
Hospital Site Suitability Assessment Using Three Machine Learning Approaches: Evidence from the Gaza Strip in Palestine


 ,
,
Abstract
:1. Introduction
2. Background
3. Materials and Methods
3.1. Study Area and Data Used
3.2. Methodology
3.3. Data Preparation
3.3.1. Environmental Factors
3.3.2. Topographical Factors
3.3.3. Geodemographic Factors
3.4. Model Implementation and Validation
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reinicke, C.; MacDonald, J.; Donald, J. Report of a Field Assessment of Health Conditions in the Occupied Palestinian Territory; World Health Organization Reports, Palestine 2016; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/gb/Statements/Report_Palestinian_territory/Report_Palestinian_territory-en.pdf (accessed on 4 November 2021).
- Ahmed, S.; Adams, A.M.; Islam, R.; Hasan, S.M.; Panciera, R. Impact of traffic variability on geographic accessibility to 24/7 emergency healthcare for the urban poor: A GIS study in Dhaka, Bangladesh. PLoS ONE 2019, 14, e0222488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgs, G.; Langford, M.; Jarvis, P.; Page, N.; Richards, J.; Fry, R. Using Geographic Information Systems to investigate variations in accessibility to ‘extended hours’ primary healthcare provision. Health Soc. Care Commun. 2019, 27, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- Strozzi, F.; Garagiola, E.; Trucco, P. Analysing the attractiveness, availability and accessibility of healthcare providers via social network analysis (SNA). Decis. Support Syst. 2019, 120, 25–37. [Google Scholar] [CrossRef]
- Turnbull, J.; Martin, D.; Lattimer, V.; Pope, C.; Culliford, D. Does distance matter? Geographical variation in GP out-of-hours service use: An observational study. Br. J. Gen. Pract. 2008, 58, 471–477. [Google Scholar] [CrossRef]
- Zhou, L.; Wu, J. GIS-Based Multi-Criteria Analysis for Hospital Site Selection in Haidian District of Beijing. 2012. Available online: https://www.diva-portal.org/smash/record.jsf?pid=diva2:555935 (accessed on 4 November 2021).
- Al-Assar, K.A.M. The Assessment and Planning of Health Services in the Middle Governorate of the Gaza Strip Using Geographic Information System. Master’s Thesis, The Islamic University Gaza, Gaza, Palestine, 2014. [Google Scholar]
- Almansi, K.Y.M. Evaluation of the Service Areas and Accessibility of the Tertiary Hospitals Using GIS in Gaza Strip. Master’s Thesis, Universiti Putra Malaysia, Serdang, Malaysia, 2016. [Google Scholar]
- Kumar, M.; Mario Denis, D.; Mohammad Ali Gabril, E.; Nath, S.; Paul, A.; Mukesh Kumar, C. Site Suitability Analysis for Urban Development Using Geospatial Technologies and AHP: A Case Study in Prayagraj, Uttar Pradesh, India. Pharma Innov. J. 2019, 8, 676–681. [Google Scholar]
- LaGro, J.A., Jr. Site Analysis: Informing Context-Sensitive and Sustainable site Planning and Design; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Samani, Z.N.; Karimi, M.; Alesheikh, A.A. A novel approach to site selection: Collaborative multi-Criteria decision making through geo-social network (Case study: Public parking). ISPRS Int. J. Geo-Inf. 2018, 7, 82. [Google Scholar] [CrossRef] [Green Version]
- Jebur, M.N. Universiti Putra Malaysia Multi Remote Sensing Data in Landslide Detection and Modelling. 2015. Available online: http://psasir.upm.edu.my/id/eprint/58131/1/FK2015105IR.pdf (accessed on 4 November 2021).
- Mojaddadi, H.R. Flood Risk Assessment Using Multi-Sensor Remote Sensing, Geographic Information System, 2D Hydraulic and Machine Learning Based Models. 2018. Available online: https://opus.lib.uts.edu.au/handle/10453/133315 (accessed on 4 November 2021).
