
An AI-Based Exercise Prescription Recommendation System


Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Data Preprocessing
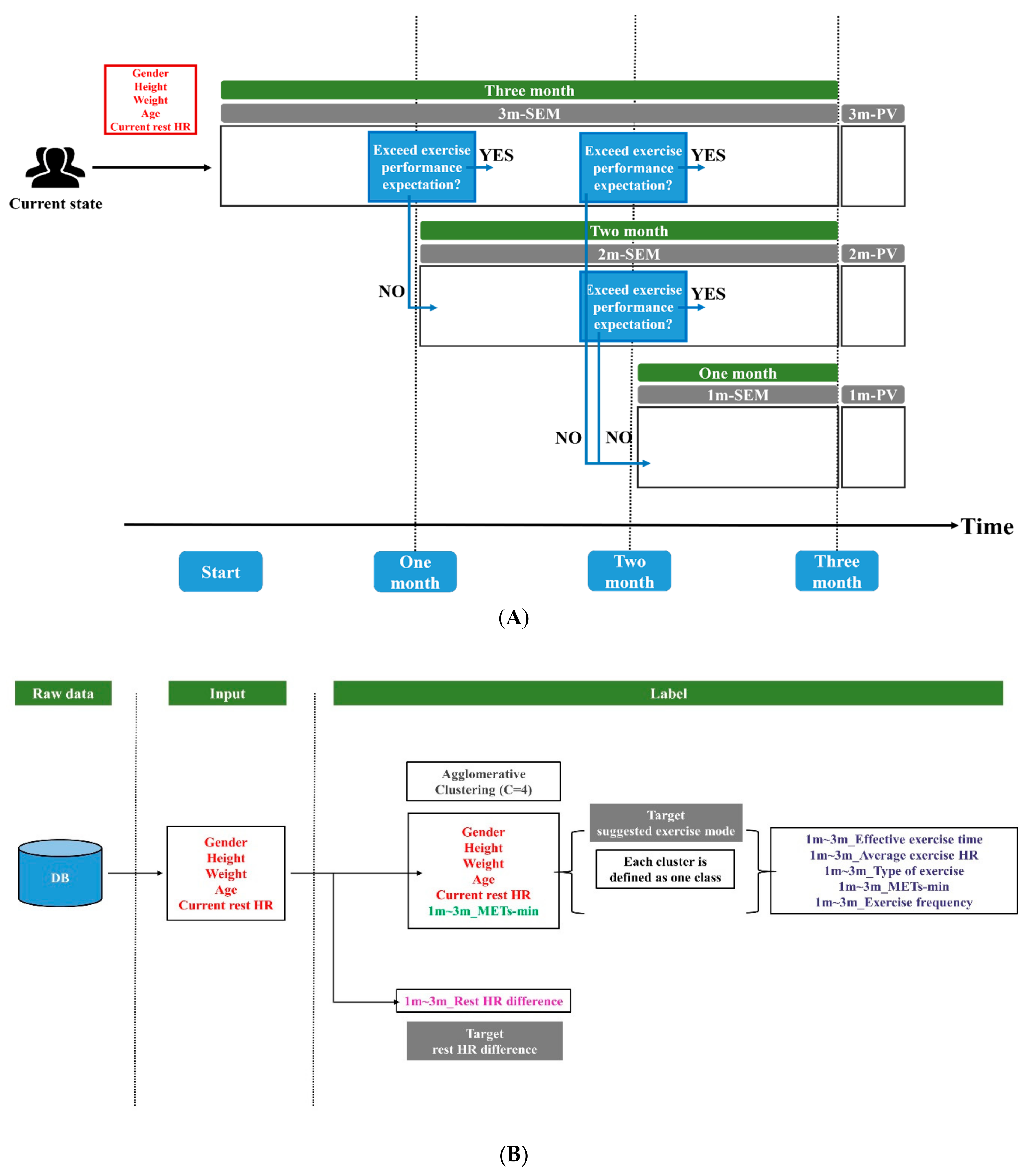
2.3. Exercise Scenario
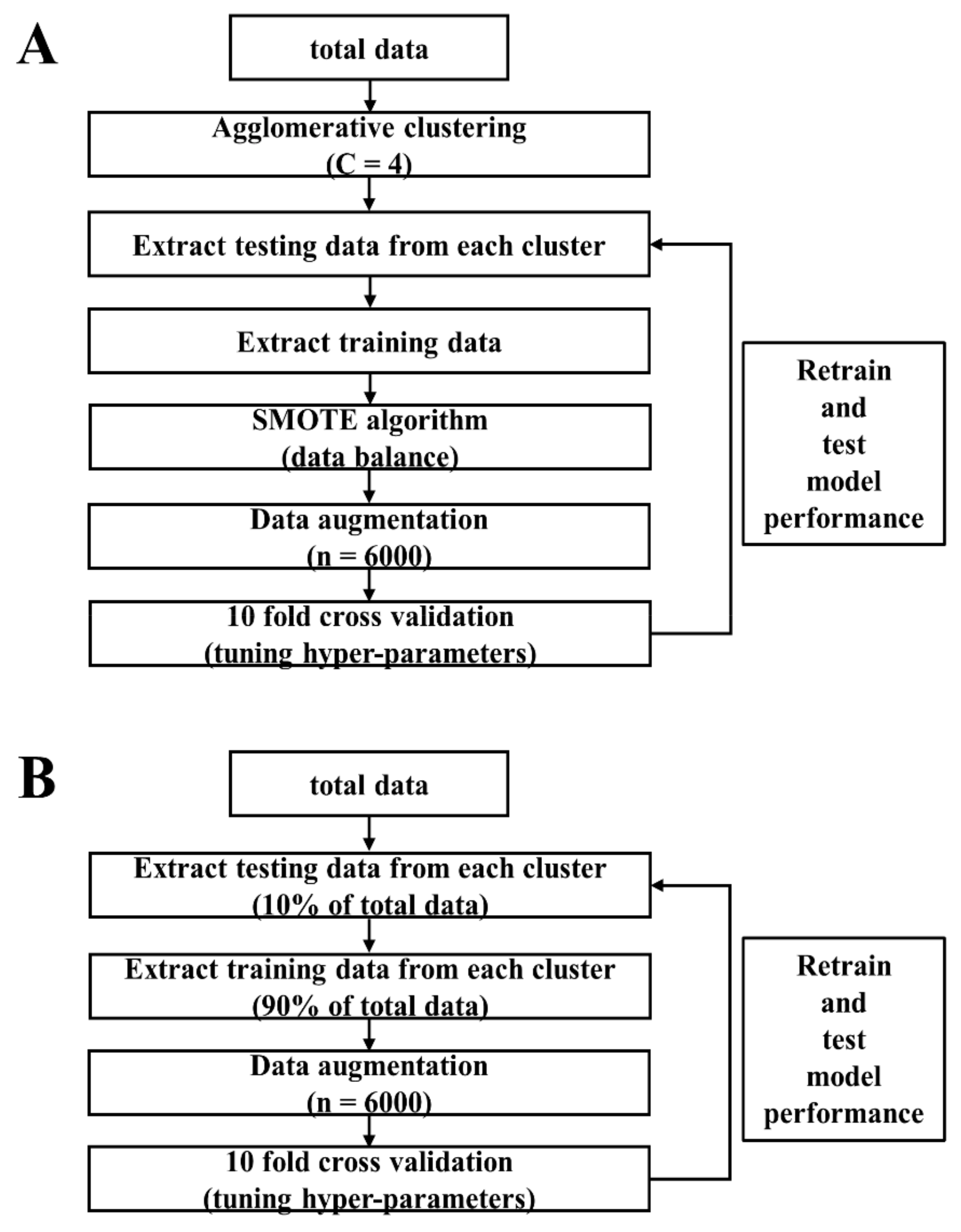
2.4. Modules Construction
3. Results
3.1. Testing Accuracy of SEM Modules
3.2. Exercise Mode Analysis in Each Group
3.3. Testing Accuracy of PV Modules
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP). Available online: https://www.cdc.gov/chronicdisease/about/costs/index.htm (accessed on 1 January 2021).
