1. Introduction
Over a billion people live with some form of disability, which represents 15% of the world’s population [
1]. Between 110–190 million adults have very significant difficulties in functioning. Rate of disability is increasing. According to [
2], approximately 2% of road accidents in Spain result in moderate, serious or total disability. The authors of [
2] point out that the acquisition of a disability is associated with a reduced ability to work, greater functional dependence, greater need for assistance, and the need for family support.
Technological and medical developments make it possible to extend and improve quality of life. A great deal of attention has been paid in recent years to activating older people and people with disabilities (DP—disabled persons). Researchers from all over the world carry out research related to different aspects of DPs’ lives, looking, for example, at how they spend their leisure time [
3], how well the infrastructure fits their needs [
4,
5,
6], or their preferences when making choices [
7]. These people in many cases possess valuable skills. Understanding the specific requirements of this social group allows the development of technical solutions that remove barriers that prevent them from active functioning, socially and professionally. This will enable the public to benefit from these skills.
Among the many factors influencing the professional and social activation of people with disabilities, aspects related to the mobility of DPs and the adaptation of existing systems of transportation to the needs of older and disabled people are often mentioned [
5,
8]. While in large cities, DPs can count on public transport adapted to their needs, in smaller towns and villages DPs are practically dependent on having individual means of transport or on third parties to provide them. One possible solution of this problem is the individual adaptation of a car to the needs of the particular person with disabilities [
9]. However, it should be considered to ensure that any structural changes made do not result in reduced road safety, other people, and disabled driver.
Among many causes of road accidents, the human factor is indicated as one of the main ones [
10]. It is difficult to eliminate all the imperfections and limitations of the physical driver, but thanks to technological developments, the driver has more and more systems to support his actions. Among these are constantly developed active safety systems. Their use, combined with appropriate training of drivers to operate them, can significantly reduce the number of road accidents [
11,
12].
New solutions for use in the automotive industry must be tested in accordance with product standards. The most extensive testing applies to new vehicles, as each must pass very stringent tests before it can be put into road traffic. Of course, cars on the market have varying levels of safety (depending, among other things, on the number of active driver assistance systems), but any new car that does not meet the minimum requirements cannot be put on the road. Another point worth noting is that new cars are designed with the average consumer in mind, and tests are carried out for the chosen body configuration and weight of the occupants. Therefore, modification of the vehicle by changing the steering equipment or adjusting the car for a person with a physique significantly different from the one assumed during design, requires additional tests [
13].
There are now very many methods in use for analysing dangerous situations that may occur on the road. Experimental research is undoubtedly the most important of these. Their disadvantage is the very high unit cost of each test and restrictions on carrying out certain measurements. Therefore, a very popular method of verifying the operation of technical objects is the numerical analysis [
14,
15,
16,
17,
18]. Testing in virtual space allows for evaluating the structure in a short period of time in order to check the compliance with many standards [
19,
20], and for predicting the structure’s behaviour in different load scenarios. The lack of the need to physically build new prototypes and prepare experimental research also allows for significant financial savings. An additional advantage of computer simulations is the possibility to record more data than in the case of experimental studies [
21].
Many different numerical tools are currently available for analyzing dangerous traffic situations [
22]. One of the fastest are calculations using analytical formulae that take into account, among other things, the velocity, weight and stiffness of vehicles [
23,
24,
25]. They allow many scenarios to be analyzed in a very short time and, when supplemented with a reliable vehicle database, make it possible to assess a real accident. An additional advantage of analytical methods is the possibility of transferring the loads acting on the driver to 3D models and further local analysis of his behavior.
Another fast and accurate method based on Reduced Order Dynamic Model [
26], in which discretization of vehicle’s perimeter takes place only in a 2D environment. It reduces the number of equation and thus reduce time calculation.
Analytical and 2D models do not allow an accurate analysis of driver behavior. Therefore, if the aim of the study is to determine e.g., injuries to the driver, methods based on multibody analyzes [
19] or FEM are used [
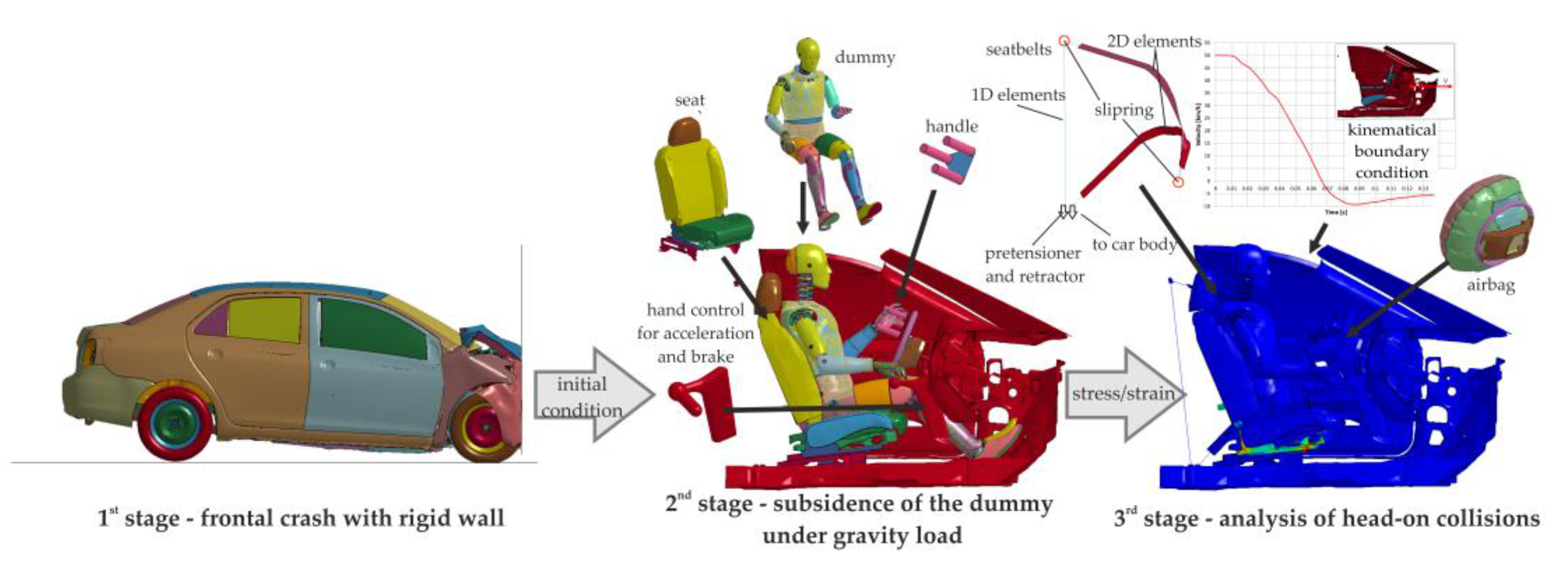
27]. The big disadvantage of these methods is the long calculation time. To reduce it, it is possible to use different strategies. One of them is an approach in which a global collision is analyzed using analytical or 2D models and the results are transferred to 3D models and further analysis of only a selected area. A second solution is to use multi-stage analyses, in which selected aspects of a hazardous road event are investigated independently.
3. Results
The results for the first and second stage, which covers the frontal impact of the whole car and subsidence, are presented in [
28]. This study will only present the results for stage three.
During all analysed cases, characteristic time moments presented in
Figure 6 can be distinguished. The subsidence stage ended at time t = 0.3 s and this is also the beginning of the analysis of the third stage. After approx. 10 ms, the airbag and belt pretensioner were activated. At t = 0.316 s the initial airbag opening is visible. After 36.0 ms, the airbag is close to full inflation, which pushes the upper limbs out of the steering wheel or handles. After 56.0 ms, the dummy’s head encounters the airbag. At t = 0.380 s, the head reaches the maximum forward tilt, followed by the driver’s rebound and a rearward movement to the seat. The contact between the driver’s head and the airbag lasts until the time t = 0.400 s. At a time of approx. t = 0.432 s, the dummy hits the seat’s backrest. This impact is asymmetrical to the seat.
