1. Introduction
Obesity is a prominent disease around the world. According to WHO, global obesity has nearly tripled since the 1970s [
1]. This is a topic of concern because gaining weight is a risk factor for the noncommunicable diseases and the prevalence is still increasing globally [
2].
Despite the efforts and the various strategies outlined by the different agencies and nations, no significant changes have been achieved that contribute to changing this reality [
3].
However, healthy lifestyles behavior has become an important strategy to avoid excessive caloric intake. Having a good level of adherence to a diet, despite the nutritional strategy, guarantees better results [
4,
5,
6]. According to Pagoto et al. [
6], adherence is defined as “the degree to which participants continued in the program or met program goals for diet and physical activity”. Taking into consideration that the use of mobile phones is rising around the world [
7] and people tend to have a strong attachment to them, especially young people [
8,
9], Health Mobile Apps could act as a strategic tool to empower consumers’ knowledge in order to support weight loss and reach the desired adherence, at least in the short term [
10].
Computational technologies such as artificial intelligence, machine learning, and deep learning could help to offer an integrated framework of the patient information, improving not only the diagnosis but also the recommendations in individuals [
11]. Classic dietary assessment methods are prone to have measurement errors [
12], whereas new technologies could help to measure in a more accurate way as well as reduce costs.
According to a recent review, health professionals do not always tend to recommend these types of apps because of their limitations: food composition is inaccurate, they do not have local food composition, there is a need for some technical expertise, poor quality, poor usability, inaccurate database, inaccurate energy calculations, or because they are not personalized [
13].
On the other hand, individuals tend to underreport due to poor image quality or negligence, or because they estimate the portions erroneously [
14].
Despite the fact that there is an increasing number of reviews analyzing mobile apps utility, there is still an important gap in knowledge, since there is a significant heterogeneity in the types of apps available in the mobile market. Some tend to focus on one nutritional outcome; others tend to investigate a specific target group or different behaviors [
15].
In the present paper, the authors provide a description of the status of the different recommender systems and analyze the involving machine learning algorithms used, in order to find out if they accomplish their purpose.
The article is structured as follows:
Section 2 explains how the method used in the systematic review was developed;
Section 3 provides an analysis of records; lastly,
Section 4 contains the discussion and conclusions about future work.
2. Material and Methods
The purpose of the SRL is to determine the current situation of the different recommender systems used in the nutrition and health areas, also involving machine learning algorithms. Research manuscripts reporting large datasets that are deposited in a publicly available database should specify where the data have been deposited and provide the relevant accession numbers. If the accession numbers have not yet been obtained at the time of submission, please state that they will be provided during review. They must be provided prior to publication.
Review Protocol
Firstly, the different objectives and search questions were defined (
Table 1), and the following databases were used: (1) ACM was used as the main digital library of scientific content in the area of informatics and computing, (2) Scopus was taken into account as a database that has access to important different research in different areas of knowledge, and (3) PubMed was used as a more specific dataset related to the health area. No filter was used for the population filter; all available items were used.
Considering the mapping of the literature, the keywords were selected; these are the words that have been used: Nutrition, Recommendation System (recommender system), and Machine Learning. A more precise search was possible due to the advanced searches of the different repositories, which enables to search using logical operators. The terms “Recommendation System” AND “Nutrition” were searched all through the full texts, AND “Machine Learning” just in the author keywords.
Table 2 shows the records obtained for each database between the years 2016 and 2021.
