
Unstimulated Parotid Saliva Is a Better Method for Blood Glucose Prediction


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Glucose Collection
2.3. Saliva Glucose Assay
2.4. Statistics
3. Results
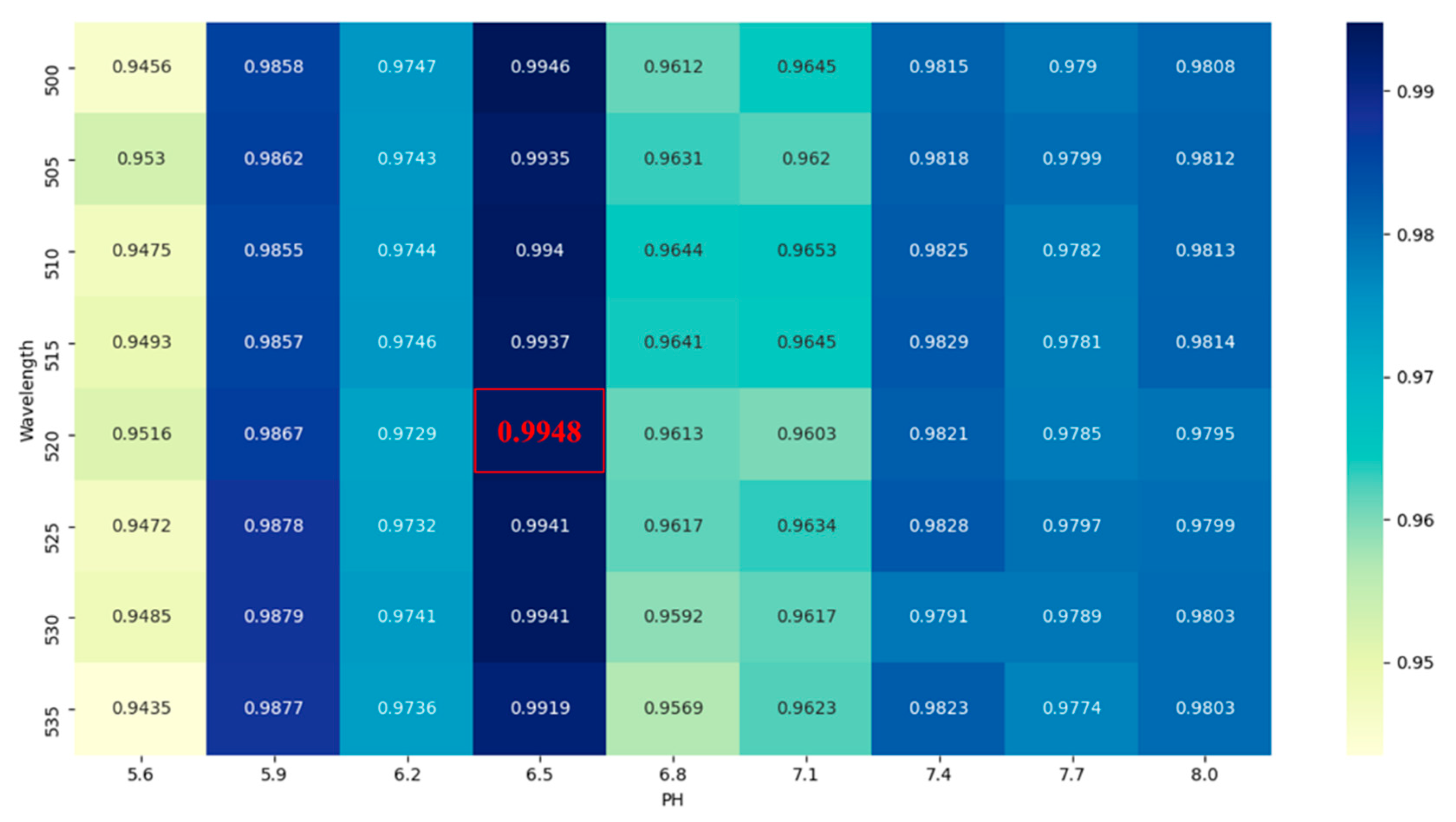
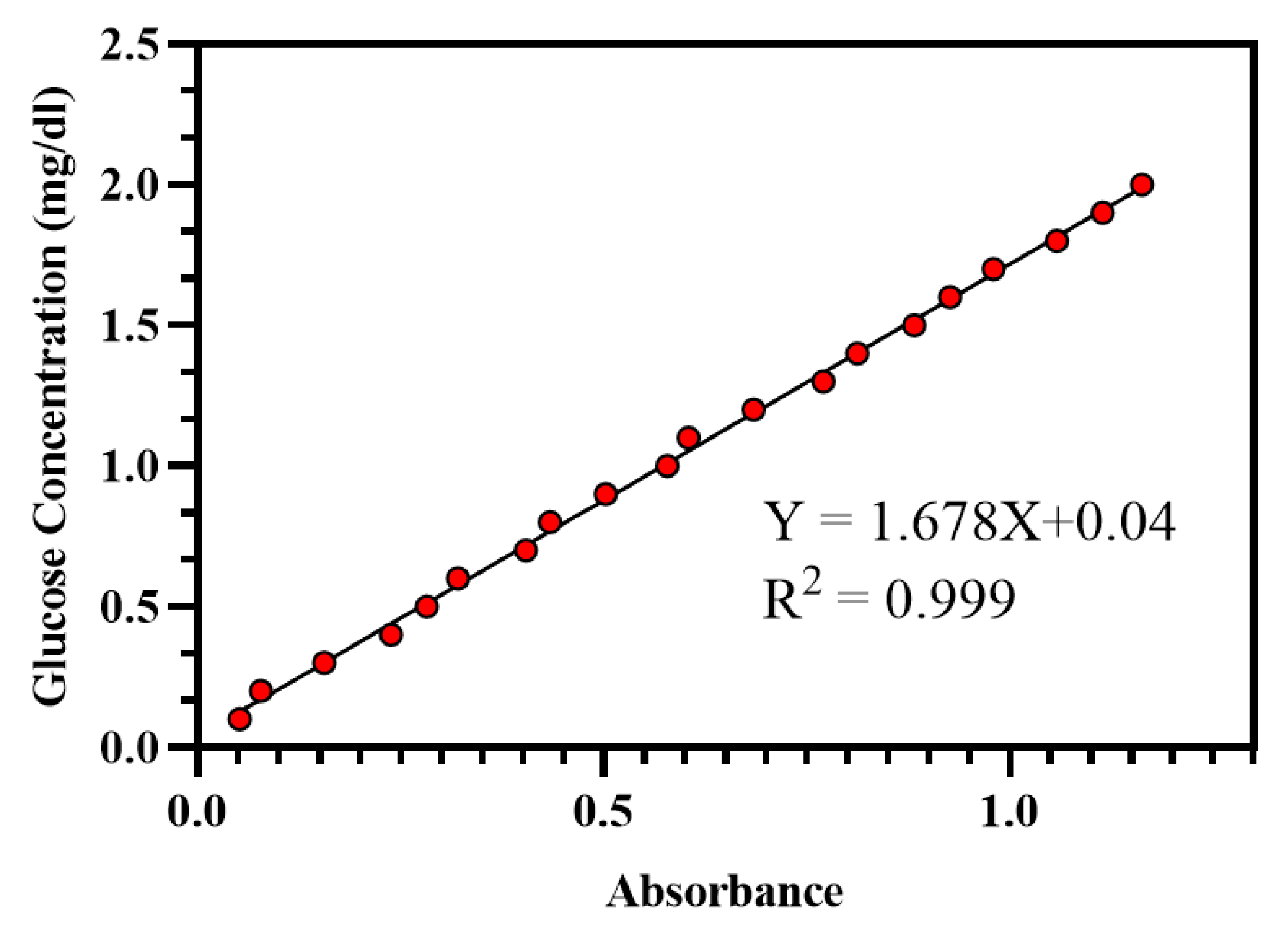
3.1. Saliva Detection Method
3.2. Sample Characteristics
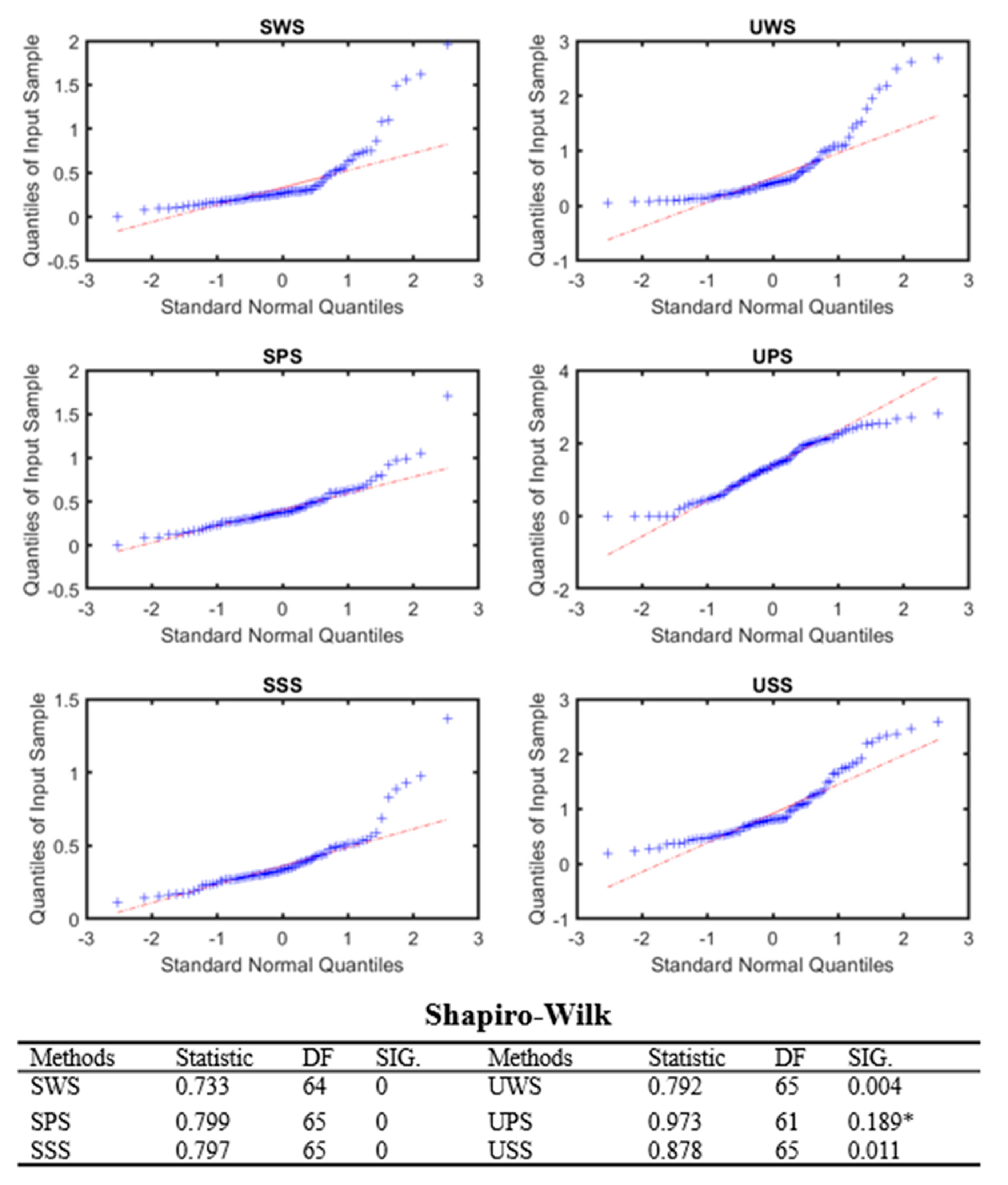
3.3. The Normal Distribution Curve of Each Collection Method
3.4. The Correlation of Blood Glucose and Unstiimulated Saliva Glucose
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- Jovanovi, J.; Mihailovi, M.; Uskokovi, A.; Grdović, N.; Dinić, S.; Vidaković, M. The Effects of Major Mushroom Bioactive Compounds on Mechanisms That Control Blood Glucose Level. J. Fungi—Open Access Mycol. J. 2021, 7, 58–65. [Google Scholar]
- Meyhöfer, S.; Wilms, B.; Ihling, F.; Windjäger, A.; Kalscheuer, H.; Augustinov, A.; Herrmann, V.; Lehnert, H.; Schmid, S.M. Evaluation of a near-infrared light ultrasound system as a non-invasive blood glucose monitoring device. Diabetes Obes. Metab. 2020, 22, 694–698. [Google Scholar] [CrossRef]
- Baghelani, M.; Abbasi, Z.; Daneshmand, M.; Light, P.E. Non-invasive continuous-time glucose monitoring system using a chipless printable sensor based on split ring microwave resonators. Sci. Rep. 2020, 10, 12980. [Google Scholar] [CrossRef]
- Agrawal, R.P.; Sharma, N.; Rathore, M.S.; Gupta, V.B.; Jain, S.; Agarwal, V.; Goyal, S. Noninvasive method for glucose level estimation by saliva. J. Diabetes Metab. 2013, 4, 266. [Google Scholar]