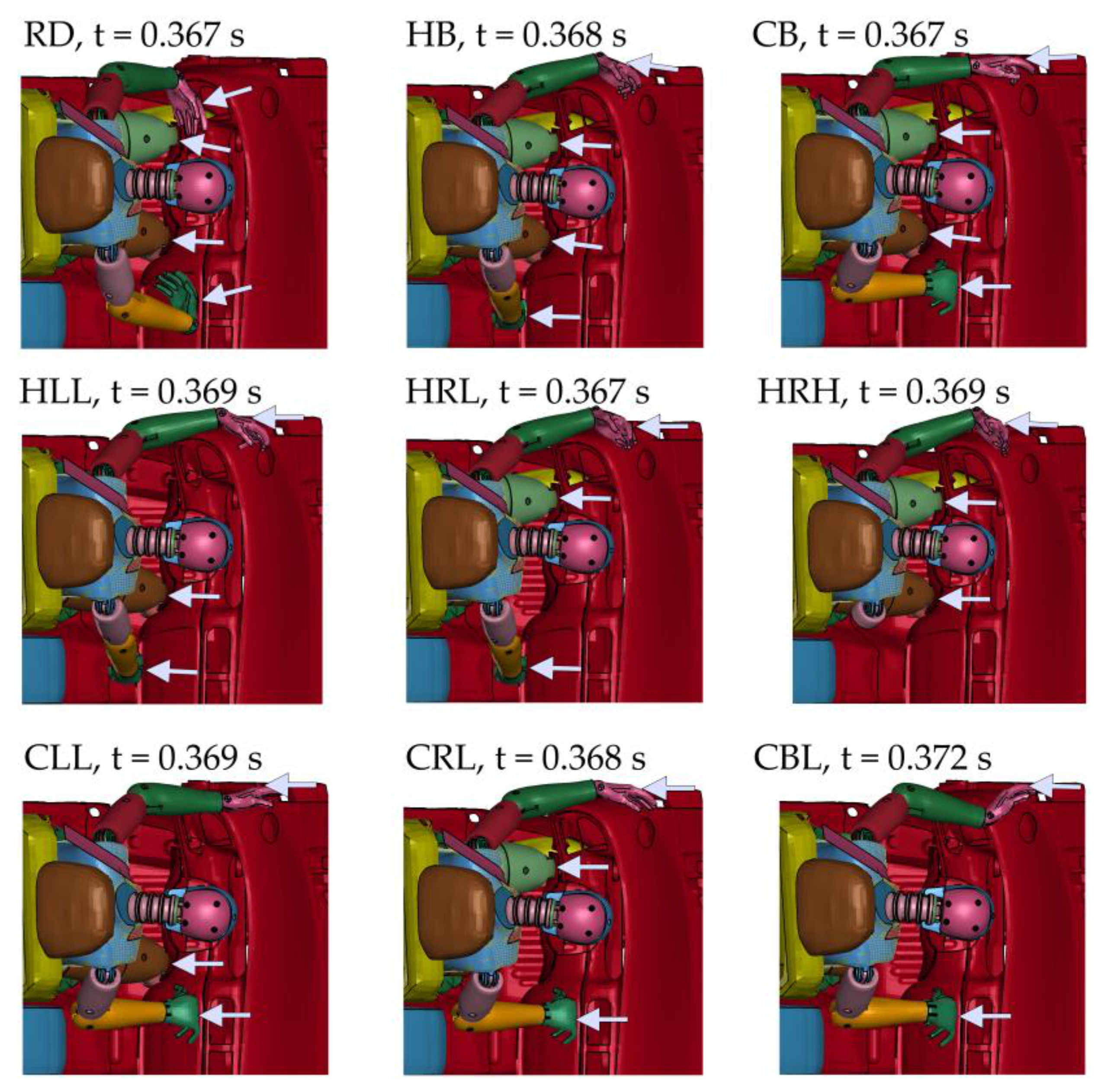
The maximum longitudinal displacement of the conventional centre of gravity of the dummy (i.e., corresponding to the centre of mass without amputation) is achieved at different times in each case (
Figure 7). It is worth noting that at this moment, depending on the equipment used, the position of the dummy differs. In the RD case, the forearms and arms are pushed outwards while keeping the hands within the steering wheel. Knees hit the elements of the space under the steering wheel. In cases H, the left hand is pushed completely out of the steering wheel and the right hand hits the lower part of the central console. In cases C, the right hand strikes higher and in a different position. In cases H and C, the number of zones of contact between the dummy and the vehicle interior depends on the disability under consideration.
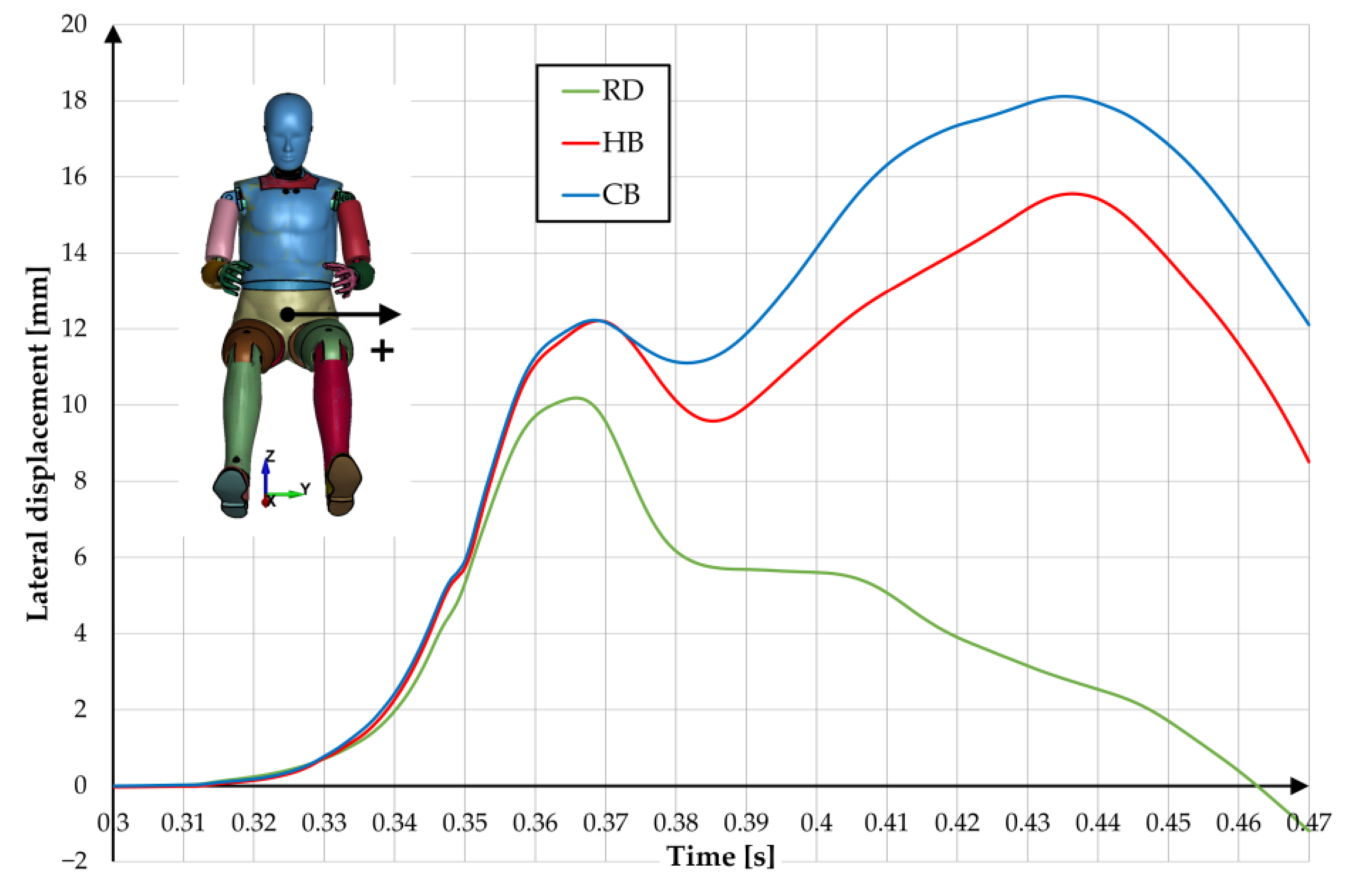
The type of equipment used significantly affects the lateral displacements of the driver’s conventional centre of gravity. In the RD case, the maximum displacement was about 10 mm and, importantly, in the final stage of impact the pelvis almost returned to its initial position (
Figure 8). In the HB and CB cases, there is no return to the initial position and much greater maximum lateral displacement when the dummy hits the seat (approx. 15.5 mm and 18.0 mm respectively).
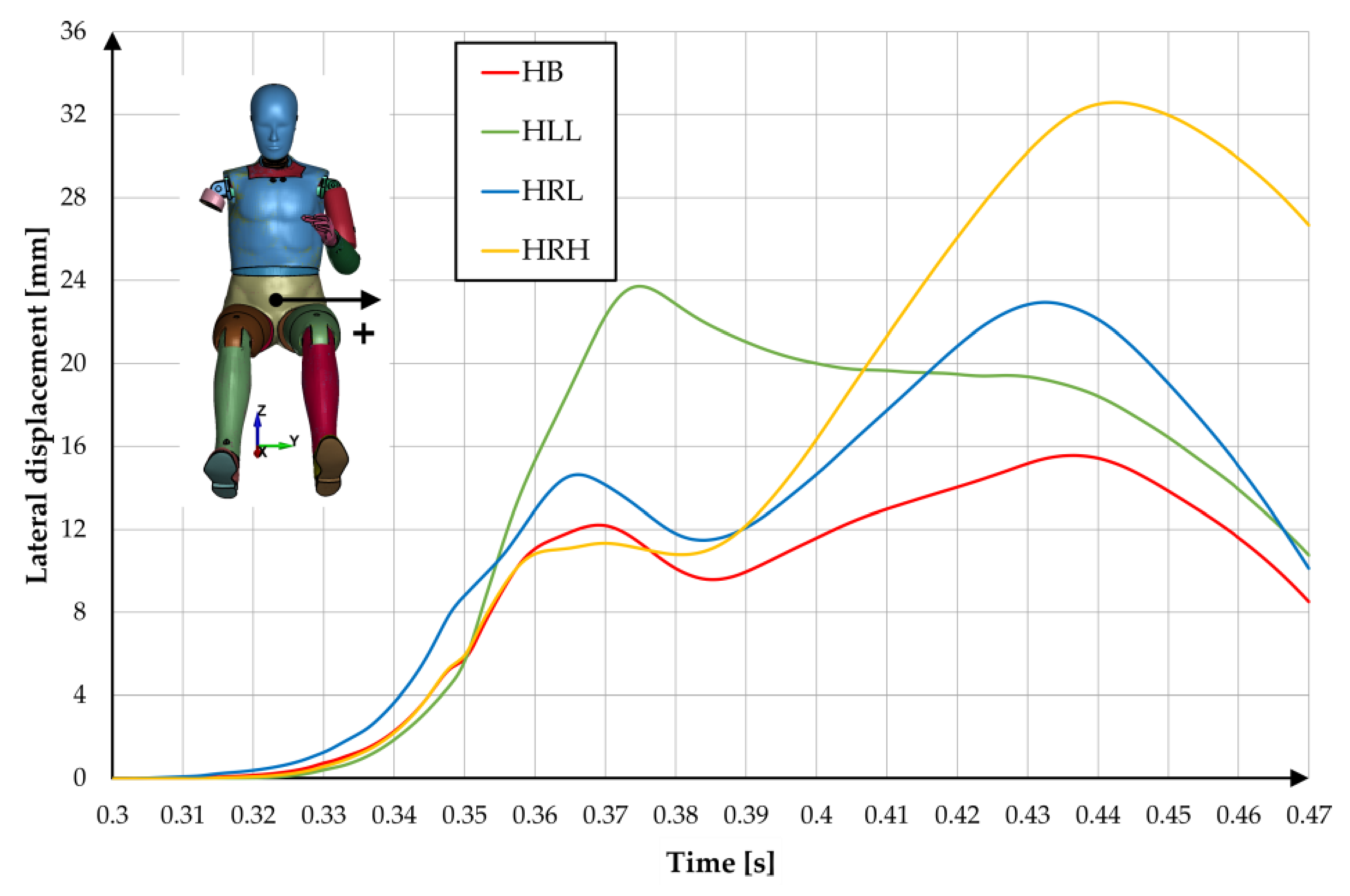
Analysing the H group, it can be seen that at the moment of the maximum longitudinal displacement of the dummy’s centre of gravity in relation to the seat, the maximum lateral displacement occurs for HLL (
Figure 9). In turn, when the dummy hits the seat’s backrest, the maximum lateral displacement is for HRH (about 29 mm).