- Tehrany, M.S.; Kumar, L.; Shabani, F. A novel GIS-based ensemble technique for flood susceptibility mapping using evidential belief function and support vector machine: Brisbane. Aust. Peer J. 2019, 7, e7653. [Google Scholar] [CrossRef]
- Ornella, L.; Tapia, E. Supervised machine learning and heterotic classification of maize (Zea mays L.) using molecular marker data. Comput. Electron. Agric. 2010, 74, 250–257. [Google Scholar] [CrossRef]
- Xiong, J.; Li, J.; Cheng, W.; Wang, N.; Guo, L. A GIS-based support vector machine model for flash flood vulnerability assessment and mapping in China. ISPRS Int. J. Geo-Inf. 2019, 8, 297. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Singh, K.K. Satellite image classification using Genetic Algorithm trained radial basis function neural network, application to the detection of flooded areas. J. Vis. Commun. Image Represent. 2017, 42, 173–182. [Google Scholar] [CrossRef]
- Tehrany, M.S.; Pradhan, B.; Jebur, M.N. Flood susceptibility analysis and its verification using a novel ensemble support vector machine and frequency ratio method. Stoch. Environ. Res. Risk Assess. 2015, 29, 1149–1165. [Google Scholar] [CrossRef]
- Pandey, V.K.; Pourghasemi, H.R.; Sharma, M.C. Landslide susceptibility mapping using maximum entropy and support vector machine models along the highway corridor, Garhwal Himalaya. Geocarto Int. 2020, 35, 168–187. [Google Scholar] [CrossRef]
- Pham, B.T.; Tien Bui, D.; Prakash, I.; Dholakia, M.B. Hybrid integration of Multilayer Perceptron Neural Networks and machine learning ensembles for landslide susceptibility assessment at Himalayan area (India) using GIS. Catena 2017, 149, 52–63. [Google Scholar] [CrossRef]
- Bui, D.T.; Tuan, T.A.; Klempe, H.; Pradhan, B.; Revhaug, I. Spatial prediction models for shallow landslide hazards: A comparative assessment of the efficacy of support vector machines, artificial neural networks, kernel logistic regression, and logistic model tree. Landslides 2016, 13, 361–378. [Google Scholar]
- Thach, N.N.; Ngo DB, T.; Xuan-Canh, P.; Hong-Thi, N.; Thi, B.H.; Nhat-Duc, H.; Dieu, T.B. Spatial pattern assessment of tropical forest fire danger at Thuan Chau area (Vietnam) using GIS-based advanced machine learning algorithms: A comparative study. Ecol. Inform. 2018, 46, 74–85. [Google Scholar] [CrossRef]
- Stojanova, D.; Panov, P.; Kobler, A.; Džeroski, S. Learning to predict forest fires with different data mining techniques. In Proceedings of the Data Mining and Data Warehouses (SiKDD 2006), Ljubljana, Slovenia, 17 October 2006. [Google Scholar]
- Kim, G.B. A study on the establishment of groundwater protection area around a saline waterway by combining artificial neural network and GIS-based AHP. Environ. Earth Sci. 2020, 79, 117. [Google Scholar] [CrossRef]
- Lu, F.; Zhang, H.; Liu, W. Development and application of a GIS-based artificial neural network system for water quality prediction: A case study at the Lake Champlain area. J. Oceanol. Limnol. 2019, 38, 1835–1845. [Google Scholar] [CrossRef]
- Maier, H.R.; Dandy, G.C. Neural networks for the prediction and forecasting of water resources variables: A review of modelling issues and applications. Environ. Model. Softw. 2000, 15, 101–124. [Google Scholar] [CrossRef]
- Chatterjee, D.; Mukherjee, B. Potential hospital location selection using AHP: A study in rural India. Int. J. Comput. Appl. 2013, 71, 1–7. [Google Scholar] [CrossRef]
- Kahraman, C.; Gundogdu, F.K.; Onar, S.C.; Oztaysi, B. Hospital Location Selection Using Spherical Fuzzy TOPSIS. In Proceedings of the 2019 Conference of the International Fuzzy Systems Association and the European Society for Fuzzy Logic and Technology (EUSFLAT 2019), Prague, Czech Republic, 9–13 September 2019; Atlantis Press: Prague, Czech Republic, 2019. [Google Scholar]
- Dey, P.K.; Ramcharan, E.K. Analytic hierarchy process helps select site for limestone quarry expansion in Barbados. J. Environ. Manag. 2008, 88, 1384–1395. [Google Scholar] [CrossRef]
- Saaty, T. The Analytic Hierarchy Process; McGraw-Hill: New York, NY, USA, 1980. [Google Scholar]
- Wu, C.R.; Lin, C.T.; Chen, H.C. Optimal selection of location for Taiwanese hospitals to ensure a competitive advantage by using the analytic hierarchy process and sensitivity analysis. Build. Environ. 2007, 42, 1431–1444. [Google Scholar] [CrossRef]