- Arakawa, T.; Kuroki, Y.; Nitta, H.; Chouhan, P.; Toma, K.; Sawada, S.-I.; Takeuchi, S.; Sekita, T.; Akiyoshi, K.; Minakuchi, S.; et al. Mouthguard biosensor with telemetry system for monitoring of saliva glucose: A novel cavitas sensor. Biosens. Bioelectron. 2016, 84, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Caixeta, D.C.; Aguiar, E.; Cardoso-Sousa, L.; Coelho, L.M.D.; Oliveira, S.W.; Espindola, F.S.; Raniero, L.; Crosara, K.T.B.; Baker, M.J.; Siqueira, W.L.; et al. Salivary molecular spectroscopy: A rapid and non-invasive monitoring tool for diabetes mellitus during insulin treatment. PLoS ONE 2019, 15, e0223461. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; Vieira, W.; Siqueira, W.L.; Agostini, B.A.; Moffa, E.B.; Paranhos, L.R. Saliva as a tool for monitoring hemodialysis: A systematic review and meta-analysis. Braz. Oral Res. 2021, 35, e016. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, B.; Choi, C.S.; Lee, K.; Kim, S. Recent trends in the development of diagnostic tools for diabetes mellitus using patient saliva. TrAC Trends Anal. Chem. 2017, 89, 60–67. [Google Scholar] [CrossRef]
- Makaram, P.; Owens, D.; Aceros, J. Trends in nanomaterial-based non-invasive diabetes sensing technologies. Diagnostics 2014, 4, 27–46. [Google Scholar] [CrossRef]
- Lee, H.; Hong, Y.-J.; Baik, S.; Hyeon, T.; Kim, D.-H. Enzyme-based glucose sensor: From invasive to wearable device. Adv. Healthc. Mater. 2018, 7, 1701150. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Chang, S.-J.; Chen, C.-J.; Liu, J.-T. Non-invasive blood glucose monitoring technology: A review. Sensors 2020, 20, 6925. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Sun, H.; Wang, P.; Wang, X. Salivary proteomics in biomedical research. Clin. Chim. Acta 2013, 415, 261–265. [Google Scholar] [CrossRef]