- Murtagh, E.M.; Nichols, L.; Mohammed, M.A.; Holder, R.; Nevill, A.M.; Murphy, M.H. The effect of walking on risk factors for cardiovascular disease: An updated systematic review and meta-analysis of randomised control trials. Prev. Med. 2015, 72, 34–43. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Zhang, X.; Guo, J.; Roberts, C.K.; McKenzie, S.; Wu, W.; Liu, S.; Song, Y. Effects of Exercise Training on Cardiorespiratory Fitness and Biomarkers of Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2015, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pattyn, N.; Cornelissen, V.A.; Eshghi, S.R.T.; Vanhees, L. The Effect of Exercise on the Cardiovascular Risk Factors Constituting the Metabolic Syndrome: A Meta-Analysis of Controlled Trials. Sports Med. 2013, 43, 121–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Authors/Task Force Members; Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; et al. 2016 European Guidelines on Cardiovascular Disease Prevention in Clinical Practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by Representatives of 10 Societies and by Invited Experts): Developed with the Special Contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. J. Prev. Cardiol. 2016, 23, NP1–NP96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Martin, E.; Costa, A.; Cazorla, M. PHAROS 2.0-A PHysical Assistant RObot System Improved. Sensors 2019, 19, 4531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulikowski, P.; Zdziebko, T. Deep learning-enhanced framework for performance evaluation of a recommending interface with varied recommendation position and intensity based on eye-tracking equipment data processing. Electronics 2020, 9, 266. [Google Scholar] [CrossRef] [Green Version]
- Sulikowski, P.; Zdziebko, T.; Turzyński, D.; Kańtoch, E. Human-website interaction monitoring in recommender systems. Procedia Comput. Sci. 2018, 126, 1587–1596. [Google Scholar] [CrossRef]
- Schwalbe, N.; Wahl, B. Artificial intelligence and the future of global health. Lancet 2020, 395, 1579–1586. [Google Scholar] [CrossRef]
- Loellgen, H.; Zupet, P.; Bachl, N.; Debruyne, A. Physical Activity, Exercise Prescription for Health and Home-Based Rehabilitation. Sustainability 2020, 12, 10230. [Google Scholar] [CrossRef]
- Tran, T.N.T.; Felfernig, A.; Trattner, C.; Holzinger, A. Recommender systems in the healthcare domain: State-of-the-art and research issues. J. Intell. Information Syst. 2020, 1–31. [Google Scholar] [CrossRef]
- Hansen, D.; Dendale, P.; Coninx, K.; Vanhees, L.; Piepoli, M.F.; Niebauer, J.; Cornelissen, V.; Pedretti, R.; Geurts, E.; Ruiz, G.R. The European Association of Preventive Cardiology Exercise Prescription in Everyday Practice and Rehabilitative Training (EXPERT) tool: A Digital Training and Decision Support System for Optimized Exercise Prescription in Cardiovascular Disease. Concept, Definitions and Construction Methodology. Eur. J. Prev. Cardiol. 2017, 24, 1017–1031. [Google Scholar] [PubMed]
- Hansen, D.; Niebauer, J.; Cornelissen, V.; Barna, O.; Neunhäuserer, D.; Stettler, C.; Tonoli, C.; Greco, E.; Fagard, R.; Coninx, K. Exercise prescription in patients with different combinations of cardiovascular disease risk factors: A consensus statement from the EXPERT working group. Sports Med. 2018, 48, 1781–1797. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Lu, Y.; Feng, L.Y.; Qiu, J.C.; Zou, L.A.; Qu, R.J.; Fan, X.X.; Xie, J.; Wei, Q. Preliminary study of Sub-Health Measurement Scale Version1.0 Norms for Chinese Civil Servants. J. South. Med. Univ. 2011, 31, 1654–1662. [Google Scholar]