- Lin, C.T.; Tsai, M.C. Development of an expert selection system to choose ideal cities for medical service ventures. Expert Syst. Appl. 2009, 36, 2266–2274. [Google Scholar] [CrossRef]
- Vahidnia, M.H.; Alesheikh, A.A.; Alimohammadi, A. Hospital site selection using fuzzy AHP and its derivatives. J. Environ. Manag. 2009, 90, 3048–3056. [Google Scholar] [CrossRef]
- Aydın, Ö. Hospital Location for Ankara with Fuzzy AHP. Dokuz Eylül Univ. Fac. Econ. Adm. Sci. J. 2009, 24, 87–104. [Google Scholar]
- Soltani, A.; Marandi, E.Z. Hospital site selection using two-stage fuzzy multi-criteria decision-making process. J. Urban Environ. Eng. 2011, 5, 32–43. [Google Scholar] [CrossRef]
- Ahmad, I.; Basheri, M.; Iqbal, M.J.; Rahim, A. Performance comparison of support vector machine, random forest, and extreme learning machine for intrusion detection. IEEE Access 2018, 6, 33789–33795. [Google Scholar] [CrossRef]
- Hall, M.A. Correlation-Based Feature Selection for Machine Learning. Ph.D. Thesis, University of Waikato, Hamilton, New Zealand, 1999. [Google Scholar]
- Onik, A.R.; Haq, N.F.; Alam, L.; Mamun, T.I. An analytical comparison on filter feature extraction method in data mining using J48 classifier. Int. J. Comput. Appl. 2015, 124, 1–8. [Google Scholar]
- Sahoo, G.; Kumar, Y. Analysis of parametric & non parametric classifiers for classification technique using WEKA. Int. J. Inf. Technol. Comput. Sci. 2012, 4, 43. [Google Scholar]
- Sadeghi, R.; Zarkami, R.; Sabetraftar, K.; Van Damme, P. Application of genetic algorithm and greedy stepwise to select input variables in classification tree models for the prediction of habitat requirements of Azolla filiculoides (Lam.) in Anzali wetland, Iran. Ecol. Model. 2013, 251, 44–53. [Google Scholar] [CrossRef]
- Wald, R.; Khoshgoftaar, T.M.; Napolitano, A. Optimizing wrapper-based feature selection for use on bioinformatics data. In Proceedings of the The Twenty-Seventh International Flairs Conference, Pensacola Beach, FL, USA, 21–23 May 2014. [Google Scholar]
- Walker, A.L. Machine learning in geosciences and remote sensing. Geosci. Front. 2016, 7, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Gardner, M.W.; Dorling, S.R. Artificial neural networks (the multilayer perceptron)—A review of applications in the atmospheric sciences. Atmos. Environ. 1998, 32, 2627–2636. [Google Scholar] [CrossRef]
- Adeyemo, O.O.; Adeyeye, T.O.; Ogunbiyi, D. Comparative study of ID3/C4. 5 decision tree and multilayer perceptron algorithms for the prediction of typhoid fever. Afr. J. Comput. ICT 2015, 8, 103–112. [Google Scholar]
- Haykin, S. Neural Networks and Learning Machines, 3/E; Pearson Education India: Delhi, India, 2010. [Google Scholar]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Jain, P.; Garibaldi, J.M.; Hirst, J.D. Supervised machine learning algorithms for protein structure classification. Comput. Biol. Chem. 2009, 33, 216–223. [Google Scholar] [CrossRef]
- Bao, Y.; Hu, Z.; Xiong, T. A PSO and pattern search based memetic algorithm for SVMs parameters optimization. Neurocomputing 2013, 117, 98–106. [Google Scholar] [CrossRef] [Green Version]
- Friedrichs, F.; Igel, C. Evolutionary tuning of multiple SVM parameters. Neurocomputing 2005, 64, 107–117. [Google Scholar] [CrossRef]
- Lorena, A.C.; De Carvalho, A.C. Evolutionary tuning of SVM parameter values in multiclass problems. Neurocomputing 2008, 71, 3326–3334. [Google Scholar] [CrossRef]
- Bamakan SM, H.; Wang, H.; Yingjie, T.; Shi, Y. An effective intrusion detection framework based on MCLP/SVM optimized by time-varying chaos particle swarm optimization. Neurocomputing 2016, 199, 90–102. [Google Scholar] [CrossRef]
- Shelke, M.B.; Badade, K.B. Processing of Incomplete Data Sets: Prediction of Missing Values by using Multiple Regression. Int. J. Comput. Electron. Res. 2013, 2, 5. [Google Scholar]
- Al-Qutob, M.A.; Al-Rimawi, F. Analysis of Different Rare Metals, and Rare Earth Metals in Harvested Rain Water in Gaza Strip/Palestine by ICP/MS-Data and Health Aspects. Sci. Res. Publ. 2016, 8, 905–912. [Google Scholar] [CrossRef] [Green Version]
- Palestinian Central Bureau of Statistics (PCBS). Statistical Year Book of Palestine; PCBS: Ramallah, Palestine, 2017.