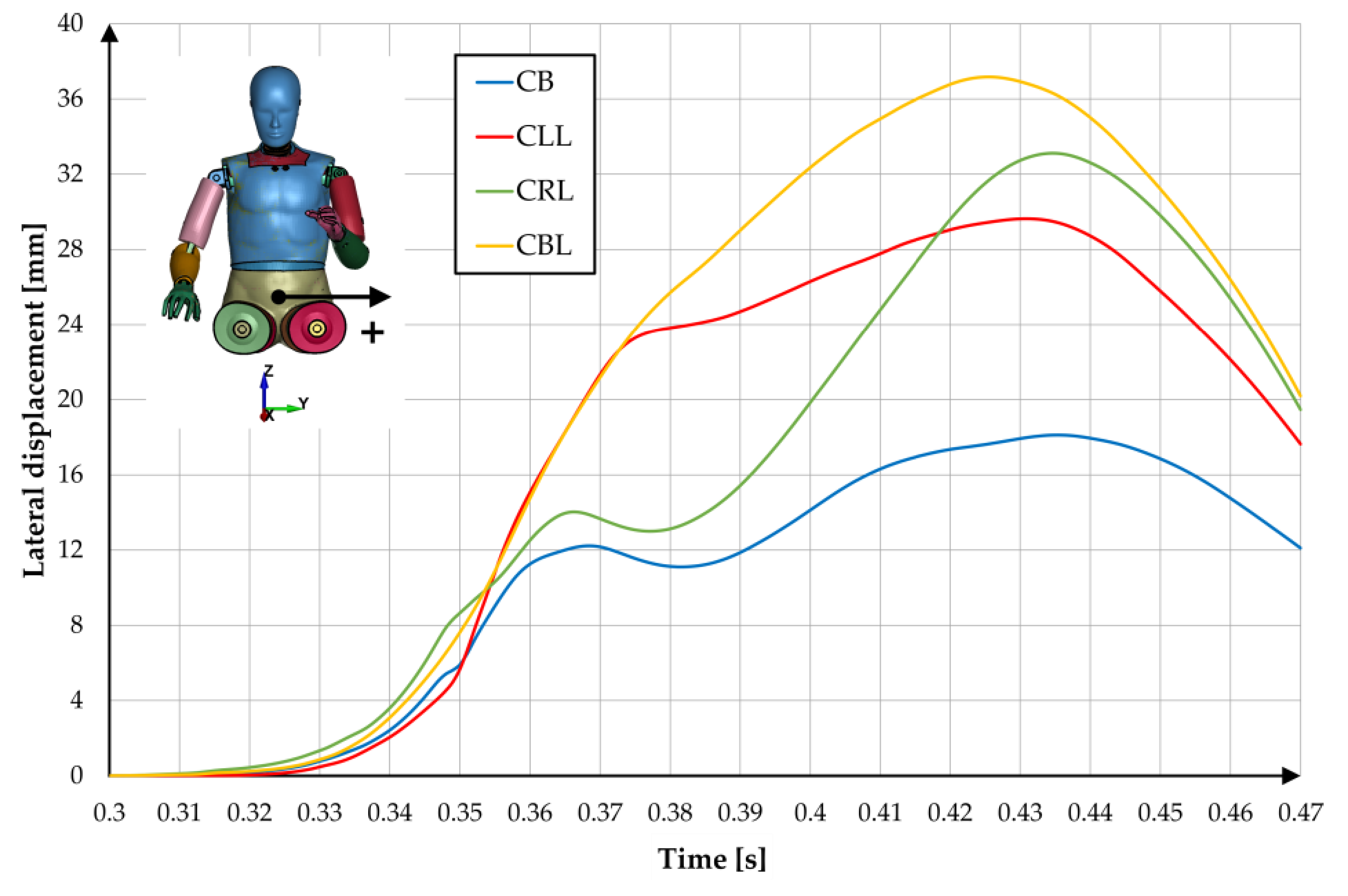
In group C the greatest lateral displacement can be observed for CLL, CRL and CBL cases (
Figure 10).
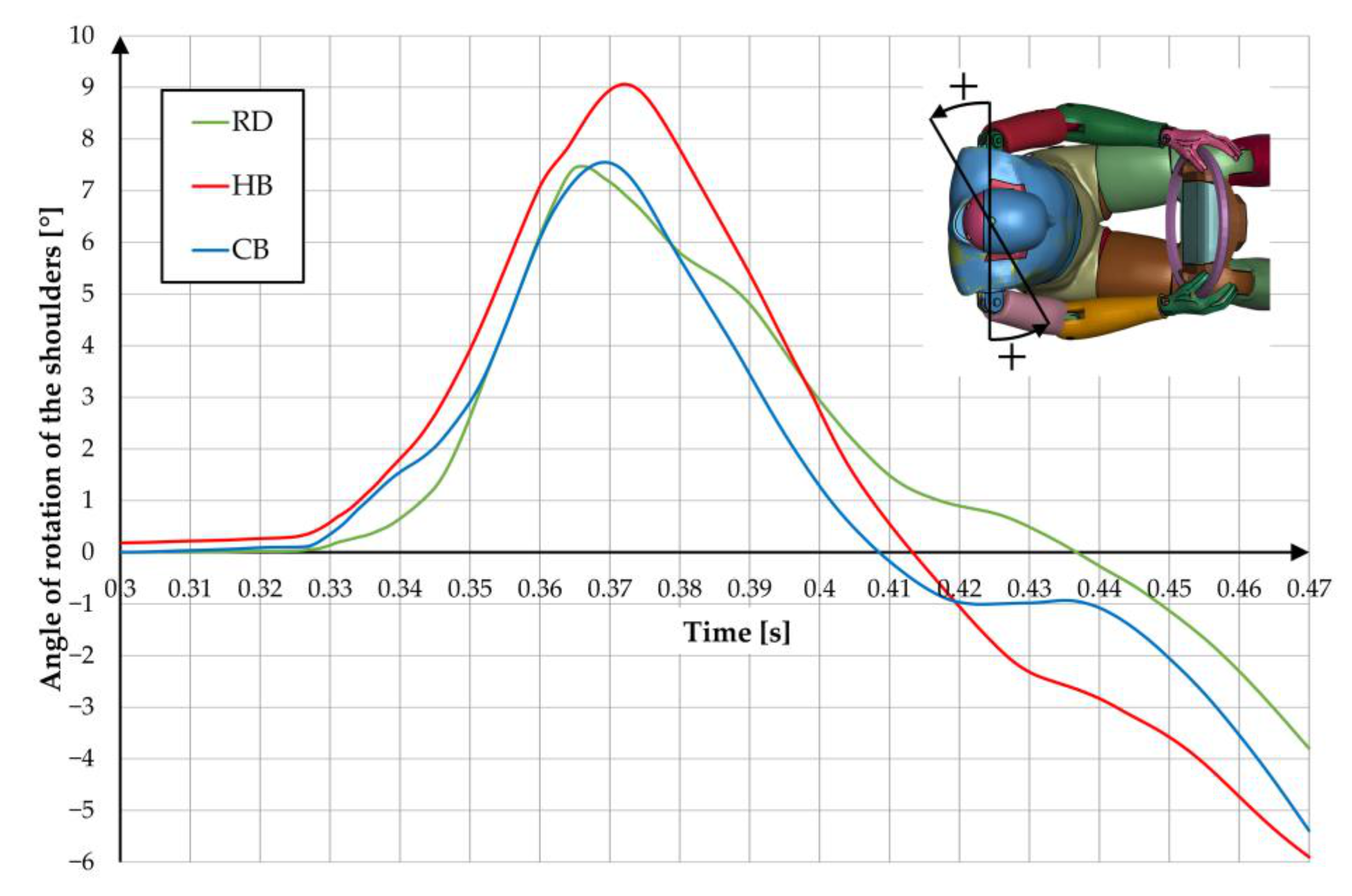
Lateral movements go with shoulder rotation. When analysing the influence of the equipment used for DP (
Figure 11), there is no significant change. At the initial impact phase, in all cases, the right shoulder extends forwards more and, after rebounding from the airbag, the arms start to rotate in the opposite direction.