- Al-Tarawneh, S.K.; Border, M.B.; Dibble, C.F.; Bencharit, S. Defining salivary biomarkers using mass spectrometry-based proteomics: A systematic review. Omics A J. Integr. Biol. 2011, 15, 353–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matricali, G.A.; Dereymaeker, G.; Muls, E.; Flour, M.; Mathieu, C. Economic aspects of diabetic foot care in a multidisciplinary setting: A review. Diabetes/Metab. Res. Rev. 2007, 23, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.M.L.; Sørensen, C.E.; Proctor, G.B.; Carpenter, G.; Ekström, J. Salivary secretion in health and disease. J. Oral Rehabil. 2018, 45, 730–746. [Google Scholar] [CrossRef] [PubMed]
- Sigurðardóttir, Á.K. Self-care in diabetes: Model of factors affecting self-care. J. Clin. Nurs. 2005, 14, 301–314. [Google Scholar] [CrossRef]
- Atkinson, K.R.; Lo, K.R.; Payne, S.R.; Mitchell, J.S.; Ingram, J.R. Rapid saliva processing techniques for near real-time analysis of salivary steroids and protein. J. Clin. Lab. Anal. 2008, 22, 395–402. [Google Scholar] [CrossRef]
- Skálová, A.; Stenman, G.; Simpson, R.H.W.; Hellquist, H.; Slouka, D.; Svoboda, T.; Bishop, J.A.; Hunt, J.L.; Nibu, K.-I.; Rinaldo, A.; et al. The role of molecular testing in the differential diagnosis of salivary gland carcinomas. Am. J. Surg. Pathol. 2018, 42, e11–e27. [Google Scholar] [CrossRef]
