
An Automatic Approach for Individual HU-Based Characterization of Lungs in COVID-19 Patients



 , ,
, , 
Abstract
:1. Introduction
- To develop an automated, operator-independent quantitative method to identify the different lung regions for COVID-19 patients, based on individually optimized Hounsfield unit (HU) thresholds; the proposed method is based on an intuitive, interpretable phenomenological characterization of lungs, with clear functional meaning;
- To achieve a feasible implementation of the proposed method in such a way as to be potentially usable by other institutions;
- To demonstrate the robustness of the method with respect to inter-scanner variability within a single institute;
- To report inter-patient distribution of the HU-based parameters extracted by our approach over a large single-center population of 166 patients during the first wave of the pandemic.
2. Materials and Methods
2.1. Patient Database
- Lightspeed VCT (64sl), General Electric Medical System(Boston, MA, USA);
- Brilliance (64sl), Philips (Amsterdam, Netherlands);
- Incisive (64sl), Philips (Amsterdam, Netherlands).
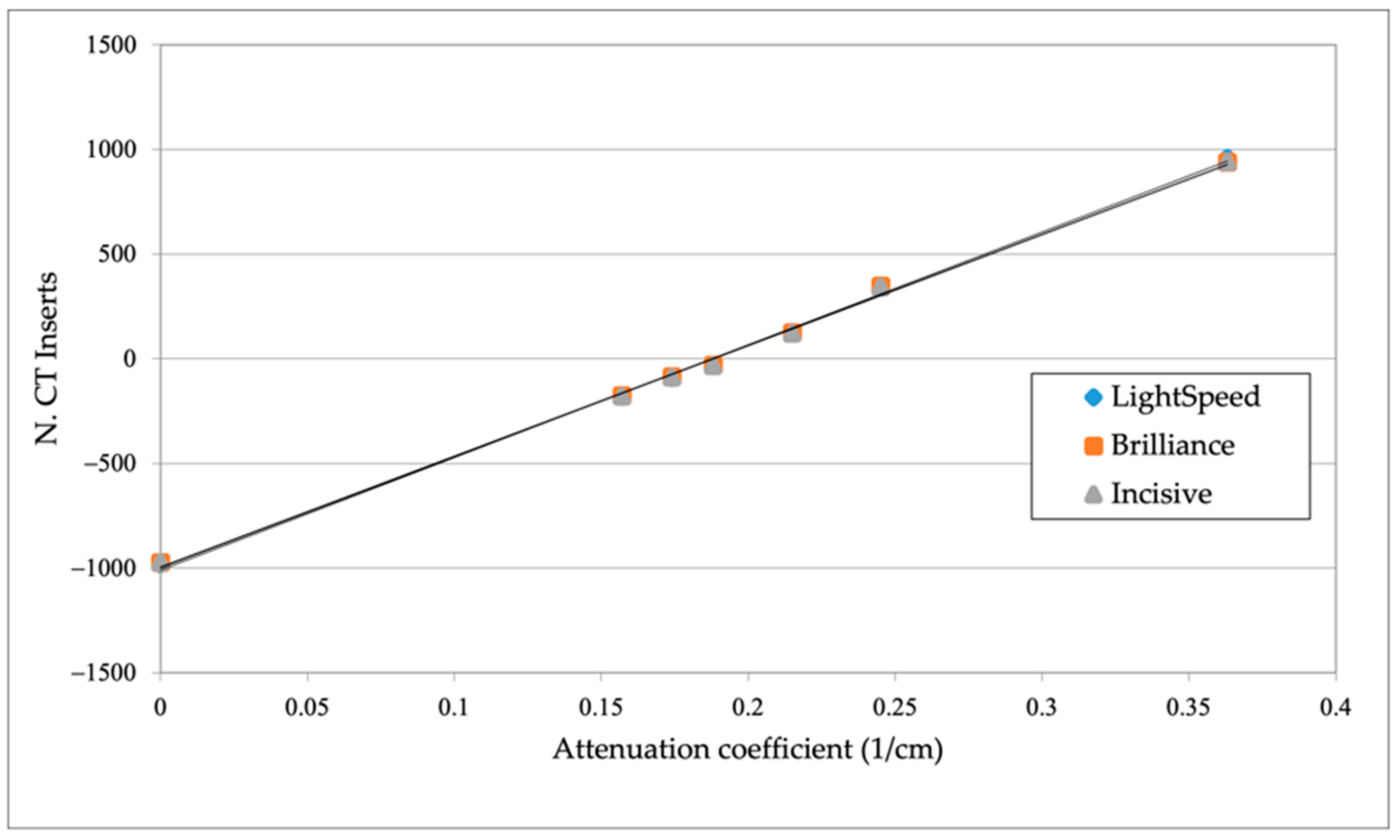
2.2. Assessing Inter-Scanner Variations of HU-Density Calibration Curves
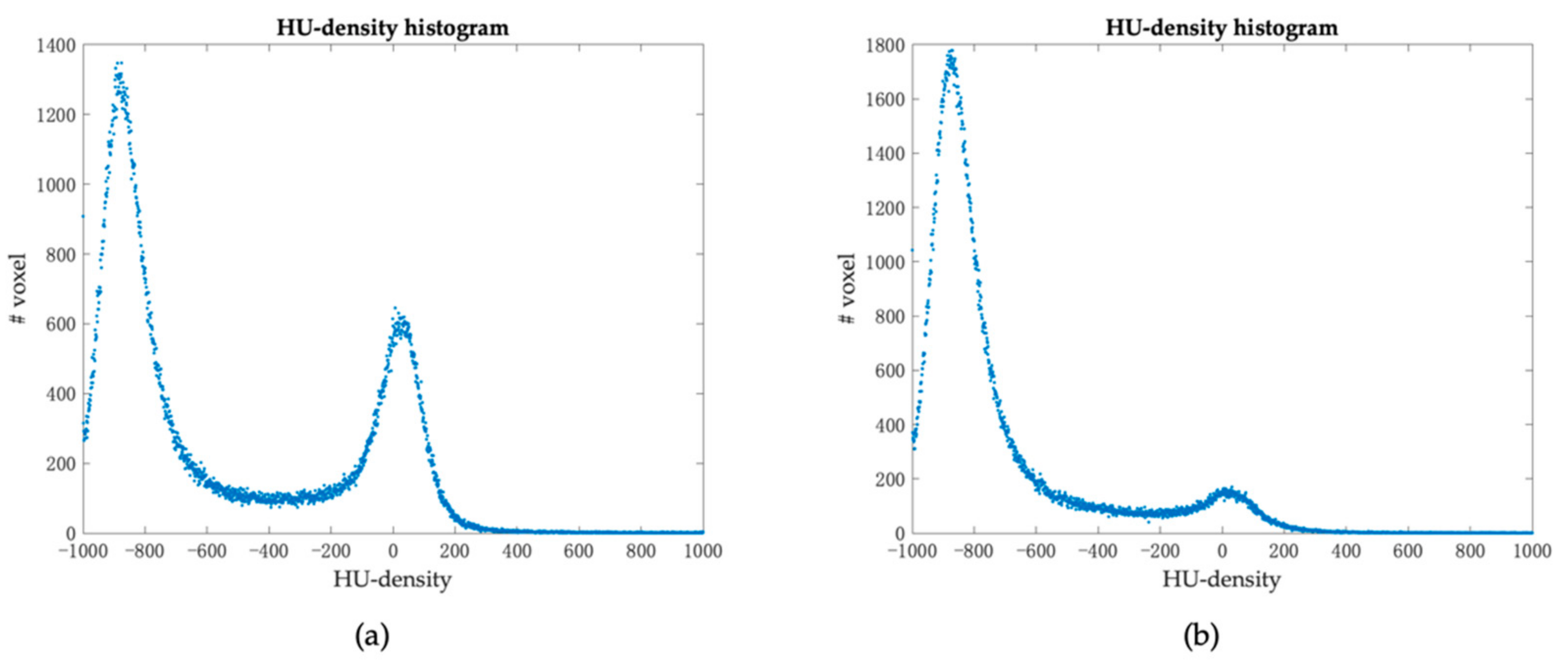
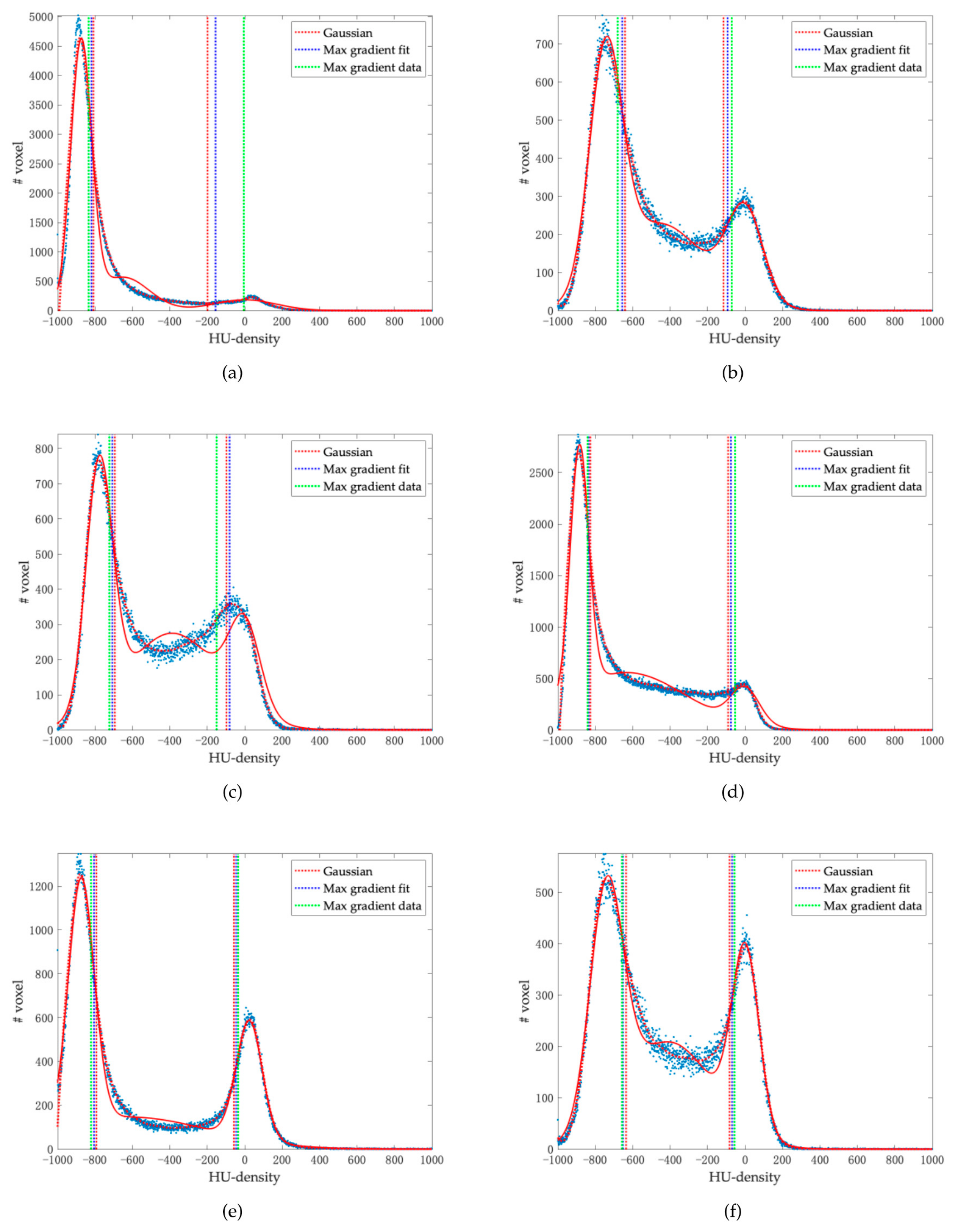
2.3. HU-Density Histograms
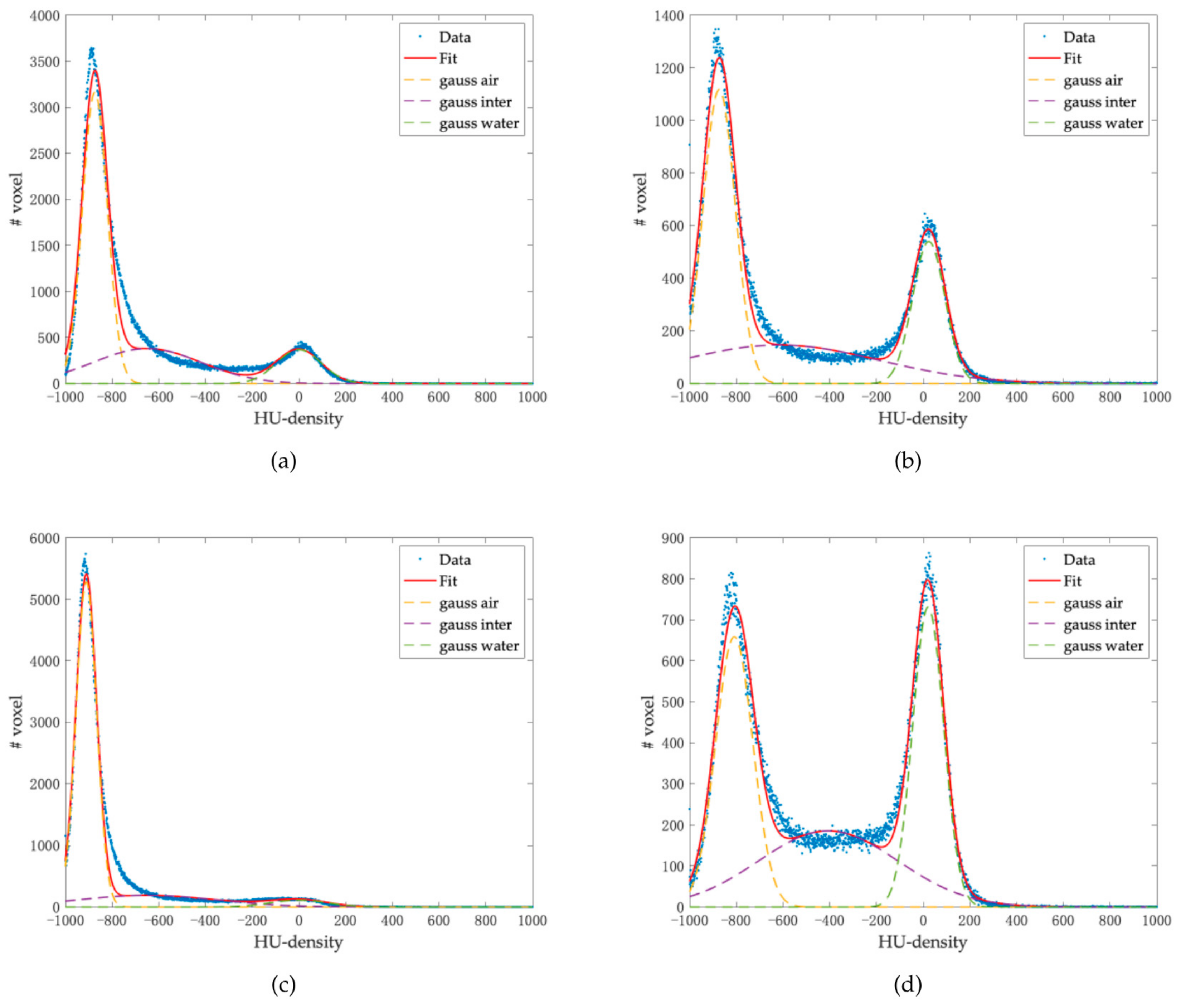
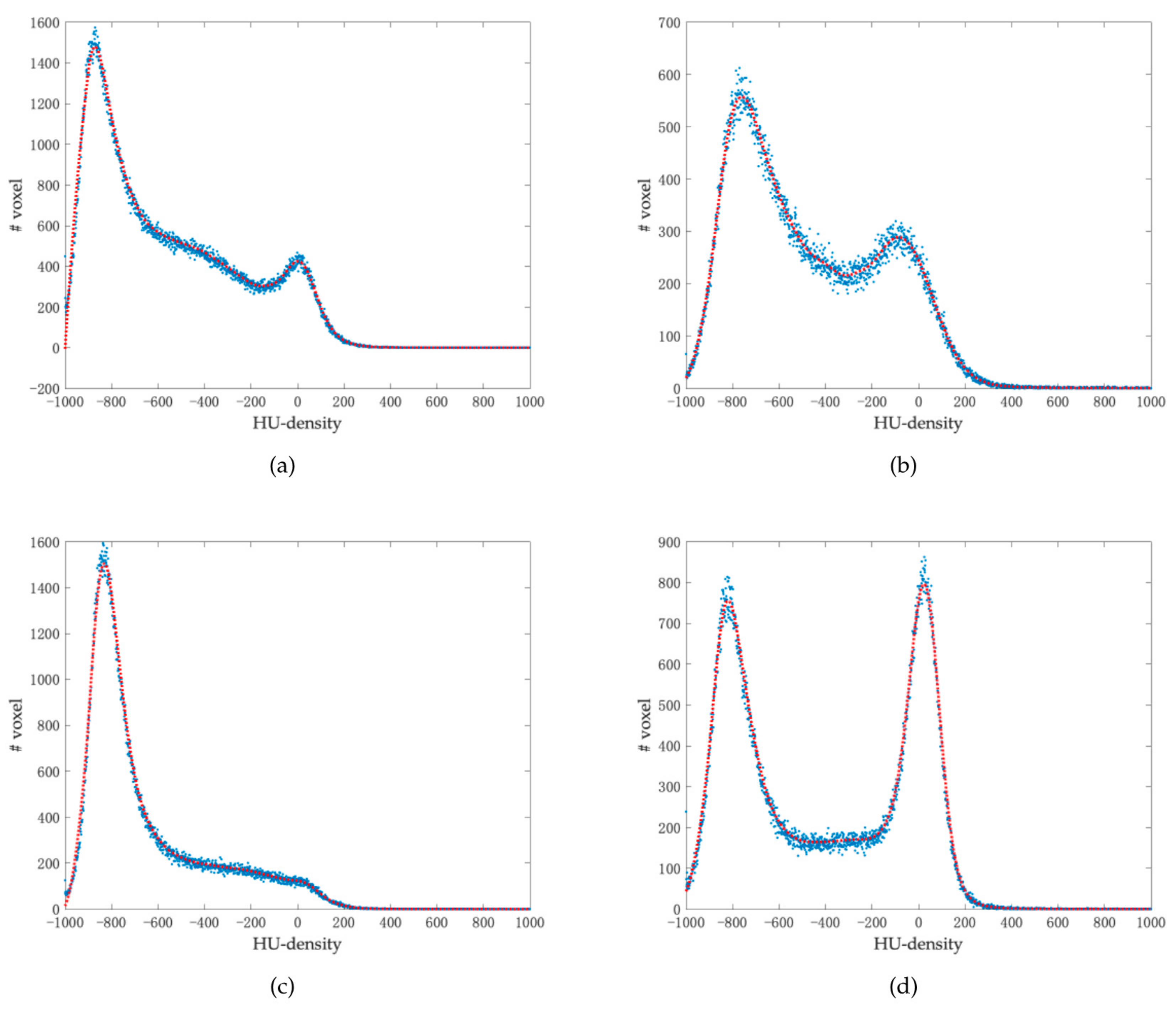
2.4. Threshold Definition Methods
- x are the values of the densities HU;
- a1, a2, and a3 are the multiplicative coefficients of the Gaussians;
- b1, b2, and b3 represent the mean values of the Gaussians;
- c1, c2, and c3 are related to the standard deviation from the relation c2 = 2σ2;