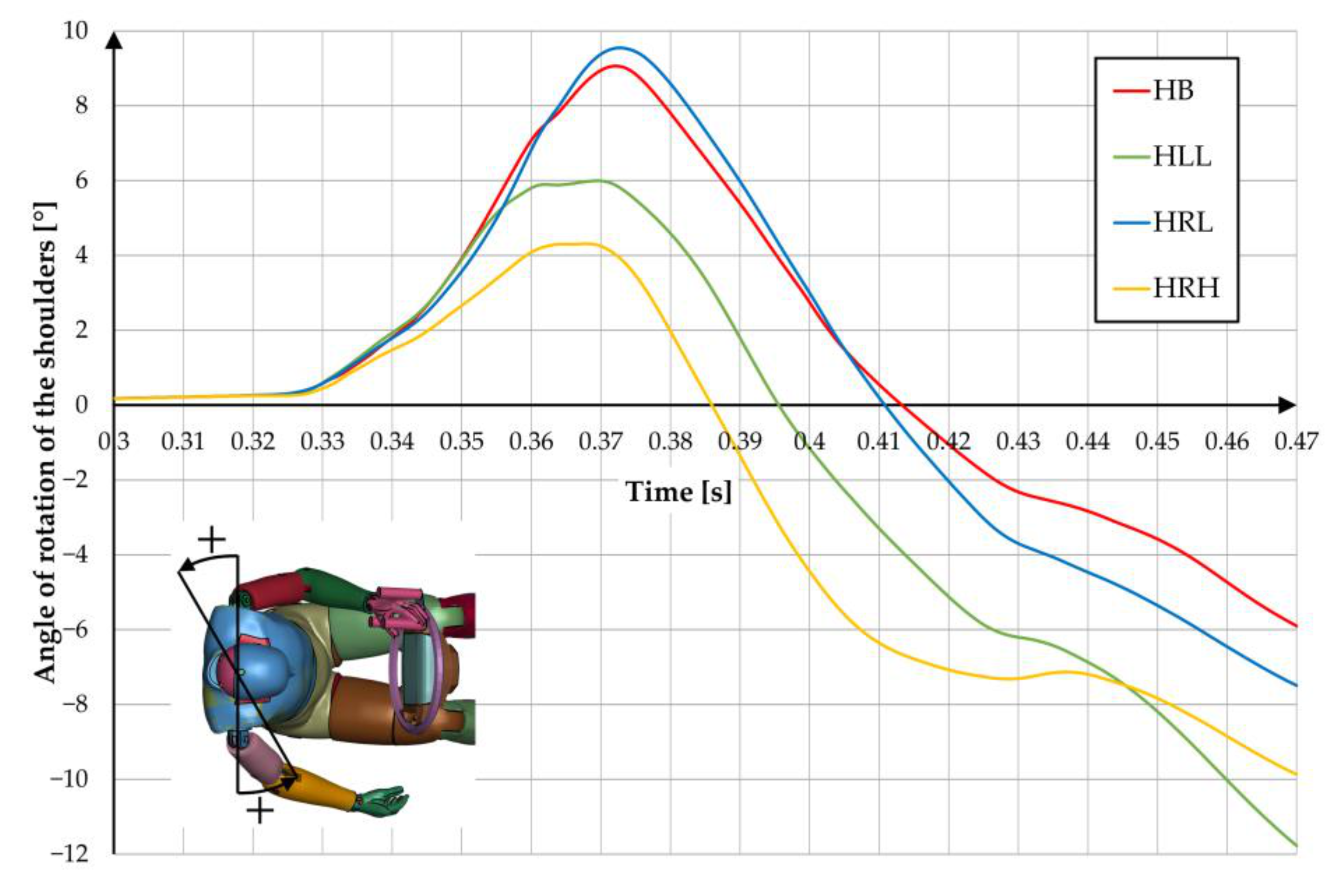
Analysing group H, one can see the same type of changes, but with different levels of them (
Figure 12). The highest rotation in the first impact phase is for HB and HRL cases (about 9°). In the second phase, for HLL and HRH (above 10°).
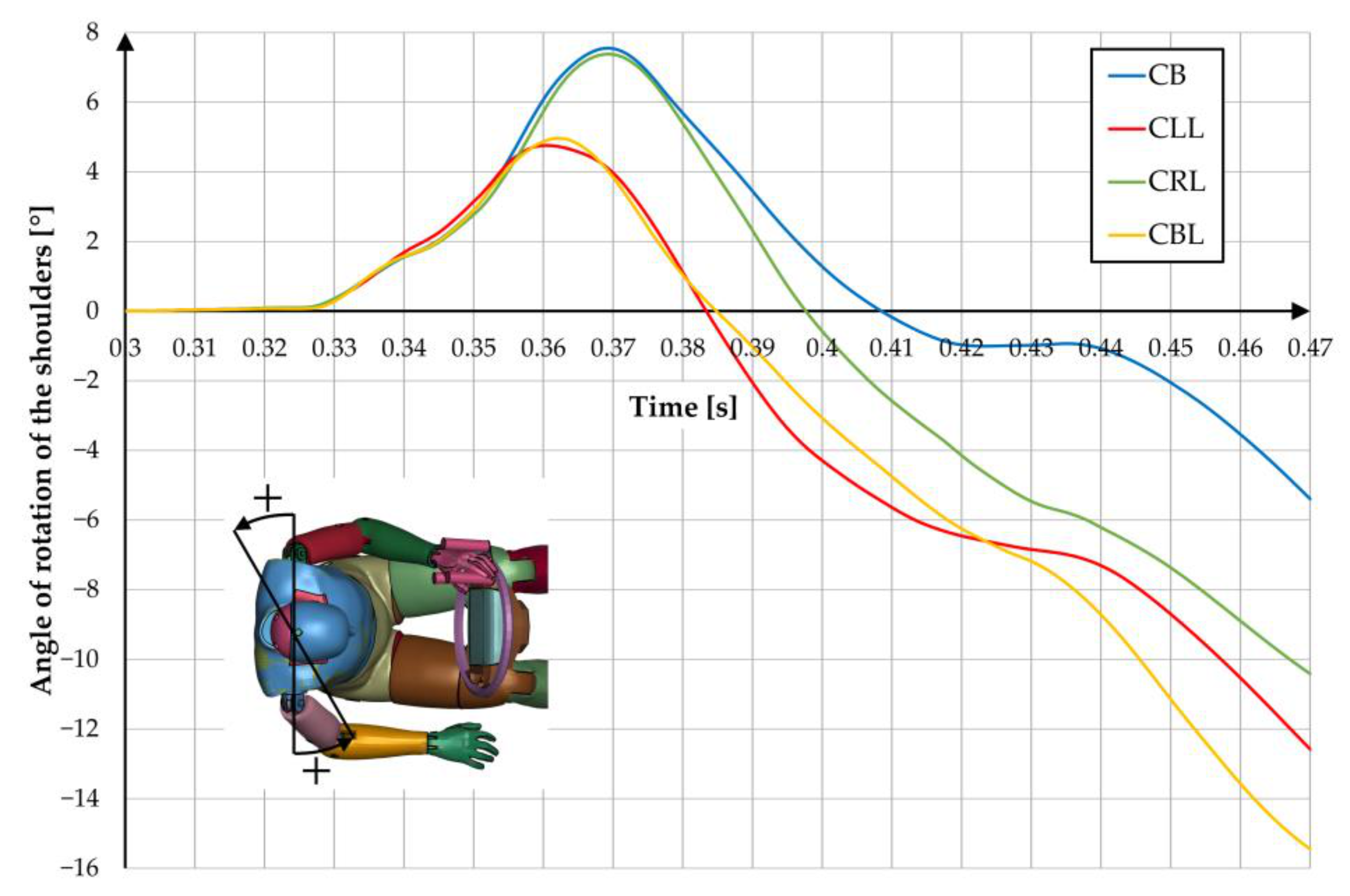
Similarly, for group C (
Figure 13). In the first phase, the highest rotation is for CB and CRL (about 7.5°) and in the second phase for CLL (over 12°) and CBL (over 15°).