- El Baba, M.; Kayastha, P.; Huysmans, M.; De Smedt, F. Evaluation of the groundwater quality using the water quality index and geostatistical analysis in the Dier al-Balah Governorate, Gaza Strip, Palestine. Water 2020, 12, 262. [Google Scholar] [CrossRef] [Green Version]
- Ajjur, S.B.; Mogheir, Y.K. Flood hazard mapping using a multi-criteria decision analysis and GIS (case study Gaza Governorate, Palestine). Arab. J. Geosci. 2020, 13, 1–11. [Google Scholar] [CrossRef]
- Miller, A.J. Assessing landslide susceptibility by incorporating the surface cover index as a measurement of vegetative cover. Land Degrad. Dev. 2013, 24, 205–227. [Google Scholar] [CrossRef]
- Mojaddadi, H.; Pradhan, B.; Nampak, H.; Ahmad, N.; Ghazali AH, B. Ensemble machine-learning-based geospatial approach for flood risk assessment using multi-sensor remote-sensing data and GIS. Geomatics. Nat. Hazards Risk 2017, 8, 1080–1102. [Google Scholar] [CrossRef] [Green Version]
- Tehrany, M.S.; Pradhan, B.; Jebur, M.N. Flood susceptibility mapping using a novel ensemble weights-of-evidence and support vector machine models in GIS. J. Hydrol. 2014, 512, 332–343. [Google Scholar] [CrossRef]
- Pham, B.T.; Tien Bui, D.; Dholakia, M.B.; Prakash, I.; Pham, H.V. A Comparative Study of Least Square Support Vector Machines and Multiclass Alternating Decision Trees for Spatial Prediction of Rainfall-Induced Landslides in a Tropical Cyclones Area. Geotech. Geol. Eng. 2016, 34, 1807–1824. [Google Scholar] [CrossRef]
- Kalantar, B.; Ueda, N.; Idrees, M.O.; Janizadeh, S.; Ahmadi, K.; Shabani, F. Forest Fire Susceptibility Prediction Based on Machine Learning Models with Resampling Algorithms on Remote Sensing Data. Remote Sens. 2020, 12, 3682. [Google Scholar] [CrossRef]
- Chen, W.; Yan, X.; Zhao, Z.; Hong, H.; Bui, D.T.; Pradhan, B. Spatial prediction of landslide susceptibility using data mining-based kernel logistic regression, naive Bayes and RBFNetwork models for the Long County area (China). Bull. Eng. Geol. Environ. 2019, 78, 247–266. [Google Scholar] [CrossRef]
- McLafferty, S.L. GIS and health care. Annu. Rev. Public Health 2003, 24, 25–42. [Google Scholar] [CrossRef]
- Maantay, J.A.; Maroko, A.R.; Herrmann, C. Mapping population distribution in the urban environment: The Cadastral-based expert dasymetric system (CEDS). Cartogr. Geogr. Inf. Sci. 2007, 34, 77–102. [Google Scholar] [CrossRef]
- Devkota, K.C.; Regmi, A.D.; Pourghasemi, H.R.; Yoshida, K.; Pradhan, B.; Ryu, I.C.; Dhital, M.R.; Althuwaynee, O.F. Landslide susceptibility mapping using certainty factor, index of entropy and logistic regression models in GIS and their comparison at Mugling-Narayanghat road section in Nepal Himalaya. Nat. Hazards 2013, 65, 135–165. [Google Scholar] [CrossRef]
- Youzi, H.; Nemati, G.; Emamgholi, S. The Optimized Location of Hospital Using an Integrated Approach GIS and Analytic Hierarchy Process: A Case Study of Kohdasht City. Int. J. Econ. Manag. Sci. 2018, 7. [Google Scholar] [CrossRef]
- Dai, F.C.; Lee, C.F. Landslide characteristics and slope instability modeling using GIS, Lantau Island, Hong Kong. Geomorphology 2002, 42, 213–228. [Google Scholar] [CrossRef]
- Ayalew, L.; Yamagishi, H.; Ugawa, N. Landslide susceptibility mapping using GIS-based weighted linear combination, the case in Tsugawa area of Agano River, Niigata Prefecture, Japan. Landslides 2004, 1, 73–81. [Google Scholar] [CrossRef]
- Gómez, H.; Kavzoglu, T. Assessment of shallow landslide susceptibility using artificial neural networks in Jabonosa River Basin, Venezuela. Eng. Geol. 2005, 78, 11–27. [Google Scholar] [CrossRef]
- Lawther, A. The Application of GIS-Based Binary Logistic Regression for Slope Failure Susceptibility Mapping in the Western Grampian Mountains, Scotland. 2008. Available online: http://lup.lub.lu.se/student-papers/record/3558914 (accessed on 4 November 2021).