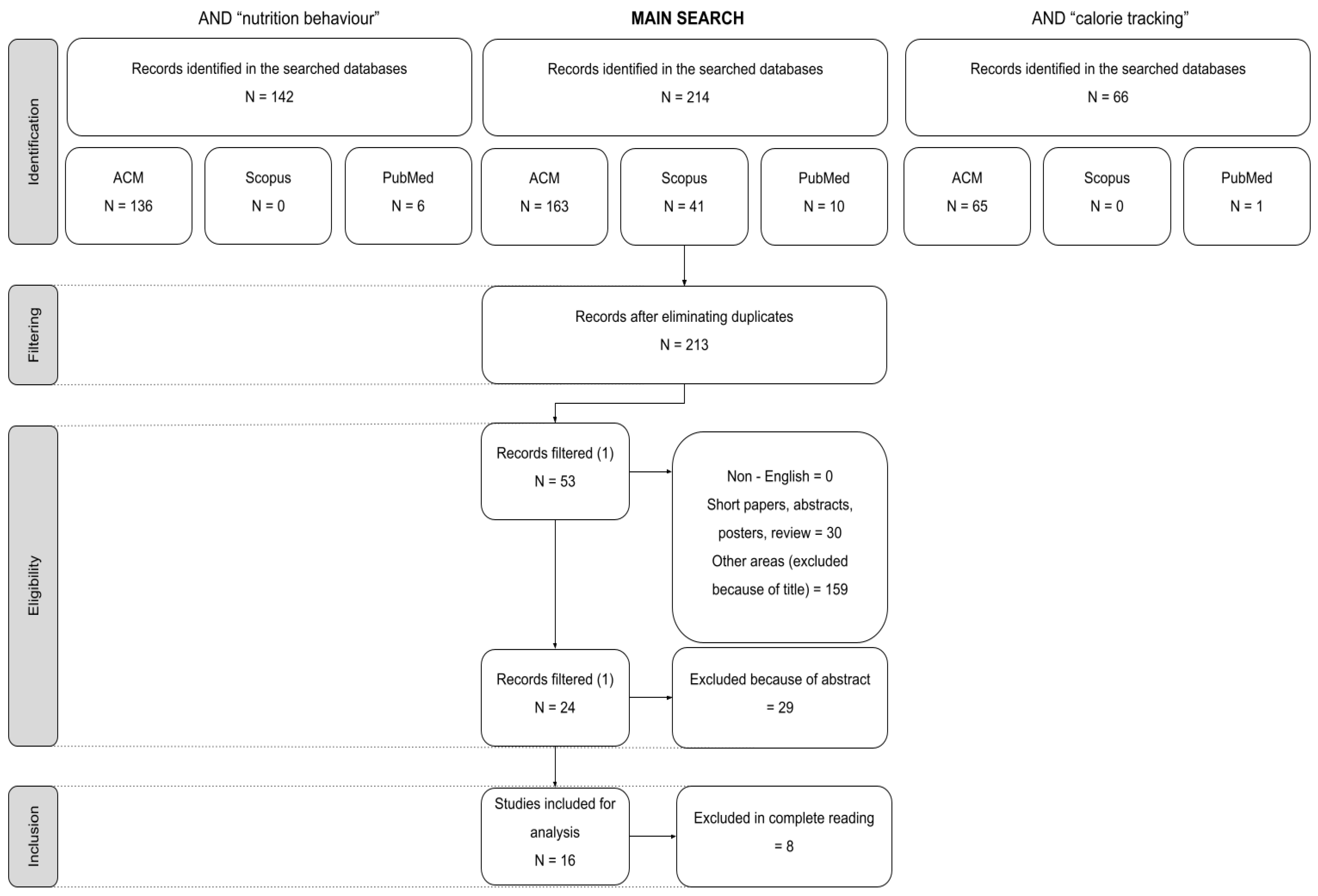
The PRISMA guidelines were followed to filter the different articles from the SRL, which suggests applying four steps: (1) Identification, (2) Filtering, (3) Eligibility, and (4) Inclusion.
Figure 1 represents the PRISMA-based flow chart, which shows all the details about the records that were included and excluded.
In total, 214 records were obtained, and the first filter was applied. The aim of this filter was to eliminate the duplicates; in this case, there was just one text repeated in two of the databases. After this criterion, there were 213 records still available.
Secondly, the second filter was applied excluding all those text that were non-English, short papers, abstracts, posters or reviews. Moreover, by the reading of the titles some of the results have also been discarded, leaving 53 records to analyze in depth.
After the reading of the remaining abstracts, there were another 29 records discarded; this filter left 24 results to read. Finally, after completely reading all the remaining records, just 18 studies were included for analysis.
After this analysis, a review of words related to the study that could offer another point of view to the search was carried out. Among the terms found, a new identification stage was carried out with two of these (nutrition behavior and calorie tracking) and the results of the searches can be seen in
Table 3 and
Table 4.
As a conclusion, we can observe that the search by adding the term nutrition behavior shows that most of the studies stored in ACM are related to nutrition (136). In addition, it can be seen that the Scopus database does not have any results, which shows that it is a more technical database. Finally, PubMed shows only six results (
Table 3).
If we look at the other search, which added the term calorie tracking, it shows similar results, although in the ACM database fewer results are obtained, since they are reduced to slightly more than half (65) (
Table 4).
In the end, we realized that the two complementary searches that were performed were included in the main search carried out in the first place; therefore, taking into account that the search did not obtain many results, we used the main search to analyze the articles.
Certain inclusion and exclusion criteria have been used in the filtering of documents found in the searches, and are defined in
Table 5.