- Saxena, A.; Minton, D.; Lee, D.-C.; Sui, X.; Fayad, R.; Lavie, C.J.; Blair, S.N. Protective Role of Resting Heart Rate on All-Cause and Cardiovascular Disease Mortality. Mayo Clin. Proc. 2013, 88, 1420–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.I.; Kim, H.C.; Jeon, J.Y. The association of resting heart rate with diabetes, hypertension, and metabolic syndrome in the Korean adult population: The fifth Korea national health and nutrition examination survey. Clin. Chim. Acta 2016, 455, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Togni, M.; Schaub, M.C.; Wenaweser, P.; Hess, O.M. High heart rate: A cardiovascular risk factor? Eur. Hear. J. 2006, 27, 2387–2393. [Google Scholar] [CrossRef]
- Aune, D.; Sen, A.; Ó’Hartaigh, B.; Janszky, I.; Romundstad, P.; Tonstad, S.; Vatten, L. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality—A systematic review and dose–response meta-analysis of prospective studies. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 504–517. [Google Scholar] [CrossRef]
- Aladin, A.I.; Al Rifai, M.; Rasool, S.H.; Keteyian, S.J.; Brawner, C.A.; Michos, E.D.; Blaha, M.J.; Al-Mallah, M.H.; McEvoy, J.W. The Association of Resting Heart Rate and Incident Hypertension: The Henry Ford Hospital Exercise Testing (FIT) Project. Am. J. Hypertens. 2016, 29, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reimers, A.K.; Knapp, G.; Reimers, C.-D. Effects of Exercise on the Resting Heart Rate: A Systematic Review and Meta-Analysis of Interventional Studies. J. Clin. Med. 2018, 7, 503. [Google Scholar] [CrossRef] [Green Version]
- A Cornelissen, V.; Verheyden, B.; E Aubert, A.; Fagard, R.H. Effects of aerobic training intensity on resting, exercise and post-exercise blood pressure, heart rate and heart-rate variability. J. Hum. Hypertens. 2010, 24, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.-M. Effects of a cardiorespiratory synchronization training mobile application on heart rate variability and electroencephalography in healthy adults. Int. J. Psychophysiol. 2018, 134, 168–177. [Google Scholar] [CrossRef]
- Yager, R.R. Intelligent control of the hierarchical agglomerative clustering process. IEEE Trans. Syst. Man Cybern. Part B Cybern. 2000, 30, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.; Belo, D.; Gamboa, H. Noise detection on ECG based on agglomerative clustering of morphological features. Comput. Biol. Med. 2017, 87, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Su, S.; Huang, Z.; Guo, X.; Zuo, Z.; Sun, X.; Li, L. Wireless Sensor Networks Intrusion Detection Based on SMOTE and the Random Forest Algorithm. Sensors 2019, 19, 203. [Google Scholar] [CrossRef] [Green Version]
- JoiiUp Technology Corporation. Available online: https://www.joiiup.com/news/content/20 (accessed on 1 January 2021).