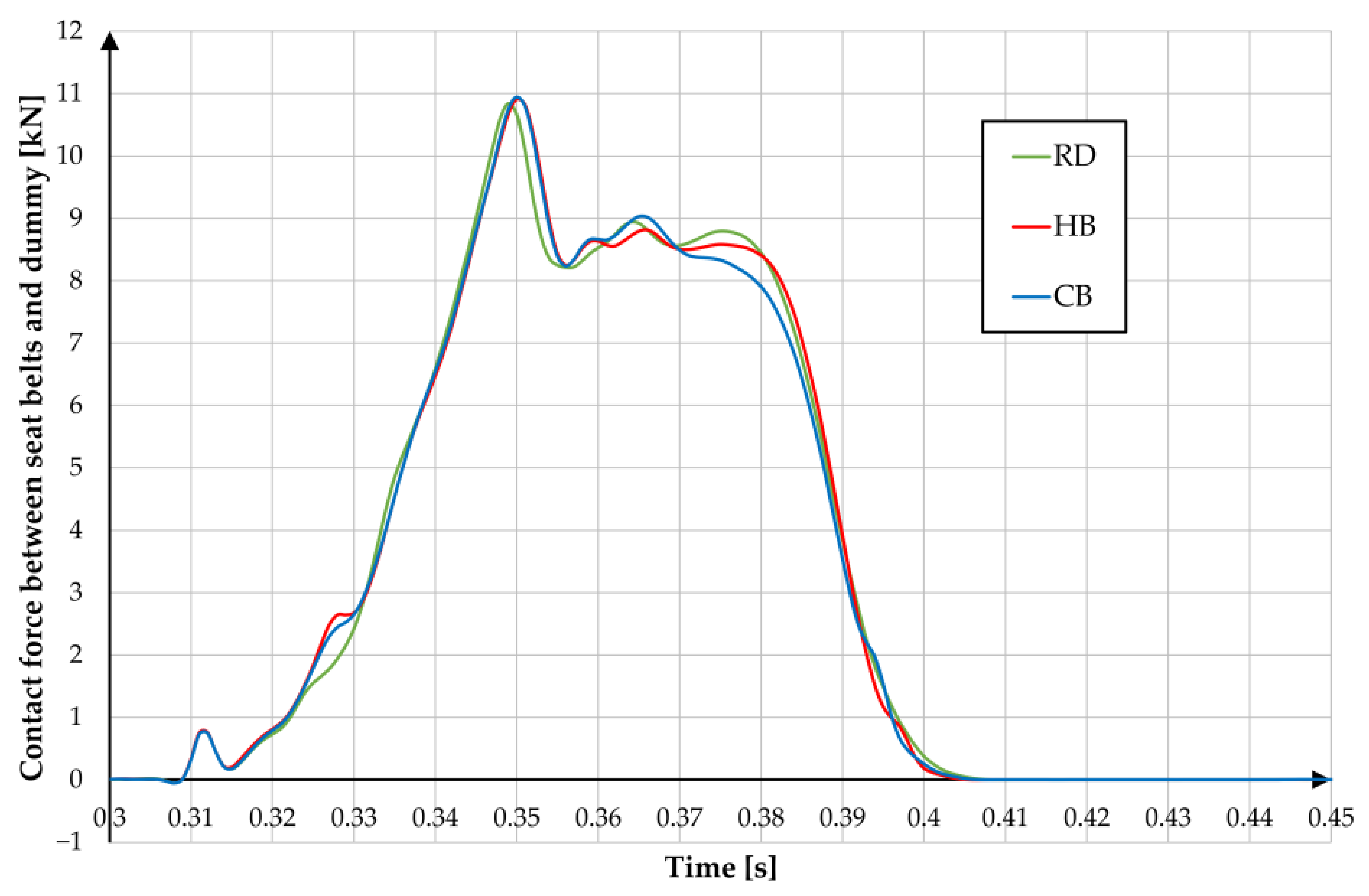
The work also analysed the course of change of forces between the dummy and seat belts. In cases where the dummy had all the limbs, no significant changes between the individual runs are visible (
Figure 14). The highest peak of strength occurs immediately before the head of the dummy (and thus part of the chest) contacts the airbag. After that time, the value drops by about 2 kN and is maintained until the maximum longitudinal displacement of the dummy in relation to the chair is reached.
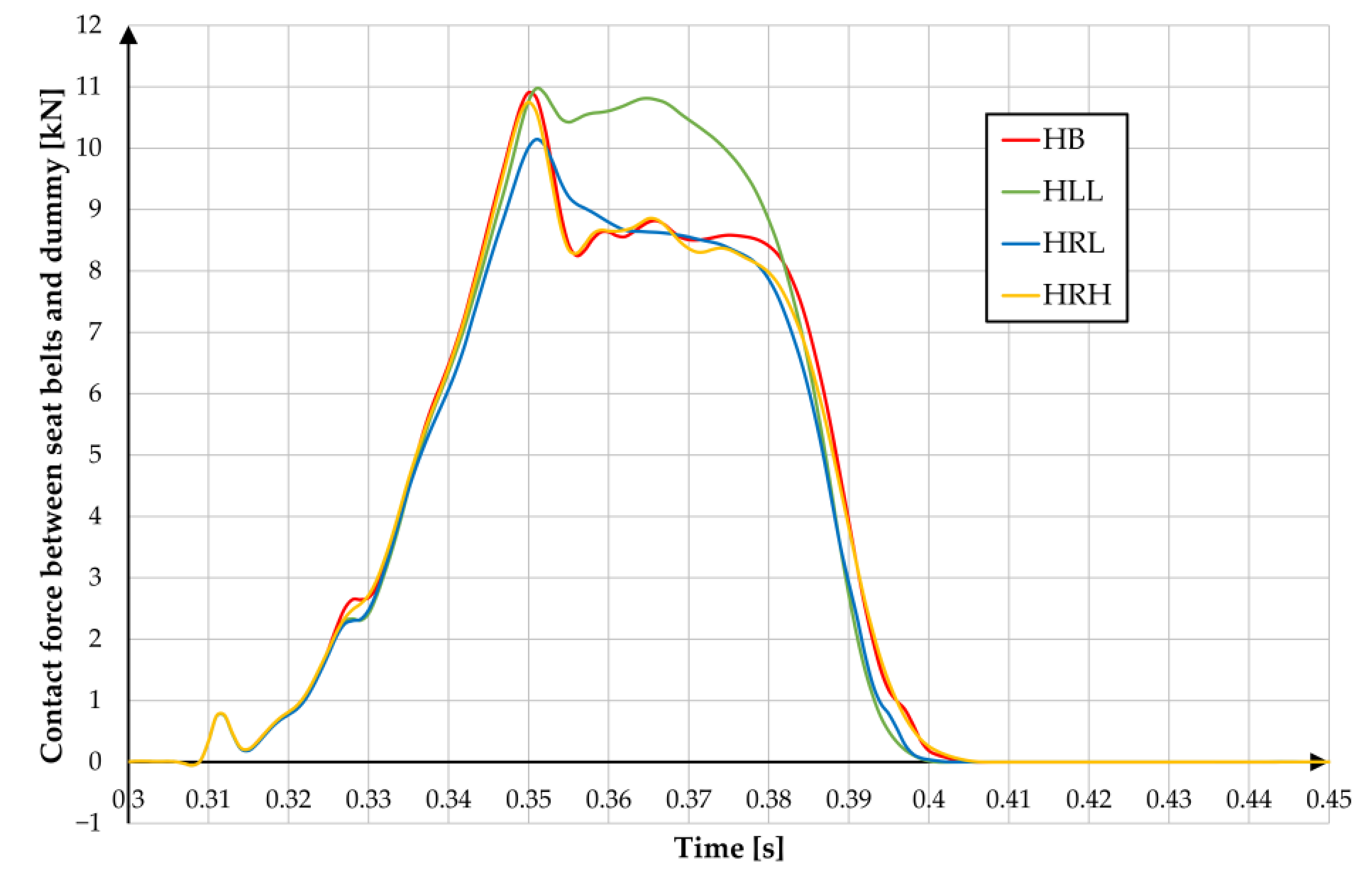
A similar character of the course of force between the belts and the dummy can be observed for analyses from group H (
Figure 15). Only in the HLL there is no decrease in force, it remains at a constant level until the time when the maximum movement of the longitudinal dummy in relation to the seat is reached.
