–3633. [Google Scholar] [CrossRef] [PubMed]
- Der Simonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. The statistical basis of meta-analysis. Stat. Methods Med. Res. 1993, 2, 121–145. [Google Scholar] [CrossRef] [PubMed]
- Berlin, J.A.; Laird, N.M.; Sacks, H.S.; Chalmers, T.C. A comparison of statistical methods for combining event rates from clinical trials. Stat. Med. 1989, 8, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.R.; Kim, S.-J. Intervention meta-analysis: Application and practice using R software. Epidemiol. Health 2019, 41, e2019008. [Google Scholar] [CrossRef]
- Arteagoitia, I.; Ramos, E.; Santamaria, G.; Barbier, L.; Alvarez, J.; Santamaria, J. Amoxicillin/clavulanic acid 2000/125 mg to prevent complications due to infection following completely bone-impacted lower third molar removal: A clinical trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 8–16. [Google Scholar] [CrossRef]
- Arteagoitia, I.; Diez, A.; Barbier, L.; Santamaria, G.; Santamaria, J. Efficacy of amoxicillin/clavulanic acid in preventing infectious and inflammatory complications following impacted mandibular third molar extraction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 11–18. [Google Scholar] [CrossRef]
- Bulut, E.; Bulut, S.; Etikan, I.; Koseoglu, O. The value of routine antibiotic prophylaxis in mandibular third molar surgery: Acute-phase protein levels as indicators of infection. J. Oral Sci. 2001, 43, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Bystedt, H.; Nord, C.E.; Nordenram, A. Effect of azidocillin, erythromycin, clindamycin and doxycycline on postoperative complications after surgical removal of impacted mandibular third molars. Int. J. Oral Surg. 1980, 9, 157–165. [Google Scholar] [CrossRef]
- Curran, J.B.; Kennett, S.; Young, A.R. An assessment of the use of prophylactic antibiotics in third molar surgery. Int. J. Oral Surg. 1974, 3, 1–6. [Google Scholar] [CrossRef]
- Kaczmarzyk, T.; Wichlinski, J.; Stypulkowska, J.; Zaleska, M.; Panas, M.; Woron, J. Single-dose and multi-dose clindamycin therapy fails to demonstrate efficacy in preventing infectious and inflammatory complications in third molar surgery. Int. J. Oral Maxillofac. Surg. 2007, 36, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Lacasa, J.M.; Jiménez, J.; Ferrás, V.; Bossom, M.; Sóla-Morales, O.; García-Rey, C.; Aguilar, L.; Garau, J. Prophylaxis versus pre-emptive treatment for infective and inflammatory complications of surgical third molar removal: A randomized, double-blind, placebo-controlled, clinical trial with sustained release amoxicillin/clavulanic acid (1000/62.5 mg). Int. J. Oral Maxillofac. Surg. 2007, 36, 321–327. [Google Scholar] [CrossRef] [PubMed]
- López-Cedrún, J.L.; Pijoan, J.I.; Fernández, S.; Santamaria, J.; Hernandez, G. Efficacy of amoxicillin treatment in preventing postoperative complications in patients undergoing third molar surgery: A prospective, randomized, double-blind controlled study. J. Oral Maxillofac. Surg. 2011, 69, e5–e14. [Google Scholar] [CrossRef] [PubMed]
- Milani, B.A.; Bauer, H.C.; Sampaio-Filho, H.; Horliana, A.C.R.T.; Perez, F.E.G.; Tortamano, I.P.; Jorge, W.A. Antibiotic therapy in fully impacted lower third molar surgery: Randomized three-arm, double-blind, controlled trial. Oral Maxillofac. Surg. 2015, 19, 341–346. [Google Scholar] [CrossRef]