- Pappa, E.; Vastardis, H.; Rahiotis, C. Chair-side saliva diagnostic tests: An evaluation tool for xerostomia and caries risk assessment in children with type 1 diabetes. J. Dent. 2020, 93, 103224. [Google Scholar] [CrossRef]
- Tettamanti, G.; Bassi, R.; Viani, P.; Riboni, L. Salvage pathways in glycosphingolipid metabolism. Biochimie 2003, 85, 423–437. [Google Scholar] [CrossRef]
- Jurysta, C.; Bulur, N.; Oguzhan, B.; Satman, I.; Yilmaz, T.M.; Malaisse, W.J.; Sener, A. Salivary glucose concentration and excretion in normal and diabetic subjects. J. Biomed. Biotechnol. 2009, 2009, 430426. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, A.C.U.; Soares, M.S.M.; Almeida, P.C.; Soares, T.C. Comparative study of the concentration of salivary and blood glucose in type 2 diabetic patients. J. Oral Sci. 2010, 52, 293–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Wong, D.T. Saliva: An emerging biofluid for early detection of diseases. Am. J. Dent. 2009, 22, 241. [Google Scholar]
- Goudet, G.; Nadal-Desbarats, L.; Douet, C.; Savoie, J.; Staub, C.; Venturi, E.; Ferchaud, S.; Boulot, S.; Prunier, A. Salivary and urinary metabolome analysis for pre-puberty-related biomarkers identification in porcine. Animal 2019, 13, 760–770. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Sandhu, S.V.; Bansal, H.; Sharma, D. Comparison of salivary and serum glucose levels in diabetic patients. J. Diabetes Sci. Technol. 2014, 9, 91–96. [Google Scholar] [CrossRef]