- Subscript 1 refers to the Gaussian related to the aerated component;
- Subscript 2 refers to the Gaussian related to the intermediate component;
- Subscript 3 to the Gaussian related to the consolidated component.
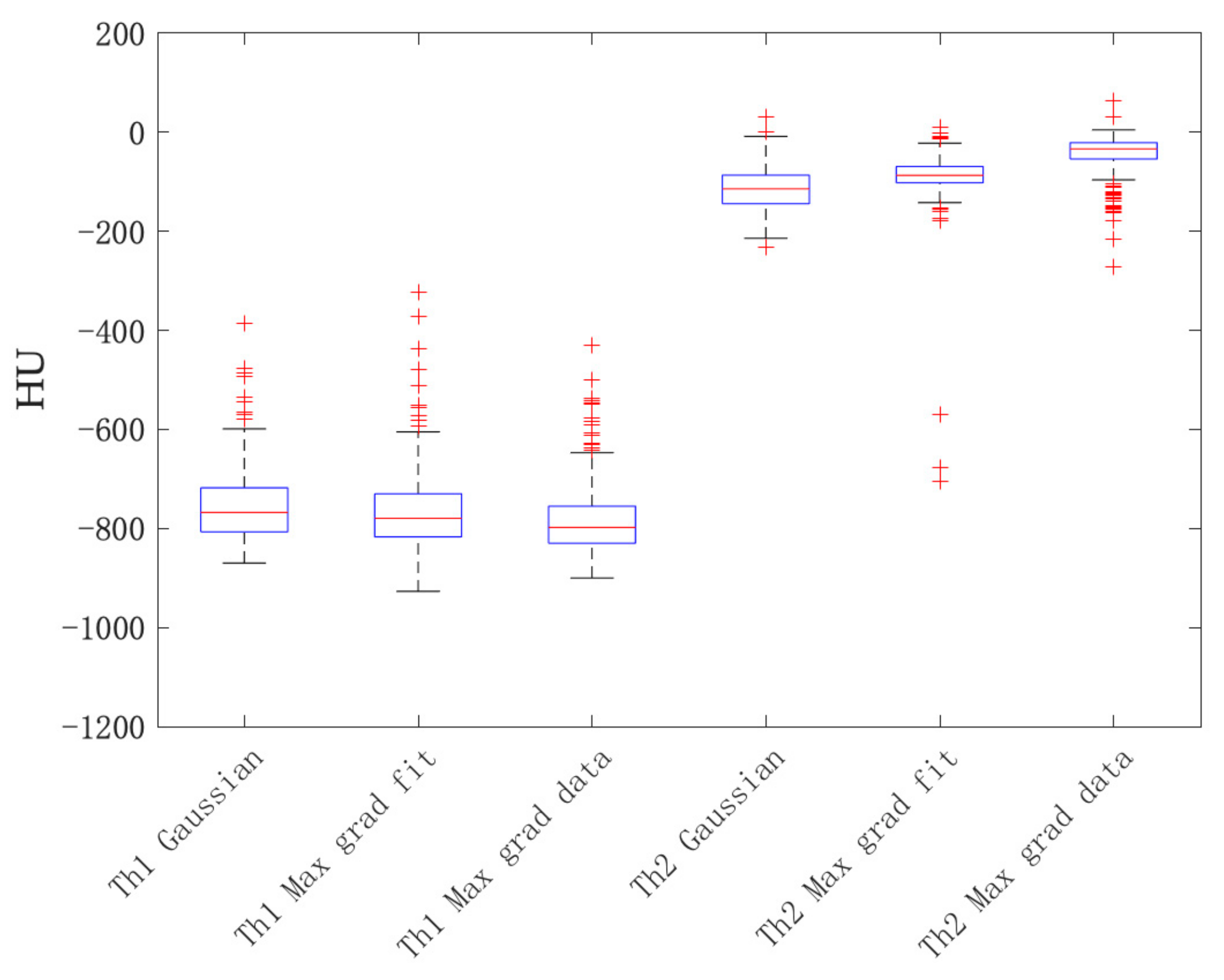
- th1 is the value of HU that separates the aerated component from the intermediate one;
- th2 is the value of HU that separates the intermediate component from the consolidated one;
- b1 and b3 are the mean values of the Gaussians and σ1 and σ3 are the relative standard deviations.