- Mitchell, D.A. A controlled clinical trial of prophylactic tinidazole for chemoprophylaxis in third molar surgery. Br. Dent. J. 1986, 160, 284–286. [Google Scholar] [CrossRef]
- Monaco, G.; Tavernese, L.; Agostini, R.; Marchetti, C. Evaluation of Antibiotic Prophylaxis in Reducing Postoperative Infection After Mandibular Third Molar Extraction in Young Patients. Am. Assoc. Oral Maxillofac. Surg. 2009, 67, 1467–1472. [Google Scholar] [CrossRef]
- Pasupathy, S.; Alexander, M. Antibiotic prophylaxis in third molar surgery. J. Craniofacial Surg. 2011, 22, 551–553. [Google Scholar] [CrossRef]
- Poeschl, P.W.; Eckel, D.; Poeschl, E. Postoperative Prophylactic Antibiotic Treatment in Third Molar Surgery—A Necessity? J. Oral Maxillofac. Surg. 2004, 62, 3–8. [Google Scholar] [CrossRef]
- Sekhar, C.H.; Narayanan, V.; Baig, M.F. Role of antimicrobials in third molar surgery: Prospective, double blind, randomized, placebo-controlled clinical study. Br. J. Oral Maxillofac. Surg. 2001, 39, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Xue, P.; Wang, J.; Wu, B.; Ma, Y.; Wu, F.; Hou, R. Efficacy of antibiotic prophylaxis on postoperative inflammatory complications in Chinese patients having impacted mandibular third molars removed: A split-mouth, double-blind, self-controlled, clinical trial. Br. J. Oral Maxillofac. Surg. 2015, 53, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg. Infect. 2013, 14, 73–156. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.A.; Morris, A.J. Surgical antibiotic prophylaxis: More is not better. Lancet Infect. Dis. 2020, 20, 1110–1111. [Google Scholar] [CrossRef]
- Phillips, B.T.; Sheldon, E.S.; Orhurhu, V.; Ravinsky, R.A.; Freiser, M.E.; Asgarzadeh, M.; Viswanath, O.; Kaye, A.D.; Roguski, M. Preoperative Versus Extended Postoperative Antimicrobial Prophylaxis of Surgical Site Infection During Spinal Surgery: A Comprehensive Systematic Review and Meta-Analysis. Adv. Ther. 2020, 37, 2710–2733. [Google Scholar] [CrossRef] [PubMed]
- Savitz, M.H.; Malis, L.I.; Savitz, S.I. Efficacy of prophylactic antibiotic therapy in spinal surgery: A meta-analysis. Neurosurgery 2003, 53, 243–244. [Google Scholar] [CrossRef]
- Mcdonald, M.; Grabsch, E.; Marshall, C.; Forbes, A. Single-versus multiple-dose antimicrobial prophylaxis for major surgery: A systematic review. Aust. N. Z. J. Surg. 1998, 68, 388–395. [Google Scholar] [CrossRef]
- Crader, M.F.; Varacallo, M. Preoperative Antibiotic Prophylaxis. StatPearls. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK442032/ (accessed on 7 September 2021).
- Sayed, N.; Bakathir, A.; Pasha, M.; Al-Sudairy, S. Complications of Third Molar Extraction. Sultan Qaboos Univ. Med. J. 2019, 19, 230–235. [Google Scholar] [CrossRef]
- Gill, A.S.; Morrissey, H.; Rahman, A. A Systematic Review and Meta-Analysis Evaluating Antibiotic Prophylaxis in Dental Implants and Extraction Procedures. Medicina 2018, 54, 95. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| (randomized controlled trial [PT] OR controlled clinical trial [PT] OR randomized controlled trials [MH] OR random allocation [MH] OR double-blind method [MH] OR single-blind method [MH] OR clinical trial [PT] OR clinical trials [MH] OR ("clinical trial" [TW]) OR ((singl* [TW] OR doubl* [TW] OR trebl* [TW] OR tripl* [TW]) AND (mask* [TW] OR blind* [TW])) OR (placebos [MH] OR placebo* [TW] OR random* [TW] OR research design [MH:noexp]) NOT (animals [MH] NOT humans [MH])) AND (((Molar, Third/surgery [MH]) OR (*Tooth Extraction/adverse effects [MH])) AND ((Amoxicillin/therapeutic use [MH]) OR (Anti-Bacterial Agents/therapeutic use [MH]) OR (Antibiotic Prophylaxis/*utilization [MH]) OR (Endocarditis, Bacterial/prevention and control [MH]) OR (Pain, Postoperative/prevention and control [MH]) OR (Surgical Wound Infection/prevention and control [MH]) OR (Surgical Wound Infection/prevention and control [MH]))) |