To measure the quality of the analyzed articles, 10 indicators have been defined. The first 7 are related to the content of the article and to publication quality metrics. The M8 metric was used to differentiate those articles that have published in conferences from the journals. We thought it would be interesting to point out the articles that give the possibility to obtain the data used in the research, so that the experiment might be reproduced, which is why M9 was included. Lastly, M10 gives importance to those articles that use diagrams and images to help with the explanation (
Table 6).
The results of the review of the articles will be obtained using the criteria shown in
Table 6.
3. Results
In the analyzed cases, we can see that most of the recommendation systems are designed to recommend different diets; some of them do not recommend whole diets but some specific foods. Rarely do we see systems that offer physical activity recommendations in addition to diet.
On the other hand, most of the analyzed systems have made use of collaborative filtering. However, content-based, hybrid, and knowledge-based filtering have also been used. As for the type of platforms used, in most studies this was not specified, and in those where it was, online platforms were used.
Finally, it should be noted that most studies and platforms have been motivated to help patients with a disease that may improve as a result of maintaining a healthier diet.
Once the comparative table of the studies (
Table 7) had been made, articles 1 to 11 were graded taking into account the criteria defined in
Table 6 so that an overview of the quality of each article could be obtained. For this purpose, three levels of quality have been defined: High (H) the articles with a score between 8 and 11, Medium (M) between 5.1 and 7.9, and Low (L) less than 5. After the qualification, we can affirm that within the metrics used in this study, the articles [
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28,
29,
30,
31] are of high impact.
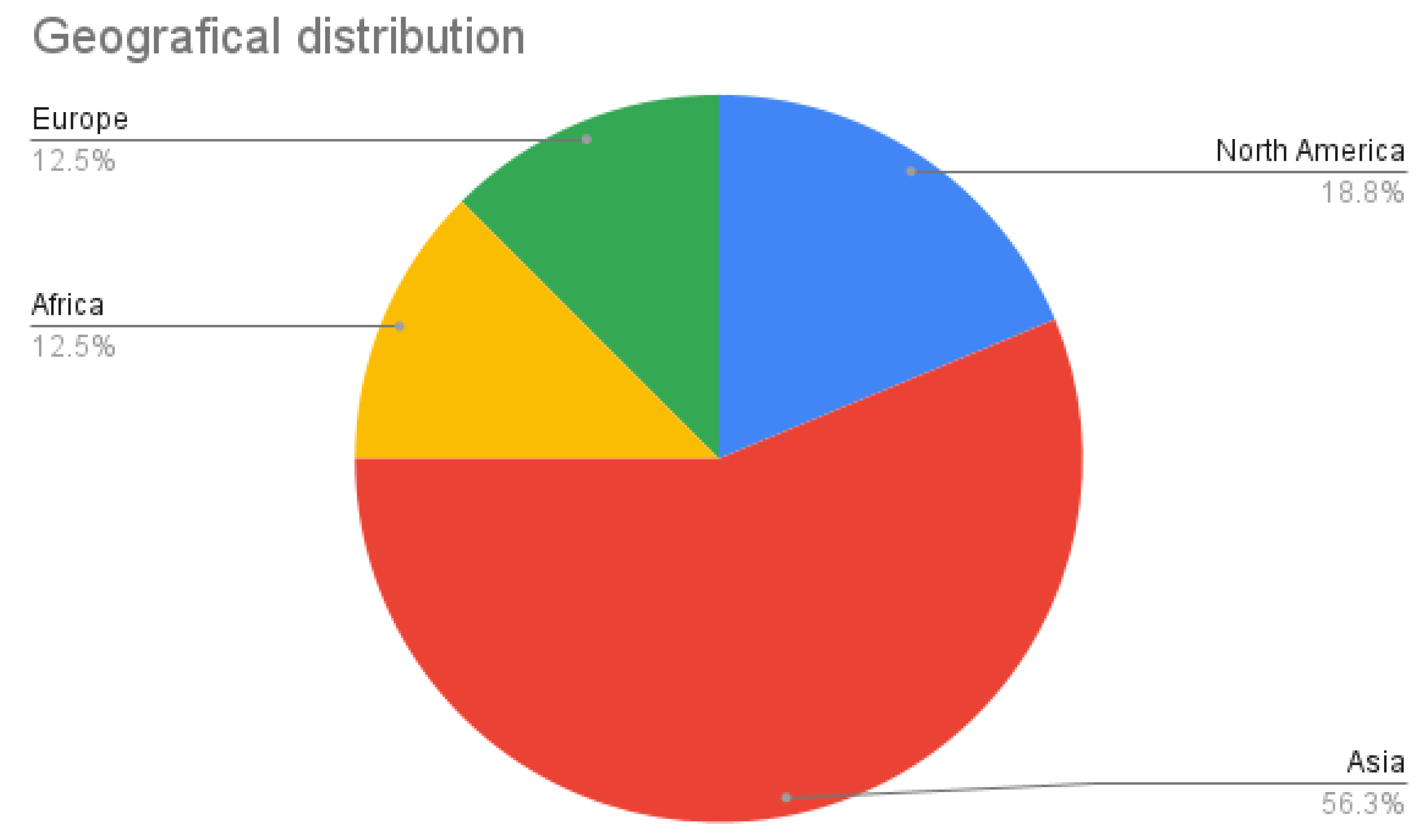
3.1. Geographical Distribution
As for the geographic distribution of the different articles written, it can be seen that the majority of these have been written in Asia (56.3%) and North America (18.8%); the remaining articles come from Europe (12.5%) and Africa (12.5%) (
Figure 2).