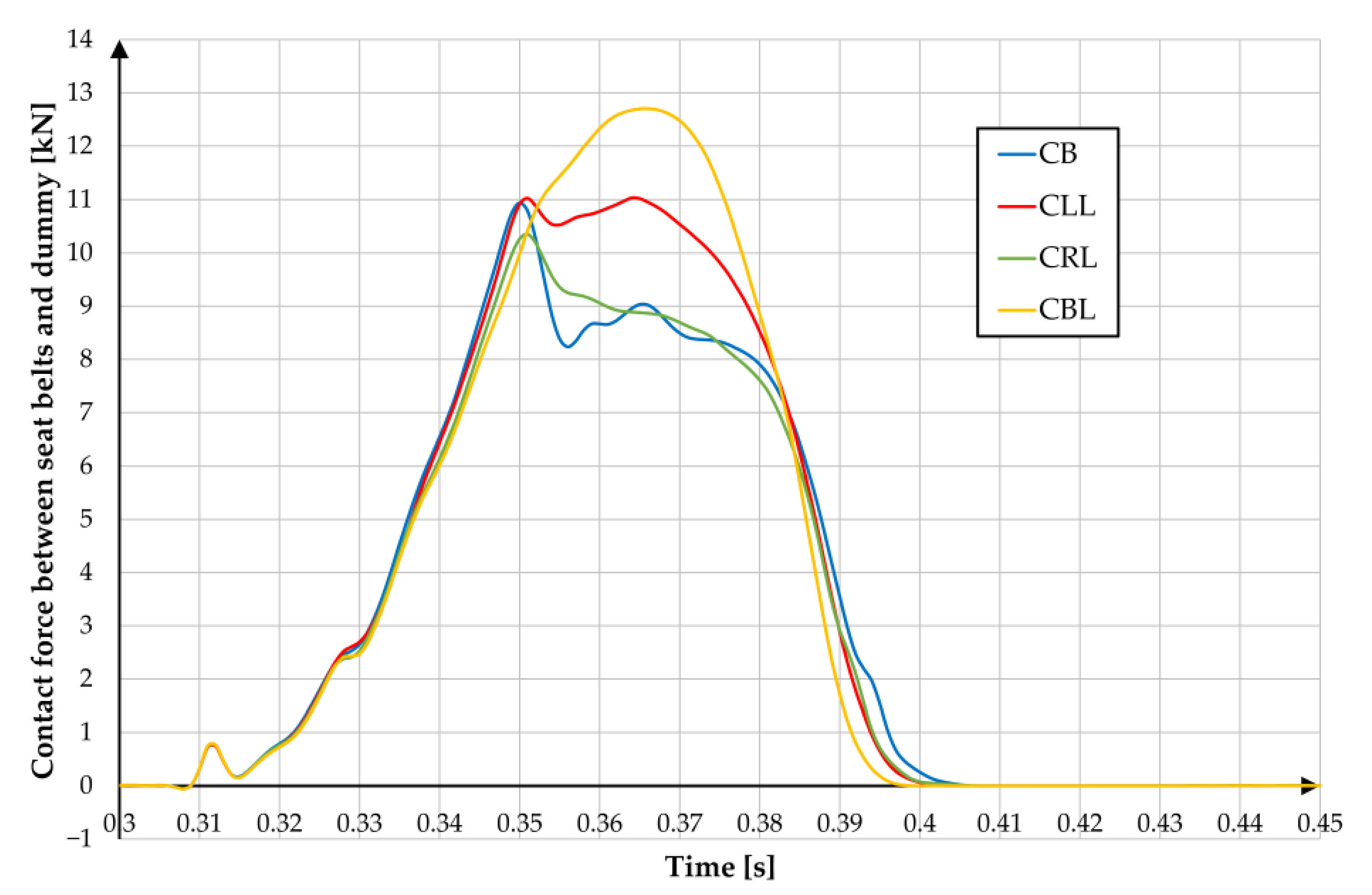
In group C (
Figure 16), no loss of strength after the dummy starts to contact the airbag is visible in two cases—CBL and CLL.
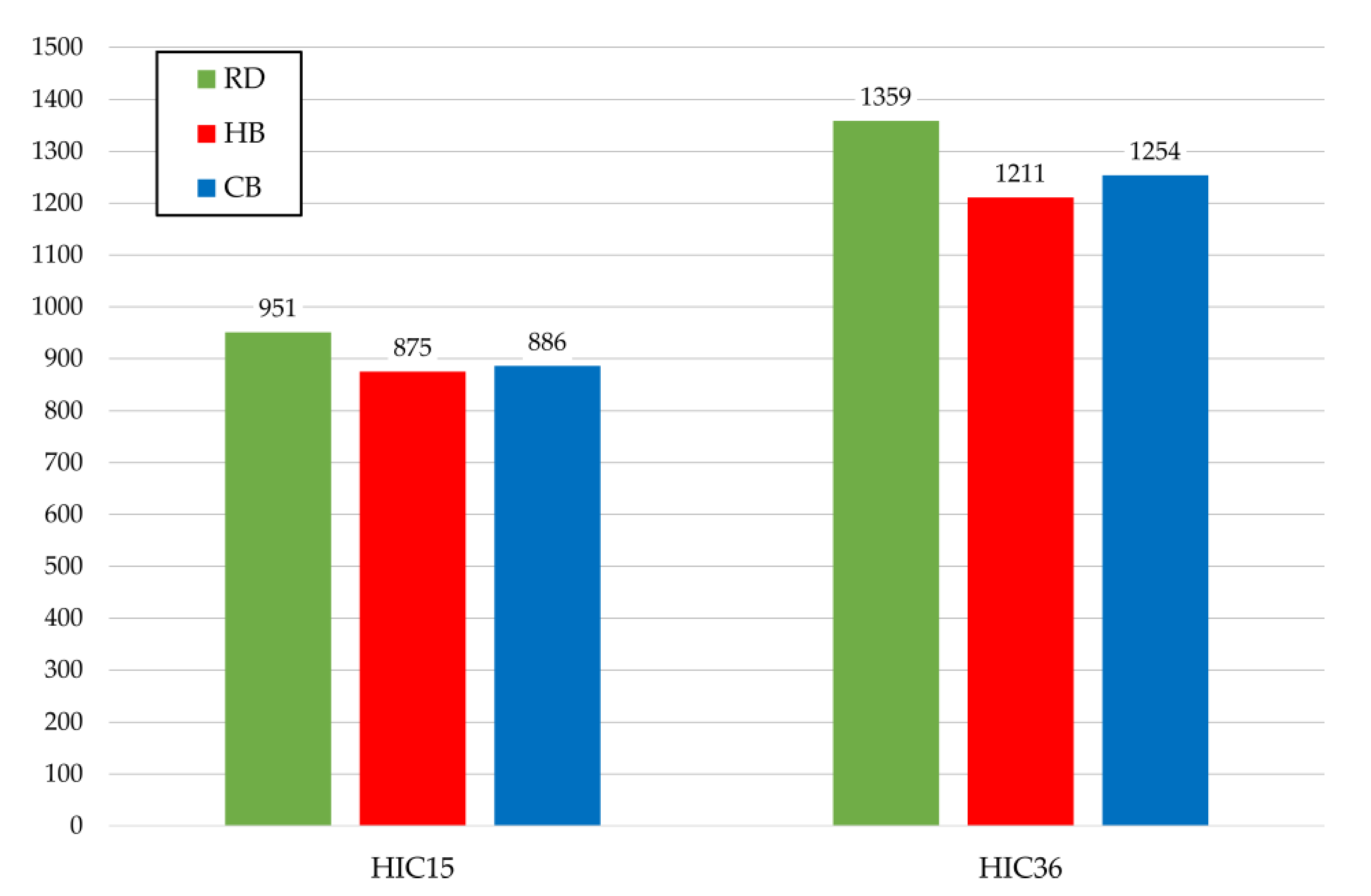
The use of additional equipment for the DP, in addition to influencing lateral displacement, shoulder rotation and the course of force between the belts and the dummy, also affects skull injuries expressed as HIC (Head Injury Criterion) (
Figure 17). Compared to RD, HB and CB have at least 6% lower HIC15 and 7% lower HIC36 values.
In the H group (
Figure 18), different HIC15 and HIC36 values were obtained for individual cases, but no significant differences were observed. The maximum reaches respectively 4% and 3%.
In group C (
Figure 19) for HIC15 the difference between the maximum and minimum result is about 4%. For HIC36 the difference increases less than 6%. The smallest value was obtained for CLL and the largest for CB.
4. Discussion
The main objective of the study is to examine the effect of the change in driver’s centre of gravity due to various disabilities and the change in the points of support of the body due to the use of additional equipment on the driver’s behaviour during a frontal collision. Due to the inability to carry out such studies through experimental tests, it was decided to employ a research methodology based on numerical analyses using the finite element method, with an explicit integration step. Thanks to FE studies, it was possible, among other things, to consider (in a virtual environment) the vulnerabilities of the car’s interior structures, crucial from the point of view of the driver’s behaviour, and of the dummy itself. A common approach to analyses of this type is to isolate a single phenomenon (with all the key elements) from the global system and to conduct studies on the influence of single parameters on the course of this phenomenon [
19,
21,
32,
33,
34]. For frontal crash analyses aimed at assessing the driver’s safety, this is most often a restriction of the numerical model to the area around the driver and modelling selected safety components such as seat belts [
19,
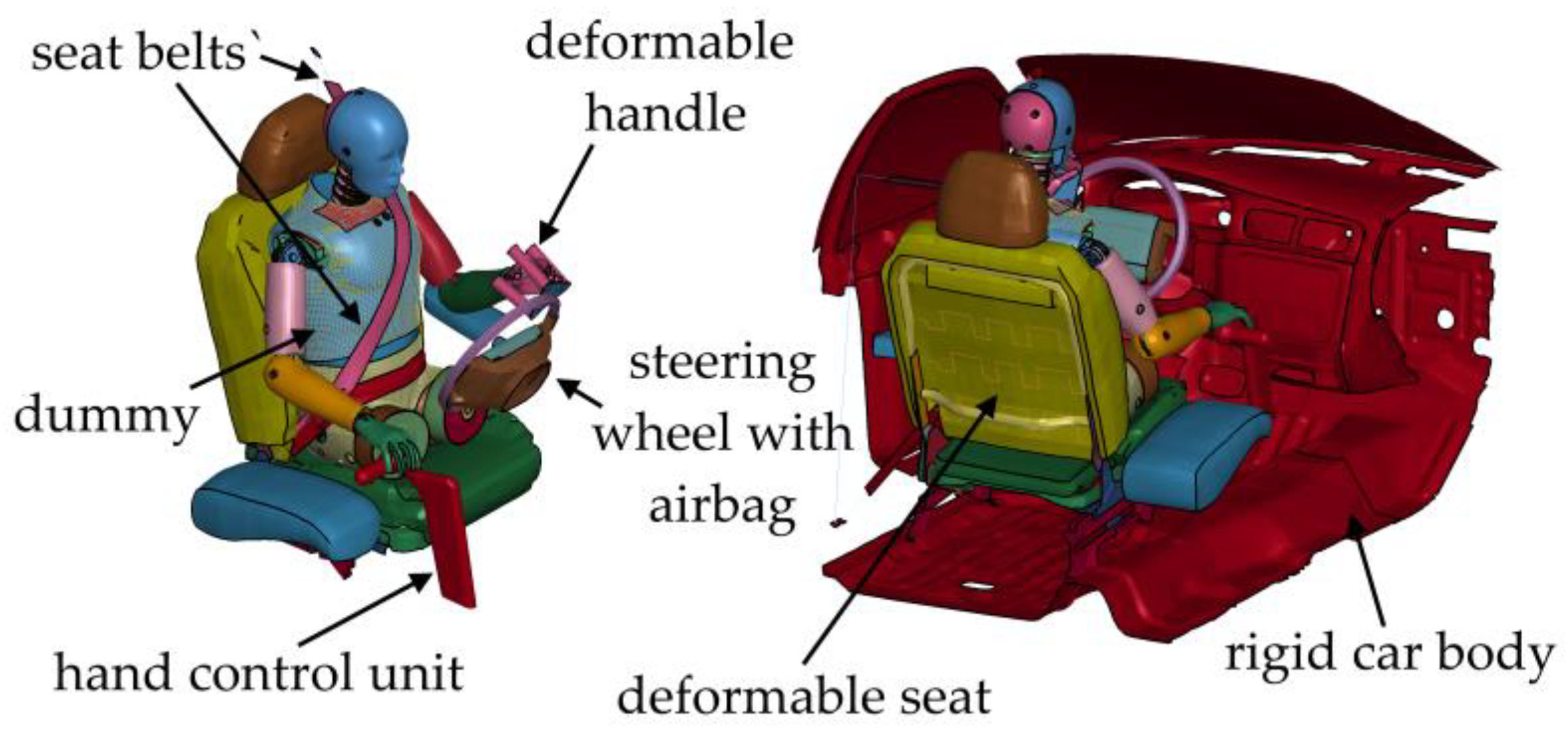
34] or an airbag. In this study the best possible reproduction of real objects and phenomena was sought, therefore a great deal of emphasis was placed on the use of the full characteristics of the car body delay during the collision, considering the deformation of the seat under the influence of the weight of the dummy, the friction between them, and the representation of the full operation of the seat belt system and the airbag. This was made possible by dividing the whole frontal impact into three phases—frontal impact of the car with a rigid barrier, subsidence of the dummy under the influence of gravity and the numerical analysis of the behaviour of the dummy inside an isolated part of the vehicle.