- Conforti, M.; Pascale, S.; Robustelli, G.; Sdao, F. Evaluation of prediction capability of the artificial neural networks for mapping landslide susceptibility in the Turbolo River catchment (northern Calabria, Italy). Catena 2014, 113, 236–250. [Google Scholar] [CrossRef]
- Moore, I.D.; Wilson, J.P. Length-slope factors for the revised universal soil loss equation: Simplified method of estimation. J. Soil Water Conserv. 1992, 47, 423–428. [Google Scholar]
- Bui, D.T.; Ho, T.C.; Revhaug, I.; Pradhan, B.; Nguyen, D.B. Landslide susceptibility mapping along the national road 32 of Vietnam using GIS-based J48 decision tree classifier and its ensembles. In Cartography from Pole to Pole; Springer: Berlin/Heidelberg, Germany, 2014; pp. 303–317. [Google Scholar]
- Beven, K.J.; Kirkby, M.J.; Kirkby, A.J. A physically based, variable contributing area model of basin hydrology/Un modèle à base physique de zone d’appel variable de l’hydrologie du bassin versant) A physically based, variable contributing area model of basin hydrology/Un modèle à base physique de zone d’appel variable de l’hydrologie du bassin versant A physically based, variable contributing area model of basin hydrology. Hydrol. Sci. J. 1979, 24, 43–69. [Google Scholar] [CrossRef] [Green Version]
- Althuwaynee, O.F.; Pradhan, B.; Park, H.J.; Lee, J.H. A novel ensemble bivariate statistical evidential belief function with knowledge-based analytical hierarchy process and multivariate statistical logistic regression for landslide susceptibility mapping. Catena 2014, 114, 21–36. [Google Scholar] [CrossRef]
- Riley, S.J.; DeGloria, S.D.; Elliot, R. Index that quantifies topographic heterogeneity. Intermt. J. Sci. 1999, 5, 23–27. [Google Scholar]
- Katla, S.; Xu, D.; Wu, Y.; Pan, Q.; Wu, X. DPWeka: Achieving Differential Privacy in WEKA. In Proceedings of the 2017 IEEE Symposium on Privacy-Aware Computing, PAC 2017, Washington, DC, USA, 1–4 August 2017. [Google Scholar] [CrossRef] [Green Version]
- Hall, M. Correlation-Based Feature Selection for Discrete and Numeric Class Machine Learning. Ph.D. Thesis, University of Waikato, Hamilton, New Zealand, 2000. [Google Scholar]
- Pourhashemi, S.; Mashalizadeh, A. A Novel Feature Selection Method Using CFS with Greedy-Stepwise Search Algorithm in e-mail Spam Filtering; AMO—Advanced Modeling and Optimization: 2013. Available online: https://camo.ici.ro/journal/vol15/v15c21.pdf (accessed on 4 November 2021).