| Study | Country | Total Sample Size | Comparisons | Conclusions |
|---|---|---|---|---|
| Arteagoitia et al., 2015 [20] | Spain | 118 |
| Insufficient evidence to recommend routine use of this antibiotic treatment |
| Arteagoitia et al., 2005 [21] | Spain | 490 |
| A/aC is efficacious in reducing the incidence of inflammatory complications following third molar extraction but should not be prescribed in all cases |
| Bulut et al., 2001 [22] | Turkey | 60 |
| The results revealed no statistically significant difference between treated and control patients in terms of incidence of postoperative infection. |
| Bystedt et al. 1980 [23] | Sweden | 140 |
| Systemically administered antibiotics offered only slight advantages in routine operations of impacted third mandibular molars, but could decrease the rate of infections after traumatic operations |
| Curran et al. 1974 [24] | Canada | 133 |
| Use of prophylactic antibiotics in third molar surgery is unnecessary unless specific systemic factors are present |
| Kaczmarzyk et al., 2007 [25] | Poland | 86 |
| Clindamycin applied in a single pre-surgical dose of 600 mg with or without subsequent 5-day therapy does not demonstrate efficacy in prophylaxis for postoperative inflammatory complications |
| Lacasa et al., 2007 [26] | Spain | 222 |
| Prophylaxis was beneficial in simpler procedures and may be suitable in cases where ostectomy is not performed. |
| Lopez Cedrun et al., 2011 [27] | Spain | 123 |
| Amoxicillin administered pre- or postoperatively demonstrated greater efficacy than placebo in preventing postoperative complications in patients undergoing third molar surgery. The best results were obtained using the postoperative protocol. |
| Milani et al., 2015 [28] | Brasil | 80 |
| No advantage in the administration of antibiotics in healthy patients undergoing extraction of fully impacted lower third molars with a controlled aseptic chain |
| Mitchell 1986 [29] | United Kingdom | 89 |
| Antibiotic prophylaxis is effective in preventing complications and infections following the extraction of included mandibular third molars |
| Monaco et al., 2009 [30] | Italy | 59 |
| Significative difference between patients receiving preoperative amoxicillin and the control group in wound infections and consumption of analgesics |
| Pasupathy & Alexander 2011 [31] | India | 89 |
| No statistically significant difference between the groups |
| Poeschl et al., 2004 [32] | Austria | 528 |
| Postoperative oral prophylactic antibiotic treatment after the removal of lower third molars does not contribute to a better wound healing, less pain, or increased mouth opening and could not prevent the cases of inflammatory problems after surgery, respectively, and therefore it is not recommended for routinary use |
| Sekhar et al., 2001 [33] | India | 125 |
| Antimicrobial prophylaxis does not seem to reduce morbidity after removal of lower third molars |