- Panchbhai, A.S. Correlation of salivary glucose level with blood glucose level in diabetes mellitus. J. Oral Maxillofac. Res. 2012, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Dhanya, M.; Hegde, S. Salivary glucose as a diagnostic tool in Type II diabetes mellitus: A case-control study. Niger. J. Clin. Pract. 2016, 19, 486–490. [Google Scholar] [CrossRef]
- Vuletic, L.; Spalj, S.; Rogic, D.; Peros, K. The rise in glucose concentration in saliva samples mixed with test foods monitored using a glucometer: An observational pilot study. J. Oral Biosci. 2019, 61, 201–206. [Google Scholar] [CrossRef]
- Takeda, I.; Stretch, C.; Barnaby, P.; Bhatnager, K.; Rankin, K.; Fu, H.; Weljie, A.; Jha, N.; Slupsky, C. Understanding the human salivary metabolome. NMR Biomed. 2010, 22, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Jha, S.K.; David, C.M.; Saluja, I.P.; Venkatesh, D.; Chaudhary, S.U. Estimation of salivary glucose level and plasma glucose level in subjects with and without diabetes mellitus: A comparative study. Natl. J. Integr. Res. Med. 2013, 5, 65–70. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NaCl Concentration | Absorbance of Different Glucose Concentration | R2 | Sy. x | ||
|---|---|---|---|---|---|
| 0.5 mg/dL | 1 mg/dL | 1.5 mg/dL | |||
| 1 mg/dL | 0.268 ± 0.05 | 0.572 ± 0.15 | 0.762 ± 0.17 | 0.9826 | 0.04654 |
| 3 mg/dL | 0.264 ± 0.09 | 0.474 ± 0.13 | 0.836 ± 0.28 | 0.977 | 0.06205 |
| 5 mg/dL | 0.28 ± 0.09 | 0.558 ± 0.12 | 0.826 ± 0.27 | 0.9999 ** | 0.004082 ** |
| 7 mg/dL | 0.3 ± 0.05 | 0.654 ± 0.28 | 0.75 ± 0.22 | 0.9012 | 0.1053 |
| 9 mg/dL | 0.238 ± 0.03 | 0.564 ± 015 | 0.902 ± 0.23 | 0.9999 * | 0.004899 * |
| 11 mg/dL | 0.262 ± 0.15 | 0.654 ± 0.25 | 1.302 ± 0.61 | 0.9802 | 0.1045 |