- Guyon, I.; Elisseeff, A. An introduction to variable and feature selection. J. Mach. Learn. Res. 2003, 3, 1157–1182. [Google Scholar]
- Mayfield, C.J. Automating the Classification of Thematic Rasters for Weighted Overlay Analysis in GeoPlanner for ArcGIS. Ph.D. Thesis, University of Redlands, Redlands, CA, USA, 2015. [Google Scholar]
- Borra, S.; Di Ciaccio, A. Measuring the prediction error. A comparison of cross-validation, bootstrap and covariance penalty methods. Comput. Stat. Data Anal. 2010, 54, 2976–2989. [Google Scholar] [CrossRef]
- Azeez, O.S.; Pradhan, B.; Shafri, H.Z.; Shukla, N.; Lee, C.W.; Rizeei, H.M. Modeling of CO emissions from traffic vehicles using artificial neural networks. Appl. Sci. 2019, 9, 313. [Google Scholar] [CrossRef] [Green Version]
- Idrees, M.O.; Pradhan, B. Hybrid Taguchi-Objective Function optimization approach for automatic cave bird detection from terrestrial laser scanning intensity image. Int. J. Speleol. 2016, 45, 289–301. [Google Scholar] [CrossRef] [Green Version]
- Murata, N.; Yoshizawa, S.; Amari, S.I. Network information criterion-determining the number of hidden units for an artificial neural network model. IEEE Trans. Neural Netw. 1994, 5, 865–872. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.; Cai, N.; Pacheco, P.P.; Narrandes, S.; Wang, Y.; Xu, W. Applications of support vector machine (SVM) learning in cancer genomics. Cancer Genom. Proteom. 2018, 15, 41–51. [Google Scholar]
- Noble, W.S. What is a support vector machine? Nat. Biotechnol. 2006, 24, 1565. [Google Scholar] [CrossRef]
- Krell, M.M. Generalizing, decoding, and optimizing support vector machine classification. arXiv preprint 2018, arXiv:1801.04929. [Google Scholar]
- Hoang, N.D.; Bui, D.T.; Liao, K.W. Groutability estimation of grouting processes with cement grouts using differential flower pollination optimized support vector machine. Appl. Soft Comput. 2016, 45, 173–186. [Google Scholar] [CrossRef]
- Hoang, N.D.; Tien Bui, D. A novel relevance vector machine classifier with cuckoo search optimization for spatial prediction of landslides. J. Comput. Civ. Eng. 2016, 30, 04016001. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Values | Relative Influence % |
|---|---|---|
| Population density | Density of population | 100% |