3. Results
3.1. Impact of the HU-Density Calibration Curve
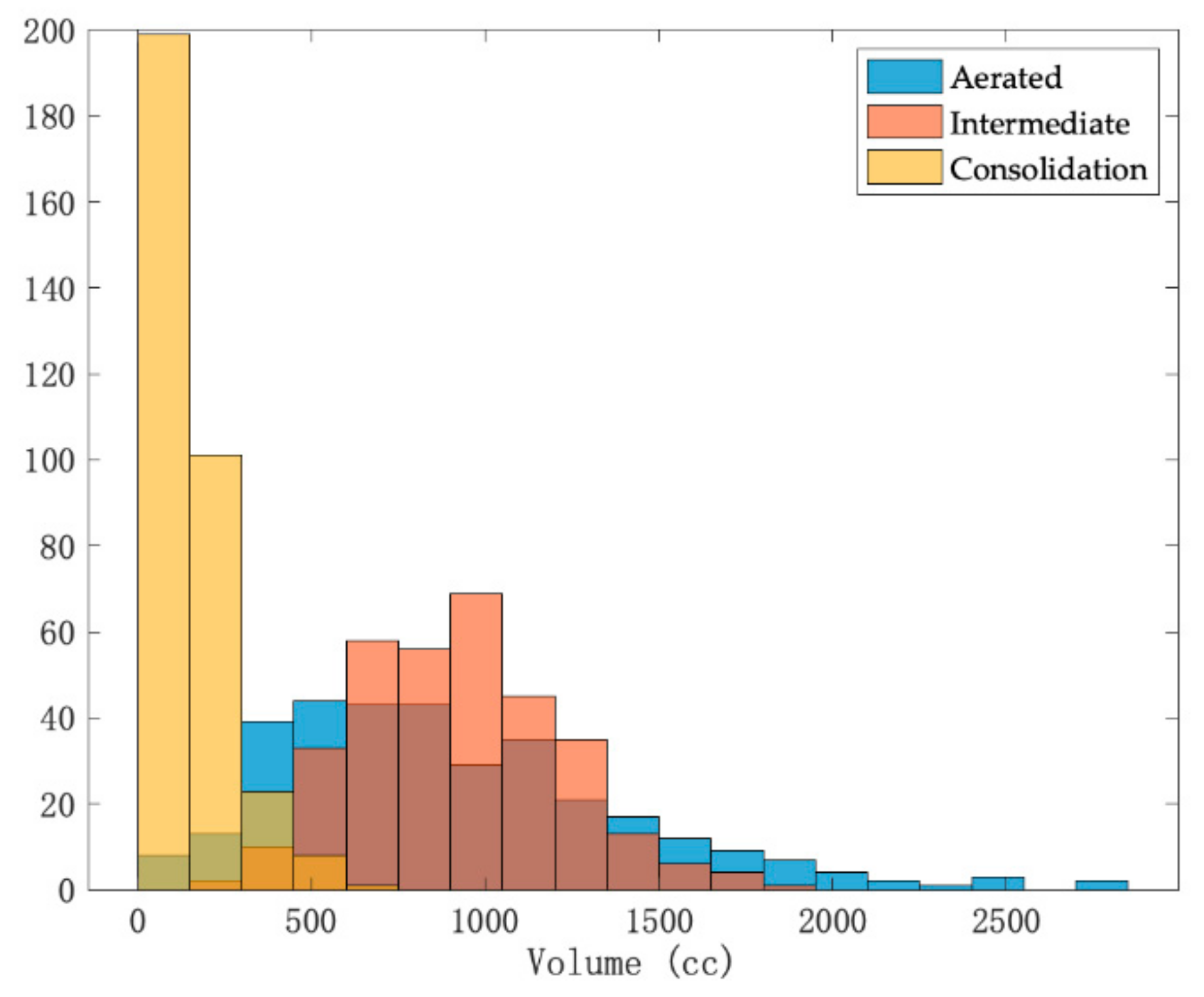
3.2. HU-Density Histogram Parameters—Extraction and Analysis of 166 COVID-19 Patients
- Gaussian;
- Maximum gradient on the fit;
- Maximum gradient on the data.