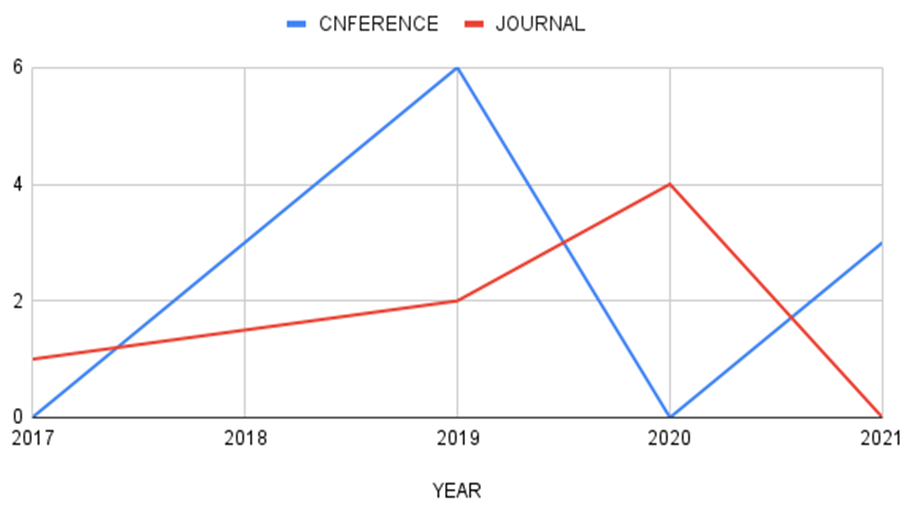
3.2. Journals per Year
In total, nine of the articles have appeared in conferences and the other seven in journals (
Figure 3).
As a conclusion, we can see that an increase in conferences has a direct impact on the publication of articles on the subject; this is due to the time required to publish an article in journals, whereas conferences have shorter publication times.
3.3. Different Recommendation System Used in the Article
In addition, the percentage of the different recommendation systems used in the studies was analyzed (
Table 8).
4. Discussion
Nutrition mobile apps are an emerging field that could act as a cost-effective tool that can instruct different type of populations in improving their nutritional habits. However, there is a high variability in the recommendations. Some tend to focus on diets, others on specific food, and they rarely offer physical activity recommendations. At the same time, differences exist between apps in the nutrition tools and the type of technology used.
Answering question Q4 defined in
Table 1, if we focus on the different filtering methods used by the analyzed systems, we can see a tendency in the use of the collaborative filter. This is not a common result; normally content-based filters are used as starting filtering methods [
32,
33,
34,
35,
36,
37,
38,
39,
40,
41,
42,
43,
44,
45,
46,
47], and once a considerable amount of data from the users are obtained, collaborative filters are launched. This might be because some studies were started with some initial data about the users.
Additionally, the methods used for the caloric and nutrients need are not explained in depth, which is the reason why Q3 could not be answered.
On the one hand, in Q1, which talks about the areas of nutrition used in SR, most of the systems are related to health problems linked to nutrition or that can be improved by certain specific diets, and some studies focus on improving the diet regardless of whether the user suffers from a disease or not.
Finally, question Q2, which is focused on answering whether different recommendations are used for the different systems developed, is linked to Q1, since depending on the target user group, certain recommendations are offered or others.
Almost all the data used by the different research are not available. In some cases (which can be seen in
Table A1), the obtained data have been made available under request. On the other hand, some research cited the data used for the investigation.