| Xue et al., 2015 [34] | China | 384 |
| Prophylactic amoxicillin (or clindamycin) is not effective in the prevention of postoperative inflammatory complications after impacted mandibular third molars removal |
| Study | Random Allocation | Double Blinded | Explanation for Withdrawals | JADAD Score |
|---|---|---|---|---|
| Arteagoitia et al., 2015 [20] | Yes | Yes | Yes | 4 |
| Arteagoitia et al., 2005 [21] | Yes | Yes | Yes | 4 |
| Bulut et al., 2001 [22] | Yes | Yes | No | 2 |
| Bystedt et al. 1980 [23] | Yes | Yes | No | 2 |
| Curran et al. 1974 [24] | Yes | Yes | Yes | 2 |
| Kaczmarzyk et al., 2007 [25] | Yes | Yes | Yes | 4 |
| Lacasa et al., 2007 [26] | Yes | Yes | Yes | 4 |
| Lopez Cedrun et al., 2011 [27] | Yes | Yes | Yes | 3 |
| Milani et al., 2015 [28] | Yes | Yes | Yes | 4 |
| Mitchell 1986 [29] | Yes | Yes | Yes | 3 |
| Monaco et al., 2009 [30] | Yes | No | No | 1 |
| Pasupathy & Alexander 2011 [31] | Yes | Yes | Yes | 4 |
| Poeschl et al., 2004 [32] | Yes | No | Yes | 2 |
| Sekhar et al., 2001 [33] | Yes | Yes | Yes | 3 |
| Xue et al., 2015 [34] | Yes | Yes | No | 3 |
| Comparison | N. Included Studies | N. Test | N. Control | N. Total | RR Fixed | p Fixed | RR Random | p Random | I2 | p | NNT |
|---|---|---|---|---|---|---|---|---|---|---|---|
| All methods of administration | |||||||||||
| ATBs (overall) vs. placebo | 15 | 1618 | 1108 | 2726 | 0.43 (0.32; 0.59) | <0.0001 | 0.40 [0.26; 0.63] | <0.0001 | 43% | 0.04 | 15 |
| Pre-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 8 | 356 | 296 | 652 | 0.29 (0.16; 0.52) | <0.0001 | 0.29 [0.16; 0.52] | <0.0001 | 0% | 0.47 | 9 |
| ATBs (penicillin) vs. placebo | 5 | 207 | 191 | 398 | 0.39 (0.18; 0.85) | 0.0164 | 0.40 [0.17; 0.94] | 0.0421 | 10% | 0.35 | 13 |
| ATBs (others) vs. placebo | 4 | 149 | 134 | 283 | 0.23 (0.10; 0.53) | 0.0005 | 0.23 [0.10; 0.53] | 0.0005 | 0% | 0.52 | 6 |
| Pre- and post-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 7 | 484 | 456 | 940 | 0.56 (0.34; 0.94) | 0.0265 | 0.56 [0.34; 0.94] | 0.0265 | 0% | 0.68 | 28 |
| ATBs (penicillin) vs. placebo | 4 | 312 | 300 | 612 | 0.72 (0.33; 1.54) | 0.3935 | 0.72 [0.33; 1.54] | 0.3935 | 0% | 0.77 | 68 |
| ATBs (others) vs. placebo | 3 | 172 | 156 | 328 | 0.47 (0.24; 0.92) | 0.0277 | 0.47 [0.23; 0.97] | 0.0404 | 10% | 0.33 | 13 |
| Post-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 4 | 778 | 552 | 1330 | 0.46 (0.29; 0.74) | 0.0012 | 0.26 [0.07; 0.94] | 0.0393 | 79% | <0.01 | 15 |
| ATBs (penicillin) vs. placebo | 4 | 551 | 518 | 1069 | 0.40 (0.24; 0.66) | 0.0004 | 0.26 [0.08; 0.89] | 0.0314 | 75% | <0.01 | 12 |
| ATBs (others) vs. placebo | 1 | 227 | 206 | 433 | 0.96 (0.48; 1.89) | 0.8964 | 0.96 [0.48; 1.89] | 0.8964 | NA | NA | 148 |
| Subgroup analysis: Surgery requiring osteotomy—All methods of administration | |||||||||||
| ATBs (overall) vs. placebo | 11 | 1032 | 731 | 1763 | 0.54 (0.38; 0.76) | 0.0003 | 0.50 [0.32; 0.77] | 0.0015 | 28% | 0.18 | 19 |
| Subgroup analysis: Surgery requiring osteotomy—Pre-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 5 | 156 | 150 | 306 | 0.27 (0.13; 0.57) | 0.0005 | 0.27 [0.13; 0.57] | 0.0005 | 0% | 0.41 | 6 |
| ATBs (penicillin) vs. placebo | 3 | 96 | 87 | 183 | 0.35 (0.12; 1.07) | 0.0650 | 0.43 [0.09; 2.14] | 0.3042 | 44% | 0.17 | 10 |
| ATBs (others) vs. placebo | 2 | 60 | 63 | 123 | 0.22 (0.08; 0.59) | 0.0028 | 0.22 [0.08; 0.59] | 0.0028 | 0% | 1.00 | 4 |