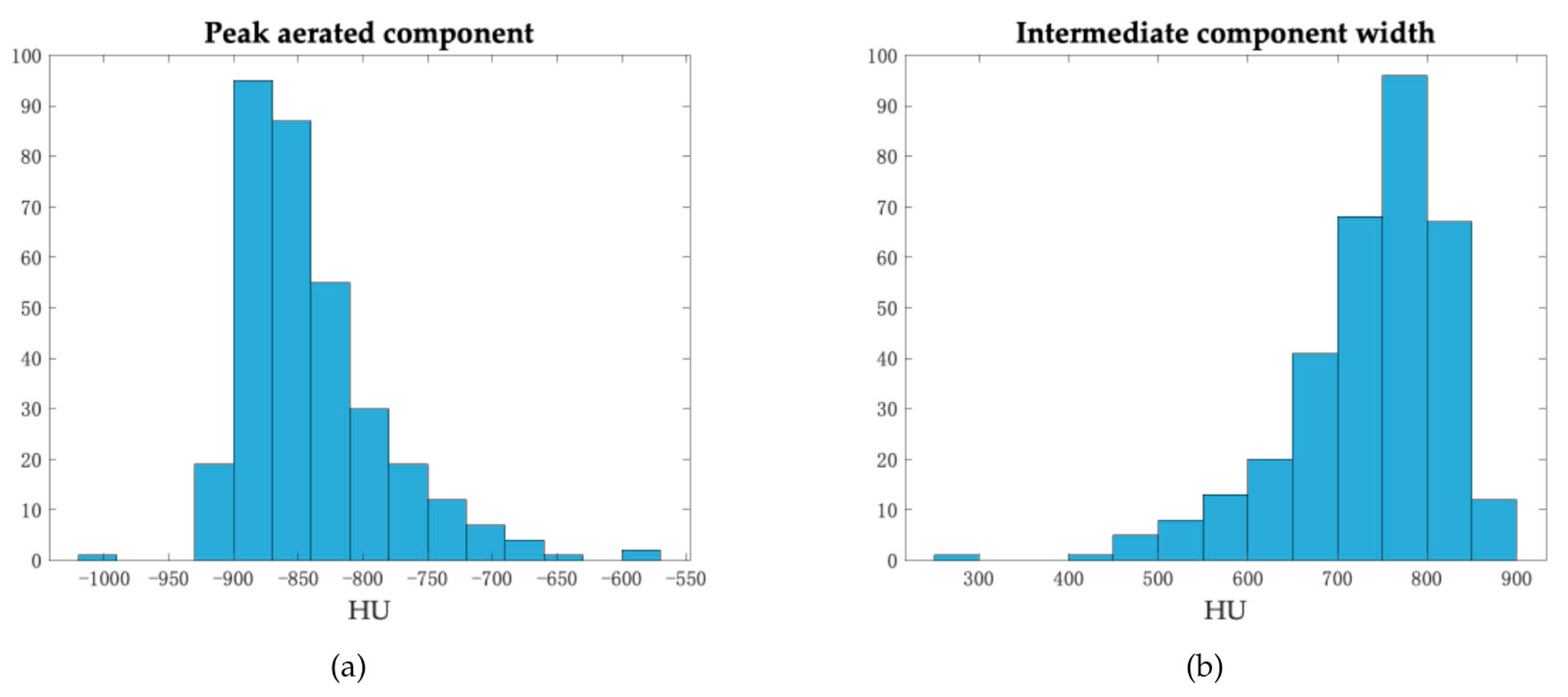
- HU value corresponding to the peak of the curve for the aerated regions;
- Shift with respect to −1000 HU, a characteristic value of the aerated component under normal conditions;
- Width in HU of the intermediate region.
4. Discussion
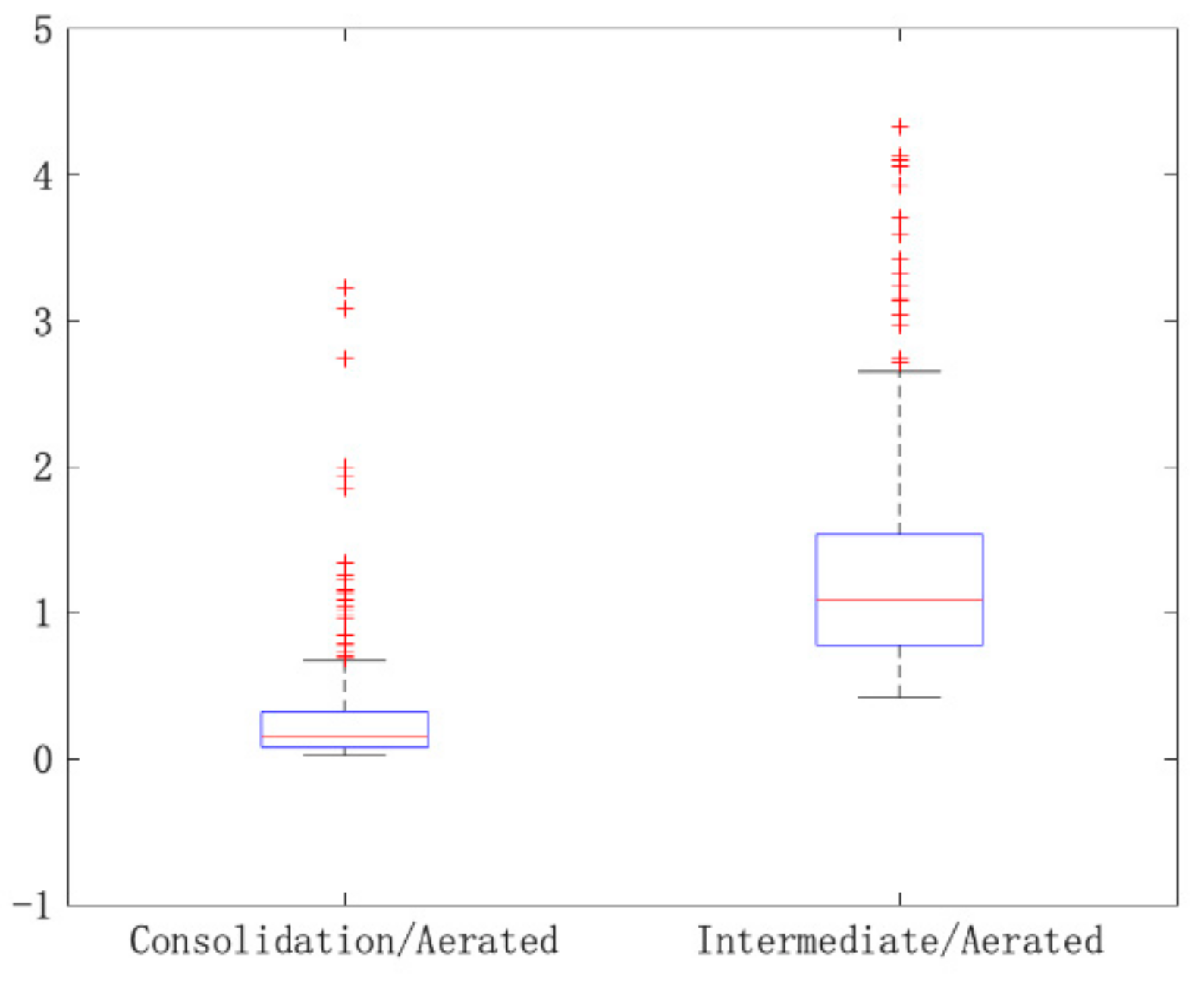
- Ratio between the consolidated component and the aerated component (0.16 ± 0.89);
- Ratio between the intermediate component and the aerated component (1.09 ± 2.56);
- HU value corresponding to the peak of the curve for the aerated regions (−853 ± 56 HU);
- Width in HU of the intermediate region (754 ± 88 HU).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coronavirus Disease (COVID-19) n.d. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 9 November 2020).
- Agricola, E.; Beneduce, A.; Esposito, A.; Ingallina, G.; Palumbo, D.; Palmisano, A.; Ancona, F.; Baldetti, L.; Pagnesi, M.; Melisurgo, G.; et al. Heart and Lung Multimodality Imaging in COVID-19. JACC: Cardiovasc. Imaging 2020, 13, 1792–1808. [Google Scholar] [CrossRef]
- Wen, Z.; Chi, Y.; Zhang, L.; Liu, H.; Du, K.; Li, Z.; Chen, J.; Cheng, L.; Wang, D. Coronavirus Disease 2019: Initial Detection on Chest CT in a Retrospective Multicenter Study of 103 Chinese Patients. Radiol. Cardiothorac. Imaging 2020, 2, e200092. [Google Scholar] [CrossRef] [Green Version]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT findings in coronavirus disease 2019 (COVID-19): Relationship to duration of infection. Radiology 2020, 295, 685–691. [Google Scholar] [CrossRef] [Green Version]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time course of lung changes at chest CT during recovery from coronavirus disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: A multicenter study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 novel coronavirus (2019-NCoV) pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of terms for thoracic imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [Green Version]
- Hamer, O.W.; Salzberger, B.; Gebauer, J.; Stroszczynski, C.; Pfeifer, M. CT morphology of COVID-19: Case report and review of literature. RöFo 2020, 192, 386–392. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated with Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Han, R.; Huang, L.; Jiang, H.; Dong, J.; Peng, H.; Zhang, D. Early Clinical and CT Manifestations of Coronavirus Disease 2019 (COVID-19) Pneumonia. Am. J. Roentgenol. 2020, 215, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA—Secondary Publication. J. Thorac. Imaging 2020, 35, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Zhang, Q.; Huang, C.; Shi, C.; Wang, L.; Shi, N.; Fang, C.; Shan, F.; Mei, X.; Shi, J.; et al. CT quantification of pneumonia lesions in early days predicts progression to severe illness in a cohort of COVID-19 patients. Theranostics 2020, 10, 5613–5622. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, A.; Scipione, R.; Alfieri, G.; Petrillo, R.; Dolciami, M.; Ciccarelli, F.; Perotti, S.; Cartocci, G.; Scala, A.; Imperiale, C.; et al. Role of computed tomography in predicting critical disease in patients with covid-19 pneumonia: A retrospective study using a semiautomatic quantitative method. Eur. J. Radiol. 2020, 130, 109202. [Google Scholar] [CrossRef] [PubMed]