| 13 mg/dL | 0.25 ± 0.15 | 0.592 ± 0.31 | 0.992 ± 0.45 | 0.998 | 0.02368 |
| 15 mg/dL | 0.266 ± 0.07 | 0.504 ± 0.21 | 0.782 ± 0.36 | 0.998 | 0.01633 |
| 17 mg/dL | 0.368 ± 0.19 | 0.53 ± 0.19 | 0.872 ± 0.24 | 0.9592 | 0.07348 |
| 19 mg/dL | 0.254 ± 0.21 | 0.506 ± 0.11 | 0.744 ± 0.33 | 0.9997 | 0.005715 |
| Collection Methods | UWS | SWS | UPS | SPS | USS | SSS |
|---|---|---|---|---|---|---|
| SFR (μL/min) | 1347 ± 322 | 1632 ± 314 | 113 ± 21 | 145 ± 55 | 413 ± 89 | 571 ± 111 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Y.; Zhang, H.; Zhu, J.; Peng, L.; Duan, Z.; Liu, T.; Zuo, J.; Xing, L.; Liao, Z.; Wang, S.; et al. Unstimulated Parotid Saliva Is a Better Method for Blood Glucose Prediction. Appl. Sci. 2021, 11, 11367. https://doi.org/10.3390/app112311367
Cui Y, Zhang H, Zhu J, Peng L, Duan Z, Liu T, Zuo J, Xing L, Liao Z, Wang S, et al. Unstimulated Parotid Saliva Is a Better Method for Blood Glucose Prediction. Applied Sciences. 2021; 11(23):11367. https://doi.org/10.3390/app112311367
Chicago/Turabian StyleCui, Yangyang, Hankun Zhang, Jia Zhu, Lu Peng, Zhili Duan, Tian Liu, Jiasheng Zuo, Lu Xing, Zhenhua Liao, Song Wang, and et al. 2021. "Unstimulated Parotid Saliva Is a Better Method for Blood Glucose Prediction" Applied Sciences 11, no. 23: 11367. https://doi.org/10.3390/app112311367
APA StyleCui, Y., Zhang, H., Zhu, J., Peng, L., Duan, Z., Liu, T., Zuo, J., Xing, L., Liao, Z., Wang, S., & Liu, W. (2021). Unstimulated Parotid Saliva Is a Better Method for Blood Glucose Prediction. Applied Sciences, 11(23), 11367. https://doi.org/10.3390/app112311367