| Subgroup analysis: Surgery requiring osteotomy—Pre- and post-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 7 | 484 | 456 | 940 | 0.56 (0.34; 0.94) | 0.0265 | 0.56 [0.34; 0.94] | 0.0265 | 0% | 0.68 | 28 |
| ATBs (penicillin) vs. placebo | 4 | 312 | 300 | 612 | 0.72 (0.33; 1.54) | 0.3935 | 0.72 [0.33; 1.54] | 0.3935 | 0% | 0.77 | 68 |
| ATBs (others) vs. placebo | 3 | 172 | 156 | 328 | 0.47 (0.24; 0.92) | 0.0277 | 0.47 [0.23; 0.97] | 0.0404 | 10% | 0.33 | 13 |
| Subgroup analysis: Surgery requiring osteotomy—Post-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 2 | 392 | 212 | 604 | 0.76 (0.44; 1.32) | 0.3268 | 0.53 [0.14; 2.11] | 0.3700 | 69% | 0.07 | 26 |
| ATBs (penicillin) vs. placebo | 2 | 212 | 212 | 424 | 0.70 (0.37; 1.31) | 0.2652 | 0.52 [0.14; 2.02] | 0.3470 | 66% | 0.09 | 24 |
| Subgroup analysis: Surgery requiring odontotomy—All methods of administration | |||||||||||
| ATBs (overall) vs. placebo | 5 | 404 | 326 | 730 | 0.54 (0.27; 1.10) | 0.0894 | 0.54 [0.27; 1.10] | 0.0894 | 0% | 0.55 | 41 |
| Subgroup analysis: Surgery requiring odontotomy—Pre-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 3 | 122 | 76 | 198 | 0.45 (0.13; 1.52) | 0.1990 | 0.51 [0.10; 2.45] | 0.3978 | 36% | 0.21 | 23 |
| ATBs (penicillin) vs. placebo | 3 | 93 | 76 | 169 | 0.62 (0.19; 2.10) | 0.4459 | 0.66 [0.15; 2.95] | 0.5901 | 30% | 0.24 | 36 |
| Subgroup analysis: Surgery requiring odontotomy—Pre- and post-surgery administration | |||||||||||
| ATBs (overall) vs. placebo | 3 | 282 | 270 | 552 | 0.67 (0.29; 1.55) | 0.3505 | 0.67 [0.29; 1.55] | 0.3505 | 0% | 0.62 | 62 |
| ATBs (penicillin) vs. placebo | 3 | 282 | 270 | 552 | 0.67 (0.29; 1.55) | 0.3505 | 0.67 [0.29; 1.55] | 0.3505 | 0% | 0.62 | 62 |
| Subgroup analysis: Penicillin antibiotics vs. non-penicillin antibiotics—All methods of administration | |||||||||||
| ATBs (penicillin) vs. ATBs (others) | 2 | 207 | 209 | 416 | 1.04 (0.52; 2.04) | 0.9186 | 1.06 [0.49; 2.26] | 0.8881 | 3% | 0.31 | 181 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupi, S.M.; Olivieri, G.; Landini, J.; Ferrigno, A.; Richelmi, P.; Todaro, C.; Rodriguez y Baena, R. Antibiotic Prophylaxis in the Prevention of Postoperative Infections in Mandibular Third Molar Extractions: Systematic Review and Meta-Analysis. Appl. Sci. 2021, 11, 9449. https://doi.org/10.3390/app11209449
Lupi SM, Olivieri G, Landini J, Ferrigno A, Richelmi P, Todaro C, Rodriguez y Baena R. Antibiotic Prophylaxis in the Prevention of Postoperative Infections in Mandibular Third Molar Extractions: Systematic Review and Meta-Analysis. Applied Sciences. 2021; 11(20):9449. https://doi.org/10.3390/app11209449
Chicago/Turabian StyleLupi, Saturnino Marco, Giorgia Olivieri, Jessica Landini, Andrea Ferrigno, Plinio Richelmi, Claudia Todaro, and Ruggero Rodriguez y Baena. 2021. "Antibiotic Prophylaxis in the Prevention of Postoperative Infections in Mandibular Third Molar Extractions: Systematic Review and Meta-Analysis" Applied Sciences 11, no. 20: 9449. https://doi.org/10.3390/app11209449
APA StyleLupi, S. M., Olivieri, G., Landini, J., Ferrigno, A., Richelmi, P., Todaro, C., & Rodriguez y Baena, R. (2021). Antibiotic Prophylaxis in the Prevention of Postoperative Infections in Mandibular Third Molar Extractions: Systematic Review and Meta-Analysis. Applied Sciences, 11(20), 9449. https://doi.org/10.3390/app11209449