- Matos, J.; Paparo, F.; Mussetto, I.; Bacigalupo, L.; Veneziano, A.; Bernardi, S.P.; Biscaldi, E.; Melani, E.; Antonucci, G.; Cremonesi, P.; et al. Evaluation of novel coronavirus disease (COVID-19) using quantitative lung CT and clinical data: Prediction of short-term outcome. Eur. Radiol. Exp. 2020, 4, 1–10. [Google Scholar] [CrossRef]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 296, E86–E96. [Google Scholar] [CrossRef] [Green Version]
- Sperrin, M.; Grant, S.W.; Peek, N. Prediction models for diagnosis and prognosis in Covid-19. BMJ 2020, 369, m1464. [Google Scholar] [CrossRef] [Green Version]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.J.M.; Dahly, D.L.; Damen, J.A.A.G.; Debray, T.P.; et al. Prediction models for diagnosis and prognosis of covid-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Xiao, A.; Yu, X.; Zhao, Y.; Lu, Y.; Li, X.; Mei, N.; She, D.; Wang, D.; Geng, D.; et al. Development and validation of a prognostic nomogram based on clinical and CT features for adverse outcome prediction in patients with COVID-19. Korean J. Radiol. 2020, 21, 1007–1017. [Google Scholar] [CrossRef]
- Li, Y.; Yang, Z.; Ai, T.; Wu, S.; Xia, L. Association of “initial CT” findings with mortality in older patients with coronavirus disease 2019 (COVID-19). Eur. Radiol. 2020, 30, 6186–6193. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Using Artificial Intelligence to Detect COVID-19 and Community-acquired Pneumonia Based on Pulmonary CT: Evaluation of the Diagnostic Accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.; He, B.; Li, L.; Dong, D.; Yang, X.; Li, C.; Meng, L.; Zhong, L.; Li, H.; Li, H.; et al. CT radiomics can help screen the Coronavirus disease 2019 (COVID-19): A preliminary study. Sci. China Inf. Sci. 2020, 63, 1–8. [Google Scholar] [CrossRef]
- Harmon, S.A.; Sanford, T.H.; Xu, S.; Turkbey, E.B.; Roth, H.; Xu, Z.; Yang, D.; Myronenko, A.; Anderson, V.; Amalou, A.; et al. Artificial intelligence for the detection of COVID-19 pneumonia on chest CT using multinational datasets. Nat. Commun. 2020, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Long, J.B.; Ehrenfeld, J.M. The Role of Augmented Intelligence (AI) in Detecting and Preventing the Spread of Novel Coronavirus. J. Med Syst. 2020, 44, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lessmann, N.; Sánchez, C.I.; Beenen, L.; Boulogne, L.H.; Brink, M.; Calli, E.; Charbonnier, J.-P.; Dofferhoff, T.; Van Everdingen, W.M.; Gerke, P.K.; et al. Automated Assessment of COVID-19 Reporting and Data System and Chest CT Severity Scores in Patients Suspected of Having COVID-19 Using Artificial Intelligence. Radiology 2021, 298, E18–E28. [Google Scholar] [CrossRef] [PubMed]