The authors were not able to carry out a validation test for the developed numerical models. Instead, the global model is built from smaller numerical models validated in independent tests [
18,
29]. In this study, a commercially approved numerical model of the dummy [
35], an approved car model [
36] and constitutive models of seat belts were used.
Frontal collisions, both full cars and selected vehicle parts, are very well documented in the literature. Nevertheless, the authors did not find any studies on the safety of disabled persons in the literature, so it is difficult to relate the results to other works.
In personal cars, the forces exerted on the body of a non-disabled driver during a frontal collision are asymmetrical. Excluding the asymmetrical positioning of the steering wheel in relation to the torso in many cars, asymmetry is mainly caused by the position of the legs and the operation of the seat belts. In the case of cars with automatic transmission, the right leg is usually set straight ahead or more inwards on the brake pedal during a collision. The left leg rests on a footrest that in many cars is positioned to the left and is closer to the seat than the fully depressed brake pedal. Seat belts, on the other hand, restrict the movement of the left arm, which naturally causes the rotation of the driver’s shoulders visible in
Figure 11. This rotation increases until the torso rests on the airbag and the driver rebounds from it. From now on, the arms start to rotate in the opposite direction. The lower limbs mentioned previously also play a major role in the first stage of the collision, as the driver moves longitudinally to the seat and hits the space under the steering wheel with his knees. This is considered by vehicle designers at the development stage.
The introduction of additional equipment on the steering wheel or the amputation of the driver’s limb affects the process described above. When analysing the position of the dummy at the moment of maximum longitudinal displacement relative to the seat (
Figure 7) it can be seen that the use of additional equipment on the steering wheel or between the seats affects the position of the driver’s body immediately before the collision. The stiffness of these elements is so low that it does not generate significant movement resistance for the driver. The limb amputation, however, changes the number of support points of the driver, both immediately before the collision and during the loss of his kinetic energy. In addition, if one of the lower limbs is amputated, the latter is automatically more likely to suffer an injury as it will hit the components under the steering wheel with more force.
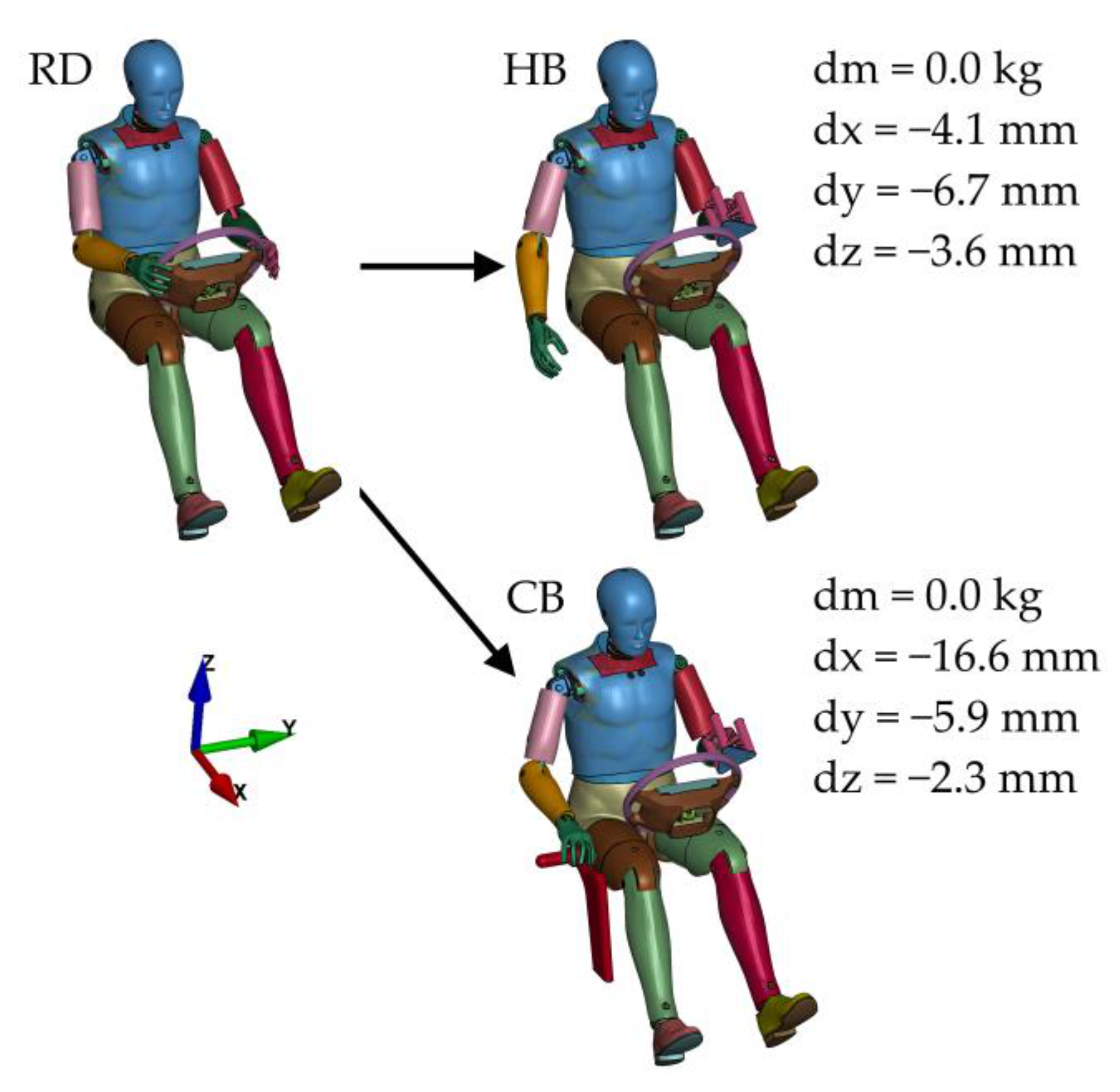
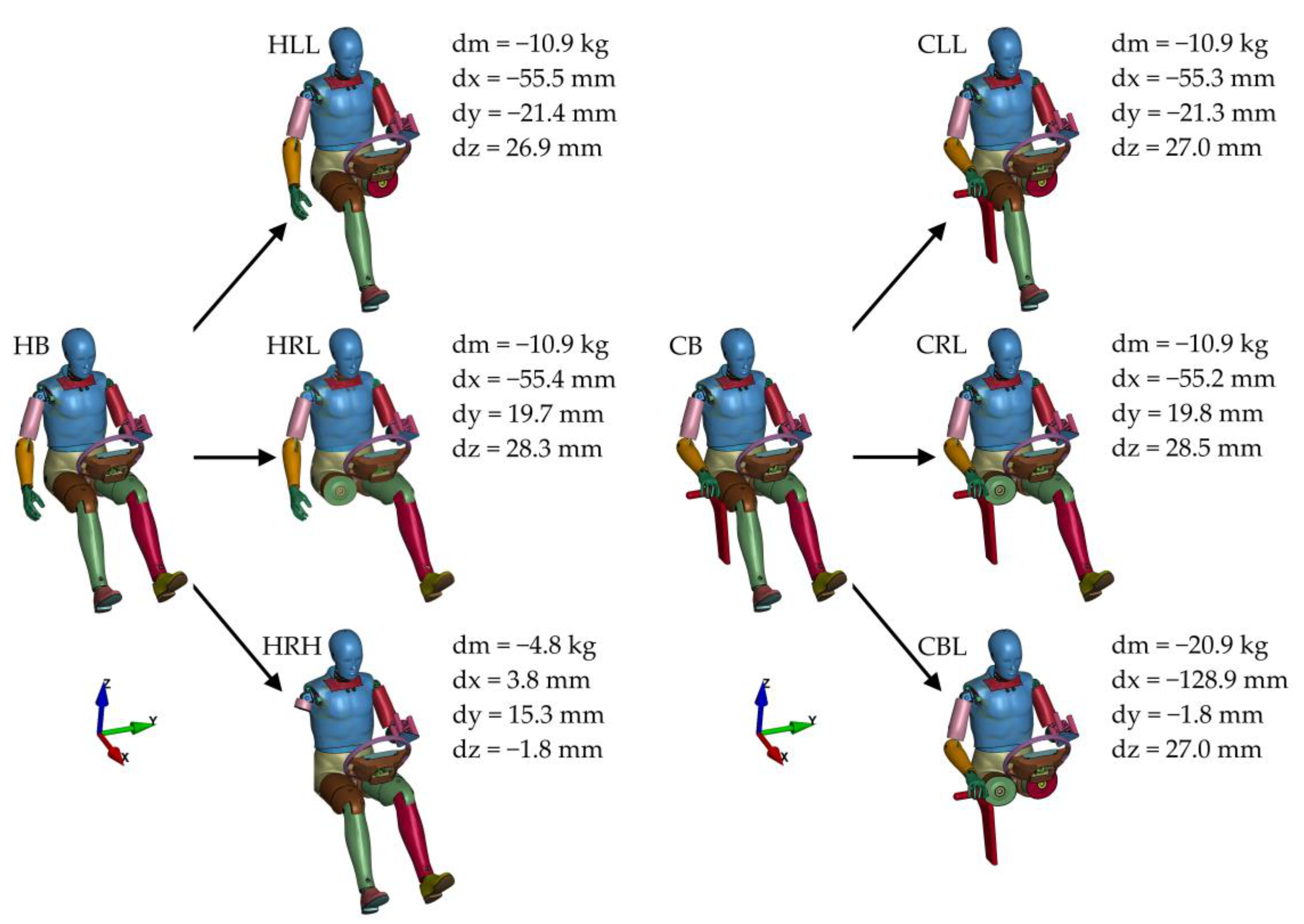
The changes in the position of the centre of gravity, as shown in
Figure 4 and
Figure 5, clearly indicate that the sole use of a disabled person’s equipment has a slight effect on the change in the driver’s centre of gravity. Amputation, in turn, results in a significant reduction in the weight of the entire driver and thus in a significant shift in the driver’s centre of gravity. On the one hand, the reduction in the driver’s weight means less kinetic energy to reduce, on the other hand, a change in body position affects the operation of safety systems.