For the future, it would be interesting to include both the methods used for the nutrient or caloric needs calculation and the data obtained in the investigation; with this information, given the easiness to reproduce it should considerably improve.
Finally, the population involved in the different articles is different from each other. Depending on the specific subject of the research, the study has chosen people related to the research, either because they are young, patients of certain pathologies, or without considering any other criteria.
Given that the population is highly heterogeneous, confusing data makes it challenging to interpret the available data, because the results change considerably depending on the population analyzed. There are no “one size fits all” diet, requirements and nutritional needs, as they differ in the entire population. It is difficult to analyze the data collected when there is such disparity between the individuals. In fact, collecting people’s caloric intake is in itself complex, since people, regardless of their body weight, tend to underestimate the calories they consume [
48].
At the same time, there is a high variability in diets responses and personalized nutrition programs tend to show better results than standardized approaches [
11]. Although some people tend to lose weight with a specific diet, this does not guarantee that the same method will work for other people. In part, this is explained by adherence and motivation. When people are comfortable with the type of diet they follow, they tend to find better results and respect the nutritional recommendations [
7,
49,
50].
As with diets, users find positive results if they are motivated, since this reinforces their degree of adherence, a key aspect when trying to lose weight. Despite the practicality and usefulness of health mobile apps, users tend to lose adherence and motivation over time. In part this is because each user is different: although some may be motivated by uploading the data to the app, others may need to constantly receive encouraging messages or be helped to modify their behavior [
51].
Measuring caloric intake is quite difficult and calorie reporting often contains errors. Additionally, the caloric report in mobile applications is influenced by the motivational level of the subjects and many of the available studies were carried out in heterogeneous populations. Consequently, analyzing the collected data becomes complex, making it difficult to draw general conclusions for the entire population.
Other limitations observed in the studies is that they do not always precisely define the type of diet, food, preparation methods, or nutrient composition. In fact, these are some of the limitations that health professionals highlight in these types of applications [
14].
We see that nutritional applications are associated with numerous sources of error, both internal (of the app itself) and external (of human behavior). Therefore, it is recommended to be careful when interpreting the data collected.
Although many people can benefit from the use of these types of applications, sometimes it may be linked to eating disorders. It is not clear if eating disorders develop from using these apps or if those who have eating disorders tend to use them. In any case, due to the great variability that exists, it is advisable to take these data with caution and educate people before encouraging their use [
52].
However, our review has limitations. Firstly, we evaluate scientific research where different types of apps were analyzed. Perhaps there is a different degree of effectiveness between them that we could not detect in this review.
Secondly, it is possible that our limited sample size obscured a larger size effect. The size and duration of the different studies were not the same; this may have affected the data collected. Additionally, not all investigations used the same intervention criteria and population. Having different data sources may have biased us in being able to identify the potential impact they really have or if they act differently in any particular population.
Thirdly, perhaps there is a different degree of adherence in the strategies that use technological support compared with traditional diets; therefore, by not considering these data, we could not find significant differences.
Fourth, we may have incurred certain bias when selecting the types of studies, affecting the quality of the data collected. However, after the qualification, we can affirm that within the metrics used in this study, the articles are of high impact.
5. Conclusions
In conclusion, although there is a massive and widespread use of Health Mobile Apps, there are still doubts about their effectiveness in improving nutritional habits, in what type of population they work best, and what type of information usually produces better results. Although these types of apps can be useful due to their growing interest and popularity in the public that wants to eat healthily, more information is still needed.
However, they can become a useful tool for developing personalized nutritional recommendations if AI and ML support is enhanced. By improving the methodology and procedures used in different scientific investigations, could help us to understand more accurately how these technologies can contribute to improve the nutritional health of the population. Although there are certain gaps and problems to be solved, the use of this technology shows encouraging results in promoting health and disease management.
The importance of nutrition during the pandemic caused by COVID-19 is noteworthy. There is clear evidence that the prevention of diseases such as obesity and type 2 diabetes reduces the risk of serious COVID-19 outcomes [
53]. A proper and healthy diet can ensure a robust immune system that can resist any onslaught by the virus; individuals consuming well-balanced diets appear to be safer with better immune systems and lower incidence of chronic diseases and infections [
54]. Apps can help in this task, as users are looking for simple options to help them with their diets, for example, and the importance of these is becoming more and more crucial.
Finally, we believe that it would be also important to consider ethical and legal issues as these applications often store, process, and share personal information. We do not know if there are any regulations so far.






{kind=link}
{kind=link}
{kind=link}