- Lyu, P.; Liu, X.; Zhang, R.; Shi, L.; Gao, J. The performance of chest CT in evaluating the clinical severity of COVID-19 pneumonia. Investig. Radiol. 2020, 55, 412–421. [Google Scholar] [CrossRef]
- Kramme, R.; Hoffmann, K.-P.; Pozos, R. Springer Handbook of Medical Technology; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- MIM Maestro®, 6.9; MIM Software Inc: Cleveland, OH, USA, 2019.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Equipment | Number of Patients | Voltage (kV) | Current (mA) | |||
|---|---|---|---|---|---|---|
| Range | Median | 1st Quartile | 3rd Quartile | |||
| Lightspeed | 146 | 120 | 149–549 | 352.5 | 219.5 | 451.5 |
| Brilliance | 12 | 120 | 240–500 | 458.5 | - | - |
| Incisive | 8 | 120 | 189–368 | 334 | - | - |
| Insert | Attenuation Coefficient @70 keV (1/cm) | Light Speed | Brilliance | Incisive | |||
|---|---|---|---|---|---|---|---|
| N. CT ROI | SD | N. CT ROI | SD | N. CT ROI | SD | ||
| Air | 0 | −981.23 | 38.35 | −972.12 | 42.43 | −972.57 | 49.64 |
| PMP | 0.157 | −181.55 | 48.03 | −175.48 | 54.13 | −181.07 | 66.68 |
| LDPE | 0.174 | −90.60 | 46.14 | −85.43 | 53.53 | −90.17 | 67.73 |
| Polystyrene | 0.188 | −35.30 | 46.56 | −30.19 | 52.44 | −34.59 | 69.33 |
| Acrylic | 0.215 | 126.99 | 47.75 | 125.71 | 57.40 | 121.08 | 66.92 |
| Delrin | 0.245 | 350.22 | 52.85 | 347.33 | 56.96 | 341.85 | 70.77 |
| Teflon | 0.363 | 960.24 | 68.70 | 940.18 | 59.92 | 940.09 | 74.29 |
| Method | Threshold | Minimun | Maximum | Median | Standard Deviation |
|---|---|---|---|---|---|
| Gaussian | Th1 | −870 | −386 | −768 | 73 |
| Th2 | −232 | 32 | −114 | 41 | |
| Maximum gradient fit | Th1 | −927 | −322 | −780 | 77 |
| Th2 | −706 | 10 | −87 | 61 | |
| Maximum gradient data | Th1 | −900 | −430 | −798 | 71 |
| Th2 | −271 | 64 | −34 | 41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzilli, A.; Fiorino, C.; Loria, A.; Mori, M.; Esposito, P.G.; Palumbo, D.; de Cobelli, F.; del Vecchio, A. An Automatic Approach for Individual HU-Based Characterization of Lungs in COVID-19 Patients. Appl. Sci. 2021, 11, 1238. https://doi.org/10.3390/app11031238
Mazzilli A, Fiorino C, Loria A, Mori M, Esposito PG, Palumbo D, de Cobelli F, del Vecchio A. An Automatic Approach for Individual HU-Based Characterization of Lungs in COVID-19 Patients. Applied Sciences. 2021; 11(3):1238. https://doi.org/10.3390/app11031238
Chicago/Turabian StyleMazzilli, Aldo, Claudio Fiorino, Alessandro Loria, Martina Mori, Pier Giorgio Esposito, Diego Palumbo, Francesco de Cobelli, and Antonella del Vecchio. 2021. "An Automatic Approach for Individual HU-Based Characterization of Lungs in COVID-19 Patients" Applied Sciences 11, no. 3: 1238. https://doi.org/10.3390/app11031238
APA StyleMazzilli, A., Fiorino, C., Loria, A., Mori, M., Esposito, P. G., Palumbo, D., de Cobelli, F., & del Vecchio, A. (2021). An Automatic Approach for Individual HU-Based Characterization of Lungs in COVID-19 Patients. Applied Sciences, 11(3), 1238. https://doi.org/10.3390/app11031238