- Chen, H.-K.; Hu, Y.-F.; Lin, S.-F. Methodological considerations in calculating heart rate variability based on wearable device heart rate samples. Comput. Biol. Med. 2018, 102, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L.; et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 2016, 354, i3857. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Raw Data | One-Hot Encoding | Transferred Data |
|---|---|---|
| Gender | 0 | [1,0] |
| 1 | [0,1] | |
| Height | Height < 150 | [1,0,0,0,0] |
| 150 ≦ Height < 160 | [0,1,0,0,0] | |
| 160 ≦ Height < 170 | [0,0,1,0,0] | |
| 170 ≦ Height < 180 | [0,0,0,1,0] | |
| 180 ≦ Height | [0,0,0,0,1] | |
| Weight | Weight < 50 | [1,0,0,0,0] |
| 50 ≦ Weight < 70 | [0,1,0,0,0] | |
| 70 ≦ Weight < 90 | [0,0,1,0,0] | |
| 90 ≦ Weight < 110 | [0,0,0,1,0] | |
| 110 ≦ Weight | [0,0,0,0,1] | |
| Age | Age < 17 | [1,0,0,0,0,0,0] |
| 17 ≦ Age < 25 | [0,1,0,0,0,0,0] | |
| 25 ≦ Age < 35 | [0,0,1,0,0,0,0] | |
| 35 ≦ Age < 45 | [0,0,0,1,0,0,0] | |
| 45 ≦ Age < 55 | [0,0,0,0,1,0,0] | |
| 55 ≦ Age < 65 | [0,0,0,0,0,1,0] | |
| 65 ≦ Age | [0,0,0,0,0,0,1] | |
| Rest HR | Rest HR < 50 | [1,0,0,0,0] |
| 50 ≦ Rest HR < 60 | [0,1,0,0,0] | |
| 60 ≦ Rest HR < 70 | [0,0,1,0,0] | |
| 70 ≦ Rest HR < 80 | [0,0,0,1,0] | |
| 80 ≦ Rest HR | [0,0,0,0,1] |
| (A) | Testing Accuracy (%) | 10-Fold Cross Validation | Fine-Tune | |
| Mean | Std | |||
| 1m-SEM | 95.93 | 0.86 | 95.80 (46/48) | |
| 2m-SEM | 99.02 | 0.34 | 100.00 (28/28) | |
| 3m-SEM | 98.45 | 0.41 | 95.00 (19/20) | |
| (B) | Testing MAE (BPM) | 10-Fold Cross Validation | Fine-Tune | |
| Mean | Std | |||
| 1m-PV | 2.86 | 0.08 | 3.15 | |
| 2m-PV | 2.72 | 0.09 | 2.89 | |
| 3m-PV | 2.59 | 0.08 | 2.75 | |
| 1m-SEM (n = 773) | |||||
| (A) | G1 (n = 211) | G2 (n = 163) | G3 (n = 279) | G4 (n = 120) | |
| Effective exercise time | 3202 | 3249 | 3152 | 3178 | |
| Average exercise HR | 126 | 124 | 128 | 126 | |
| Type of exercise | 1, 4 | 1, 9 | 1, 4 | 1, 4 | |
| Mets-min | 7324 | 8163 | 5922 | 9395 | |
| Exercise frequency | 3.31 | 3.36 | 3.13 | 3.61 | |
| 2m-SEM (n = 410) | |||||
| (B) | G1 (n = 158) | G2 (n = 85) | G3 (n = 68) | G4 (n = 99) | |
| Effective exercise time | 3109 | 3260 | 3351 | 3269 | |
| Average exercise HR | 127 | 124 | 121 | 128 | |
| Type of exercise | 1, 4 | 1, 4 | 1, 9 | 1, 9 | |
| Mets-min | 7001 | 11,431 | 9245 | 8377 | |
| Exercise frequency | 3.51 | 4.48 | 4.16 | 3.26 | |
| 3m-SEM (n = 269) | |||||
| (C) | G1 (n = 60) | G2 (n = 103) | G3 (n = 58) | G4 (n = 48) | |
| Effective exercise time | 3344 | 3373 | 3198 | 3206 | |
| Average exercise HR | 124 | 125 | 127 | 124 | |
| Type of exercise | 1, 9 | 1, 4 | 1, 4 | 1, 4 | |
| Mets-min | 8918 | 10,900 | 8511 | 7211 | |
| Exercise frequency | 3.87 | 4.08 | 4.14 | 3.55 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-K.; Chen, F.-H.; Lin, S.-F. An AI-Based Exercise Prescription Recommendation System. Appl. Sci. 2021, 11, 2661. https://doi.org/10.3390/app11062661
Chen H-K, Chen F-H, Lin S-F. An AI-Based Exercise Prescription Recommendation System. Applied Sciences. 2021; 11(6):2661. https://doi.org/10.3390/app11062661
Chicago/Turabian StyleChen, Hung-Kai, Fueng-Ho Chen, and Shien-Fong Lin. 2021. "An AI-Based Exercise Prescription Recommendation System" Applied Sciences 11, no. 6: 2661. https://doi.org/10.3390/app11062661
APA StyleChen, H. -K., Chen, F. -H., & Lin, S. -F. (2021). An AI-Based Exercise Prescription Recommendation System. Applied Sciences, 11(6), 2661. https://doi.org/10.3390/app11062661