Figure 8 shows the lateral displacement of the driver’s H-point, which shows that the use of a steering wheel handle or additional Hand Control Unit results in no return to the initial position of the driver’s pelvis after a rebound from the airbag. This is particularly evident at time t = 0.43 s when the driver hits the seat’s backrest. This is a very negative phenomenon, as it can result in missing the headrest and suffering a serious neck injury. This effect is even stronger in the case of amputation of any of the limbs (
Figure 9 and
Figure 10).
However, the use of additional equipment does not have a significant influence on the rotation of the arms (
Figure 11). The amputation, especially of the left leg, both legs or right hand, does influence the rotation (
Figure 12 and
Figure 13). In the case of the amputation of the right hand, the mass that causes the rotation by its inertia decreases significantly and thus the rotation diminishes. A similar diminished rotation in the initial phase of movement can be observed in the case of the amputation of the left leg or both legs. This is because the left leg rests on a footrest that is closer to the seat than the brake pedal pressed to the end. In the event of a collision, the leg pushes against its entire surface, while the right leg slides on the brake pedal. Thus, in the case of drivers without disabilities, the left leg increases the rotation, and in the case of a disabled driver, the lack of the limb reduces the rotation.
Lack of support for the left leg means that the belts and the airbag must carry more load (
Figure 15 and
Figure 16), which may result in increased chest injuries. The analyses carried out showed that the other factors examined did not have a significant impact on the course of force between the dummy and the belts. The modifications made also had no significant impact on HICs.
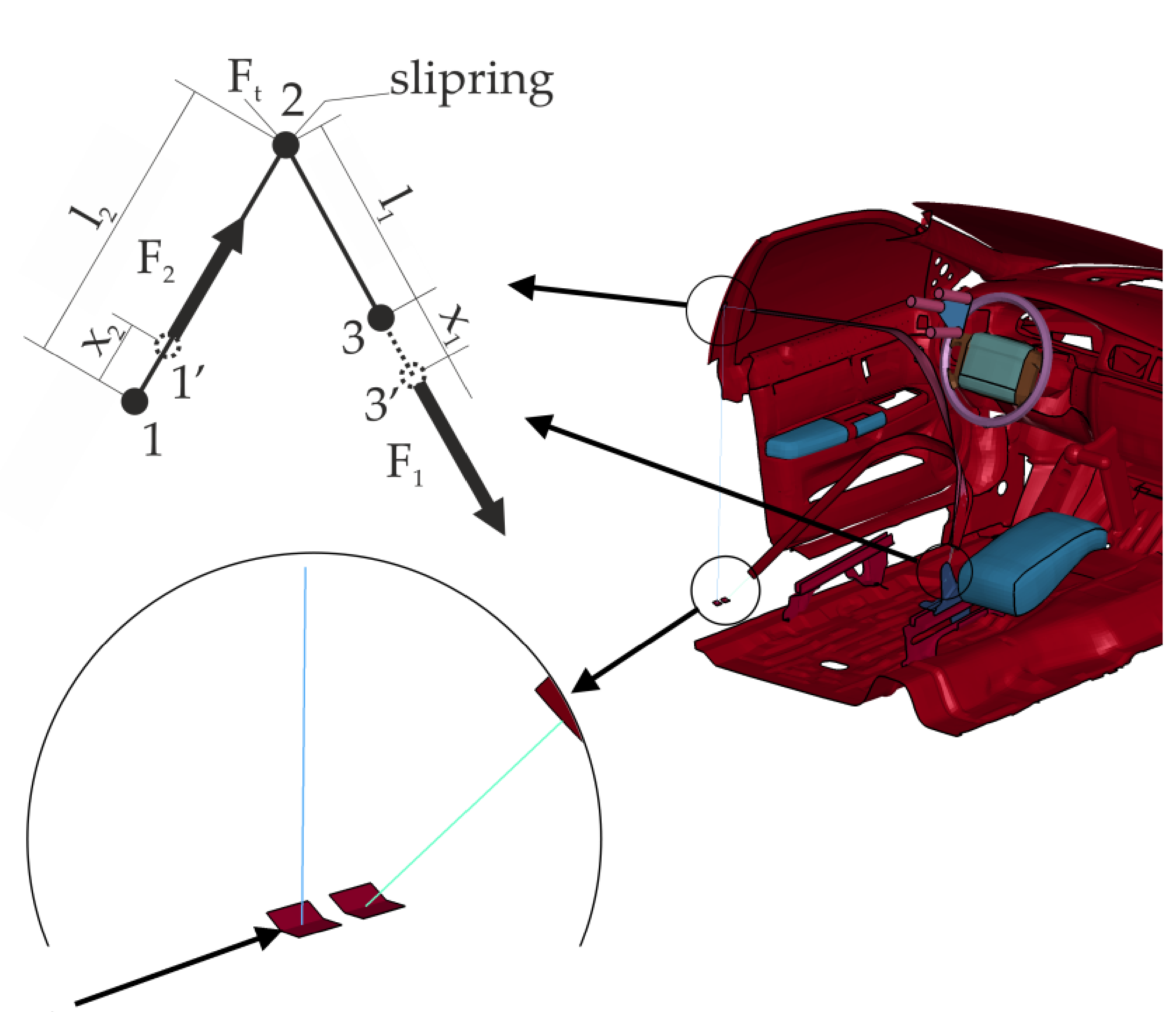
To sum up, the contribution of this paper is to present a three-stage scheme for conducting numerical analyses of the behaviour of people inside a car during a crash. The article justifies the importance of each of the stages and the use of the results of each of them in the analysis of the entire phenomenon. The paper also presents a method of seat belts modelling aimed at a faithful representation of their actual operation. Describes an approach using a combination of 2D elements (in area of contact with the driver) and 1D elements (which enable the operation of the retractor, pretensioner and slipring). A detailed diagram of the operation of the slipring elements is also presented. Based on the modelling performed, the paper presents the original results of analyses of the effect of changes in the position of the driver’s centre of gravity caused by additional equipment for disabled people and amputations of the limbs on his behaviour during a frontal collision. Based on the results, it can be concluded that it is appropriate to carry out research aimed at assessing the safety of drivers using vehicles adapted to the needs of disabled people. The position of the driver immediately before the collision and the number of support points of the body affects his interaction with the safety systems and may affect his injuries.
Further work will be aimed at studying the impact of prostheses on the safety of a disabled driver.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


