| Road | Distance from the road | 100% |
| Main road | Distance from the main road | 90% |
| Residential | Distance from the residential | 90% |
| Agriculture | Distance from the agriculture | 70% |
| Population | Populations number | 70% |
| Slope | Slope degree | 60% |
| Curvature | Plan curvature | 50% |
| Prohibited zone | No-go zone | 40% |
| Altitude | Altitude | 20% |
| Refugee camp | Distance from the refugee camp | 20% |
| River | Distance from the river | 10% |
| TRI | Topographic roughness index | 0% |
| TWI | Topographic wetness index | 0% |
| SPI | Stream power index | 0% |
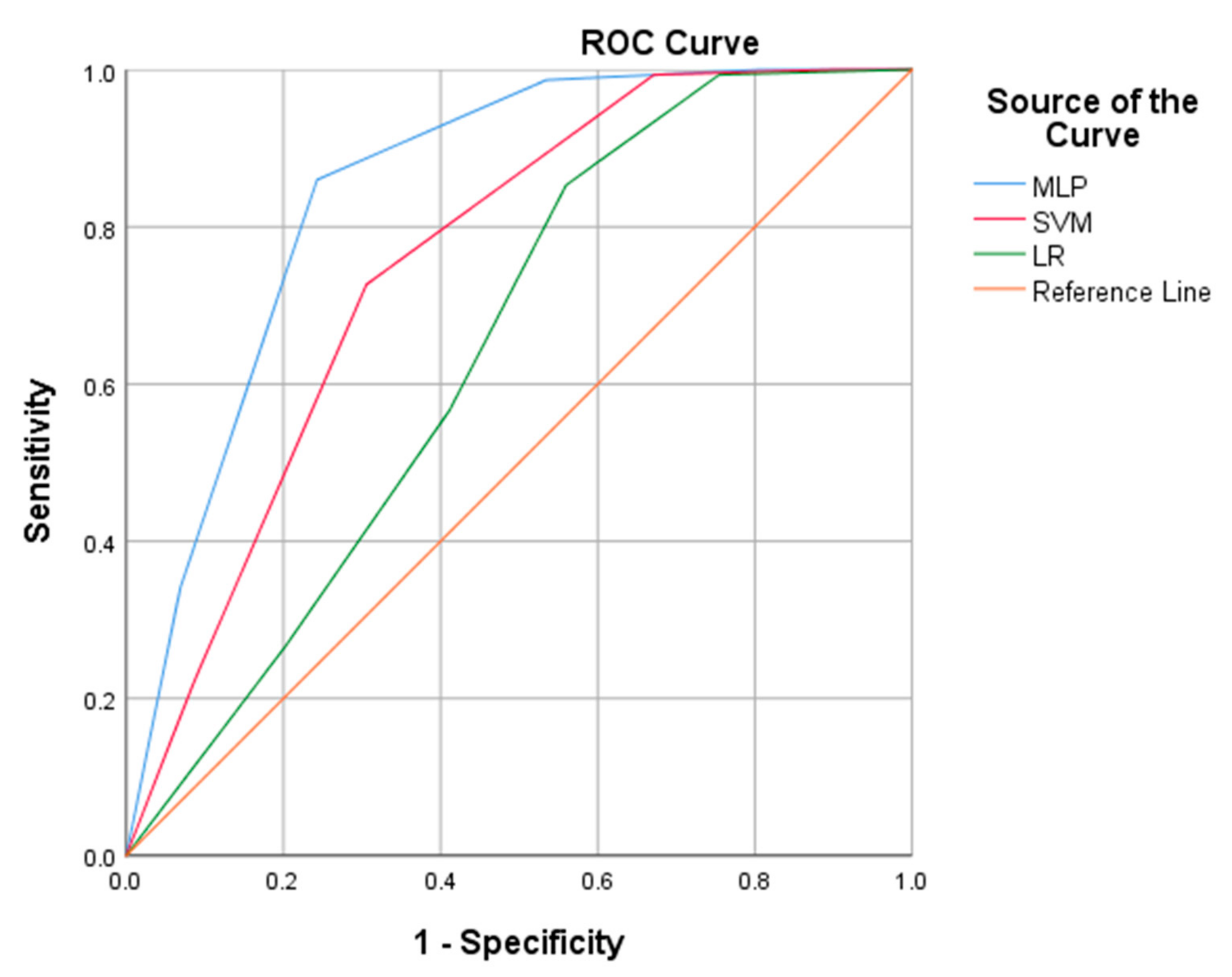
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| Model | AUC | Std Error | Lower Bound | Upper Bound | |
| MLP | 0.849 | 0.017 | 0.816 | 0.883 | |
| SVM | 0.756 | 0.021 | 0.714 | 0.798 | |
| LR | 0.644 | 0.024 | 0.596 | 0.692 | |
| 10-Fold cross-correlation method | |||||
| R2 | MAE | RMSE | RAE(%) | RRSE(%) | |
| MLP | 0.925 | 0.070 | 0.231 | 13.62 | 25.20 |
| SVM | 0.940 | 0.011 | 0.001 | 4.18 | 12.23 |
| LR | 0.751 | 0.254 | 0.310 | 19.73 | 40.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almansi, K.Y.; Shariff, A.R.M.; Abdullah, A.F.; Syed Ismail, S.N. Hospital Site Suitability Assessment Using Three Machine Learning Approaches: Evidence from the Gaza Strip in Palestine. Appl. Sci. 2021, 11, 11054. https://doi.org/10.3390/app112211054
Almansi KY, Shariff ARM, Abdullah AF, Syed Ismail SN. Hospital Site Suitability Assessment Using Three Machine Learning Approaches: Evidence from the Gaza Strip in Palestine. Applied Sciences. 2021; 11(22):11054. https://doi.org/10.3390/app112211054
Chicago/Turabian StyleAlmansi, Khaled Yousef, Abdul Rashid Mohamed Shariff, Ahmad Fikri Abdullah, and Sharifah Norkhadijah Syed Ismail. 2021. "Hospital Site Suitability Assessment Using Three Machine Learning Approaches: Evidence from the Gaza Strip in Palestine" Applied Sciences 11, no. 22: 11054. https://doi.org/10.3390/app112211054
APA StyleAlmansi, K. Y., Shariff, A. R. M., Abdullah, A. F., & Syed Ismail, S. N. (2021). Hospital Site Suitability Assessment Using Three Machine Learning Approaches: Evidence from the Gaza Strip in Palestine. Applied Sciences, 11(22), 11054. https://doi.org/10.3390/app112211054